
Abstract
Background:
The prevalence of RET somatic mutations in sporadic medullary thyroid cancer (MTCs) is ∼40%–50%, and the most frequent somatic mutation is M918T. RET-positive MTCs have been demonstrated to have a more advanced stage at diagnosis and a worse outcome.
Aims:
The aim of the present work was to compare the prevalence of RET somatic mutations in sporadic microMTCs (<1 cm) and in larger MTCs.
Patients:
We analyzed the M918T RET point mutation in 160 sporadic MTC cases. Tumors were classified according to their size: group A, <1 cm; group B, >1 and <2 cm; group C, >2 and <3 cm; and group D, >3 cm.
Results:
The overall prevalence of the somatic M918T RET mutation was 19.4% (31/160). RET mutations were distributed differently among the four groups. The prevalence was 11.3% (6/53) in group A, 11.8% (8/68) in group B, 31.8% (7/22) in group C, and 58.8% (10/17) in group D, exhibiting an increase with increasing size of the tumor. When comparing the prevalence of mutations in the four groups, we found a lower prevalence in microMTCs (p<0.0001).
Conclusions:
The overall prevalence of RET somatic mutations was lower than expected, and the prevalence of the somatic M918T RET mutation was significantly lower in microMTCs than in larger tumors. To explain this finding, we can hypothesize either that other oncogene(s) might be responsible for the majority of microMTC, thus identifying a tumor subset, or that the RET mutation might, or might not, occur later during tumor progression.
Introduction
Somatic mutations of the RET proto-oncogene in the tumor tissue of sporadic cases are the most important molecular alterations recognized to date, and their prevalence ranges from 40% to 60% (3 –5). Mutations in the Ras gene have been previously reported in only a few cases (6,7) of sporadic MTC. Very recently, a high prevalence of H- and K-Ras mutations has been described in RET-negative MTC (8).
Several types of somatic RET mutations have been reported in sporadic MTC, but the most common mutation is M918T, in exon 16, whose prevalence is ∼90% among cases with somatic mutations (9). The presence of the M918T somatic mutation has been demonstrated to be correlated with an advanced stage at diagnosis (10 –12). With regard to the effect of the somatic M918T mutation on survival in sporadic MTC, those patients with the mutation showed more aggressive development of distant metastases during follow-up and had a significantly lower survival rate than patients without the mutation (5,13).
Somatic RET mutations have been demonstrated to be inconsistently distributed within primary tumors and metastases (14). Thus, these mutations are not seen as a monoclonal change within individual MTC samples, and their leading role in MTC carcinogenesis has been doubted (14). If somatic RET mutations have a lead role in the induction of MTC, their prevalence should be similar in smaller and larger MTC. The aim of the present work was to compare the prevalence of the M918T somatic RET mutation in microMTCs to that in larger MTCs to determine whether the mutation is an early and leading event in MTC tumoral transformation.
Materials and Methods
Patients
We studied 182 patients, 70 men and 112 women, affected by sporadic MTC. All patients were submitted to total thyroidectomy and central neck dissection as the minimal standard procedure at the same institution. The lymphadenectomy of the lateral compartment(s) was performed during the first surgical treatment if node metastases were diagnosed before surgery.
Only sporadic primary MTCs were included in this study. The definition of sporadic cases was based on the absence of germline RET mutations, the absence of a familial history of the disease, and negative clinical and laboratory data for the presence of other endocrine neoplasia.
Epidemiological, pathological, and clinical data were retrieved from a computerized database and analyzed according to the presence or absence of an RET mutation. The outcomes of 150 patients (10/150 [6.6%] were lost to follow-up) were also analyzed distinguishing “cured,” (including patients with at least one or two negative postoperative pentagastrin stimulation tests for serum calcitonin), from “not cured” patients, including all the others (both biochemical and clinically affected or dead patients).
An informed consent form for RET genetic screening and other clinical procedures was signed by each of the investigated subjects. The present study was approved by the Institutional Review Board.
MTC tissues
Eighty-four MTC tissues were collected at surgery, immediately frozen in liquid nitrogen, and kept at −80°C while 98 MTC tissues were microdissected from paraffin-embedded tissues. All paraffin-embedded cases had a diameter ≤2 cm and were selected for the purpose of this study. Tumor diameter of fresh collected MTC cases ranged from 0.5 to 7 cm. Blood from all patients was collected in EDTA.
Tumors were classified according to the size of the nodule as follows: group A, ≤1 cm; group B, >1 and ≤2 cm; group C, >2 and ≤3 cm; and group D, >3 cm.
Sensitivity assessment of the sequencing assay
The TT and MZCRC cell lines, derived from human MTCs harboring the RET mutations C634W and M918T, respectively, were used to determine the sensitivity of our sequencing method. The HeLa cell line was used to dilute MTC cells. The TT cell line was cultured in RPMI-1640 with 20% fetal calf serum, 2 mM L-glutamine, and 100 units/mL penicillin-streptomycin. The MZCRC cell line was cultured in Dulbecco's modified Eagle's medium with 10% fetal calf serum, 2 mM L-glutamine, and 100 units/mL penicillin-streptomycin. (15). HeLa cells were grown in Eagle's minimum essential medium with 10% fetal bovine serum.
As shown in Table 1, five different dilutions of both TT and MZCRC were prepared by adding HeLa cells. Five hundred, 200, and 100 ng of genomic DNA from each dilution were used for polymerase chain reaction (PCR) amplification of exon 11 or exon 16 based on the cell line used (TT or MZCRC, respectively). The sequencing analysis of the PCR products was performed as just described to detect the C634W and M918T mutations, respectively.
Extraction of DNA, PCR amplification, and sequencing
Genomic DNA was purified from peripheral blood lymphocytes, from fresh tumor tissues, and from cell lines as previously described (16). Paraffin-embedded tumor tissue was manually microdissected from one or two sections (Fig. 1). The presence of the tumor tissue was confirmed in the first and the last section for each section series. Deparaffinized samples were lysed and digested with proteinase K. DNA extraction was performed using the spin column procedure and a QIAAMP DNA mini kit (QIAGEN, Hilden, Germany) and finally reconstituted in 30 μL of H2O.
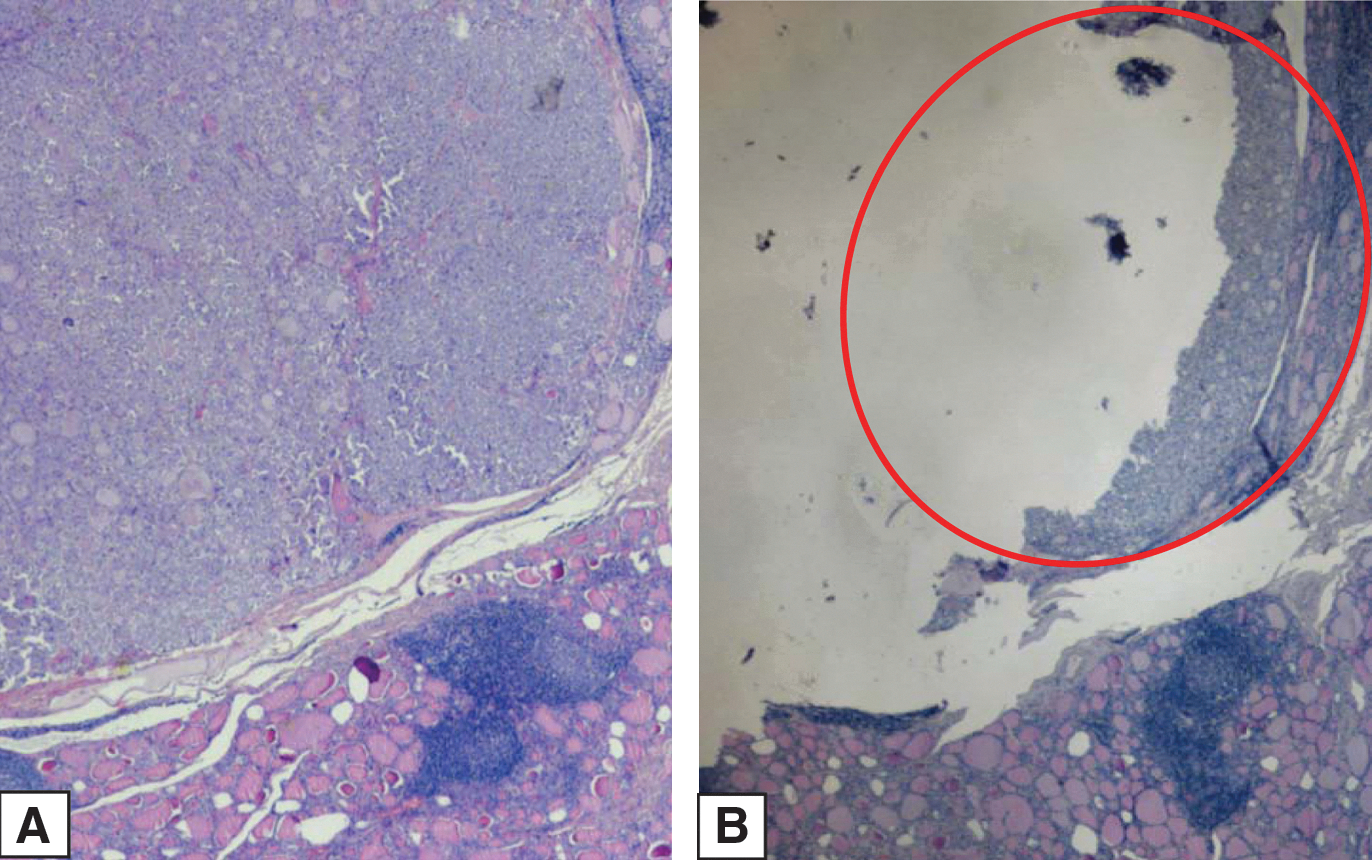
Tissue microdissection.
DNA concentrations were measured using an UV spectrophotometer (SmartSpec Plus Spectrophotometer, BioRad, Hercules, CA), and 200 ng of genomic DNA was used for PCR amplification.
Exon 16 of the RET gene was analyzed in all cases using PCR and sequencing, as previously reported (16,17). In 100 cases, exon 11 of the RET gene was also sequenced.
Results
Sensibility assessment of sequencing assay
For both cell lines, the amount of DNA used for PCR amplification (i.e., 500, 200, or 100 ng) did not affect the detection of the mutation. As shown in Figure 2, the presence of the C634W mutation in TT cells was evident even when only 10% mutated cells were present in the sample. A lower sensitivity was observed when the presence of the M918T mutation was analyzed in the different dilutions of MZCRC cells; it was detectable in dilutions with at least 30% mutated cells, thus suggesting that if the number of 918 mutated cells is <30%, we could miss this information and those cases that we considered negative are “true negative” or “positive for <30% of cells.”
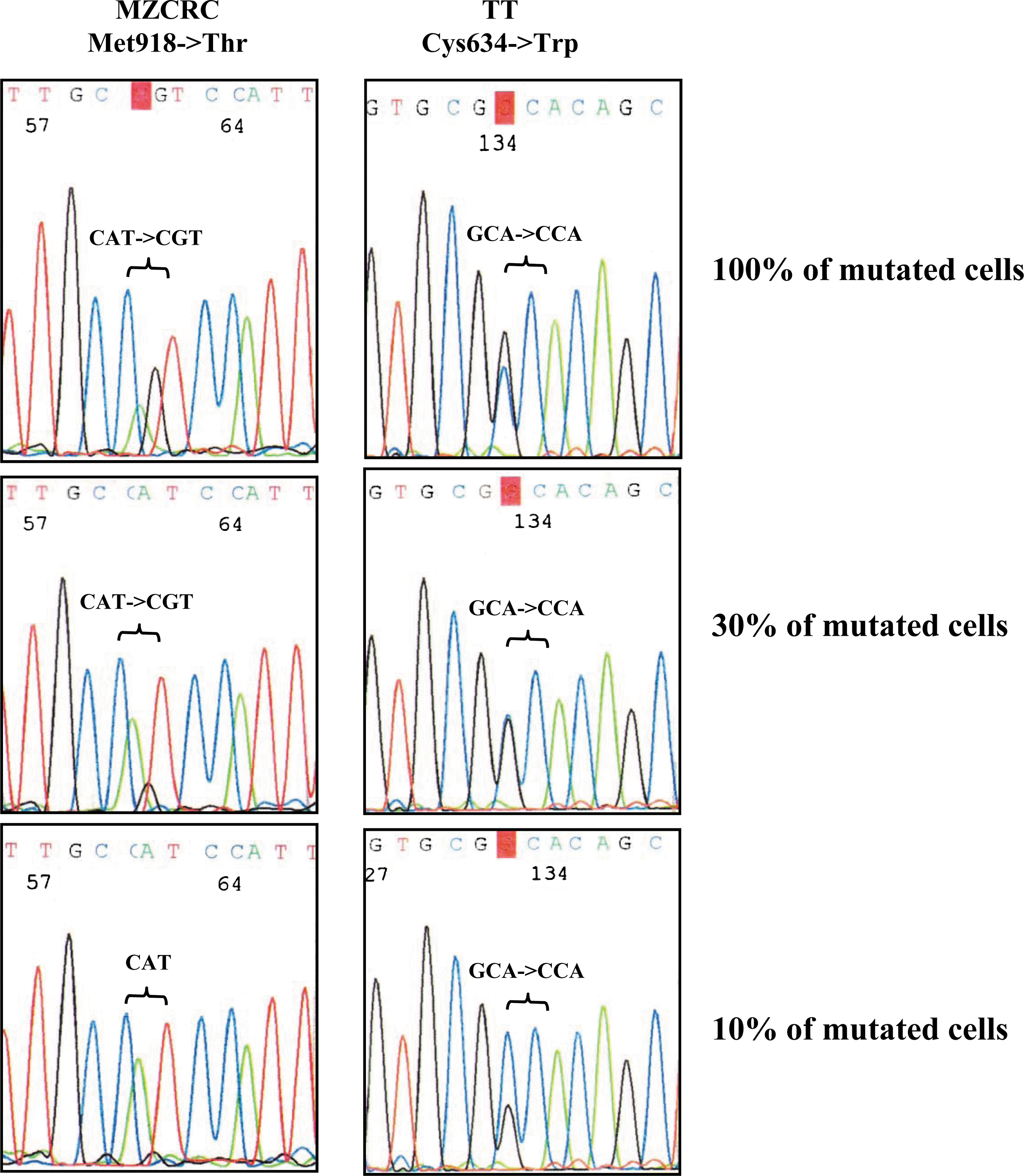
Sensitivity assessment of the sequencing assay: sequence analysis of RET exon 11 in serial dilutions of MZCRC cells (left) and of exon 16 in serial dilutions of TT cells (right). The pherograms show the anti-sense sequence.
Prevalence of RET mutation
The DNA of 22 out of 98 (22.4%) microdissected MTC cases could not be amplified by PCR and were excluded from the study. Conversely, the DNA from all fresh tumor tissues was adequately amplified. Whenever possible, we tested both fresh and paraffin-embedded tissues belonging to the same tumor, and the results were all repeatable. Among the 160 cases for which the DNA was successfully amplified, 53 belonged to group A (<1 cm), 68 to group B (>1 and <2 cm), 22 to group C (>2 and <3 cm), and 17 to group D (>3 cm). The four groups were homogeneous for the mean age of patients at diagnosis (mean age 53 year, range 17–79), while a significantly higher prevalence of women was observed in groups A+B (67%) than in groups C+D (41%).
In the total series of sporadic MTC, we found 31/160 (19.4%) cases with the M918T somatic RET mutation. As shown in Figure 3A, the highest prevalence (10/17, 58.8%) of the M918T mutation was found in MTC cases with the largest size (group D); lower prevalence of the RET mutation was observed in group C (7/22, 31.8%) and group B (8/68, 11.8%). The lowest prevalence (6/53, 11.3%), though similar to that of group B, was found in MTCs <1 cm in size (group A). The prevalence of the M918T somatic RET mutation in groups C and D were significantly higher (17/39, 43.6%) than those in groups A and B (14/121, 11.6%) (p<0.0001) (Fig 3B).
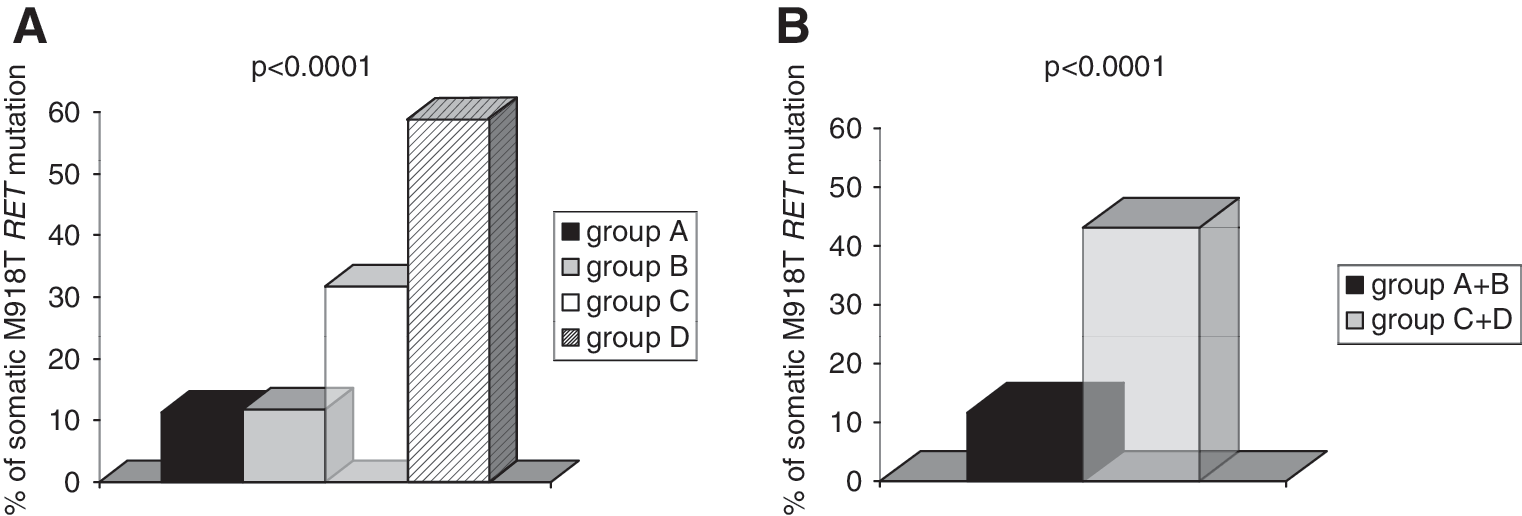
Prevalence of somatic the M918T RET mutation according to tumor size.
Codon 634 mutations were found in only 6/100 cases (3 C634R, 1 C634W, 2 C634Y). The prevalence of exon 11 mutations was not different among the groups; these cases are not included in the overall frequency of RET mutations.
RET mutation and outcome of MTC patients
As shown in Table 2, we distinguished the overall group of MTC patients as “cured” and “not cured” MTC patients, and we found that 36% of “not cured” versus 9.3% of “cured” patients had an RET 918 somatic mutation (p<0.0001), thus confirming our previous results that the presence of the RET 918 somatic mutation is significantly correlated with the persistence of the disease (5). Similarly, a statistically significant difference was observed in group C+D; in particular, 59.2% of “not cured” patients of this group had an RET somatic mutation, while only 8.3% of “cured” patients had an RET somatic mutation (p=0.003). In group A+B, the same trend of the prevalence of the RET somatic mutation was observed (18.9% vs 9.4% in not cured vs cured patients), but this difference did not reach a statistical significance.
10/160 patients lost to follow-up.
C+D>2 cm; A+B<2 cm.
NS, not significant.
We also observed that 41/119 (34.4%) of nonmutated MTC patients were not cured (Table 2): this percentage was 30.9% in group A+B and 50% in group C+D. When we looked at all the epidemiological and pathological data, we found that the RET negative not cured patients were those with a more advanced stage (data not shown).
Discussion
Recently, several observations have been reported which demonstrated that somatic RET mutations represent a risk factor for more aggressive biological behavior and reduced survival (5,11 –13). The prevalence of these mutations varies from 23% to 66% (3 –5,9,18), and the most common RET mutation is M918T, which is the most powerful transforming RET mutation (19). In the present study, we found an overall prevalence of RET of ∼20%, which is much lower than the prevalence found by us as well as others in previous studies (3 –5,9,18). In agreement with previous observations that somatic RET mutations are inconsistently distributed within primary tumors and metastases (14), one possible explanation of these discrepancies in the RET prevalence could be the nonuniform distribution of the M918T mutation. Alternatively, the relatively large group of small RET M918T-negative tumors included in this study could represent the real explanation. At least in our previous series (5), but also in the series of Moura et al. (13), the percentage of small MTCs was indeed much lower.
Tumors are believed to be clonal, arising from a single altered cell that acquires the ability to grow faster than normal cells. However, it is generally accepted that tumoral transformation is a multistep process, because other genetic alterations can occur during tumor growth (20). The leading genetic alteration should be present from the beginning and should be found in very small tumors. This is the case for the BRAF V600E mutation and the RET/PTC rearrangements that have been demonstrated to be present in small papillary thyroid cancers (PTCs), with a prevalence that was similar to that found in larger PTCs (21,22). In the present study, we compared the prevalence of somatic RET mutations, in particular the M918T mutation, in microMTCs, and in larger MTCs to verify whether the mutation is or is not an early event in MTC tumoral transformation. We found that in MTC cases smaller than 2 cm, the prevalence of the M918T somatic RET mutation was significantly lower than in larger tumors. No difference was observed in the prevalence of the M918T mutation when the MTCs <2 cm were subdivided into tumors of <1 cm and between 1 cm and 2 cm in size. These results indicated that the somatic RET mutation is not an early event, as previously suggested (14), but the information obtained in the two studies were both different and relevant. Eng et al. (14) demonstrated that cells either harboring or not the somatic RET mutation co-existed in the same tumoral tissue, but no information about the time of occurrence of the mutation was given. At variance, the present study suggested that the occurrence of the somatic RET mutation is more frequently late with regard to the tumoral initiation and proliferation, as it is rarely found in MTC smaller than 2 cm.
We and others demonstrated that patients with sporadic MTC harboring a somatic RET mutation had a more aggressive disease and a lower survival (5,13,23). In the present study, we compared the follow-up data, the mutation status, the tumor size, and the stage of our sporadic MTCs, and we observed that mutated cases were prevalently not cured. This evidence was statistically significant both in the total group and in MTC tumors >2 cm. The same trend was observed in MTC <2 cm, but this difference did not reach a statistical significance. On the basis of these findings, we can hypothesize that the occurrence of the somatic RET mutation is an event that accelerates the growth and malignant behavior of MTC. In agreement with our previous study (5), in which we demonstrated that both RET mutation and a more advanced stage were independent poor prognostic factors for a worse outcome, a great percentage of not cured patients of this series were also not mutated, but all these cases showed an advanced stage at diagnosis. Other unknown oncogenes could be responsible for the aggressive behavior and poor outcome observed in this group of RET negative cases.
The heterogeneity of MTCs was demonstrated several years ago (14). By analyzing subpopulations of MTCs, it was shown that 80% of sporadic MTCs had at least one tumor cell subpopulation with an RET mutation. We demonstrated that at least 10%–30% of mutated cells should be present in the sample to allow detection of the mutation by our sequencing system. Thus, MTCs with a percentage of mutated cells <10%–30% could yield a false-negative result in this assay. Therefore, we cannot completely exclude the possibility that the mutation is indeed present from the beginning but is present only in a small number of cells and is, thus, undetectable. We hypothesize that it is more likely that the sequencing results will be positive for tumors that are larger than 2 cm than for tumors that are <2 cm in size because of the greater number of mutated cells in the larger tumors. This hypothesis implies that mutated cells will grow faster than not mutated cells, because the prevalence of mutated cells should increase to at least 30% to be detected. Thus, this hypothesis strongly supports the idea that the M918T somatic RET mutation can confer a strong selective advantage to tumor cells.
An alternative hypothesis to explain the lower prevalence of the M918T somatic RET mutation in microMTCs is that small tumors originate from different genetic alterations. Recently, H- and K-Ras somatic mutations have been reported in ∼28% of sporadic MTCs (8). No correlation with the tumor size was found, but the series comprised primarily large tumors (i.e., mean size ∼3.5–4.0 cm). Therefore, we do not know whether the Ras mutation is that common in smaller MTCs. We did not have the opportunity to look for this mutation in the present series. However, the two mutations have been demonstrated to be almost mutually exclusive, thus suggesting that the two genetic alterations give rise to different tumors. If this is the case, the presurgical search for genetic alterations in fine-needle aspiration specimens could be useful for planning a more or less aggressive surgical treatment, particularly for microMTCs whose clinical impact is still debated (24,25).
In conclusion, our data indicate that the overall prevalence of RET somatic mutations is lower than expected and that the prevalence of the M918T RET somatic mutation is significantly lower in microMTCs than in larger tumors. This latter finding suggests that the somatic RET mutation is not an early and leading event but, rather, an event acquired later during the clonal expansion of the MTC whose presence makes tumor cells more aggressive. An alternative hypothesis is that microMTCs could be caused by other oncogene(s) with lower transforming activity.
Footnotes
Acknowledgments
This study was supported in part by grants from the Ministero della Istruzione Universitaria e Ricerca Scientifica (MIUR), the Associazione Italiana per la Ricerca sul Cancro (AIRC), the Istituto Toscano Tumori (ITT), and the Ministero della Salute, Progetto Ricerca Oncologica RF-CAM 2006353005.
Disclosure Statement
The authors have nothing to disclose.