
Abstract
Background:
Thyroid storm (TS) is a rare life-threatening condition that is characterized by fever and altered mental status precipitated by endogenous or exogenous critical events, illness/injury, acute iodine load, and thyroid or non thyroid surgery. A large number of thyroid extracts are available and extensively used, even though they are not recommended clinically in hypothyroid or euthyroid patients. Consumption of such products can be dangerous and result in life-threatening TS. Here, we report a case of TS caused by inadvertent intake of very high dosages of triiodothyronine (T3) and thyroxine (T4) in compounded thyroid extracts. Plasmapheresis may be considered an option for the management of exogenous TS.
Patient Findings:
A 62-year-old woman with no significant past medical history presented with severe myalgia, fever, tachycardia, and blood pressure of 170/80 mmHg, which precipitated to an altered mental state within 24 hours. Neurological examination did not reveal any focal deficit or any signs of meningeal irritation. Further investigation revealed that she had been taking thyroid supplements. The patient had accidentally been supplied with a batch of thyroid extract pills that had an inadvertently high content of T4. Her free T3 (FT3) and free T4 (FT4) levels were found to be very high beyond the laboratory readable range (FT3>30 pg/mL; FT4>6.06 ng/dL; thyrotropin [TSH]=0.07 IU/mL).
Summary:
Three days post commencement of standard conservative management of TS, the patient developed posterior reversible encephalopathy syndrome, resulting in a seizure. She remained unresponsive and in a poor mental state. The confirmed exogenous etiology for TS led to a decision to conduct plasmapheresis. Plasmapheresis conducted for two consecutive days proved successful as a therapeutic measure for TS and improved her thyroid profile as well as her mental state.
Conclusions:
The inappropriate use of thyroid extracts in euthyroid and hypothyroid patients can result in life-threatening TS. Plasmapheresis is probably a life-saving treatment in patients who are exposed to amounts of thyroid hormone far in excess of that usually produced by the thyroid gland.
Introduction
A large number of thyroid extracts are available and extensively used at wellness centers (5,6) and also by some physicians and endocrinologists, even though they are not recommended clinically in hypothyroid or euthyroid patients. Consumption of such products can be dangerous and result in life-threatening situations. Here, we report a case of TS caused by inadvertent intake of very high dosages of triiodothyronine (T3) and T4 as thyroid extracts. Plasmapheresis may be considered an option for the management of exogenous TS. We are not in favor of the practice of thyroid extract use in euthyroid and hypothyroid patients.
Patient
A 62-year-old healthy woman presented to us with severe myalgia and fever for the past 7 days. She also reported a few episodes of nausea and diarrhea 3–4 days before presentation. Her past medical history was devoid of any major illness. Physical examination revealed that the patient was febrile with a temperature of 101°F. She had a regular pulse of 130 beats/min and a blood pressure (BP) of 170/80 mmHg. There was no icterus, lymphadenopathy, rash, petechiae, hemorrhages, clubbing, or pedal edema. The cardiovascular system, respiratory, and abdominal findings were normal. A provisional diagnosis of fever with viral etiology was considered, and investigations were initiated. Peripheral smear examination was done to rule out malaria, and immunoglobulin M immunoassay was done to rule out dengue. The complete blood count, electrolytes, blood urea nitrogen, liver function, and echocardiography were normal. There was no evidence of any local infection.
Within 24 hours of her admission, she had episodes of vomiting and became restless and delirious. Neurological examination did not reveal any focal neurological deficit or any signs of meningeal irritation. The patient was shifted to the intensive care unit, and a provisional diagnosis of meningoencephalitis was made. Next, antibiotics and supportive treatment were initiated. Lumbar puncture revealed normal results. The cerebrospinal fluid was negative for Cryptococcus, fungus, bacteria, and herpes simplex virus (I and II). All blood samples were culture negative and had normal electrolyte levels. Reports of computed tomography and magnetic resonance imaging (MRI) scans of the brain were normal.
The delirium persisted till the next day with fever and tachycardia with conservative management. On obtaining further history from the patient's daughter, it was discovered that the patient had been taking thyroid extracts prescribed from a wellness center, although her thyrotropin (TSH) had always been within the normal range. This led to a suspicion of thyrotoxicosis. After persistent discussions with the physician at the wellness center, it was found that the patient had accidentally been supplied with a batch of thyroid extract pills which had an inadvertently high content of T3 and T4 and which she had been consuming for 6 days before her hospitalization. The physician later confirmed that due to an error by the compounding pharmacist, her total T3 and T4 ingestion would have been 720,000 and 30,000 μg, respectively.
Based on this information, the patient's free T3 (FT3) and free T4 (FT4) levels were tested and found to be elevated beyond the laboratory readable range. Her thyroid profile showed FT3>30 pg/mL (reference range 1.5–4.1 pg/mL), FT4>6.06 ng/dL (reference range 0.8–1.9 ng/dL), and TSH=0.07 IU/mL (reference range 0.4–4.0 IU/mL). However, her previous thyroid profile had been normal (6 months back: TSH 3.0 IU/mL and one month back: TSH 0.67 IU/mL). A score of 45 points as per Burch and Wartofsky scoring system (1) confirmed our diagnosis of TS with exogenous etiology. Retrospectively, on studying the recently published diagnostic criteria proposed by Akamizu et al., we found that she had satisfied the first combination of the criteria for what was referred to as TS1 (TS grade 1) (2). An immediate treatment with propranolol, intravenous steroid, neomercazole, and Lugol's iodine was initiated, which reduced the patient's restlessness and agitation but the mental state remained variable. Cholestyramine was considered but not administered due to her symptoms of nausea and vomiting. Propranolol dosage was titrated based on her heart rate. On further evaluation and discussion, neomercazole and iodine were discontinued, as TS was due to an exogenous cause. After 48 hours of treatment, the patient's FT3 levels were reduced to 26.6 pg/mL. However, her FT4 levels remained beyond the laboratory readable range.
Three days after the diagnosis and standard management of TS, the patient suffered a seizure, and an MRI brain scan confirmed the presence of posterior reversible encephalopathy syndrome (PRES), which is characterized by headache, seizures, encephalopathy, and visual disturbances, as well as radiologic findings of focal reversible vasogenic edema. She remained unresponsive, in a state of delirium, with a BP of 170/80 mmHg and a regular pulse of 120–130 beats/min. An ultrasound of thyroid revealed normal symmetry of bilateral lobes and isthmus with no focal lesions. Her FT4 levels continued to be elevated beyond the laboratory's upper limit, and her BP was fluctuating. In our opinion, the high amount of T3 as compared with T4 was most likely the precipitating cause of TS. Due to the long half life of T4, conventional methods of thyrotoxicosis management failed to reduce the elevated serum hormone levels and worsened the clinical condition of the patient. The confirmed exogenous etiology for TS led to a decision to conduct plasmapheresis.
Plasmapheresisis is well respected for rapid and efficient removal of large molecules such as hormones bound to serum proteins from blood and has been used as an alternative therapeutic option in the treatment of TS (7). In our case, the patient underwent plasmapheresis for two consecutive days. During the procedure, she was kept on a ventilator, and her mean BP remained fairly stable at 135 mmHg. Two hours after plasmapheresis, her pulse was 110 beats/min, BP was fairly constant at 140/70 mmHg, the FT3 was 8.77 pg/mL, and, most importantly, the FT4, at 4.58 ng/dL, was readable for the first time in 10 days. As shown in Figure 1, 2 hours post plasmapheresis on the second day, this treatment had apparently significantly improved the FT3 (6.18 pg/mL) and FT4 levels (4.94 ng/dL) and the serum TSH (0.02 IU/mL). After stabilization of her BP and heart rate and improvement of her mental state, plasmapheresis was discontinued. She gradually improved during her subsequent 2 week hospital stay and was discharged without persistent complaints. A follow-up MRI scan showed the absence of PRES. She was euthyroid when evaluated 6 months after her discharge.
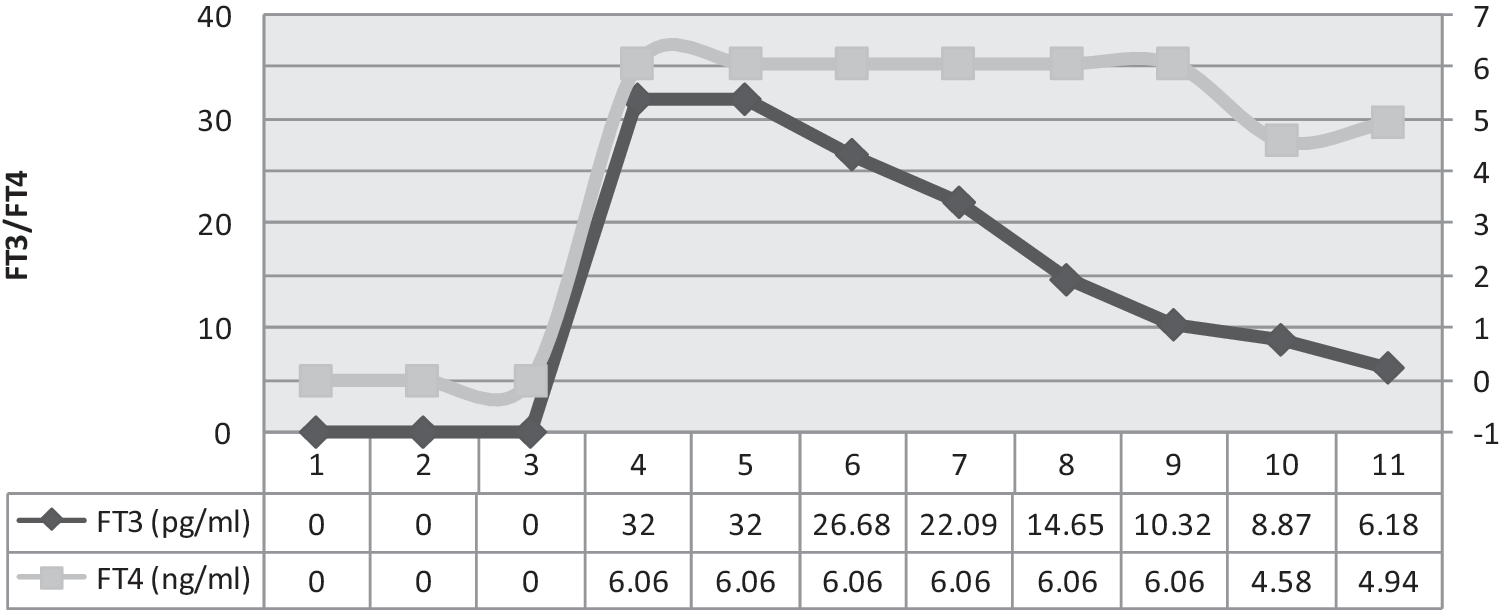
The actual level of FT3 was beyond the readable range of the machine. In the graph just depicted, FT3 on days 4 and 5 is depicted as 32 pg/mL, which is the highest readable value, while the actual value of FT3 was higher than 32 pg/mL. The actual level of FT4 was beyond the readable range of the machine. In the graph just depicted, FT4 on days 4–9 is depicted as 6.06 ng/dL, which is the highest readable value, while the actual value of FT4 was higher than 6.06 ng/dL. Arrow marks the day plasmapheresis was done. FT3, free triiodothyronine; FT4, thyroxine.
Discussion
This was a unique case in which TS, caused by excessive ingestion of erroneously compounded thyroid hormone supplement, was successfully treated by plasmapheresis. TS, a life-threatening condition of thyrotoxicosis, is usually caused by Graves' disease, often with a precipitating event (intercurrent illness, trauma, infection, or an acute iodine load) (8). This rare condition with high mortality requires a multi-disciplinary therapeutic approach in the intensive care setting. Historically, diagnosis is on clinical evaluation based on Burch and Wartofsky scoring. Recently, members of the Japan Thyroid Association proposed new diagnostic criteria that assigned two grades based on signs and symptoms (2). Along with elevated levels of T3 and T4, diagnostic criteria for TS should include either cardiovascular symptoms of tachycardia disproportionate to the fever or gastrointestinal dysfunction in the form of nausea, diarrhea, and neurological symptoms of agitation, delirium, psychosis, stupor, or coma. In this case, the patient fulfilled their criteria for TS1 (2).
Adulterated dietary supplements of T4 leading to a medical emergency were reported 25 years ago in Spain (9) and 4 years ago in Paris (5). One study on the overdose of herbal pills for weight loss by Ohye et al. reports 1 μg of T3 and 3–4 μg of T4 per tablet (6). In our patient, a compounding error occurred, and, hence, the dose ingested could be reliably estimated. In other reported cases of T4 overdose, the amount of ingested T3 ranged from 3000 to 9500 μg (3,4) as compared with 720,000 μg of T3 estimated in our case. The estimation of ingested amounts of T4 has been rarely reported.
For treating TS, gastric decontamination has been recommended (10,11) along with the use of betablockers, digoxin, or hydrocortisone to counteract the action of thyroid hormones or reduce the conversion of T4 to T3. In our case, the patient had inadvertently ingested extremely high quantities of T3 and T4 supplements for 6 days before her admission; therefore, gastronomical decontamination and cholestyramine may not have been beneficial. Conventional medical management of TS also failed to improve her exogenous thyrotoxic state. Therapy was, therefore, targeted at reducing serum hormone levels, and plasmapheresis was considered the most appropriate approach.
A systematic literature search in PubMed® with keywords TS, thyrotoxicosis, and plasmapheresis revealed 32 articles. All, except one report (12), recommended plasmapheresis as being beneficial. Plasmapheresis or therapeutic plasma exchange (PE), an extracorporeal blood purification technique designed for the rapid removal of large-molecular-weight substances from the plasma, is a well-established, effective therapeutic measure in various immunological and non-immunological diseases. It has been used in preoperative and post-operative management of severely hyperthyroid patients with contraindications to antithyroid drugs (13). It has also been used for the management of TS, predominantly in patients with Graves' disease with ophthalmopathy (14,15) or agranulocytosis (16,17) and in selected patients with toxic multinodular goiter (18). In a recent case of TS, plasmapheresis was done post surgery, where sleeve pneumonectomy was the precipitating event and the patient had not responded to standard antithyroid treatment (19). In another case, plasmapheresis was opted for in a patient with Graves' disease having methimazole-induced agranulocytosis worsening to pericarditis, thrombocytopenia, and, finally, TS (17). While plasmapheresis was decidedly a therapeutic option, the challenge lay in the fact that plasmapheresis could potentially lead to hypocalcemia, which, in turn, could cause seizures. This posed a significant risk to our patient who had already had seizure and PRES. The most common cause of PRES is acute hypertension, which was the most likely reason in our case (20). Complications associated with plasmapheresis also include anaphylactoid reactions during the procedure and later risk of infection due to its immunosuppressant effect. The urgent need for removal of circulating hormones outweighed the potential complications in our hemodynamically compromised patient with TS. Close monitoring of the patient under appropriate multi-disciplinary supervision during and after the procedure ensured two successful sessions of plasmapheresis.
Studies have been conducted to determine the required duration of PEs to be fully effective in extracting thyroid hormones (21). During the clinical management of our patient, we did not evaluate the amount of thyroid hormone extracted during plasmapheresis. Previous reports have suggested that the amount of thyroid hormone removed may be insignificant compared with the amount ingested (22).We focused on the clinical improvement and levels of circulating hormone to determine the efficacy of plasmapheresis. It should be noted, however, in a recent report that plasmapheresis failed to produce clinical response in two sessions (23) and in another report, a 71 year-old woman experienced initial clinical deterioration after the second PE, presumably due to a rise in the FT4 level. In our patient, in a worsening case of TS where conventional management had failed, the normal thyroid profile was restored by plasmapheresis along with an improvement in her mental state. We conclude that with a few exceptions, plasmapheresis is generally a useful therapeutic option, in both exogenously and endogenously caused TS, when conventional management fails to improve the clinical course.
Footnotes
Disclosure Statement
The authors have nothing to disclose. No competing financial interests exist for any of the authors.