
Abstract
Background:
The role of prophylactic central lymph node dissection in papillary thyroid cancer (PTC) is controversial in patients who have no pre- or intraoperative evidence of nodal metastasis (clinically N0; cN0). The controversy relates to its unproven role in reducing recurrence rates while possibly increasing morbidity (permanent hypoparathyroidism and unintentional recurrent laryngeal nerve injury).
Methods and Results:
We examined the design and feasibility of a multi-institutional prospective randomized controlled trial of prophylactic central lymph node dissection in cN0 PTC. Assuming a 7-year study with 4 years of enrollment, 5 years of average follow-up, a recurrence rate of 10% after 7 years, a 25% relative reduction in the rate of the primary endpoint (newly identified structural disease; i.e., persistent, recurrent, or distant metastatic disease) with central lymph node dissection and an annual dropout rate of 3%, a total of 5840 patients would have to be included in the study to achieve at least 80% statistical power. Similarly, given the low rates of morbidity, several thousands of patients would need to be included to identify a significant difference in rates of permanent hypoparathyroidism and unintentional recurrent laryngeal nerve injury.
Conclusion:
Given the low rates of both newly identified structural disease and morbidity after surgery for cN0 PTC, prohibitively large sample sizes would be required for sufficient statistical power to demonstrate significant differences in outcomes. Thus, a prospective randomized controlled trial of prophylactic central lymph node dissection in cN0 PTC is not readily feasible.
Introduction
Surgery, radioactive iodine treatment, and thyroid hormone suppression are the mainstays of treatment for PTC (2). Due to the overall excellent outcomes in patients with PTC and the lack of prospective controlled trials, many of the current recommendations and guidelines for treatment of PTC are controversial, such as the extent of surgery, the role of radioactive iodine treatment in low-risk patients, and the extent and frequency of surveillance. With regard to the extent of surgery for PTC, the debate has shifted from thyroid lobectomy versus total thyroidectomy (3), to a debate regarding the initial management of cervical lymph nodes (4).
Lymph nodes typically involved in PTC are level VI (central compartment); levels II, III, and IV lymph nodes along the internal jugular vein corresponding to the upper, mid, and lower neck; and less frequently the level V (posterior triangle of the neck) lymph nodes. There is general agreement that formal lymph node dissection should be performed in the setting of imageable, biopsy-proven, or palpable nodal disease. The American Thyroid Association (ATA) Guidelines Taskforce published in 2006 a statement that “Routine central-compartment (level VI) neck dissection should be considered for patients with papillary thyroid carcinoma and suspected Hürthle cell carcinoma” (5). These recommendations caused significant controversy because of the ambiguity leading to vastly different interpretations amongst clinicians and the paucity of strong supporting data. Thus, the revised 2009 management guidelines state “Prophylactic central-compartment neck dissection (ipsilateral or bilateral) may be performed in patients with papillary thyroid carcinoma with clinically uninvolved central neck lymph nodes, especially for advanced primary tumors (T3 or T4; Grade C recommendation; expert opinion)” (2). The current guidelines also indicate that “these recommendations should be interpreted in the light of available surgical expertise,” acknowledging that this approach could be associated with increased morbidity especially among low-volume surgeons with less experience (2).
Although central lymph node dissection can be achieved with low morbidity in experienced hands, prophylactic dissection is, to date, of unproven benefit (4,6). The importance of regional lymph node disease in PTC may have been understated in the past partly due to the excellent overall prognosis associated with well-differentiated thyroid cancer and the observation that lymph node metastases did not influence survival rates (7). More recent large-scale population-based studies, mainly from Sweden, have shown that regional lymph node metastases among patients with thyroid cancer impact both local recurrence and cause-specific mortality (8,9). The association between lymph node metastasis and mortality seems to be preferentially identified in older patients (10,11), whereas such an association is less certain in their younger counterparts. Further complicating these analyses are potential prognostic differences including BRAF mutation status, and between microscopic (more likely to be clinically N0; cN0) and macroscopic lymph node metastases (less likely to be cN0), which are often not independently evaluated in retrospective cohort analyses. These competing considerations coupled with the drive to achieve low or undetectable thyroglobulin (Tg) levels in surveillance have refocused the debate on how best to manage regional nodal spread. The goals of treatment are no longer aimed at simply avoiding mortality. The secondary goals of achieving athyroglobulinemia, avoiding reoperative surgery, and simplifying follow-up have become the primary endpoints of therapy for many patients and treating physicians (12).
While possibly beneficial, prophylactic central lymph node dissection in patients with PTC could also lead to an increased rate of complications, including permanent hypoparathyroidism and recurrent laryngeal nerve injury (4,6). In an attempt to better define the risk–benefit ratio of prophylactic central lymph node dissection, several groups have considered embarking on prospective clinical trials to address this issue.
The inherent weakness of retrospective analyses limits the ability to extrapolate the findings to a broad population. Thus, in order to provide the basis for a prospective randomized controlled trial comparing prophylactic central node dissection versus no prophylactic central node dissection for cN0 PTC, the feasibility of such a study was analyzed by a multidisciplinary subcommittee of the ATA Surgical Affairs Committee. The data are extrapolated from current retrospective and meta-analysis studies and examined in terms of their implications on trial design and sample size.
Design
The study would be a multi-institutional, prospective, randomized, blinded (until total thyroidectomy has been performed) study (Table 1). All adult patients (≥18 years of age) with fine-needle aspiration (FNA) proven PTC and cN0 would be eligible for inclusion in the study. Informed consent would be obtained for all participants, and approval from the institutional review boards would be sought from participating institutions.
ATA, American Thyroid Association; FNA, fine-needle aspiration; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; TSH, thyrotropin.
As part of the initial assessment, demographic information (age, sex, history of radiation exposure, history of thyroid disease, past and current use of thyroid hormone treatment, known or suspected familial PTC) and the baseline characteristics outlined in Table 2 would be obtained.
Pathology report includes TNM stage, size, multifocality, margins, extrathyroidal extension number of lymph nodes removed, number of positive lymph nodes, presence of parathyroid tissue; POD, postoperative day; TSH, thyrotropin; PTH, parathyroid hormone; Tg, thyroglobulin; WBS, whole-body scan.
All measurements of Tg would include measurement of thyroglobulin antibodies.
All patients would need to have documentation of normal vocal cord mobility by preoperative laryngoscopy. A preoperative comprehensive neck ultrasound (US) of the thyroid and central and lateral neck compartments would be required as part of the routine preoperative planning for diagnosed PTC (13). US-guided FNA would be performed of the primary tumor and selected lymph nodes suspicious for metastatic disease in the central and/or lateral neck as part of the routine preoperative planning for PTC. The slides of patients with a cytological diagnosis of PTC at an outside hospital/institution would be reviewed by a cytopathologist at the participating institution. For cases in which there is disagreement between the findings at the outside institution and at the participating institution, the preoperative diagnosis would be based on the findings at the participating institution after review at a cytopathology consensus conference and/or referral to a third consulting cytopathologist. The use of molecular diagnostic tools (e.g., BRAF V600E mutational status) as an aid to the cytopathological diagnosis would not change the eligibility to participate in the study but would be tracked (e.g., a patient with indeterminate FNA results and BRAF mutation positivity, which indicates a preoperative diagnosis of PTC, would be eligible for enrollment).
Exclusion criteria
Only patients with pre- and intraoperatively diagnosed T (1 –4), cN0, cM0 PTC would be randomized (Fig. 1). We estimate that approximately 15% of patients with PTC would present with metastatic disease or be found to have lateral and/or central node metastasis during the initial evaluation (14 –20). These patients would be excluded from the study and would undergo standard management. Furthermore, we estimate that approximately 10% of patients with PTC would have intraoperative findings of central lymph node metastasis based on surgeon suspicion or intraoperative frozen section analysis (12,14 –20). Intraoperative frozen section analysis of lymph nodes would be obtained at the discretion of the operating surgeon. Patients with intraoperative positive central lymph node metastasis would be excluded from the study and undergo standard surgical management. Similarly, the rare cases with lateral lymph node metastasis diagnosed intraoperatively would not be included. In addition, we estimate that approximately 2% of patients with PTC would have concomitant primary hyperparathyroidism (21). These patients would be excluded from the study and undergo standard surgical management, since concomitant parathyroidectomy likely would affect the incidence of postoperative hypoparathyroidism. Other exclusion criteria would be previous central cervical operation and inability to give informed consent or meet follow-up requirements.
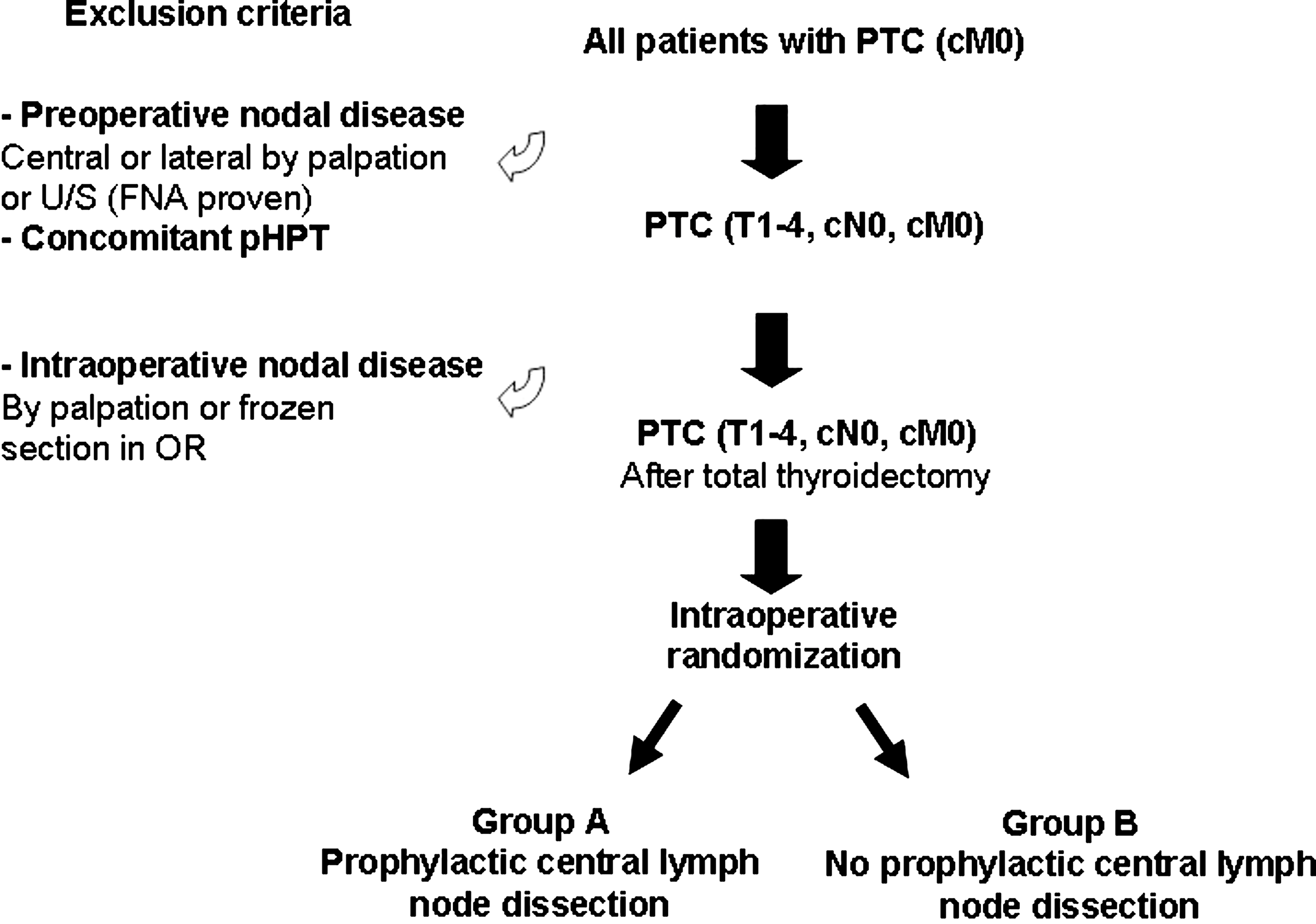
Study design. Prospective randomized controlled trial of prophylactic central node dissection for papillary thyroid carcinoma.
Intraoperative randomization process
After a total thyroidectomy and central neck evaluation by the surgeon and when no suspicious lymphadenopathy has been detected, patients would be randomized to either prophylactic central lymph node dissection or to no central lymph node dissection using equal allocation. The individual surgeon would be blinded to the randomization process until after total thyroidectomy. A web-based intraoperative randomization procedure would be developed, accessible to participating investigators.
Central neck dissection
In patients randomized to the treatment arm, an ipsilateral prophylactic central lymph node dissection would be performed for unilateral PTC. For clinically apparent bilateral PTC, a bilateral central lymph node dissection would be performed. The goal of a prophylactic central lymph node dissection is to remove all lymphatic tissue en bloc. The superior margin is at the level of the hyoid bone, the inferior margin is at the level of the brachiocephalic vessels, the lateral margin at the medial aspect of the common carotid artery, and the contralateral margin is past the midline of the trachea but not encompassing the contralateral inferior parathyroid gland (22). The dissection includes lymph nodes posterior (deep) to the recurrent laryngeal nerve. The number of removed lymph nodes would be recorded on the pathology report, thus mandating collaboration with the pathology departments at the participating institutions.
Parathyroid autotransplantation of one or more normal parathyroid glands would be performed at the discretion of the operating surgeon after frozen section confirmation.
Endpoints
The primary endpoint is newly identified structural disease,1 which may include persistent, recurrent, or distant metastatic disease defined as follows. 1) Persistent disease would be defined as cervical/superior mediastinal disease identified by an imaging study (US, radioisotope scan, computed tomography [CT], magnetic resonance imaging [MRI, positron emission tomography [PET], etc.), which would ideally be biopsy proven. Direct measurements of recombinant human thyrotropin (rhTSH)-stimulated (Thyrogen®, Genzyme, Cambridge, MA) pre–radioactive iodine treatment Tg levels (and antibodies) would aid in identifying persistent structural disease. Persistent disease is defined as being diagnosed≤6 months after total thyroidectomy and radioactive iodine treatment. 2) Recurrent/distant metastatic disease would be defined as occurring>6 months after total thyroidectomy and radioactive iodine treatment. a. Locoregional recurrence is defined as cervical/superior mediastinal disease identified by an imaging study (US, radioisotope scan, CT, MRI, PET, etc.) and ideally biopsy proven. Direct measurements of rhTSH-stimulated or unstimulated Tg levels (and antibodies) would aid in identifying recurrent structural disease. b. Distant metastatic disease is defined as disease identified outside of the neck by an imaging study (US, radioisotope scan, CT, MRI, PET, etc) or biopsy proven. Direct measurements of rhTSH-stimulated or unstimulated Tg levels (and antibodies) would aid in identifying distant metastatic disease.
The secondary endpoints are
1) Disease-specific mortality
2) Surgical mortality and morbidity
a. Operative mortality (defined as within 30 days postoperatively). General operative morbidity such as pulmonary embolism, pneumonia, cardiac complications, and deep venous thrombosis would be recorded.
b. Specific morbidities
i. Permanent hypoparathyroidism (transient hypoparathyroidism would be monitored but not considered a morbidity endpoint)
ii. Transient recurrent laryngeal nerve paresis (documented paresis that recovers within 6 months postoperatively)
iii. Permanent recurrent laryngeal nerve paresis (documented paresis that extends beyond 6 months postoperatively)
iv. Cervical neck hematoma
3) Other outcomes
a. Presence of undetectable suppressed Tg at 1-year follow-up.
b. Presence of undetectable stimulated Tg at 1-year follow-up.
c. Biochemical persistent disease defined based on elevated Tg levels is more likely to represent persistent disease rather than residual postoperative normal thyroid tissue. Persistent disease is defined as being diagnosed≤6 months after total thyroidectomy and radioactive iodine treatment.1
d. Biochemical recurrent disease which is defined based on elevated Tg levels in a patient with a previously undetectable Tg diagnosed>6 months after total thyroidectomy and radioactive iodine treatment.1
e. Requirement of cervical reoperation for thyroid cancer after initial total thyroidectomy and radioactive iodine treatment.
f. Requirement of radioactive iodine treatment for thyroid cancer after initial total thyroidectomy and radioactive iodine treatment.
g. Operative time
h. Duration of hospital stay
i. Number of frozen section analyses during surgery
j. Molecular marker status
k. Quality of life assessment
Radioactive iodine treatment
All patients would undergo postoperative radioactive iodine treatment. The dose would be standardized to approximately 50 mCi for all patients in both group A and B, independent of the underlying stage of PTC. A pretherapy whole-body iodine scan would not be obtained since it would not affect the decision to treat or the activity of radioactive iodine that is administered (2). The treatment would ideally be performed at the participating institutions, but treatment at another institution/hospital would not be in violation of the protocol. All patients would be on a pretherapy low-iodine diet and the treatment would be performed after rhTSH stimulation. Posttherapy whole-body iodine scanning would be performed in all patients in accordance with ATA guidelines (2).
Surveillance and identification of newly identified structural disease, and biochemical persistent or recurrent disease
In this protocol, all patients would undergo surveillance for recurrence as well as TSH suppression, in accordance with ATA guidelines (2). The diagnosis of newly identified structural disease and biochemical persistent or recurrent disease is as outlined in the endpoints section. The time points for surveillance are as outlined in Table 2.
Definition of surgical complications
Permanent hypoparathyroidism would be defined as requirement of therapeutic vitamin D and/or calcium replacement at 6 months or a fasting albumin-corrected serum calcium below 8.0 mg/dL. In this study, unintentional recurrent laryngeal nerve paresis would be defined as new vocal cord paralysis diagnosed within 6 months postoperatively in a patient who had normal vocal cord movement preoperatively. Permanent recurrent laryngeal nerve injury is by definition persistent beyond the 6-month postoperative period. Routine laryngoscopy would be performed in all patients at 6 months following thyroid surgery unless demonstrated to be normal prior to 6 months postoperatively. In addition, durations of surgery and hospital stay would be recorded. Postoperative cervical hematoma is defined as postsurgical bleeding requiring reoperative intervention.
Sample size estimation
Sample size was estimated for the primary outcome, newly identified structural disease (i.e., persistent, recurrent or distant metastatic disease), using the method of Lakatos (23,24) to approximate a discrete time hazard model. In the calculations we assumed a 7-year study with 4 years of recruitment and 5 years of average follow-up (minimum=3 years, maximum=7 years), a type I error of 5% (two-sided), 80% power, annual dropout rates from 1% to 5% in both treatment groups, and a range of reductions in the hazard rate with prophylactic central lymph node dissection compared with no central lymph node dissection (20%, 25%, 33%, and 40%). The estimates of the newly identified structural disease rate for the no prophylactic central lymph node dissection group were obtained from contemporary series and author experiences and were assumed to not be constant over the study period. The sample sizes were not inflated for interim monitoring for efficacy and futility, which would be approximately 4%–6%.
Sample sizes to detect differences in complication rates between the two treatment groups were estimated for binomial proportions assuming a Type I error of 5% (two-sided) and 80% power. These sample size determinations were made using PASS 2008 (NCSS, Kaysville, UT).
Results
Calculations of study sample size scenarios are presented in Table 3. For instance, assuming a 7-year study (4 years enrollment, 3 years minimum follow-up, 7 years maximum follow-up, 5 years average follow-up) with a newly identified structural disease cumulative event rate of 35% after 7 years and an annual dropout rate of 3%, a total of 1568 patients (355 primary outcome events) would be required to detect a 25% reduction in the hazard rate for the newly identified structural disease with central lymph node dissection with 80% power (Scenario 1, Table 3) at a type I error of 5% (two-sided). However, given that patients would all be cN0 (by preoperative US and intraoperative inspection), and thus represent low-risk PTC, the estimated newly identified structural disease rate would likely be significantly lower. PTC without pre- or intraoperative central neck nodal disease (i.e., cN0) has a low newly identified structural disease rate, even in the setting of histopathological presence of lymph node metastasis, with rates ranging from 2% to 9 % (12,14 –20). Thus, a more realistic sample size scenario is presented in Table 3 as Scenario 2. Given the same assumptions as for Scenario 1, but with a cumulative 10% newly identified structural disease rate after 7 years, a total of 5840 patients (377 primary outcome events) would be required to achieve satisfactory statistical power. The key determinates of the study sample size scenarios are the reduction in hazard rate and the newly identified structural disease cumulative event rate as depicted in Fig. 2.
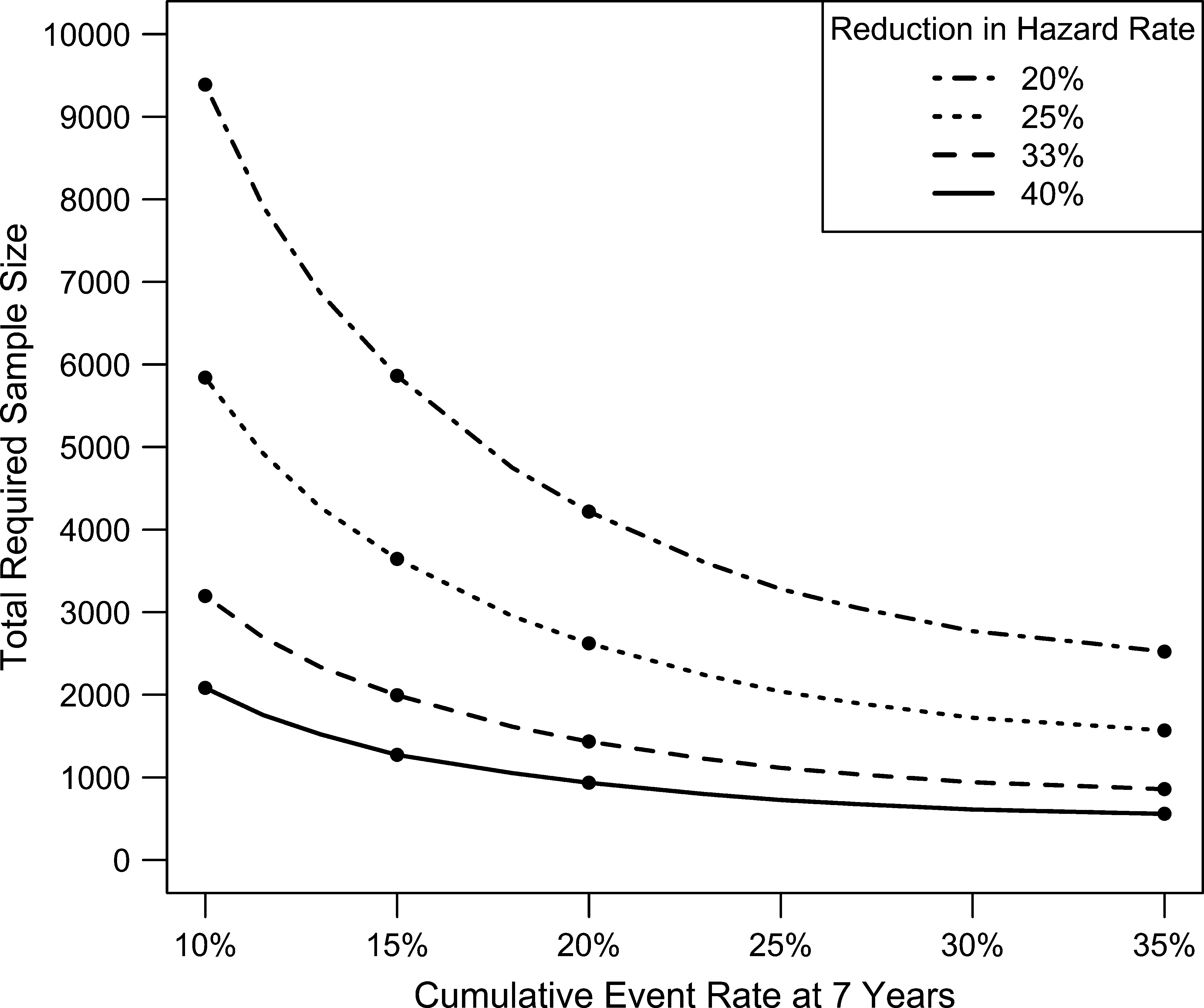
Total required sample size required in a prospective randomized controlled trial of prophylactic central lymph node dissection in cN0 PTC as a function of the cumulative event rate (newly identified structural disease) and reduction in hazard rate of 20%, 25%, 33%, and 40%. All scenarios assume a fixed annual drop-out rate of 3%.
Prophylactic central lymph node dissection compared with no prophylactic central lymph node dissection. For both scenarios, assuming a 7-year study (4 years enrollment, 3 years minimum follow-up, 7 years maximum follow-up, 5 years average follow-up); 5% Type I error (two-sided); 80% power.
Assuming the following newly identified structural disease (i.e., persistent, recurrent or distant metastatic disease) cumulative rates over the study period: Year 1=10%, Year 2=20%, Year 3=25%, Year 4=27.5%, Year 5=30%, Year 6=32.5%, Year 7=35%
Assuming the following newly identified structural disease (i.e., persistent, recurrent or distant metastatic disease) cumulative rates over the study period: Year 1=3%, Year 2=5%, Year 3=6%, Year 4=7%, Year 5=8%, Year 6=9%, Year 7=10%.
In addition, detecting an increased complication rate in patients undergoing central neck dissection would require large sample sizes as well. For example, assuming rates of permanent hypoparathyroidism of 5% and 2.5% in those with and without central neck dissection (6), respectively, would require approximately 2000 patients to detect this difference with 80% power. Similarly, to detect differences in rates of unintentional permanent recurrent laryngeal nerve injury of 2% versus 1% with 80% power would require more than 5000 total patients (6). In contrast, postoperative levels of serum calcium and intact parathyroid hormone at postoperative day 1, prior to starting postoperative prophylaxis with calcium carbonate and/or calcitriol, could be measured with more modest sample sizes (25). However, the significance of detecting differences in serum calcium and intact parathyroid hormone on postoperative day 1 is of limited clinical value.
Discussion
The use of routine prophylactic central lymph node dissection in PTC remains controversial. We have presented the design and feasibility of a randomized controlled trial to evaluate whether such an approach would lead to improved or impaired outcomes of PTC patients. The single most important factor in calculating sample size scenarios required to obtain sufficient statistical power is the event rate. It is well documented that PTC without pre- or intraoperative central neck nodal disease (i.e., cN0) has low recurrence rates, even in the setting of histopathological presence of lymph node metastasis, with rates ranging from 2% to 9 % (12,14 –20). Since event rates are low in these PTC patients, we demonstrate that thousands of patients would need to be included in the study and followed for many years. As a point of reference, approximately 3%–7% of all U.S. patients with cN0 PTC would need to be recruited into the study with long-term surveillance to achieve sufficient statistical power (1). Similarly, morbidity rates are low after surgery for PTC, and large sample sizes would be necessary to detect a statistically significant difference between the two groups. Permanent hypoparathyroidism occurs in approximately 1%–2% (range 0.8%–5.4%) of patients after total thyroidectomy (6). The reported range of permanent hypoparathyroidism after total thyroidectomy with prophylactic central lymph node dissection is 0%–14.3% (6). The rate of unintentional permanent recurrent laryngeal nerve injury after total thyroidectomy ranges between 0% and 5.5%, whereas the rate is 0%–5.7% after total thyroidectomy with central lymph node dissection (6). Similar to studies analyzing the rate of permanent hypoparathyroidism, these studies are retrospective and self-reported and laryngoscopy was used selectively. Thus, the true incidence of nerve injury is largely unknown.
The success of a multicenter prospective randomized controlled trial of prophylactic central lymph node dissection in cN0 PTC would depend largely on as much standardization as possible of the diagnosis, treatment, and surveillance of the study subjects. We realize that the proposed protocol is not uncontroversial, for instance, the attempt to standardize the operative management and postoperative radioactive iodine treatment independent of the stage of PTC at final pathology. This could potentially hamper the enthusiasm for participation of treating physicians and impede study subject enrollment.
The current investigation did not specifically address the costs of this hypothetical study. However, a large simple trial over 7 years (4 years enrollment, 3 years minimum follow-up, 7 years maximum follow-up, and 5 years average follow-up) with enrollment of 5840 patients would be expensive. Approximately 30 centers would be required to enroll 50 subjects per year over 4 years to achieve the target sample size. At a minimum, one full-time study coordinator per study site would be needed to enroll and follow 200 patients for study outcomes for an average of 5 years at a total cost of approximately $15 million over a 7-year study period. In addition, funding would be required for startup and closeout costs, a national study coordinator, statistical and data coordinating center, site monitoring, investigator meetings, data and safety monitoring board, etc. No funding would be requested for participating patients, study surgeons, endocrinologists, radiologists, pathologists, and nuclear medicine physician. No funds would be requested for the medical care of the subjects as it would adhere to recommended state-of-the-art practice. We estimate that the total cost of the study would be approximately $20 million or $3425 per enrolled study subject.
In summary, our analysis of a hypothetical randomized controlled trial to evaluate the role of routine prophylactic central lymph node dissection for cN0 PTC indicates that given the low rates of newly identified structural disease and morbidity, prohibitively large samples sizes would be required to detect statistically and clinically relevant differences between the groups. This means that no single institution could perform this study alone. Therefore, a multi-institutional collaborative trial would need to be done. This would introduce significant variation in surgical techniques, as well as local institutional variability in inclusion and follow-up of patients. In addition, a large number of surgeons, endocrinologists, radiologists, nuclear medicine physicians, and pathologists would need to participate. These issues would introduce additional variables and challenges. We thus conclude that a randomized controlled trial of prophylactic central lymph node dissection in PTC is not readily feasible. Studies reporting the absence of an outcome difference based on small sample sizes may have inadequate statistical power from which to draw such a conclusion.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
1
It is anticipated that occasionally the diagnosis of newly identified structural disease and biochemical persistent or recurrent disease may be debatable in individual cases (e.g., elevated Tg without structural disease on imaging or radioisotope scan uptake that is not biopsy proven). Such cases would be reviewed by a multidisciplinary committee of investigators to determine the diagnosis of newly identified structural disease or biochemical persistent and recurrent disease.