
Abstract
Background:
Propylthiouracil (PTU) therapy is associated with a variety of adverse reactions, among the most rare being interstitial pneumonia. To date, this has been reported in four Asian patients with autoimmune hyperthyroidism. Here we describe a Caucasian woman who developed a bronchiolitis obliterans organizing pneumonia (BOOP)-like interstitial pneumonia after PTU administration for amiodarone-induced thyrotoxicosis.
Patient Findings:
The patient was a 68-year-old woman who had been treated with amiodarone for chronic atrial fibrillation starting in May 2004. She had been a heavy smoker with a history of hypertension but no dust exposures. In October 2006, amiodarone was stopped after she developed thyrotoxicosis. In January 2007 serum thyroid-stimulating hormone (TSH) was 0.01 mIU/L (0.35–4.94) and free T4 was 17.5 pg/mL (7 to 15). She was initially started on methimazole and then changed to PTU after she developed pruritus. She developed severe dyspnea 9 months after starting PTU. At the time she was also taking warfarin, enalapril, and sotalol. Chest X-ray showed diffuse interstitial peripheral opacities and transbronchial lung biopsy revealed subacute lung injury with organizing pneumonia with hyperplasia of the alveolar type 2 pneumocytes, and characteristics of BOOP-like interstitial pneumonia. Signs and symptoms progressively improved after PTU discontinuation as confirmed at X-ray and computed tomography (CT) scan of the chest and by respiratory function tests. She has been recurrence free for 4 years after stopping PTU.
Summary:
This woman of Caucasian ancestral origin developed BOOP-like interstitial pneumonia after PTU treatment for apparent amiodarone-induced thyrotoxicosis, with resolution of her lung disease after stopping PTU. Tests for TSH receptor antibodies, thyroid peroxidase antibodies, and antinuclear cytoplasmic autoantibody were negative. Thyroid ultrasound was consistent with thyroiditis without nodules.
Conclusions:
PTU-associated interstitial pneumonia is not limited to patients of Asian origin or those with autoimmune thyroid disease. PTU must be withdrawn in the presence of respiratory symptoms and documented interstitial pneumonia. X-ray films, CT-scan, respiratory function tests, and lung biopsy are needed to diagnose PTU-induced interstitial pneumonia with certainty and to monitor the evolution of the disease after PTU discontinuation.
Introduction
Propylthiouracil (PTU) is a thionamide that inhibits thyroid hormone synthesis by interfering with thyroid peroxidase–mediated iodination of tyrosine residues in thyroglobulin and it is effective in the treatment of hyperthyroidism (1,2).
Rarely, PTU may lead to adverse reactions (7,8) such as unexplained fever, agranulocytosis, neutropenia, aplastic anemia (9), hypoprothrombinemia, exfoliative dermatitis, nephritis, hepatitis (10), or antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (11,12). Pulmonary complications include adult respiratory distress–like syndrome, cavitary lung lesions, pleural effusions, and interstitial pneumonia (13 –15). Until now four cases of interstitial pneumonia due to PTU have been reported, these occurred only in Asian subjects (14 –16), and all had Graves' disease (Table 1). Here we report the first case in a Caucasian woman, and the first case in a patient who was given PTU for thyrotoxicosis that was not due to Graves' disease. She developed interstitial pneumonia after 9 months of treatment with PTU administered for hyperthyroidism secondary to amiodarone treatment.
n.a, not available; IP, interstitial pneumonia; NISP, nonspecific interstitial pneumonia; BOOP, bronchiolitis obliterans with organizing pneumonia.
Patient
A 68-year-old woman was treated with amiodarone for chronic atrial fibrillation from May 2004 to October 2006, when it was stopped because of the onset of hyperthyroidism. She was referred to our Unit after few months in January 2007. Serum thyroid-stimulating hormone (TSH) was 0.01 μIU/mL (normal range, nr=0.35–4.94), with increased free thyroxine (fT4) levels of 17.50 pg/mL (nr=7–15) and a normal free triiodothyronine (fT3) 2.3 pg/mL (nr=1.7–3.7). Both TSH-receptor and antiperoxidase antibodies were within the normal range. Thyroid ultrasound showed a morphological aspect of thyroiditis without nodules. These findings were suggestive for amiodarone-induced thyrotoxicosis. Thus, the patient was asked to start therapy with methimazole (20 mg daily). After 2 months of treatment, however, she complained itching; thus, methimazole was interrupted and replaced by PTU at the daily dose of 150 mg, the latter was effective in restoring normal TSH values.
Suddenly, in December 2007, 9 months after starting PTU therapy, the patient was admitted to the hospital because of severe dyspnea. Her medical history included a past of heavy smoking (20 cigarettes daily for 20 years), which she stopped in 2003; a history of hypertensive heart disease; and the absence of exposure to specific dusts. At that time, her therapy also included warfarin, enalapril, and sotalol.
X-ray of the chest showed diffuse interstitial peripheral opacities (Fig. 1b). These were not present in a previous X-ray film performed one year before (Fig. 1a). The chest X-ray findings were confirmed by chest CT-scan (Fig. 2a). Respiratory function tests documented increased residual volume, 2.35 L (121.7% of predicted value), reduced forced expiratory flows—FEV1 1.82 L (95.9% of predicted value), FVC of 2.5 L (108% of predicted value), and FEV1/FVC of 73%—and a decreased single breath carbon monoxide diffusing capacity (2.37 mmoL/min/kPa, 35% of predicted value).
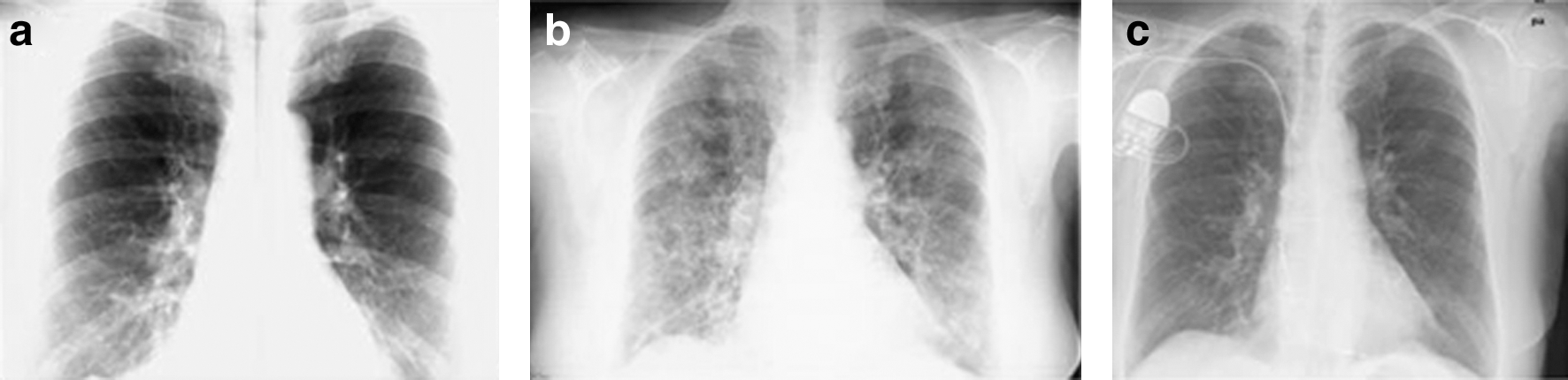
X-ray film of the chest performed one year before propylthiouracil (PTU) treatment showing a normal pattern
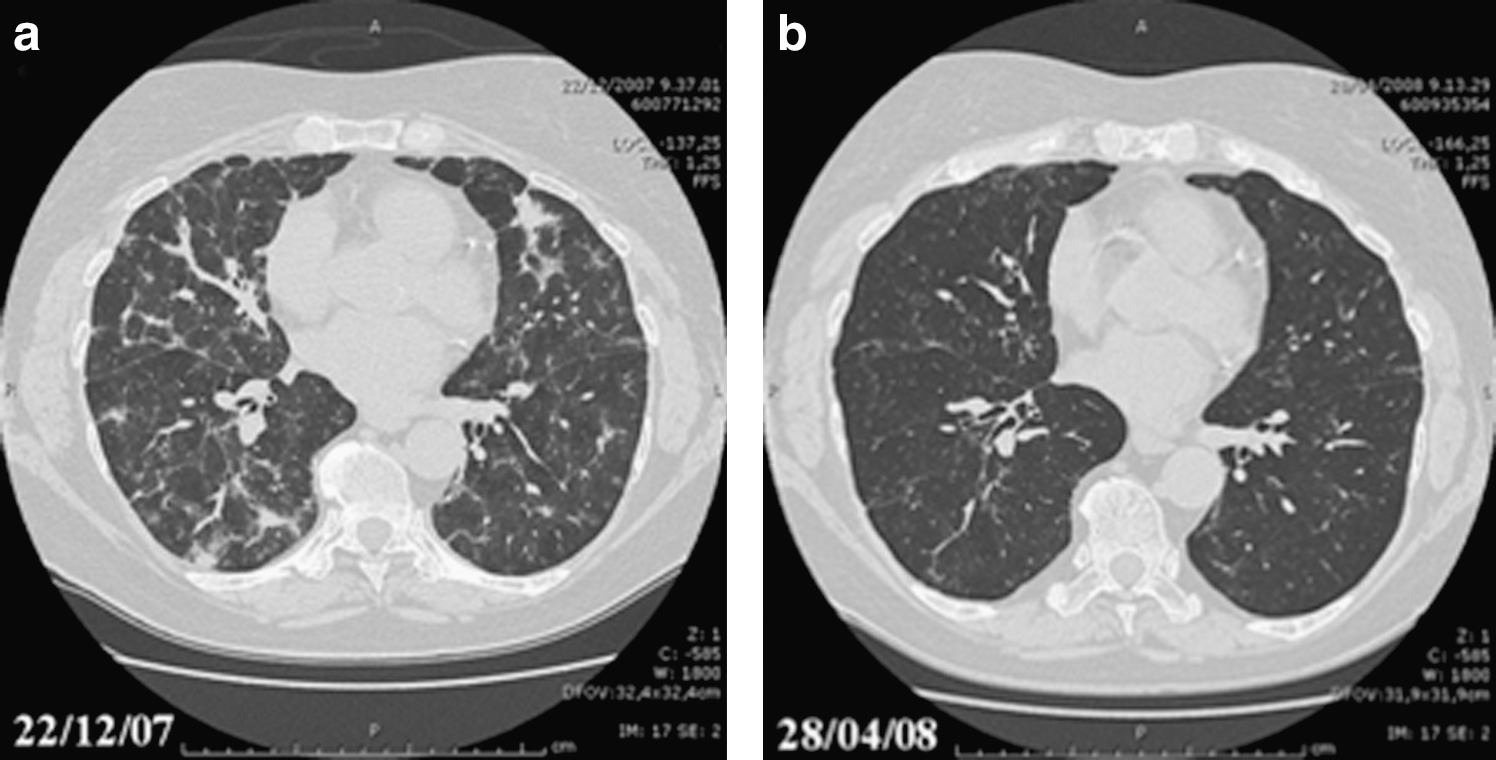
CT-scan of the chest showing interstitial pneumonia performed at the time of hospital admission
To establish the diagnosis a transbronchial lung biopsy was performed, the latter revealed interstitial pneumonitis with a subacute pattern (Fig. 3) suggesting a bronchiolitis obliterans with organizing pneumonia (BOOP)-like aspect. With this finding PTU administration was considered to be likely to have caused the pulmonary condition. The patient underwent also rheumatologic evaluation with capillaroscopy examination that excluded a “scleroderma pattern.” Serological markers such as antinuclear antibody (ANA) and antinuclear cytoplasmic autoantibody (ANCA) were negative, thus speaking against a rheumatological problem (i.e., vasculitis) as a cause for the interstitial pneumonia.
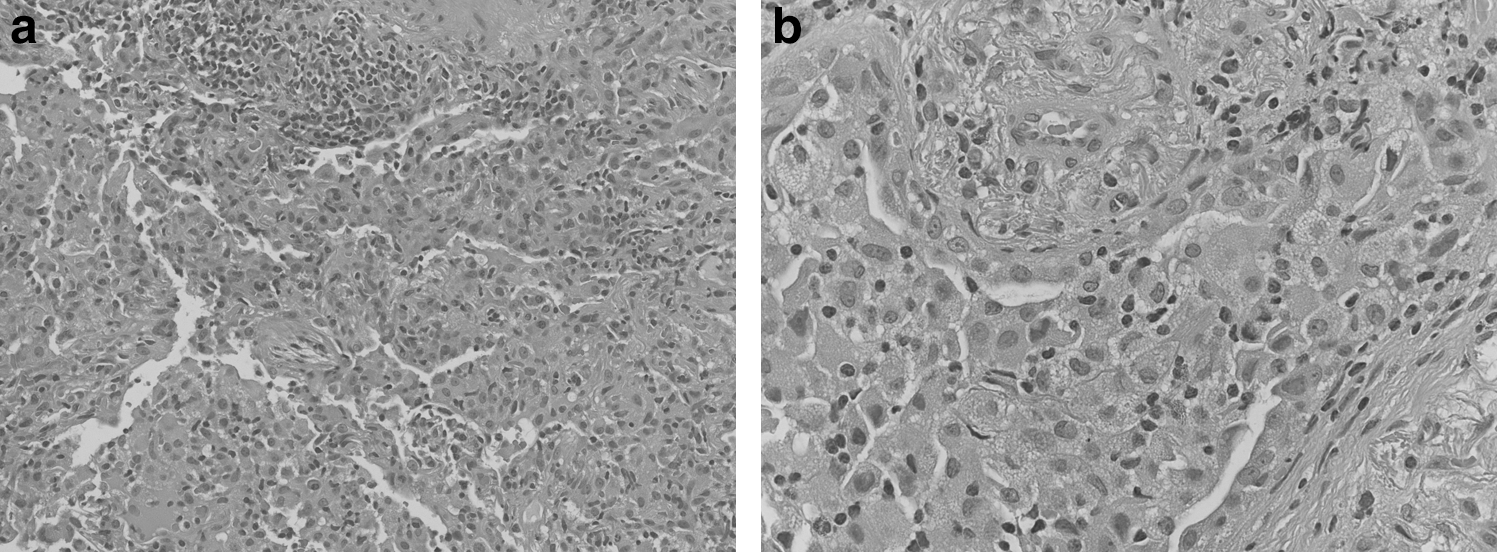
Transbronchial lung biopsy specimens revealed subacute lung injury with organizing pneumonia characterized by hyperplasia of the alveolar type 2 pneumocytes, aggregates of foamy histiocytes into the alveoli, and a moderate chronic inflammatory infiltrate with scattered eosinophils, characteristics of drug-related BOOP-like interstitial pneumonia [hematoxylin-eosin stain; original magnification
Considering the lung histology and the absence of other likely causes of the lung disease, PTU was stopped and the patient was treated with prednisone 37.5 mg (0.5 mg/kg) daily for 5 weeks. There was significant improvement of respiratory symptoms 4 weeks after the start of prednisone treatment and PTU withdrawal. In addition, a restoration to the normal aspects of the lungs was found in the chest X-ray (Fig. 1c) and subsequently confirmed also by chest CT-scan, the latter showing a dramatic improvement of pulmonary morphology—with an almost complete resume of ventilation in parenchyma regions, and only residual reticular thickening of inter- and intralobular interstitium (Fig. 2b). Respiratory function tests documented an improvement of spirometric parameters, especially the forced expiratory flows—FEV1 1.99 L (104.5% of predicted value), and the single breath carbon monoxide diffusing capacity (3.33 mmoL/min/kPa, 49.1% of predicted value).
Due to adverse reactions to both methimazole and PTU, and considering the risk for relapse of thyrotoxicosis, radioactive iodine therapy was considered to be the best treatment for the patient's thyrotoxicosis (2). She was treated with 131-iodine (15 mCi–555 MBq). Thyroid function normalized with normal TSH values (1.02 μUI/mL) and normal fT3 and fT4 levels (3.5 pg/mL and 14.1 pg/mL, respectively) being obtained 2 weeks after radioactive iodine treatment.
The patient was clinically stable, despite the persistence of episodes of tachycardia and rare supraventricular extrasystoles occurring about three times weekly. She has not experienced a recurrence of her lung disease in the 4 years after PTU treatment was discontinued.
This case report was written according to ethical standards. The suspected adverse event was reported to the local pharmacovigilance group and the patient gave her written consent for this case report including publication of images.
Discussion
This is the first case of a BOOP-like interstitial pneumonia related to PTU administration in a Caucasian woman treated for amiodarone-induced thyrotoxicosis. BOOP-like interstitial pneumonia in this patient can be attributed to PTU because of (i) a documented normal chest X-ray before PTU treatment but 18 months after amiodarone discontinuation (Fig. 1a); (ii) cytological findings suggestive for drug-induced toxicity (Fig. 3); (iii) the improvement of the lung disease after discontinuing PTU in terms of symptoms, lung morphology based on radiological examinations, and of lung function (Figs. 1c, 2b); and (4) the absence of recurrence of her respiratory disease during 4 years of follow-up after PTU withdrawal.
The patient was diagnosed with PTU-induced interstitial pneumonia after excluding a history of exposure to specific dusts, rheumatic and/or immunologic diseases that could cause pulmonary infiltrate, and pulmonary toxicity induced by amiodarone, which can also cause asymptomatic lungs fibrosis, but with a different clinical-histological pattern (17,18). The histological pattern of lung fibrosis induced by amiodarone usually consists of diffuse interstitial and patchy alveolar disease, which predominantly involves upper lobes (17). On the other hand, PTU can induce several histological patterns including bronchiolitis obliterans with organizing pneumonia (BOOP), as we found in our patient. However, we cannot exclude a role of amiodarone as a predisposing factor in the onset of lung toxicity in this patient.
To our knowledge, only four cases of interstitial pneumonia due to PTU have been previously described (14 –16). Two of them were affected by interstitial pneumonia (15), one with nonspecific interstitial pneumonia (16), and the fourth had no histological diagnosis (14). Thus, our patient is the first case with documented BOOP-like interstitial pneumonia (Table 1).
As previous cases in the literature were all of Asian (14 –16) ethnicity, the present report suggests that Asian ethnicity is not a prerequisite for PTU-induced interstitial pneumonia and that this adverse reaction also occurs in Caucasian patients.
Different from what was previously suggested (16), thyroid autoimmunity seems not to be relevant for the induction of this adverse effect to PTU, since our patient had amiodarone-induced thyrotoxicosis without evidence of Graves' disease or other autoimmune thyroid diseases. This differed (Table 1) from the prior reports (14,15). As was the case in our patient, three of the previously described subjects were treated with PTU after having an allergic reaction to methimazole (Table 1), characterized by hepatotoxicity, granulocytopenia, and drug eruption (14,15). Thus, there have been several reports that an adverse reaction to one antithyroid drug could be followed by a similar or even more severe reaction to a second antithyroid drug (15). However, the case in which interstitial pneumonia was not preceded by methimazole treatment (16) suggests that this reaction could be independent of the previous use of other antithyroid drugs.
All the patients had dyspnea after a variable time and dose of exposure to PTU (from “several” to 120 months, from 100 to 300 mg daily) (Table 1). The present case, together with the review of the literature (14 –16), suggests that both the exposure to cigarette smoking and gender are not associated with PTU-induced interstitial pneumonia (Table 1). However, all patients were older than 50 years, suggesting that PTU-induced interstitial pneumonia might be more likely to occur in middle-aged and elderly people (Table 1) (14 –16).
Some authors have suggested a possible relationship between PTU administration and autoimmunity (14), especially for the induction of ANCA positivity, as a result of immunological abnormalities arising mostly as a complication of an autoimmune condition (10 –12,19). The description of two cases of PTU-induced interstitial pneumonia with negative ANCA, our case and that of Lee et al. (16) (Table 1), speaks against a major role of such immunological reactions in the development of PTU-induced interstitial pneumonia. Thus, the present case and others do not provide definite information about the underlying mechanisms involved into the PTU-induced interstitial pneumonia.
Published case reports of adverse drug reactions remain of limited value, especially when no further confirmatory report is available (20). The description of new cases, such as the present case report, is, however, of crucial importance for confirming a previously described drug reaction, especially when more detailed research is provided (21). At present, however, a transparent policy aimed at incorporating available information from case reports into published drug information is lacking (20). Thus, adding new reports on drug reactions may help physicians in interpreting their patients' clinical features.
In summary, this is the first report of interstitial pneumonia in a patient with amiodarone-induced thyrotoxicosis treated with PTU. PTU-induced interstitial pneumonia may occur independent of ethnicity, sex, PTU dose or time of exposure, underlying thyroid disease, ANCA/ANA positivity, pretreatment with methimazole, and cigarette smoking exposure. PTU must be withdrawn in the presence of respiratory symptoms and documented interstitial pneumonia and its use should be considered with caution in patients with previous or current treatment with amiodarone. X-ray films, CT-scan respiratory function tests, and lung biopsy are needed (14,15) to diagnose PTU-induced interstitial pneumonia with certainty and to monitor the evolution of the disease after PTU discontinuation.
Footnotes
Acknowledgments
The authors are grateful to Barozzi Giuseppe, M.D., Unit of Emergency Medicine, Hospital of Pavullo nel Frignano, Modena, Italy, for helpful clinical management and for his contribution in interpreting radiological data and respiratory function tests.
We thank Claudia Polastri, M.D., for her help in collecting reference data and for technical support for figures.
Author Disclosure Statement
The authors declare that no competing financial interests exist.