
Abstract
Background:
Graves' disease is commonly treated with curative intent using radioactive iodine (RAI). While higher doses have been shown to increase success rates, more evidence is needed. Further, very few studies assess the time to treatment success without the need for antithyroid drugs after a single dose of RAI within the first year post-dose, despite earlier success being an important treatment objective. We aimed to evaluate the outcome of different RAI doses in terms of success rates and time to achieve this success (eu- or hypothyroidism). We hypothesized that higher doses would not only increase success rates, but bring about successful treatment earlier.
Methods:
We retrospectively analyzed the medical records of all patients diagnosed with Graves' disease between 1994 and 2009. Details of RAI treatment and outcomes thereof were documented. In our analysis, we divided the patients who received RAI treatment into three groups according to the dose received: I (≤15 mCi); II (16–20 mCi); III (≥21 mCi).
Results:
There were 498 patients diagnosed with Graves' disease. However, 105 were either lost to follow-up or still undergoing treatment. Of the remaining 393, there were 258 who received RAI treatment. The average initial dose was 21.42±6.5 mCi and overall success rate was 86%. Success rates were 74%, 85%, and 89% (p<0.05), while average time to successful treatment was 8.1, 4.6, and 2.9 months, respectively (p<0.001), for groups I, II, and III. When 20 mCi was given empirically, 85% obtained successful treatment; most of these within 3 months (mean 3.9; mode and median 3 months).
Conclusions:
This study provides additional evidence that success post-treatment correlates with administered dose and shows clearly, for the first time, that successful treatment is achieved earlier with higher doses. This knowledge is relevant to all clinicians managing Graves' disease as it can be taken into consideration when discussing treatment plans with patients.
Introduction
Methods
Medical records of all patients diagnosed with Graves' disease between January 1994 and July 2009 at the Thyroid Outpatient Unit of the Hospital de Clínicas at the Federal University of Parana, Curitiba, Brazil—a quaternary referral center—were retrospectively reviewed. Inclusion criteria consisted of a diagnosis of Graves' disease, RAI administration at any stage throughout the treatment course, and the arrival at a definitive clinical outcome. Exclusion criteria consisted of patients still receiving treatment and those lost to follow-up. The diagnosis of Graves' disease was made on the basis of elevated free T4 or total T4 with suppressed TSH concentrations and clinical examination, supported by thyroid autoantibodies and radionuclide imaging. The decision to use RAI as treatment for Graves' disease, and the follow-up plan thereafter, was made at the discretion of the treating endocrinologist. The age and sex of all patients were recorded. We documented the indication for therapeutic RAI (post-antithyroid drugs or first-line treatment); the dose, whether it was empirical or calculated; the need for further doses; and the time until control of thyrotoxicosis was achieved.
“Successful treatment” post–RAI administration was defined as hypothyroidism or euthyroidism off all antithyroid drugs after a single dose of RAI. “Success rates” were defined as the number of patients who achieved the latter at a determined time post–RAI dose, usually the duration of the follow-up period. While “time to successful treatment” was the average time it took to achieve the same. This was a function of when thyroid function tests were taken, usually for follow-up appointments. Given the constraints of our public system, these visits were between 6 weeks and 3 months post–RAI dose. However, some patients came with laboratory results done at their local health center many weeks prior.
In our analysis, we divided the patients who received RAI treatment into three groups according to the dose received: I (≤15 mCi); II (16–20 mCi); III (≥21 mCi).
Statistical analysis was performed using the SPSS software, version 17 (SPSS, Inc., Chicago, IL). Nonparametric analyses were used. Data were expressed as mean±standard deviation as well as mode, median, and range. The Kruskal–Wallis test and LSD analysis were used to compare the three groups in terms of age at diagnosis, RAI uptake, pretreatment with antithyroid drugs, mean initial dose, time to success, and cumulative dose. Chi-square test was used to compare groups in terms of success rates. When statistically significant differences were found, Wilcoxon rank-sum and Fisher exact tests were performed to ascertain which pair of groups was different. A p-value of <0.05 was considered statistically significant. The study was approved by the Ethics Committee for Research in Humans of our institution.
Results
Altogether over the study period (1994–2009), files from 498 patients were reviewed. One-hundred and five of these were excluded as they were lost to follow-up or were still receiving treatment; thus, final outcome data could not be obtained. Out of the remaining 393 patients, 258 were administered RAI. Of these, 221 were women (85.60%) and 37 were men. In terms of the indication for RAI treatment, 81.40% of these patients received RAI treatment after initial treatment with antithyroid drugs, because of treatment failure (70.16%) or disease recurrence (11.24%). It was used as first-line treatment in 16.28% and post unsuccessful surgery in 2.32% (six patients).
The dose of RAI was empirical in 85.27% of cases and calculated in 12.40%, while in 2.33% this variable was not known. The mean dose was higher in the empirical group (22.79±5.66 vs. 12.04±3.71, p<0.0001). The success rate and time to cure were 85.00% and 3.52 months in the calculated group, compared with 74.19% and 14.48 months in the empirical group (p=0.127; p<0.0001), respectively.
The average initial dose was 21.42±6.5 mCi (n=253) with a range between 6 and 29.9 mCi. The total dose averaged was 24.60±11 mCi (n=253) with a range between 6 and 89.7 mCi. The 24 patients who required more than 29.9 mCi received this due to treatment failure, in divided doses with an interval of at least 6 months between RAI administrations. The mean dose in these 24 patients was 50.30 mCi (range 35–89.7 mCi); only one patient was initially treated with <20 mCi of RAI. There was no correlation between pre-dose RAI uptake and the treatment dose needed or the time to success. No antithyroid drugs were administered post–RAI treatment, consistent with our clinic's protocol. The overall success rate was 85.50%, whereby 14.50% of our patients needed a second dose.
When dividing those patients whose initial dose was known into groups, there were 61 in the first (group I, ≤15 mCi), 95 in the second (group II, 16–20 mCi), and 97 in the third (group III, ≥21 mCi). The percentage of patients in each of these groups who developed hypothyroidism or euthyroidism post-dose were 73.68%, 84.95%, and 89.01%, respectively (p=0.045). This difference was significant between groups I and III and showed a trend between groups I and II. That is, 26.32% of patients in group I, 15.05% in group II, and 10.99% in group III needed additional RAI doses (Fig. 1). The average time to successful treatment was 8.12, 4.61, and 2.87 months, respectively (p<0.001) (Fig. 2). A summary of the general findings described above is depicted in Table 1.

Success rates in Graves' disease after first radioactive iodine (RAI) doses. p=0.045 overall; *p=0.09; **p=0.015.
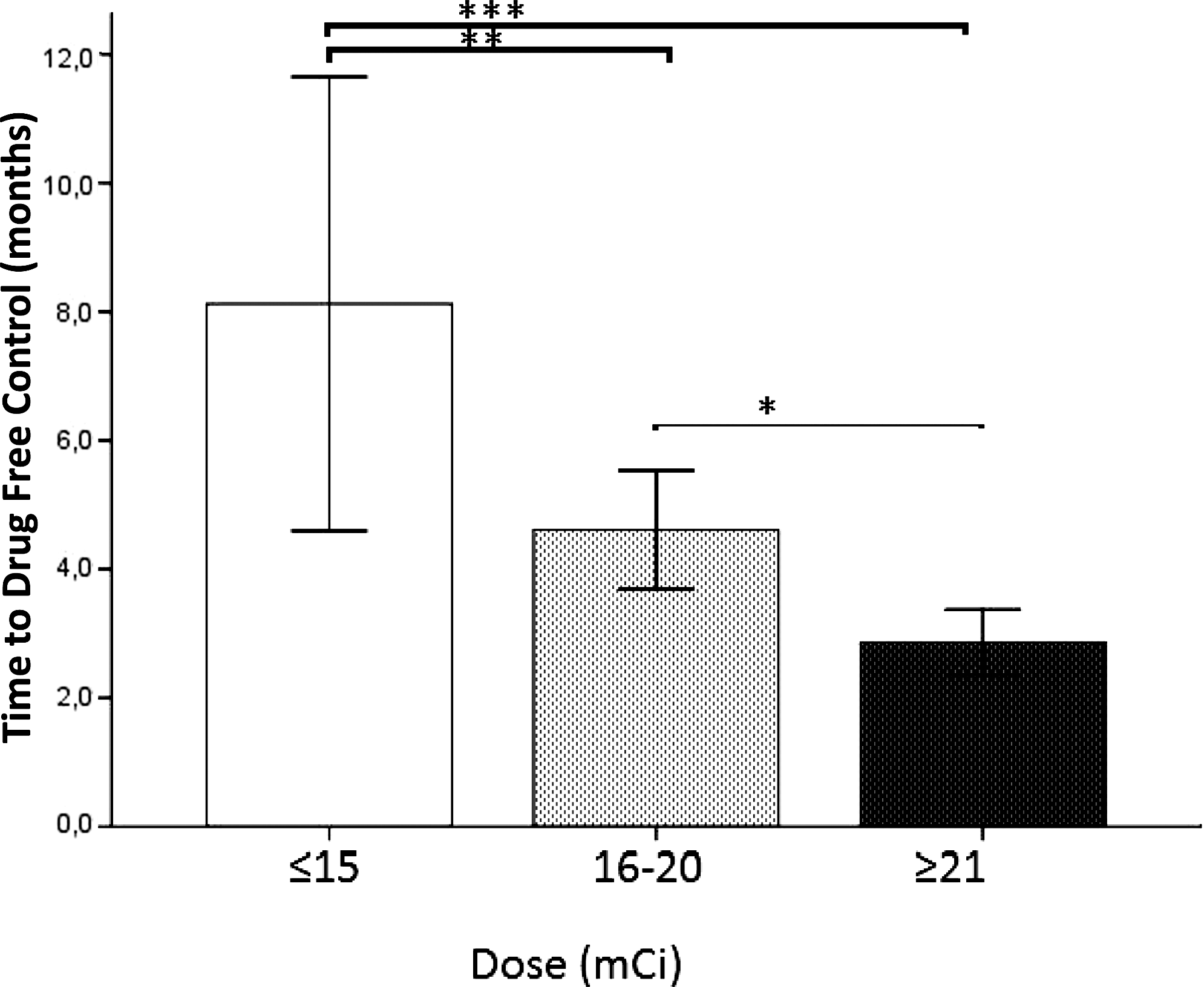
Time to successful treatment in Graves' disease depending on RAI dose administered. p<0.001 overall; *p=0.067; **p=0.002; ***p<0.001.
Group I differed significantly from group III (p=0.009).
Antithyroid drugs refer to either methimazole, proplythiouracil, or methimazole and proplythiouracil in combination.
Either alone or in combination with methimazole.
Group I differed significantly from groups II (p=0.037) and III (p=0.036) when comparing the patients who used propylthiouracil (either alone or in combination with methimazole) with those who used either methimazole alone or no pretreatment.
p<0.0001 for all pair-wise comparisons.
Group I differed significantly from group III (p=0.015).
Group I differed significantly from groups II (p=0.002) and III (p<0.001).
Of note, within group II, there were 89 patients who received an empirical dose of 20 mCi. There were 85.39% of these who were subsequently eu- or hypothyroid, while the remaining 14.61% required an additional dose. The average time to treatment success in this 20 mCi group was 3.9±2.1 months with a mode and median of 3 months (range 1–11.5 months).
Discussion
Hyperthyroidism has well-known unacceptable consequences, including cardiovascular disease, such as atrial fibrillation and heart failure; osteoporosis; and reproductive problems (2,6). Left untreated, these can progress to thyroid storm, the incidence of which is high within our service (unpublished data), which has significant morbidity and mortality. Hence, definitive therapy with RAI is frequently the treatment option chosen by patients and physicians. To avoid patients remaining exposed to the risks of hyperthyroidism as well as costly and difficult to comply with repeat hospital outpatient visits for slowly evolving hypothyroidism, a single dose is ideal. Our success rate of 85.5% is consistent with that generally referred by Ross (6). Our average initial dose is not very different from our average total dose. This means that those who had lower initial doses and then required further RAI treatment received similar cumulative doses to those who received a higher initial dose; however, they experienced prolonged hyperthyroidism and more medical interventions.
Our patients were subjected to higher doses of RAI than those recommended (5). Looking at our success rates, however, it is clear that these doses are in fact necessary. Even when patients were given more than 21 mCi, 10.99% still needed an additional dose. Further, all but one of the 24 patients who received a cumulative, divided dose above 30 mCi had initial doses of 20 mCi or higher, suggesting that these high initial doses were not superfluous. We no longer prescribe a low-iodine diet prior to ablation as patient compliance was extremely poor when we did. Countries like Chile and Brazil have an excess of iodine ingestion, whereby more than 60% of their populations have been found to have urine iodine levels >300 μg/dL (14). Indeed, it was in Brazil that the highest cumulative RAI dose (115 mCi) ever described was required to control thyrotoxicosis in a patient with Graves' disease (15). Thus, a diet high in iodine without any reduction thereof prior to treatment may reduce the efficacy of RAI administration and hence account for the high RAI doses required. Indeed, 14.3% of our patients' RAI uptake levels were within the normal reference range (unpublished data). Nevertheless, we, as others (13), did not find any correlation between our patients' RAI uptake levels and the dose required to bring about success or the time to achieve this. In fact, patients in group I, whereby less RAI was administered, had significantly more uptake than those in group III (p=0.009), while faster time to treatment success along with higher rates thereof was achieved in this group. Another potential explanation is that our patients' goiters are larger, and hence less response to lower doses of RAI (8,16), than the average Graves' disease goiter, although we have no objective evidence of this. Lastly, our average age at diagnosis was lower than that commonly described (2), a factor reported to predict worse response to RAI treatment (8).
We have shown that higher initial RAI doses are associated with higher rates of treatment success. The percentage of patients requiring at least one additional RAI dose in group I were more than twice that in group III. There were 26.32% of the patients who received ≤15 mCi and remained hyperthyroid but this rate dropped to 10.99% in those who received 21 mCi or more. With the exception of one article, in which the dose (10 vs. 15 mCi) did not alter success rates (17), other studies have found similar results as we report. A British group (9) examined a patient population as big as ours and found that those who required more than one dose of RAI had been treated with a significantly lower initial dose. A Finnish study had a 75% success rate with just 7 mCi but 25% of their patients required two to six doses to achieve this (10). A Mexican study, which advocates high fixed doses over 20 mCi, examined almost 600 patients over 10 years. The authors found that the percentage of patients who achieved remission increased in direct proportion with the RAI doses used (11). A few studies looked at the radiation dose actually absorbed by the thyroid and found a strong positive correlation between this and the success of therapy (13,18). We, and many other public hospital outpatient clinics, do not have the resources to perform routine RAI uptake scans with 4- and 24-hour readings along with detailed RAI kinetics calculations. Thus, our finding that the administered dose correlates with the rate of success, which corroborates those formerly described, provides a useful base upon which clinical decisions can be made.
This study clearly demonstrates that higher doses of RAI result in faster treatment success. The time to evolve to hypo- or euthyroidism was 8.1 months in group I (≤15 mCi), an interval significantly longer than 4.6 months seen in group II (16–20 mCi) and just 2.9 months in group III (≥21 mCi). This association has been alluded to in the literature as early as 1975 (19). More recently, Canadas et al. (12) showed, in northeastern Brazil, that higher doses resulted in higher success rates at 6 months' follow-up, a difference which was no longer observed after 12 months. The Mexican study above also found earlier remission with higher doses that, interestingly, only became apparent after 24 months (11). The actual time to successful treatment, however, was not described in either of these studies. In addition, an Italian study, referred to above (13), showed increased hypothyroidism after 1 year with higher absorbed doses. Thus, although others have directly and indirectly shown that higher doses of RAI bring about more rapid treatment success, we are unaware of any other reports that show this as clearly as we report here, with actual time frames associated with individual doses, especially within the first year post-dose. Indeed, for the most part, our patients were controlled more rapidly than those in other reported series (11,18,20), a result that we attribute to the high doses used. Indeed, the significantly shorter time to successful treatment found in our study among those treated with empirical doses of RAI is likely to be accounted for by the higher dose administered, and not whether that dose was empirical or calculated.
We achieved our desired outcome of prompt eu- or hypothyroidism in 85% of patients who received 20 mCi, most of whom achieved this within 3 months. This dose prevents unnecessary exposure to high RAI doses while avoiding repetitive interventions that delay successful treatment.
The retrospective nature of our study imposes some limitations on the time to successful treatment, in that the interval between which patients were seen could have exaggerated differences among groups. Further, on subanalysis, we found that there were more patients in group I who received proplythiouracil as compared with the other groups (Table 1). This may have biased our results given there is data that suggests resistance to RAI treatment after proplythiouracil while the same is still unclear in terms of methimazole (5). Yet another potential bias is that the average age at diagnosis tended to be younger in group I. Nevertheless our work paves the way for a prospective randomized double-blind study that controls for age as well as type of antithyroid drug given pre-dose and has fixed, frequent follow-up thyroid function tests to confirm our findings without these limitations.
In summary, we were able to demonstrate better success rates and clearly establish, for the first time, earlier treatment success with higher RAI doses in patients with Graves' disease. While 20 mCi is the ideal dose to bring about speedy success in our patient population for reasons described previously, lower doses are sufficient to achieve the same in most other centers. Nevertheless, we feel our findings are relevant to all clinicians managing Graves' disease because they equip them with a new concept—successful treatment occurs earlier with higher doses.
Footnotes
Acknowledgments
The authors would like to acknowledge the assistance of Dr. Cléo Otaviano Mesa, Jr., for his advice during discussions about this project, Dr. Fernando Mesquita Lima for his assistance with some of the data collection, and Dr. Thaís Hissami Inoue for her assistance with some of the data collection.
Disclosure Statement
The authors declare that no competing financial interests exist.