
Abstract
Background:
Cervical lymph node metastases from differentiated thyroid cancer (DTC) are common. Thirty to eighty percent of patients with papillary thyroid cancer harbor lymph node metastases, with the central neck being the most common compartment involved. The goals of this study were to: (1) identify appropriate methods for determining metastatic DTC in the lateral neck and (2) address the extent of lymph node dissection for the lateral neck necessary to control nodal disease balanced against known risks of surgery.
Methods:
A literature review followed by formulation of a consensus statement was performed.
Results:
Four proposals regarding management of the lateral neck are made for consideration by organizations developing management guidelines for patients with thyroid nodules and DTC including the next iteration of management guidelines developed by the American Thyroid Association (ATA). Metastases to lateral neck nodes must be considered in the evaluation of the newly diagnosed thyroid cancer patient and for surveillance of the previously treated DTC patient.
Conclusions:
Lateral neck lymph nodes are a significant consideration in the surgical management of patients with DTC. When current guidelines formulated by the ATA and by other international medical societies are followed, initial evaluation of the DTC patient with ultrasound (or other modalities when indicated) will help to identify lateral neck lymph nodes of concern. These findings should be addressed using fine-needle aspiration biopsy. A comprehensive neck dissection of at least nodal levels IIa, III, IV, and Vb should be performed when indicated to optimize disease control.
Introduction
Optimizing the surgical approach is fundamental to appropriate initial management of DTC and involves balancing the risks and benefits of thyroidectomy and neck dissection (11,12). Because DTC is more indolent than squamous cell carcinoma metastatic to the lymph nodes of the neck, it is not possible to universally extrapolate from one disease to the other. The primary goals of this interdisciplinary consensus review were to identify methods for determining when metastatic DTC is present in the lateral neck and to address the extent of lymph node dissection appropriate for control of the lateral neck supported by contemporary medical literature, balanced against the known risks of surgical therapy.
Regional lymph node spread from thyroid cancer can broadly be classified as central neck compartment and lateral neck compartment metastases. Lymph node metastases are most commonly found in the central neck compartment (level VI and level VII). The central neck dissection anatomy and terminology have been previously defined by the American Thyroid Association (ATA) Consensus Statement on the Terminology and Classification of Central Neck Dissection published in the November 2009 issue of Thyroid (13). Although less frequent, metastases to lymph nodes in the lateral neck, levels I–V may be associated with a worse prognosis (14). There is a clear association between central neck involvement and the likelihood of lateral neck disease, as an increase in the number of positive central neck lymph nodes is associated with a higher likelihood of lateral neck disease (15,16).
The more extensive dissection required for lateral neck lymph node metastases is associated with cosmetic concerns, such as a longer incision, and the potential for nerve injury (accessory, marginal mandibular, sympathetic, phrenic, vagus, hypoglossal, cervical sensory branches, brachial plexus, and greater auricular nerves), hemorrhage, and chyle leak that are not associated with thyroidectomy alone with or without central neck dissection (17,18). Complications from lateral neck dissections can be as high as 50%, with a 3.6% incidence of chyle leak and an 11% or greater incidence of chronic neck pain and numbness (19). Some studies show that the addition of a lateral neck dissection to central neck compartment surgery (thyroidectomy or central neck dissection) doubles the risk of transient postoperative hypoparathyroidism (19,20). Strict indications for lateral neck dissection for DTC are necessary to optimize a benefit profile expected to outweigh the risks of the procedure. Many philosophies for managing the lateral neck in DTC are presented in the literature, including elective nodal sampling, ultrasound (US) directed compartment resections, and super selective nodal dissection that is, levels III–IV, leading to some controversy regarding when and how to manage the lateral neck in DTC (21).
A subcommittee on Lateral Neck Dissection from the Surgical Affairs Committee of the ATA was organized and tasked with reviewing the existing literature regarding lateral neck dissection and DTC. Additionally, this subcommittee was tasked to review the salient anatomy and imaging as it related to the lateral neck and provide recommendations for consideration in the next iteration of the ATA management guidelines for patients with thyroid nodules and DTC and future guidelines on this topic from other sources (22). In the present report the authors, all of whom are members of this subcommittee, present a review of this topic and provide consensus opinions and recommendations.
Review
Clinical factors in detection of lateral lymph node metastasis
A number of important factors in the patient's history are relevant to the risk for and detection of lateral neck metastases in patients with DTC (Table 1). First, it is important to consider other risk factors, including but not limited to the patient's age, gender, tumor size, presence of lymphovascular invasion, extra-thyroidal extension, and presence of central compartment nodal disease. Younger patients and men appear to have a significantly higher risk of cervical lymph node metastasis than older patients or women (23). Recent identification of molecular alterations that predict more aggressive disease, such as the presence of the BRAF mutation (24), may be important markers to consider when assessing the risk for lateral neck metastasis. Consistent with the 2009 ATA guidelines (14), BRAF or other markers being positive alone are insufficient justification to do a prophylactic lateral neck dissection at the present time.
AJCC, American Joint Commission on Cancer; DTC, differentiated thyroid cancer.
In the setting of primary or recurrent DTC, features such as palpable hard/firm lymph nodes should prompt a thorough and comprehensive assessment of the lateral neck by clinical and radiographic examination. Moreover, in the 2009 Revised ATA management guidelines for patients with thyroid nodules and DTC (14), hitherto referred to as ATA Thyroid cancer guidelines, recommendation 21 suggests that preoperative high resolution US examination of the contralateral thyroid lobe and cervical lymph nodes is the standard for all patients undergoing thyroid surgery for malignant cytology (14). Central neck nodes can be challenging to image in the preoperative setting due to the presence of an intact thyroid gland, but no such limitation exists for lateral neck imaging. US-guided biopsy of sonographically suspicious nodules and/or lymph nodes in the lateral neck should be performed whenever possible (Table 2) (14). Cystic lymph nodes should be approached with a high degree of suspicion as they are frequently positive cytologically or by Tg (25). On occasions, cytologic diagnosis is not possible due to scanty material obtained from fine-needle aspiration biopsy (FNAB), and the FNAB should be repeated. Thyroglobulin washings of FNAB aspirates may also be helpful in this situation and can be reliable even in the presence of circulating thyroglobulin antibodies (26). If the node or nodule is not amenable to biopsy or will not render a diagnosis by cytologic evaluation or Tg aspirate assay, watchful waiting for growth on serial USs may be prudent.
CCA, common carotid artery.
With a history of thyroid surgery for cancer and an elevated or rising serum Tg level, a thorough search for persistent and/or recurrent/residual disease should include assessment of the lateral neck, initially using high resolution US examination. Nuclear medicine scanning may also be a part of the diagnostic evaluation of recurrence. Disease burden is roughly reflected in the Tg level in relation to the serum thyroid stimulating hormone (TSH) level; TSH provocation of Tg response can be elicited by direct TSH injection, or by thyroid hormone withdrawal and secondary TSH elevation. Positive Tg measurements measured in a state of a suppressed TSH are more concerning for recurrent/residual/bulky disease. Reliability of the Tg assay and the presence of interfering anti-thyroglobulin antibodies are important considerations when evaluating absolute Tg levels or trends.
Definition of the lateral neck anatomy
The stated goals of developing classifications for neck dissection are to uniformly define the clinical and surgical boundaries of each of the lymph node groups removed in a neck dissection and to develop a classification that correlates with the biology of cervical metastases thus meeting the compartmental excision standards following basic oncologic principles (27) (Fig. 1). This classification was used to describe the patterns of metastatic dissemination observed in more than 1000 squamous cell carcinoma patients who were treated with neck dissections from a surgeon's perspective (28). Lymph nodes in the lateral neck are grouped into levels I–V, corresponding with the submandibular and submental nodes (level I); upper, middle, and lower jugular nodes (levels II, III, IV respectively); and posterior triangle nodes (level V). Levels VI and VII, commonly referred to as the central neck have already been recently well described and will not be dealt with further in this article (13). This system of nodal levels has been widely accepted, allowing data to be reported without ambiguity and among health care providers who perform oncologic neck surgery. Boundaries of these levels are:
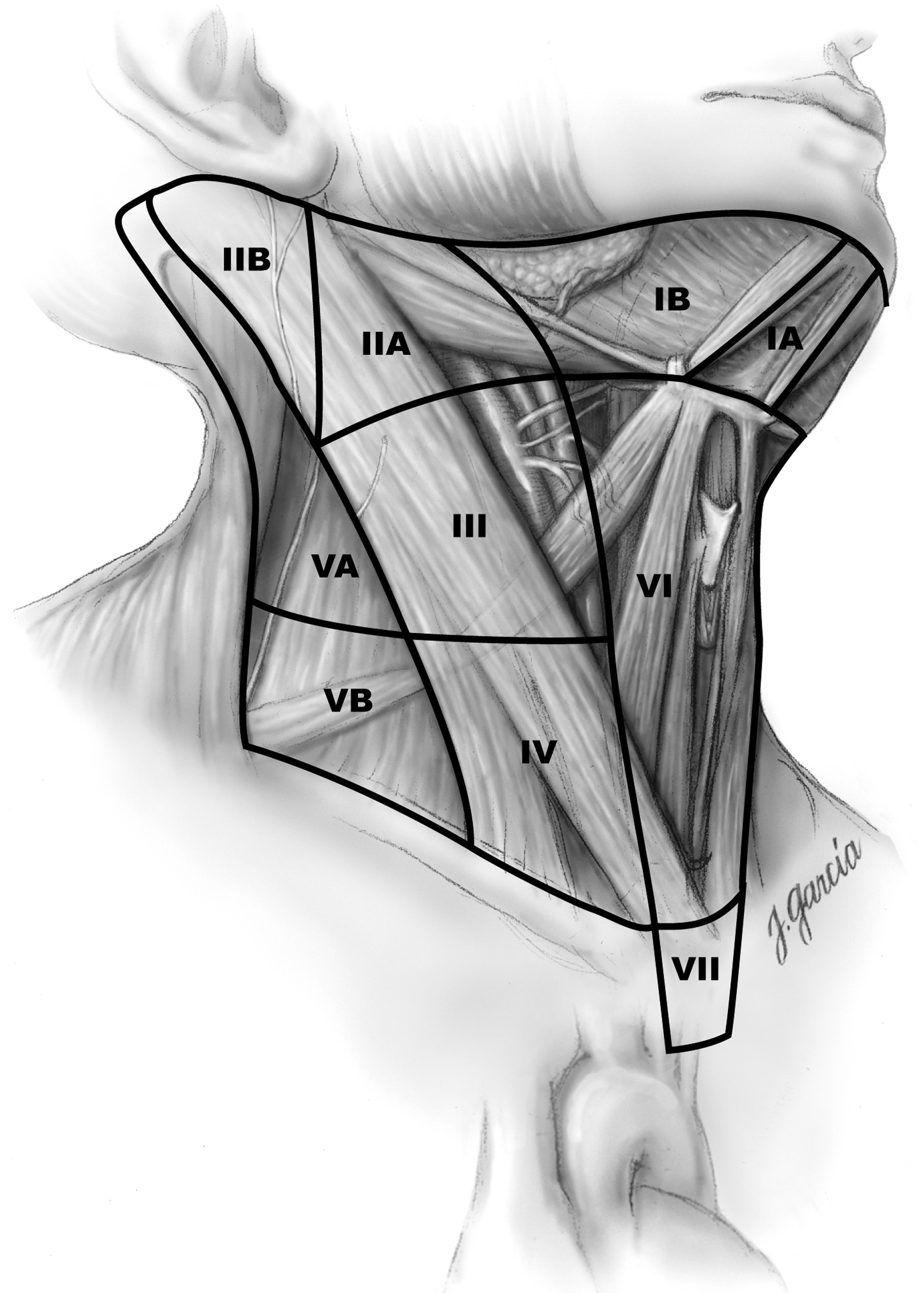
Nodal levels with corresponding anatomic landmarks (used with permission from R. Udelsman, M.D.).
• Level I: (Submandibular; submental) nodes are defined by the body of the mandible superiorly, stylohyoid muscle posteriorly, and the anterior belly of the digastric muscle on the contralateral side anteriorly. This level may be subdivided into a single midline level Ia, the submental triangle (bounded by the anterior bellies of the bilateral digastric muscles and the hyoid bone), and Ib, containing the submandibular gland and its nodes.
• Level II: (Upper jugular) are located by the upper third of the jugular vein; it extends from the skull base to the inferior border of the hyoid bone. The anterior border of level II is the stylohyoid muscle, and the posterior border is the posterior border of the sternocleidomastoid muscle (SCM). The spinal accessory nerve, which travels obliquely across this area, is used as a landmark to subdivide this group into IIb, the portion above and behind the nerve, and IIa, the portion that lays anteroinferiorly. This level contains the jugulodigastric nodes.
• Level III: (Mid jugular) nodes are located between the hyoid above and a horizontal plane defined by the inferior border of the cricoid cartilage below. The sternohyoid muscle demarcates the anterior limit of level III, and the posterior border of the SCM is the posterior border of this level.
• Level IV: (Lower jugular) nodes are adjacent to the lower third of the jugular vein. These nodes are located between the inferior border of the cricoid cartilage and the clavicle, and like level III, the anterior boundary is the sternohyoid muscle, and the posterior boundary is the posterior border of the SCM. Thyroid cancer may cause prominent metastatic disease in this region. This level may contain many lymph vessels which connect to the thoracic duct on the left.
• Level V: (Posterior triangle) is bound anteriorly by the posterior border of the SCM and posteriorly by the anterior border of the trapezius muscle. This level extends from the convergence of the sternocleidomastoid and trapezius muscles superiorly to the clavicle inferiorly. This level is subdivided by a plane defined by the inferior border of the cricoid cartilage into level Va superiorly and level Vb inferiorly. Level Va contains the nodes surrounding the spinal accessory nerve, and level Vb contains the transverse cervical and supraclavicular nodes.
Subzones were established in levels I, II, and V in response to the increasing awareness that specific sublevels had lower or higher risk for nodal metastases (29): levels Ia, Ib, IIa, IIb, Va, and Vb. In 2008, further modifications were proposed, adopting radiographic landmarks and creating alternative borders to define levels I and II: the vertical plane defined by the posterior edge of the submandibular gland instead of, or in addition to, the clinically visible border of the stylohyoid muscle. It was further proposed that the medial aspect of the common carotid artery be an alternate landmark for separating the medial border of levels III and IV from the lateral border of level VI, which had traditionally been the lateral border of the sternohyoid muscle (30).
Imaging is an integral part of the assessment of thyroid cancer patients. The use of imaging in all of its forms has proliferated over the last three decades. Imaging findings often complement the physical examination, and an imaging-based classification provides the radiologist with guidelines for classifying the location of cervical nodes and communicating these findings to clinicians. Although the level numbering system is the same, some fine nuances separating nodal levels are introduced by the image-based system. Som et al. proposed the following computerized tomography (CT)-based node level classifications (31): • Level I: All nodes above the hyoid bone, below the mylohyoid muscle, and anterior to a transverse line drawn on each axial image through the posterior edge of the submandibular gland. • Level II: Extends from the skull base at the lower level of the bony margin of the jugular fossa, to the level of the lower body of the hyoid bone. Level IIA nodes are level II nodes that surround the internal jugular vein (IJV). Level IIB nodes lie posterior to the spinal accessory cranial nerve (CN) deep to the SCM and are separated from the IJV by a fat plane. • Level III nodes lie between the level of the lower body of the hyoid bone and the level of the lower margin of the cricoid cartilage. • Level IV nodes lie between the level of the lower margin of the cricoid cartilage arch and the level of the clavicle on each side, as seen on axial CT scan. • Level V nodes extend from the skull base at the posterior border of the attachment of the SCM to the level of the clavicle. Level Va nodes lie between the skull base and the level of the lower margin of the cricoid cartilage arch, behind the posterior edge of the SCM. Level Vb nodes lie between the level of the lower margin of the cricoid cartilage and the level of the clavicle (31).
Classification of neck dissections
Consistency in description of lateral neck dissection is crucial to allow for a comparison of outcomes in those series reported in the literature. For example, it is insufficient to use qualifiers such as modified radical neck dissection without designating what levels were removed and what associated structures, if any, were sacrificed. Radical neck dissection is defined as removal of lymph nodes from levels I–V and resection of the IJV, the spinal accessory nerve (CN XI), and the SCM. This was originally described by George Crile in 1906, and it resulted in significant associated morbidity, and it is infrequently used today (32,33). Modified radical dissection describes comprehensive removal of nodal basins (levels I–V) with preservation of one or more of the following non-lymphatic structures: CN XI, IJV, or SCM. A selective neck dissection refers to removal of less than all five nodal levels, and is directed by the patterns of lymphatic drainage from the primary tumor, while preserving CN XI, IJV, and SCM (34,35). This is the most commonly used neck dissection in the management of lateral neck metastasis for thyroid cancer and should be reported with a designation of side and nodal levels and sublevels dissected (i.e., selective neck dissection of levels IIa, III, IV, and Vb).
Lateral neck dissection
The complications of lateral neck dissection are significant and must be factored into the equation of risks and benefits. The primary complication considered for lateral neck dissection is injury to the eleventh CN. Although this injury is rarely caused by nerve transection, the acts of dissection and retraction might be sufficient to cause temporary or permanent weakness in up to 20% of patients (36). This risk is increased when levels IIb and Va are dissected. Patients experience debilitating shoulder droop and inability to raise the arm above the horizon. In some chronic cases, shoulder movement can be quite limited, painful, and disabling (“shoulder syndrome”).
The most frequent permanent complication is numbness of the lateral neck and ear. This results from injury to the greater auricular nerve and sensory cervical rootlets. The area of numbness can reduce in size over time but can be permanent in some areas, especially the ear lobule. When level I is dissected, the marginal mandibular branch of the facial nerve is at risk. This branch can lie quite low in the neck as part of the investing fascia of the submandibular gland. Care to preserve this nerve branch even when defining the top of level II minimizes the risk, but weakness still results up to 23% of the time (37). Most weakness is temporary and results in an asymmetrical smile and short-term problems drinking from a glass until accommodation is made. Permanent marginal nerve weakness can be improved with facial plastic surgical procedures.
Uncommon injuries encountered during lateral neck dissection include: phrenic nerve injury, brachial plexus injury, cervical sympathetic trunk, and thoracic duct injury. The phrenic nerve lies on the anterior scalene muscle deep to the carotid sheath and should be identified and preserved. Similarly, the brachial plexus, which provides motor and sensory innervation to the upper extremity, enters the neck between the anterior and middle scalene muscles and is invested in the deep cervical fascia. It is usually unaffected by lateral neck dissection. Injury to the cervical sympathetic nerves can result in Horner's syndrome characterized by ipsilateral ptosis, miosis, and anhidrosis (38). Chyle fistula occurs when the thoracic duct in the left neck or the right neck cervical lymphatic duct is injured. Low level IV lymph nodes are typically involved in DTC and this area must be addressed to meticulously identify and avoid injuring or to ligate these lymphatic tributaries. These areas become especially problematic when bulky disease exists in low level IV or Vb requiring extensive dissection. Careful observation during a Valsalva maneuver or abdominal compression to elicit any leak in this area should be performed with ligation of this tissue when necessary. This complication can significantly increase utilization of inpatient resources and should be dealt with as best as possible at the time of neck dissection (39).
Rationale for evaluation and treatment of the lateral neck in DTC
Optimal management of patients with thyroid cancer requires removal of macroscopic clinical cervical lymph node metastases at the time of initial surgery and a comprehensive surveillance strategy to detect recurrent local and metastatic disease that may develop afterward. In accordance with ATA Thyroid cancer guidelines (14) recommendations 27a and 28, lateral neck dissection should be performed only as a therapeutic intervention for known disease. A prophylactic lateral neck dissection alone for thyroid cancer has not been proven effective to improve survival (40). There are significant risks to lateral neck dissection which have been outlined above, that render prophylactic lateral neck dissection unwarranted. The modalities and approach to establishing metastatic disease in the lateral neck follow.
Physical examination evaluation of the lateral neck for metastatic disease screens for visible or palpable lymph nodes. Medical records, including prior operative notes and pathology reports, and slides should be obtained for review in recurrent/persistent cancer cases. Imaging modalities, such as US (with or without FNAB) which allows for mapping of bilateral central and lateral neck compartments, iodine scans, CT, hybrid imaging modalities such as single photon emission computed tomography/CT and positron emission tomography/CT, technetium-99m methoxyisobutylisonitrile scintigraphy (MIBI scan), and magnetic resonance imaging can each be important in the assessment of the lateral neck. US performed by experienced hands is considered by most clinicians, and by the ATA, as the screening and surveillance imaging modality of choice for detection of lateral neck metastases (Table 2) (14) (ATA Thyroid cancer guidelines recommendations 21 and 22).
Timing of lateral neck dissection for well-DTC is less critical than is the central neck dissection for thyroid cancer or lateral neck dissection for squamous cell carcinoma. Proponents of routine prophylactic central neck dissection emphasize that an omission to perform it may result in a revision surgery being necessary that is more challenging due to entrance into the same operative field as the thyroidectomy with its resultant scar tissue (41). Negative neck US findings in DTC imply that the lateral neck be managed expectantly. As recommended by the ATA thyroid cancer guidelines (14), recommendation 48, surveillance imaging of the lateral neck should include ultrasonography. In cases when a lateral neck node is enlarged (>1.5 cm in levels I and IIa or >1.0 cm in levels IIb–Vb) or has sonographic features worrisome for disease, an US-guided fine-needle aspiration should be attempted to confirm disease including possibly testing the aspirate for Tg in a paucicellular specimen (1,3,31). Those nodes that have suspicious US characteristics and are not amenable to FNAB may be observed for growth with serial US at intervals recommended by the ATA before planning intervention.
If the node is growing on follow-up US and is still inaccessible for biopsy, an open biopsy may be undertaken to establish a diagnosis. An open biopsy of a lymph node should only be performed as an excisional biopsy with frozen section analysis to help determine if a lateral neck dissection is necessary at that time. Excisional biopsy alone without a plan to do a formal lateral neck dissection at the same time, if the frozen section is positive, is less desirable due to the complexity involved in reoperative lateral neck dissection surgery.
According to the ATA thyroid cancer guidelines (14), recommendation 48, nodes less than 5–8 mm, especially without worrisome features, might be observed rather than attempting an FNAB. The attendant risk(s) of lateral neck dissection should always be weighed against the possible benefit.
Lateral neck dissection performed for macroscopic DTC metastases should be the selective neck dissection of levels IIa, III, IV, and Vb. “Berry picking” is not recommended. Axial CT or MR may be useful in cases of extensive nodal disease to be vigilant of nodes that might be present in the retropharynx or upper mediastinum. Metastatic thyroid disease to levels I is infrequent; therefore, dissection of level I is usually not indicated (42).
Dissection of level I puts the marginal mandibular branch of the facial nerve at risk, which might result in a weak lower lip. Dissection above the accessory nerve (IIb) is generally not necessary unless there are suspicious lymph nodes at level IIb or in the high jugular region (IIa); this will help to minimize postoperative morbidity associated with “shoulder syndrome,” a condition of shoulder girdle weakness, stiffness, and chronic pain that can arise when CN XI function is impaired (43). Routine elective dissection of level Va may also be unnecessary when US evaluation shows no suspicious Va lesions. This further reduces the risk of injury to the accessory nerve. Lateral neck dissection is generally very well tolerated in most patients, may not require a drain and doesn't extend hospitalization for the majority of patients undergoing thyroid surgery.
Complications from all surgery for thyroid cancer, including lateral neck dissections, can be minimized when the operation is performed by high-volume thyroid surgeons (11,12,44,45). Thus, the surgeon's skill level, especially in performing lateral neck dissections for DTC, should always be considered when managing a patient that may require a lateral neck dissection.
Discussion
Proposals for future thyroid cancer management guidelines
As a result of our literature review, we propose that future guidelines for the management of DTC consider the following as they relate to disease or the possibility of disease in lateral neck: • Routine prophylactic lateral neck dissection for thyroid cancer has not been proven to improve survival. Thyroid cancer guidelines in the future may articulate this observation in the context of the comprehensive management of the thyroid cancer patient. • Current guidelines recommend that nodes less than 5–8 mm, especially without worrisome features, might be observed rather than attempting an FNA biopsy. Guideline recommendations in the future may address the consideration of biopsy of any highly suspicious lymph node in the lateral neck without regard to size if a positive FNA would change clinical management. • Unless findings are present to indicate dissection of compartments I or IIb, a routine dissection of these levels may not be necessary. Routine elective dissection of level Va may also be unnecessary when US evaluation shows no suspicious Va nodes, further reducing the risk of injury to the accessory nerve. Guidelines in the future may mention lateral neck levels requiring greatest attention during dissection. • In cases of lateral neck recurrence, a comprehensive neck dissection of levels IIa, III, IV, and Vb should be performed. In revision lateral neck dissection, focus upon levels of demonstrable recurrence may be appropriate. Guideline recommendations in the future may delete previous radiation alone as a contraindication to comprehensive lateral neck dissection since external beam radiotherapy is a rare adjuvant used for DTC and comprehensive neck dissection after radiation is feasible and routinely done for other disease processes.
Summary
The lateral neck lymph nodes are a significant consideration in the surgical management of patients with DTC. Metastases to these nodes must be considered in the evaluation of the newly diagnosed thyroid cancer patient, and for surveillance of the previously treated DTC patient. Initial evaluation of the new DTC patient with US, or other modalities when indicated, will help to identify lateral neck lymph nodes of concern (46). Positive imaging findings should be addressed using US guided FNAB to confirm lateral neck disease and a comprehensive neck dissection of levels IIa, III, IV, and Vb should be performed when indicated.
Footnotes
Acknowledgments
The authors wish to acknowledge Dr. Jennifer Shinn and Ms. Susan Steelman for their advice in preparing and executing the systematic literature search strategy for lateral neck metastases from thyroid cancer; Dr. Doug Evans for helpful suggestions to the article; Dr. Gerard M. Doherty, Cochair of the ATA Surgical Affairs Committee at the time of the creation of this subcommittee; Dr. Robert Udelsman for financial support of the artistic rendering of ![]() .
.
Author Disclosure Statement
No competing financial interests exist.