
Abstract
Background:
Ultrasound, and sometimes cytology, cannot differentiate between recurrent or persistent thyroid cancer and benign forms of space occupying lesions (SOLs) in the thyroid bed, including unsuspected thyroid remnants, that are noted several months to years after thyroidectomy (Tx) for thyroid cancer. The purpose of the present study was to evaluate the hypothesis that measurement of thyroglobulin (Tg) in fine-needle aspirates from these lesions might help differentiate between benign and malignant SOLs in the thyroid bed.
Methods:
We studied 47 lesions in the thyroid bed from 43 patients who, 8–240 months previously, had 43 Txs for thyroid cancer. Eleven patients had a lobectomy and 32 patients had a total Tx. Also, some patients had radioactive iodine (RAI) ablation after their thyroid surgery and some did not. “Recurrence” was defined as the SOL, which was confirmed by cytological or histopathological results. “Benign SOL” was defined as a focal lesion, which was benign or nondiagnostic result on cytology and for which there was no RAI uptake on whole-body scintigraphy with both negative serum Tg and Tg antibodies. Diagnostic performances of fine-needle aspiration cytology (FNAC), FNA-Tg, and combining FNAC with FNA-Tg level were assessed for detection of malignant SOL. The diagnostic performance of FNA-Tg was assessed using three threshold values: 1 ng/mL, 10 ng/mL, and an FNA-Tg/serum-Tg ratio of 1.0.
Results:
FNA-Tg level and combining FNA-Tg levels with FNAC had higher sensitivities (100% in all three threshold values) and diagnostic accuracies (91.5%–95.7%) than FNAC alone (sensitivity of 85.3%, accuracy of 89.4%) in all threshold values. In both the RAI ablation and non-RAI ablation groups, the FNA-Tg levels and combining the FNA-Tg levels with FNAC had a higher sensitivity and diagnostic accuracy than FNAC alone with threshold values of 10 ng/mL and FNA-Tg/serum-Tg ratio of 1.0. The non-RAI ablation group did not have a different diagnostic accuracy than the RAI ablation group in all threshold values (p>0.05). FNA-Tg level showed a negative predictive value of 100% in all threshold values, in both the RAI ablation and the non-RAI ablation groups.
Conclusions:
Measurement of Tg levels in the FNA of SOLs in the thyroid bed can be helpful in diagnosing tumor recurrence, because an FNA-Tg level lower than the threshold value has the added value of suggesting a benign lesion rather than tumor recurrence.
Introduction
Methods
This retrospective study was conducted with institutional review board approval and the patient informed consent was waived.
Study population and patient's characteristics
From December 2006 to December 2010, 100 US-FNAs were performed in 94 patients at our institution for SOLs in the thyroid bed that had been detected on postoperative follow-up US for thyroid cancer. These procedures were performed 8–240 months after the patient's initial thyroid surgery. Fifty lesions in 48 patients were excluded from the study because the Tg level in the aspirate was not measured. At least one of the following criteria was required for inclusion in the study: (i) the presence of a SOL that had a positive FNA cytology result; (ii) a SOL with a negative or nondiagnostic FNA cytology result followed by pathological confirmation of a recurrent or benign lesion obtained by subsequent surgery after the SOL was detected, or a repeat FNA that was read as recurrent or benign lesion, or follow-up US for at least one year that was read as benign lesion. Three lesions in three patients that had benign cytology results were excluded because no surgical or imaging follow-up was performed. The study ultimately included 47 lesions in 43 patients (39 patients with one SOL and 4 patients with two SOLs). All of the 47 lesions were evaluated by FNA cytology and Tg determination in the FNA sample (FNA-Tg).
Clinical information from medical records, for example, the patients' demographics, operation history (total thyroidectomy [Tx] or lobectomy), type of operation, location of initial cancer, interval from Tx to FNA, and previous radioactive iodine (RAI) ablation before FNA, was reviewed retrospectively. The results of the serum thyroid hormone level tests were also reviewed. Thyroid function tests in serum (concentration of thyrotropin [TSH], Tg, Tg antibodies [Abs], triiodothyronine, free, and total thyroxine [T4]) were performed before FNA in all patients. The reference ranges for serum Tg were 0–0.1 ng/mL for patients taking thyroid hormone with appropriately suppressed serum TSH concentrations (<0.025 μIU/mL) and 0–0.2 ng/mL for patients without suppressed TSH values. Serum Tg-Abs were considered to be elevated if Tg-Ab values were >100 U/mL (14,15).
The mean age at the time of FNA for the SOL was 47.0 years (range=23–83 years), 44.9 years (range=23–83 years) for patients with recurrence, and 52.5 years (range=29–71 years) for patients with a benign lesion (p=0.15). The study group consisted of 6 men and 37 women. Among these 43 patients, 32 patients had a previous total Tx, and the remaining 11 patients had a history of lobectomy as an initial thyroid operation. Based on the medical records, among 32 patients with total Tx, 21 patients underwent previous RAI ablation and 11 patients underwent no RAI ablation. The average interval from the initial Tx to FNA for a SOL was 88.9 months (range=8–240 months). For all patients in the study, the mean size of their SOL in the thyroid bed was 7.7 mm (range=3–20 mm). It was 7.8 mm (range=4–20 mm) for patients with recurrence and 7.6 mm (range=3–18 mm) for patients with a benign lesion (p=0.9). Of the 39 cases in which the side of the original lesion was known, 20 had SOLs occurring on the ipsilateral side, 5 had SOLs lateralizing to one side following excision of a midline primary or multiple bilateral primary disease, 12 patients had SOLs on the contralateral side from the primary lesion, and 2 patients had a midline SOL following a unilateral primary tumor. All 43 of the patients in our study were being followed for a diagnosis of papillary thyroid carcinoma.
In our institution, all patients with thyroid cancer definitively diagnosed at the time of thyroid surgery were treated with LT4 in doses that were intended to suppress serum TSH to 0.025 μIU/mL or less, referred to here as “TSH suppression therapy.” In patients with extrathyroidal extension or lymph node metastasis at diagnosis, RAI ablation treatment was usually performed for remnant thyroid tissue ablation and then RAI whole-body scintigraphy (WBS) was performed. Serum Tg concentrations were measured 3 months after thyroid surgery.
Patients were followed every 6 months in the first 3 years after surgery and every 12 months afterward. Routine follow-up evaluation consisted of clinical examination every 6 months, and measurement of serum TSH, free T4, Tg, and Tg-Ab; chest X-ray; and neck US examination every 12 months. WBS, chest computed tomography (CT), or fluorodeoxyglucose positron emission tomography with CT was performed only in selected cases (e.g., those with detectable serum Tg or persistent Tg-Abs without detectable abnormal tissue on US or WBS). WBS was performed after withdrawal of LT4 for 2 or 3 weeks.
US-FNA was usually performed if there appeared to be a recurrent mass on US. Patients with lesions diagnosed as benign by FNA cytology underwent annual US follow-up. Patients with undetectable serum Tg values, no evidence of recurrence on neck US, or a benign cytology result, and no regional or distant metastasis on WBS were considered to be disease free.
US and US-guided FNA
US was performed with a 7–15 MHz linear-array transducer (HDI 5000; Philips Healthcare) or a 8–15 MHz linear-array transducer (Acuson Sequoia; Siemens Healthcare). Compound imaging was performed, limited in all cases using the HDI 5000 machine, and the size of the SOL was measured along the longest diameter on US. Size change was considered to be present if the SOL increased 20% in diameter with a minimum increase in two or more dimensions of at least 2 mm (1), compared with the previous study. The SOL's location was also recorded.
FNA was performed on an SOL in the thyroid bed by one of three radiologists having 4, 6, and 8 years of experience, respectively, in performing thyroid FNA. A 23-gauge needle connected to a 2 mL syringe was used under US guidance and a free-hand technique was employed. Each lesion was aspirated at least twice. Immediately after the first aspiration, samples were expelled onto glass slides for cytological examination and smeared. The same needle and syringe were rinsed with 1 mL of normal saline, and Tg was measured in the washout fluid (FNA-Tg). When the aspirates were serous fluid, Tg was measured in the serous fluid without adding saline (6). After smearing the sample from the second aspiration, the remainder of the material was rinsed in saline for processing as a cell block. All smears were placed immediately in 95% alcohol for Papanicolaou staining.
Cytology interpretation was done by five cytopathologists specializing in thyroid cytology. The cytology results were grouped into three categories. These categories were positive, negative, and nondiagnostic. Table 1 indicates the assignment of the original cytology readings to these categories.
Tg measurement
Tg was assayed with a monoclonal antibody immunoradiometric assay (CIS Bio International). Analytical sensitivity, defined as the smallest detectable concentration different from zero with a probability of 95%, was 0.2 ng/mL. Functional sensitivity, calculated with the imprecision profile for a coefficient of variation equal to 20%, was 0.7 ng/mL. FNA wash samples were not assayed for Tg autoantibodies (Tg-Abs) because it has been shown that FNA-Tg measurements are not affected by serum Tg autoantibodies (16,17).
Image analysis
One radiologist (J.Y.K.) with 9 years of experience in thyroid imaging, who was blinded to the cytologic results of FNA and histopathologic results (only in cases with subsequent surgery), retrospectively reviewed the US examinations. Image analysis included assessment of echogenicity, margin, shape, heterogeneity, and presence of cystic components and calcification. The echogenicity of the lesion was evaluated by comparing it with that of the surrounding strap muscle and was then divided into three groups: hyperechoic, isoechoic, and hypoechoic. The margin was categorized as either well-defined or not well-defined. Shape was divided into two groups, “taller than wide” and “wider than tall” shape, with reference to anterior-posterior to transverse dimensions as a ratio (AP/T) of 1: “taller than wide” shape indicated AP/T>1 and “wider than tall” shape indicated that AP/T was ≤1. US features that were considered to be suspicious for tumor recurrence were the following: hypoechogenicity, a poorly defined margin, heterogeneity, taller than wide shape, presence of a cystic component, and presence of calcification (4).
Reference standard
The reference standards were by the pathology results from subsequent surgical excisions, or FNA cytologic results, or long-term imaging follow-up for at least one year that did not show interval change in size if the patient did not undergo subsequent surgical excision. Two nondiagnostic FNA cytology results were classified as negative for recurrence for statistical analysis (18). “Recurrence” was defined as the SOL, which was confirmed by cytological or histopathological results (6,18). “Benign SOL” was defined as a focal lesion, which was benign or nondiagnostic on cytology result and for which there was no RAI uptake on WBS after administration of RAI to patients with both negative serum Tg and Tg-Abs.
Statistical analysis
The Student's t-test was used to compare patient's ages and the lesion sizes on US in recurrent and benign lesions. The Chi-square test was performed to evaluate the differences between recurrent and benign groups by each US feature. FNA-Tg level was compared between recurrent and benign lesions, and between the RAI and non-RAI groups using Student's t-test.
Diagnostic performances, including sensitivity, specificity, accuracy, positive predictive value and negative predictive value (NPV) of FNA cytology, FNA-Tg, and combining FNA cytology with FNA-Tg level, were assessed. The diagnostic performance of FNA-Tg was assessed using three threshold values of 1 ng/mL, 10 ng/mL, and an FNA-Tg/serum-Tg ratio of 1.0 (6,8). The McNemar test for statistical significance was used to compare the sensitivity and accuracy of diagnosing tumor recurrence between three FNA-Tg threshold values and FNA cytology alone. Evaluating the diagnostic performance of combining FNA cytology with the FNA-Tg threshold value, the final diagnosis was considered positive for recurrence if at least one of any of the criteria was positive. When FNA cytologic results were negative or nondiagnostic for malignancy, the FNA-Tg level was evaluated and compared with the final diagnosis. Clinical information and laboratory findings of these cases were also evaluated.
The diagnostic performances were analyzed in both the RAI ablation group and the non-RAI ablation group. Receiver operating characteristic (ROC) curves were drawn for each criterion and, the area under the ROC curve (Az) for each criterion was compared between the RAI ablation and the non-RAI ablation groups for the comparison of diagnostic performances between two groups. The univariate z-score test was used to assess the significance of differences in the Az of the RAI ablation and non-RAI ablation groups. The diagnostic performances were also compared between groups according to the presence of lesion size change.
For all analyses, the results were considered statistically significant if the p value was <0.05. For statistical analysis, we used a computerized statistics program (SAS version 9.1 for Windows; SAS Institute).
Results
Final diagnosis
The reference standard diagnosis was based on pathologic confirmation after subsequent surgery following FNA or the initial FNA cytology in 32 lesions, by the follow-up FNA cytology in 5 lesions, and by follow-up imaging for at least one year in 10 lesions (Fig. 1).
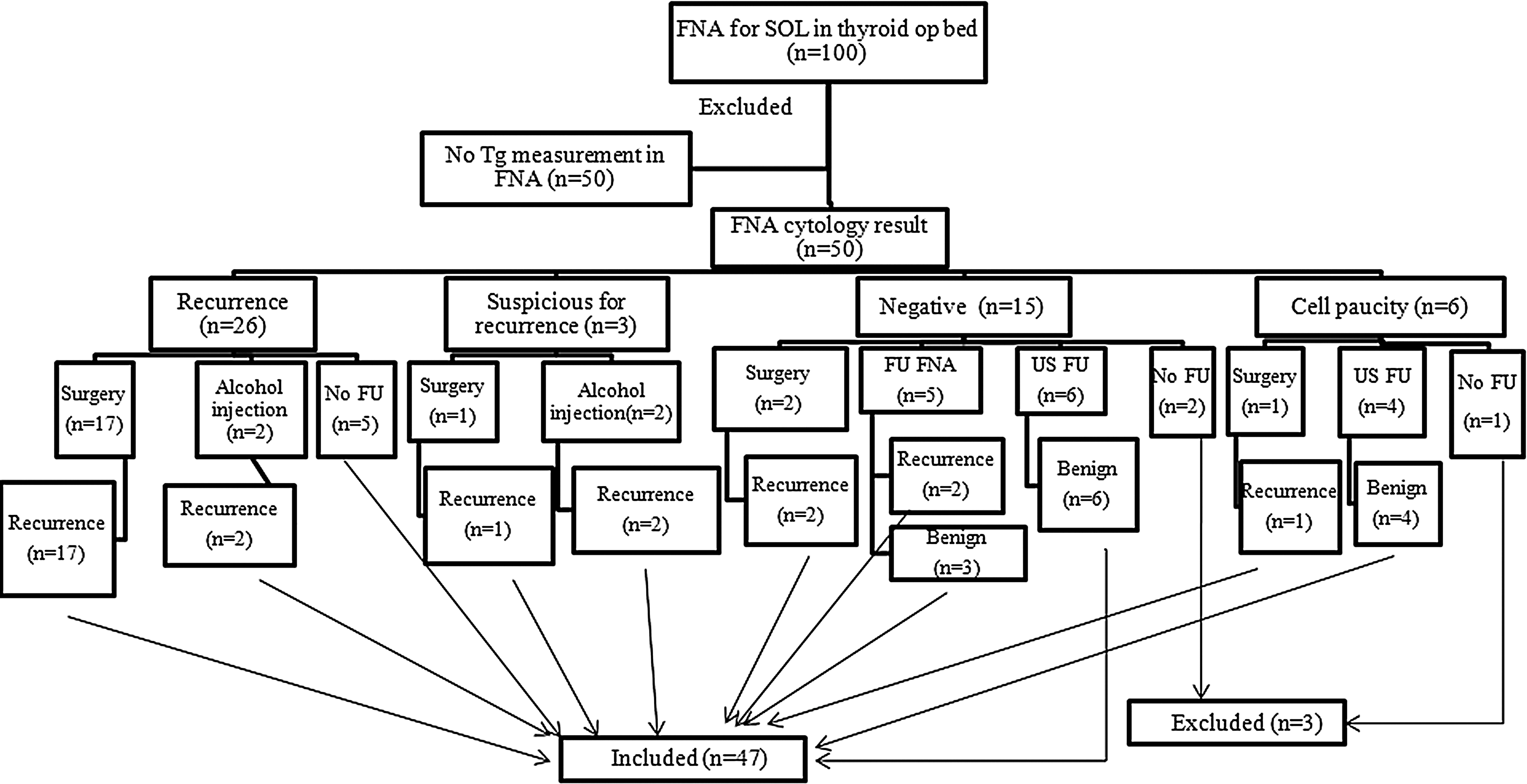
Diagram of FNA cytologic results and standard reference. FNA, fine-needle aspiration; SOL, space occupying lesion; Tg, thyroglobulin; FU, follow-up; US, ultrasound.
US features relating to final diagnosis
Among the six US features reviewed, none showed a statistically significant difference between recurrent and benign lesion (Table 2; Figs. 2 and 3).

US of tumor recurrence in a 49-year-old man who underwent total thyroidectomy for PTC 175 months ago and no subsequent RAI ablation. Longitudinal US image demonstrates a space occupying lesion (maximum diameter=8 mm) showing hyperechogenicity compared with that of strap muscle (asterisk) in the left thyroid bed (arrows). The lesion showed a well-defined margin, wider than tall shape, and overall heterogenous echogenicity. There are multiple, dot-like internal echoes suggesting microcalcifications (arrowhead). This lesion was diagnosed as negative for malignancy on US-FNA cytology but showed an FNA-Tg level of 500 ng/mL, and repeat FNA cytology result after 10 months showed tumor recurrence. PTC, papillary thyroid carcinoma; RAI, radioactive iodine.

US of benign lesion in a 66-year-old man who underwent total thyroidectomy for PTC 40 months ago and subsequent RAI ablation. Transverse US image demonstrates an isoechoic space occupying lesion (maximum diameter=7 mm) relative to the strap muscle (asterisk) with a taller-than-wide shape in the left thyroid bed (arrow; T=trachea). The lesion shows a well-defined margin and overall homogenous echogenicity. This lesion twice showed a negative result on US-FNA cytology, with an FNA-Tg level of 0.2 ng/mL. Serum Tg and Tg-Ab level at the time of FNA was undetectable. There was no increase in size on follow-up imaging study after one year and it was considered as a benign lesion.
US, ultrasound.
FNA results
On the initial FNA cytology, 29 lesions were considered positive for malignancy, 26 of which were recurrent for malignancy and 3 of which were read as suspicious for recurrence. All of these 29 lesions were considered to be recurrent for malignancy based on either pathology after subsequent surgery (n=18) or the initial FNA cytologic result (n=11). Among these 11 SOLs that were considered to be recurrent based on the initial positive FNA cytology results, 4 were treated with alcohol injection and were then followed, 1 received RAI ablation, and 6 did not undergo follow-up. Among the remaining 18 lesions, 13 were negative for malignancy, and 5 yielded nondiagnostic results due to cell paucity (Table 3). Among 13 lesions with negative cytology results, 4 were considered to be recurrent: 2 based on subsequent surgery and 2 based on positive readings for malignancy in follow-up FNA procedures. The remaining nine lesions were considered to be benign: five based on negative results in follow-up FNAs and the other four based on a decrease in size, or no interval change, in follow-up imaging studies. One of five cases with nondiagnostic cytology results was confirmed as recurrence by surgery, and the other four cases were regarded as benign lesions on further follow-up: one showed no change in size on follow-up US after 14 months and a second SOL disappeared at 3-month follow-up after FNA. The third and fourth SOLs in this category showed no change in size on follow-up US after one year. Consequently, 34 lesions were considered to be recurrent and the other 13 lesions were considered to be benign.
The pathologic diagnosis of initial tumor was papillary carcinoma in all lesions.
False positive cases of FNA-Tg.
FNA, fine-needle aspiration; RAI, radioactive iodine; Tg, thyroglobulin; ND, nondiagnostic.
Tg in washout fluid readings
Figure 4 shows Tg levels measured in FNA washout fluid in recurrent and benign lesions. In recurrent lesions, the mean FNA-Tg level was 387.5 ng/mL (range=12.27–500.0 ng/mL, median=500.0 ng/mL) and in benign lesions it was 38.9 ng/mL (range=0.2–460.0 ng/mL, median=0.2 ng/mL; p<0.001). There were 18 cases with negative or nondiagnostic FNA cytology that had a mean FNA-Tg level of 2.99 ng/mL (range=0.1–33.0 ng/mL, median=0.4 ng/mL). The diagnostic performances of FNA-Tg in all threshold values were not significantly different when changes in lesion size were detected (p>0.05).
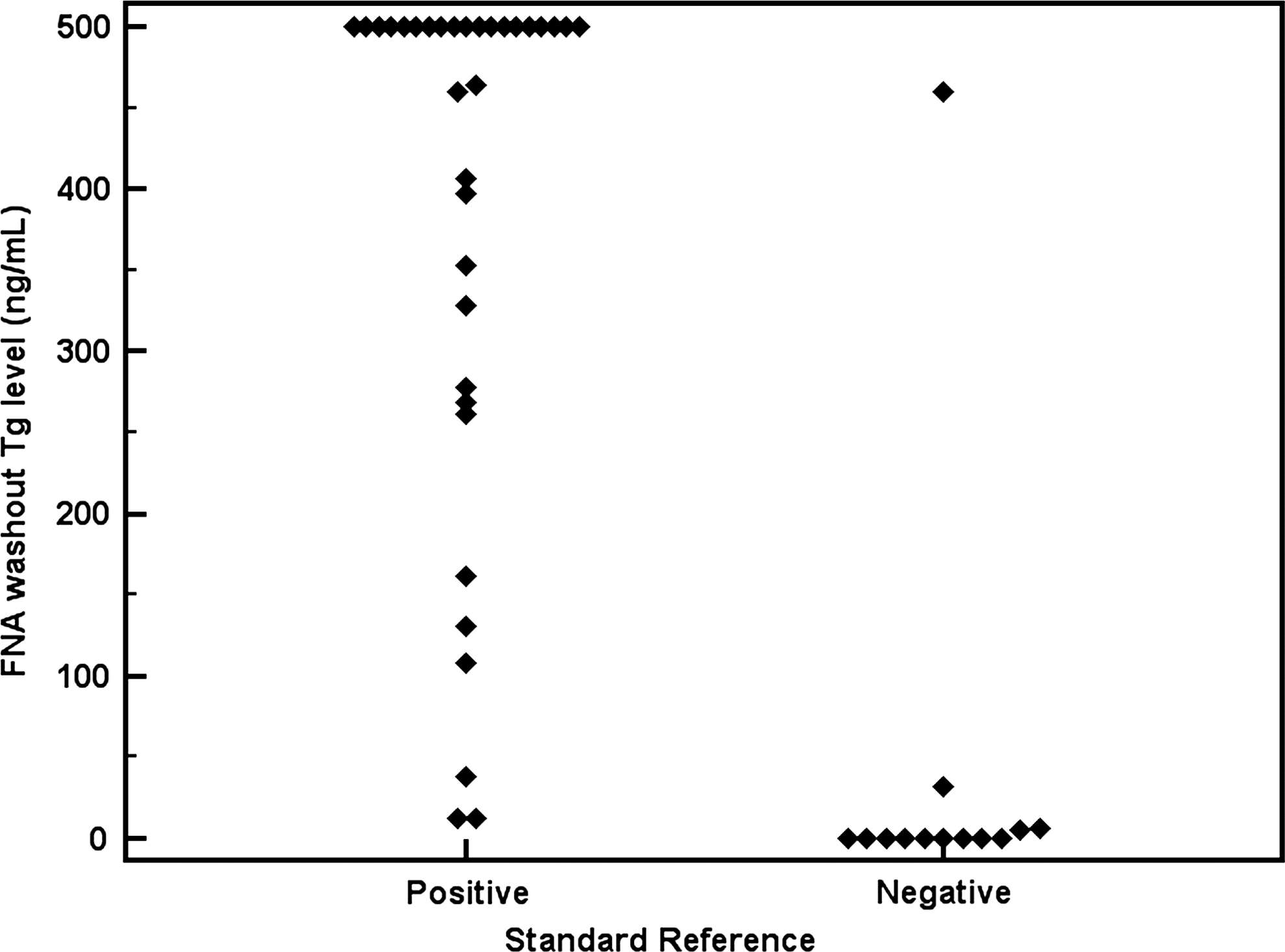
Plots of Tg concentrations in FNA washouts according to standard reference.
Utility of combining FNA cytology readings with Tg in washout fluid readings
Table 4 shows the diagnostic performances of FNA cytology, FNA-Tg level, and combining FNA cytology and Tg level (for the three threshold values). The NPV of FNA-Tg levels and combining FNA-Tg levels with FNA cytology was 100% for all three threshold values. FNA-Tg levels and combining FNA-Tg levels with FNA cytology had a higher sensitivity (100% in all three threshold values) and accuracy (91.5%, 95.7%, and 91.5% in each threshold value, respectively) than FNA cytology alone (sensitivity of 85.3% and accuracy of 89.4%) in all threshold values (p=0.004 for threshold of 1 ng/mL and FNA-Tg/serum-Tg ratio of 1, and p=0.016 for 10 ng/mL).
TP, true-positive; TN, true-negative; FP, false-positive; FN, false-negative; PPV, positive predictive value; NPV, negative predictive value; FNAC, fine-needle aspiration cytology; S-Tg, serum Tg.
There were four false positive cases of FNA-Tg, which had negative FNA cytology but an FNA-Tg level exceeding the serum Tg level (threshold level of FNA-Tg/serum-Tg level or 1; Table 3, lesion numbers 11, 13, 15, and 17). One case (lesion 11) had an FNA-Tg level of 32.1 ng/mL and a serum Tg level of <0.2 ng/mL. The cause of this false positive result may be remnant thyroid tissue that could not be seen on US, because this patient had previously undergone a lobectomy without subsequent RAI ablation. The measurement of the serum Tg and FNA-Tg level was performed on the same day and the serum TSH level was suppressed (<0.04 ng/mL) in this patient. The second case (lesion 13) had an FNA-Tg level of 460.0 ng/mL and a serum Tg level of <0.2 ng/mL. The time interval between measurement of serum Tg and the FNA-Tg level was 29 days, and the serum TSH level was suppressed (<0.04 ng/mL) in this patient. The other two cases (lesions 15 and 17) had an FNA-Tg level lower than 10 ng/mL (0.4 ng/mL and 5.18 ng/mL, respectively) but the serum Tg levels of these patients were very low (<0.2 ng/mL and 0.5 ng/mL, respectively), leading to an FNA-Tg/serum-Tg ratio of >1. These two cases were considered as false positive when applying the threshold value of FNA-Tg/serum-Tg ratio of 1, but not considered as false positive when the other two threshold values were used. The time interval between the serum Tg and FNA-Tg levels was 96 days and 1 day, and TSH level was 14.35 ng/mL (stimulated) and <0.04 ng/mL (suppressed), respectively. In our study, there was no false negative FNA-Tg case.
Table 5 indicates the diagnostic value of the FNA-Tg level in 18 patients with initial FNA cytology results that were negative or nondiagnostic.
Relationship of FNA and FNA-Tg level with clinical and laboratory data
Correlation of FNA and FNA-Tg with serum Tg and Tg-Ab level was performed only in 36 thyroid bed lesions with previous total Tx. Among the six lesions with elevated serum Tg levels with a normal serum Tg-Ab level in total Tx patients (four had received previous RAI ablation and two had not received RAI ablation), five recurrences had positive FNA cytology results and increased FNA-Tg levels over 300 ng/mL. Another was considered to be a benign lesion with a nondiagnostic FNA cytology result and an FNA-Tg level of 5.97 ng/mL; the cause of this serum Tg elevation was unclear, but the follow-up serum Tg level was normal. Two SOLs with normal serum Tg levels but elevated serum Tg-Ab levels in total Tx patients were recurrences with surgical confirmation; they had positive FNA cytology results and an FNA-Tg level of 500 ng/mL. Of the remaining 28 lesions with total Tx with normal Tg and Tg-Ab levels in the serum, 19 lesions were considered to be recurrences.
Medical records of previous RAI ablation were available for all patients. Table 6 shows the diagnostic values of FNA cytology and the FNA-Tg level in the group with previous RAI ablation (23 lesions in 21 patients) and the group without RAI ablation (24 lesions in 22 patients). In both the RAI ablation and the non-RAI ablation groups, the FNA-Tg level had an NPV of 100% in the three threshold values. The FNA-Tg level and combining the FNA-Tg levels with the FNA cytology had a higher sensitivity and diagnostic accuracy than FNA cytology alone with threshold values of 10 ng/mL and an FNA-Tg/serum-Tg ratio of 1.0. For all threshold values, the non-RAI ablation group had the same diagnostic accuracy as the RAI ablation group (p>0.05).
Discussion
The American Thyroid Association guidelines recommend periodic serum Tg measurements and neck US after thyroidectomy in patients being treated for thyroid cancer (1). Although serum Tg has a high degree of sensitivity to detect thyroid cancer, especially after total Tx and remnant ablation, with the highest degrees of sensitivity following thyroid hormone withdrawal or stimulation using recombinant TSH (19,20), the utility of the serum Tg level in detecting tumor recurrence is limited by interference by Tg-Abs, issues relating to quality control, low basal or stimulated Tg levels in aggressive or poorly differentiated tumors, and noise created by non-cancer remnant thyroid tissue (14,19,21,22). In patients with a previous thyroid-preserving surgery (e.g., lobectomy or subtotal Tx) or total Tx without subsequent RAI ablation who are thought to have remnant thyroid tissue, serum Tg levels can be elevated without tumor recurrence (22).
US can be a highly sensitive method for detecting recurrence even when the serum Tg level is not elevated (1,22,23). Indeed, in our study, 28 SOLs out of a total of 36 lesions in patients with previous total Tx were detected on US without evidence of elevation of serum Tg or Tg-Ab levels. However, although US may be an excellent diagnostic modality for recurrence in the neck, the diagnostic value of US to differentiate between malignant and benign lesions when a SOL is newly detected in the thyroid bed on follow-up US is somewhat controversial (3,18,24,25). Although US features were not helpful in our study, this result may come from interobserver variability in the interpretation of US findings and a relatively small number of cases included in our study. Also, in our study, SOLs in the thyroid bed were usually aspirated when a recurrence was suspected on US. Therefore, some selection bias might exist and could affect the results. Thus, further studies should address this topic (4,5).
Although FNA is a useful and excellent modality with high diagnostic accuracy for the detection of tumor recurrence or neck node metastasis, several factors can lead to false negative or nondiagnosis in up to 20% of cases (7,12,26). Measurements of FNA-Tg levels can be helpful in diagnosing false negative or nondiagnostic cases and combining FNA cytology with FNA-Tg levels can improve the diagnostic value of neck node metastasis (6,10,12,26). In cases where lateral neck metastases are suspected, measurement of Tg levels in FNA needle washout will have a high accuracy because there is no remnant thyroid tissue. In contrast, the presence of remnant thyroid tissue in patients who do not have subsequent RAI ablation, decreases the specificity of the serum Tg determinations (13). For the same reason, we think that noncancerous remnant thyroid tissue may affect the diagnostic accuracy of FNA-Tg of SOLs in the thyroid bed if patients do not undergo RAI ablation. Until now, there have been no studies addressing the value of FNA-Tg determinations in the thyroid bed with a focus on whether RAI ablation was performed. Therefore, we considered the possibility that remnant thyroid tissue would affect FNA-Tg and our study investigated the added value of FNA-Tg measurement combined with FNA cytology in the diagnosis of recurrences in the thyroid bed, comparing results between the RAI ablation and the non-RAI ablation groups. Because the diagnostic FNA-Tg threshold value has not yet been well established, and because it can be affected by the serum Tg level, we analyzed cases using three different threshold values—1 ng/mL, 10 ng/mL, and an FNA-Tg/serum-Tg ratio of 1.0 (6,8,27).
In our study, the NPV of the FNA-Tg level was 100% for all threshold values, regardless of previous RAI ablation after surgery. Although previous studies addressing the value of FNA-Tg in the diagnosis of metastatic cervical lymph nodes reported an overlapping range of FNA-Tg levels between benign and metastatic lymph nodes, a negative FNA-Tg level was observed only in benign lesions. Therefore, no false negative FNA-Tg case was present. This suggests that a negative FNA-Tg level indicates a benign lesion rather than a recurrence, which may be an important reason for the measurement of an FNA-Tg level. However, since the number of cases was relatively small, future studies with a larger number of cases are needed to establish the true NPV of a negative FNA-Tg determination.
We measured Tg levels in FNA needle washouts of 47 SOLs and found that the diagnostic performance of FNA-Tg levels, whether alone or in combination with FNA cytology, had higher sensitivity and accuracy than FNA cytology alone. The non-RAI ablation group had a slightly lower diagnostic accuracy than the RAI ablation group for all diagnostic criteria, but this was not statistically significant. Moreover, sensitivity and accuracy improved in both the RAI ablation group and the non-RAI ablation group for all Tg threshold values. Therefore, measurements of Tg levels in FNA of SOLs in the thyroid bed may be a useful diagnostic method in patients with remnant thyroid tissue.
Although FNA-Tg measurement had a higher diagnostic accuracy than FNA cytology alone, discordant FNA-Tg positive and FNA cytology negative cases occurred. There were four false positive cases of FNA-Tg in our study using the threshold value for FNA-Tg/serum-Tg ratio of 1; however, only two false positive cases were observed when two threshold values other than the FNA-Tg/serum-Tg ratio of 1 were applied. These two false positive cases among 47 SOLs (4.3%) had elevated FNA-Tg levels (32.1 ng/mL and 460.0 ng/mL, respectively) compared with all threshold values used in the analysis, which was similar to the false positive rate (1%–6%) of FNA-Tg levels in previous studies (8,10,11). The cause of the false positive result in the first patient (Table 3; lesion 11) may be remnant thyroid tissue that could not be seen on US, because this patient had previously undergone a lobectomy without subsequent RAI ablation. However, because the second false positive case (Table 3; lesion 13) had undergone a total Tx and subsequent RAI ablation, remnant thyroid tissue does not appear to be the reason for the result. Rather, some aspects of the FNA procedure may contribute to the result, for example, the contamination of aspirates with blood containing high Tg levels or the inadvertent passage of the needle through normal thyroid tissue (6).
Our study has several limitations. First, it was retrospective and included only patients who underwent US-guided FNA with additional Tg tests in FNA washouts of SOL in the thyroid bed, and who underwent subsequent surgery or imaging follow-up for at least one year. Therefore, some degree of selection bias may exist. Second, the number of cases included in our study was relatively small, especially cases with total Tx and no subsequent RAI treatment. Future studies with a larger group of patients will be needed in order to generalize our results. Third, the appropriate threshold values of FNA-Tg levels could not be determined in our study due to the small number of cases. A recent study suggested appropriately combined diagnostic threshold values for Tg in the FNAs of metastatic lymph nodes, based on diagnostic performance (6). However, regarding SOL in the thyroid bed, only a few studies have investigated the utility of FNA of SOLs (5), and the proper threshold value of Tg levels has not been determined. Finally, not all lesions were confirmed by histopathology. However, the diagnosis of lesions without pathologic confirmation was made carefully, by the FNA cytology result in the case of positive cytology results, and by follow-up FNA cytology or imaging in the case of a negative or nondiagnostic result.
In conclusion, measurement of Tg levels in FNA of SOLs in the thyroid bed can be helpful in diagnosing tumor recurrence. An FNA-Tg level lower than the threshold value may have the added value of indicating a benign lesion rather than tumor recurrence.
Footnotes
Disclosure Statement
No competing financial interests exist.