
Abstract
Background:
Considerable evidence suggests that hypothyroidism could promote atherosclerotic vascular changes. We planned this study to investigate whether serum free thyroxine (FT4) or thyroid-stimulating hormone (TSH) levels are associated with coronary artery calcification measured in healthy euthyroid subjects.
Methods:
A cross-sectional analysis was performed among subjects who visited our hospital for a health checkup. Among 1849 subjects, 669 (mean age 55.3±8.8 years; 392 men) with FT4 and TSH in the normal ranges were included after excluding those with diabetes, a history of current smoking and cardiovascular disease (CVD), or the use of drugs for hypertension, antithyroid drugs, or thyroid hormone preparations. Coronary artery calcium scores (CACS) were measured by multi-detector computed tomography.
Results:
Subjects with a CACS >100 had lower FT4 levels than those with a lower CACS (p=0.017), whereas no difference was observed in the TSH levels among CACS categories. FT4 levels had an odds ratio of 0.06 for high CACS (95% confidence interval=0.01–0.74; p=0.028) after the adjustment for CVD risk factors. In multivariate regression analysis, CACS was negatively correlated with FT4 levels (β=−0.823, p=0.032), and the inverse association between FT4 and CACS remained significant only in men (p=0.011).
Conclusion:
FT4 levels were inversely associated with coronary artery calcification in euthyroid healthy subjects, especially in men independent of conventional CVD risk factors. Further studies are needed to validate whether subjects with decreased FT4 levels within the normal reference range are at a high CVD risk and have poor cardiovascular outcomes.
Introduction
Thyroid hormone plays a major role in regulating energy expenditure and metabolic activity at the cellular level (2), and thyroid insufficiency causes hemodynamic alterations and metabolic disturbances in glucose and lipid concentrations (3,4), all of which can initiate and promote the process of atherosclerosis. Naturally, whether mild thyroid hormone deficiency could promote atherosclerotic CVD has gained considerable attention, as most of it occurs without overt hypothyroidism. Some prospective studies and meta-analyses have reported that even subclinical insufficiency has a predictive role for cardiovascular(CV) death (5). In addition, several cross-sectional studies have suggested that thyroid function could influence atherosclerotic vascular changes even in the euthyroid state (6 –8). However, controversy persists about the association between small changes in thyroid function and increased CV risks (9).
Recently, multi-detector computed tomography (MDCT) was introduced as a noninvasive, powerful method that evaluates coronary arteries and quantifies coronary artery calcium (10). The coronary artery calcium score (CACS) is a reliable surrogate marker of atherosclerotic vascular changes (11). The CACS correlates well with the cardiac plaque burden observed in histopathologic findings and intravascular ultrasound (12). Moreover, many studies reported that the CACS assigns high predictive values for future coronary artery disease and even mortality (13).
This study was planned to investigate whether the serum free thyroxine (FT4) or thyroid-stimulating hormone (TSH) levels are associated with coronary artery calcification measured by MDCT in healthy euthyroid subjects independent of other confounding factors.
Methods
Study population
We retrospectively recruited subjects who had undergone a general health check-up at Seoul St. Mary's Hospital Health Promotion Center between March 2009 and December 2010. Among 1849 subjects between the ages of 20 and 80 with data on a cardiac CT and thyroid function tests, we excluded individuals with FT4 and TSH values out of the normal range (n=246), use of antithyroid drugs or thyroid hormone medication (n=53), a history of CV, cerebrovascular, or peripheral artery disease (n=88), a history of diabetes or fasting glucose ≥126 mg (n=196), use of antihypertensive drugs (n=305) or lipid lowering agents (n=64), current smokers (n=223), serum creatinine levels ≥1.5 mg/dL (n=1), and liver enzyme levels >2.5× the upper normal limit (n=4). A total of 669 subjects were included in the final analysis. This study was approved by the institutional review board of Seoul St. Mary's Hospital, Seoul, Korea.
Measurement of anthropometric and biochemical parameters
Medical history and social-behavioral information were collected through questionnaires completed by the patients. Physical examinations were performed by measuring height, weight, waist circumference (WC), and blood pressure (BP) according to standardized methods. During measurements, the subjects were barefoot and wearing light clothing. Body mass index (BMI) was calculated by dividing weight by the height squared (kg/m2). Before the measurement of BP, the subjects were resting in a sitting position for 10 minutes. The BP was measured twice with at least a 5-minute interval to obtain an average value. Blood samples were collected after the subjects had fasted at least 10 hours. The fasting plasma glucose (FPG), hemoglobin A1c, total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) were enzymatically determined using the Hitachi 7600 chemistry analyzer (Hitachi). Fasting insulin levels were measured using commercially available RIA kits (Insulin RIA beads; TFB-Japan Co. Ltd.). Insulin resistance was calculated by homeostasis model assessment (HOMA-IR=fasting insulin [μIU/mL]×FPG [mmol/L]/22.5). The serum FT4 and TSH levels were measured by enzyme immunoassay using a commercially available kit (ADVIA Centaur®; Seimens). The reference ranges of FT4 and TSH were 0.93–1.70 ng/dL and 0.35–5.50 mIU/L, respectively. The Framingham risk score (FRS) was calculated to estimate a 10-year risk for coronary heart diseases using validated algorithms (14).
Cardiac CT: CACS
Cardiac CT was performed using a 64-slice multidetector CT scanner (SOMATOM Definition; Siemens Medical Systems). Intravenous esmolol (10–30 mg) was given if patients had a heart rate of >70 beats per minute. A calcium score scan was performed using a retrospective method with a tube voltage of 120 kV and 110 effective mAs with a 200 mm field of view. Data were reconstructed to a 5-mm slice thickness at a −400 ms acquisition window. CACS analysis was performed onsite with a dedicated workstation and analysis software using TeraRecon workstations (Aquaris workstation; TeraRecon, Inc.). CACS were determined according to the method described by Agaston's scoring system.
Statistical analysis
Statistical analyses were performed using SAS version 9.1 (SAS Institute). Data were expressed as mean±standard deviation or percentage unless otherwise stated. Differences of laboratory values between men and women were evaluated using the Student's t-test or Chi-square test. Due to skewed distribution, log-transformed CACS+1 were used in the analysis by including CACS as a continuous variable. Pearson correlation analyses were performed to examine the association between CACS and various parameters. The odds ratios (ORs) and 95% confidence intervals (CI) for high CACS (>100) were assessed using multivariate logistic regression analyses according to FT4 or TSH levels. To determine the independent association between thyroid function and CACS as a continuous measure, multiple linear regression analysis was performed. A subgroup analysis stratified by gender was done using analysis of covariance. p-Values of <0.05 were considered statistically significant.
Results
A total of 669 subjects (392 men) aged 55.3±8.8 years were recruited, and their general characteristics are shown in Table 1. Men were more likely to have higher BMI, WC, systolic BP, diastolic BP, TG, FPG, 10-year FRS, and FT4 levels but lower HDL-C and TSH levels than women. CACS was also different with regard to both mean and categorical values between men and women. No significant difference was shown for either age or HOMA-IR.
Data are expressed as means±standard deviation.
BMI, body mass index; WC, waist circumference; BP, blood pressure; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; FPG, fasting plasma glucose; HOMA-IR, homeostasis model assessment-insulin resistance; FRS, Framingham risk scores; FT4, free thyroxine; TSH, thyroid stimulating hormone.
Table 2 shows that the association between CACS and clinical variables. CACS was significantly correlated with age (r=0.36, p<0.001), WC (r=0.10, p=0.009), systolic BP (r=0.19, p<0.001), diastolic BP (r=0.18, p<0.001), TC (r=0.09, p=0.017), TG (r=0.08, p=0.047), LDL-C (r=0.09, p=0.025), and FT4 levels (r=−0.10, p=0.013), but not with TSH levels. Subjects with CACS>100 had lower FT4 levels than those with lower CACS (p=0.017), whereas no difference was shown in TSH levels among CACS categories (Fig. 1).
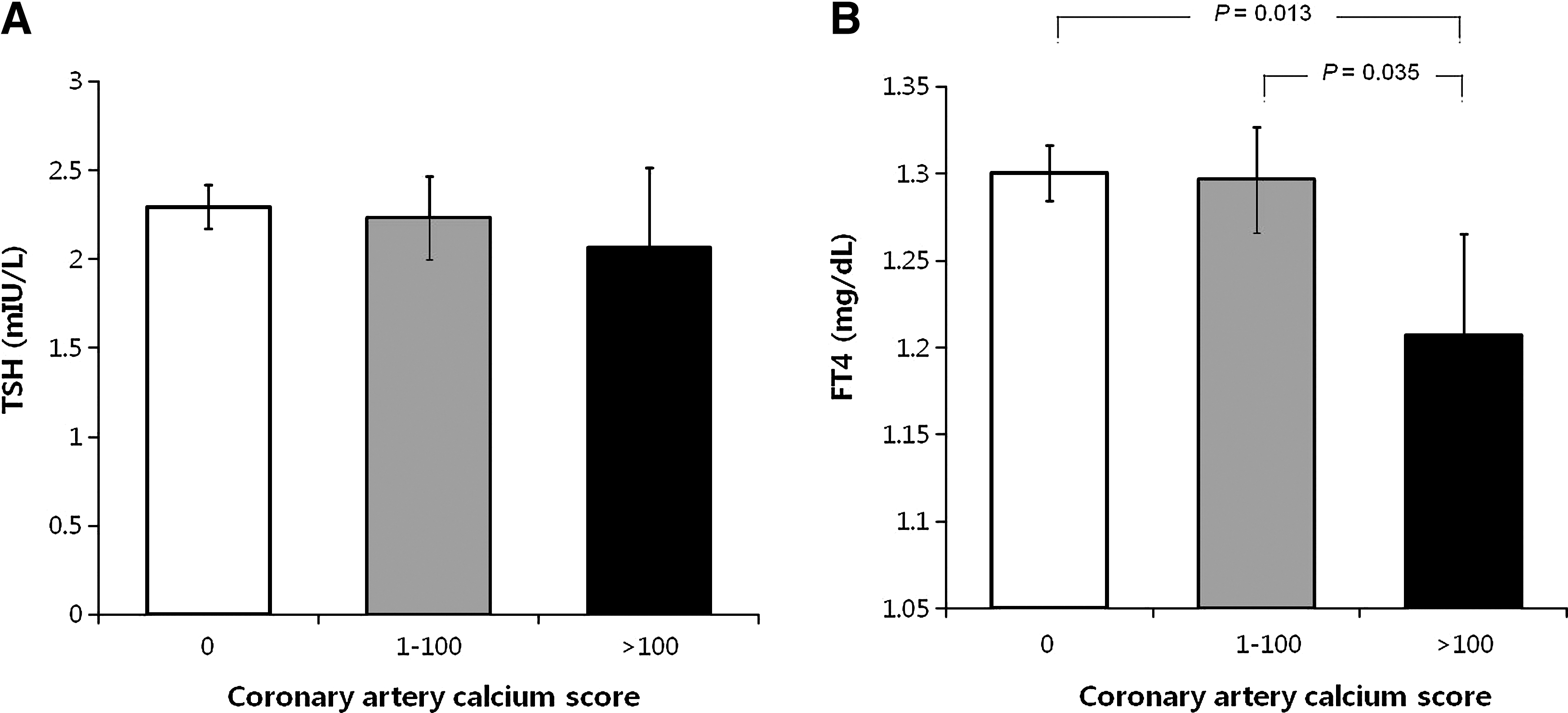
Mean values of thyroid stimulating hormone (TSH)
Subsequently, a multivariate logistic analysis was performed to investigate the independent association between thyroid function and the high CACS shown in Table 3. FT4 was significantly associated with high CACS (OR=0.06 [95% CI=0.01–0.74], p=0.028 in Model 1) besides age and male sex, whereas no association was present in TSH (Model 2). Furthermore, CACS was significantly associated with FT4 levels (β=−0.823, p=0.032) using a multivariate linear regression model adjusted for age, sex, BMI, WC, systolic BP, diastolic BP, TC, TG, HDL-C, LDL-C, FPG, HOMA-IR, and TSH (Table 4). In the subgroup stratified by gender, the association between FT4 and CACS was statistically significant in men (p=0.011) (Fig. 2). Due to the markedly low incidence of CACS>100 (0.7%), we could not determine the association between FT4 and CACS in women.
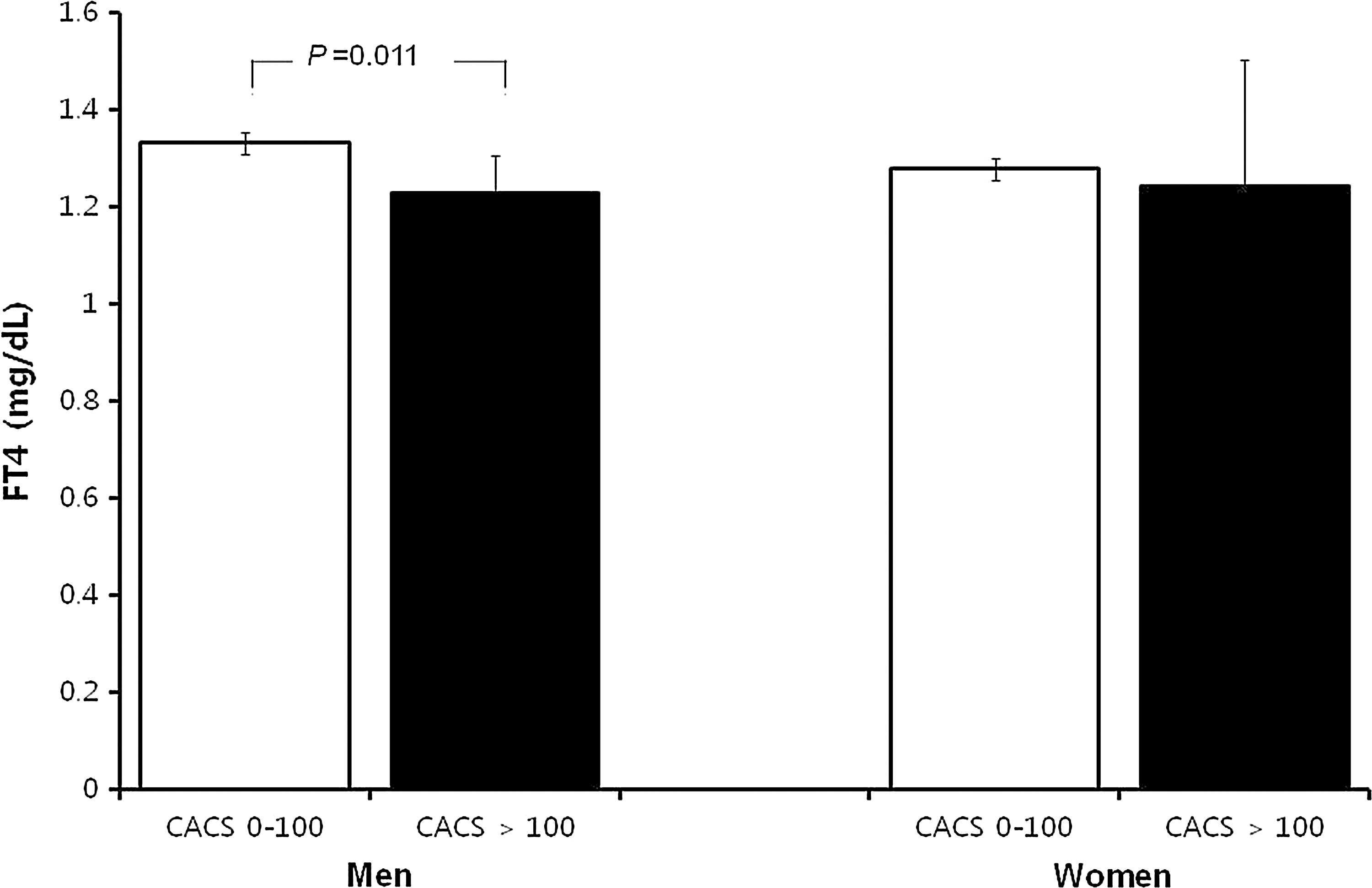
Comparison of FT4 values according to categorized CACS by gender. CACS>100 was present in 40 (10.2%) men and 2 (0.7%) women. All variables were adjusted for age, sex, body mass index, waist circumference, systolic blood pressure, diastolic blood pressure, total cholesterol, triglyceride, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, fasting plasma glucose, homeostasis model assessment-insulin resistance, and thyroid-stimulating hormone.
The odds ratios were calculated after adjusting for variables shown in the first column.
OR, odds ratio; CI, confidence interval.
SE, standard error.
Discussion
In the present study, we found that lower serum FT4 levels were associated with higher coronary artery calcification. This association remained significant after an adjustment for conventional risk factors, including age, sex, BMI, BP, lipid, and glucose profiles in healthy euthyroid subjects. These results suggest that serum FT4 levels which are within the lower part of the reference range could be a significant risk factor for CVD and be indicative of coronary atherosclerosis.
In line with our study, several cross-sectional studies have suggested that mild thyroid hormone insufficiency has a close link to vascular dysfunction and structural changes (6 –8). An association has been observed between lower FT4 levels within normal values and impaired endothelium-dependent vasodilatation, an early marker of vascular dysfunction (6). In addition, an independent association of carotid intima-media thickness (CIMT) with FT4 levels in euthyroid subjects have been reported (7,8), although one study did not find an association between CIMT and categorized TSH levels (15).
To the best of our knowledge, only one cross-sectional study has investigated the relationship between thyroid dysfunction and coronary artery calcification. In this study, the relationship between subclinical hypothyroidism and CAD was assessed in 2404 subjects with intermediate to high risk for CVD (16). Of these, 2355 were euthyroid, and 49 had subclinical hypothyroidism. They noted an association between occult CAD (based on the presence of coronary artery plaques) and subclinical hypothyroidism. Their finding that the association occurred only in men, and could not be documented in women, is consistent with our data. However, contrary to our results, they did not find an association between CACS and subclinical hypothyroidism by multivariate analysis (16). This discrepancy might be related to differences in the methods dealing with the thyroid functional status of patients. They compared the CACS between subclinical hypothyroidism and euthyroidism (16), but our study assessed the association between FT4 levels and CACS in euthyroid subjects. In addition, their study subjects, having an intermediate to a high risk of developing CAD (Framingham 10-year risk≥10%), were quite different from our healthy euthyroid subjects who did not have major risk factors, such as diabetes, the use of antihypertensive or lipid lowering agents, or smoking.
At least three hypotheses can be formulated that explain the association between FT4 levels in the lower part of the normal range and coronary calcification. First, the lowered FT4 levels could mediate atherosclerosis indirectly by promoting unfavorable metabolic changes that are similar but to a lesser degree than that observed in overt or subclinical hypothyroidism (17). This hypothesis postulates a direct influence of the thyroid hormone on vascular dysfunction. The hypothesis is supported by the data that the thyroid hormone induces relaxation of vascular smooth muscle cells (VSMC) (18), increases endothelial nitric oxide production via the phosphatidylinositol 3-kinase/Akt pathway, matrix Gla protein (an inhibitor of vascular calcification) (19), adrenomedulline (an antioxidant) (20) and adenosine (vasodilator) by AMP hydrolysis (21), and inhibits VSMC proliferation by angiotensin II type 1 receptor signaling activated by angiotensin II (22).
The second hypothesis is that atherosclerosis could in some way promote lower serum FT4 levels without evoking a rise in serum TSH. This could be postulated to be a protective mechanism. Lowered thyroid hormone could have a benefit on the vasculature, by reducing cardiac burden and metabolic demand (23). Weakening this hypothesis is that many longitudinal studies have consistently reported that a decline in thyroid function has an adverse effect on CVD outcome. Furthermore, several studies have reported that thyroxine replacement in subclinical hypothyroidism restored the increased IMT in a normal direction (24). The third hypothesis is that low FT4 levels could be associated with CAC score due to shared genetic (25) or environmental factors (26,27), rather than a causal relation. Either way, slightly low FT4 levels within the reference ranges have clinical implications by indicating subjects at a higher risk for CVD.
Significantly, the present study found that only serum FT4 levels and not serum TSH levels were associated with CACS. Consistently, many studies have reported an association between low normal FT4 levels and the metabolic parameters associated with atherosclerosis (6,25,28 –33) or atherosclerotic vascular changes themselves (6 –8). This occurred either with (6,8,25,29 –31) or without (7,28,32) serum TSH changes that are consistent with primary thyroid failure. The biological mechanisms for this association are not clear, but some researchers postulate that the serum FT4 concentrations could be a more sensitive indicator of “cardiac thyroid status” than serum TSH concentrations (34,35). It may or may not be pertinent that TSH levels, while very sensitive for detecting pituitary hypothyroidism, are not considered reliable for estimating the severity of the thyroid hormone deficit in hypothyroidism (36). In a study of mildly hypothyroid patients, albeit having mildly elevated serum TSH concentrations, an increased FT4 within the reference ranges, but not TSH, was the most significant variable predicting improvement in brachial artery flow-mediated dilatation after levothyroxine replacement in subclinical hypothyroidism (35).
The present study was performed in healthy subjects with low CV risk profiles having mean FRS values of 7.0% in men and 1.4% in women in order to minimize potentially confounding influences that might, in themselves, affect CACS. However, considering the low prevalence of CACS>100 of 6.3% in the current study, the findings cannot be used to support a clinical recommendation for routine diagnostic tests based on FT4 values in the lower part of the reference range in the general population. Recently, a multi-ethnic study of atheroslcerosis showed the superiority of CAC to high-sensitivity C-reactive protein (hsCRP) in predicting coronary events among subjects at a low risk, and suggested that CAC measurements could help further stratify risk groups on statin treatment in the population with low LDL-C and high hsCRP concentrations (37). Based on our study, thyroid function tests could provide additional information for selecting the population who would receive benefits from CT evaluation. Howerer, the hypothesis that medical and cost effectiveness of routine CAC measurements would ensue requires validation. Basic research on the effects of T4 in the heart vasculature might enhance our biological knowledge of atherosclerosis and provide new therapeutic options.
There are several limitations to this study. First, its cross-sectional nature limits our ability to infer causal influence of the relative thyroxine deficit on the coronary vasculature. Further, only FT4 levels measured by immunoassay were available among thyroid hormones. Measurements of total T4, total, or free T3 levels could provide useful information to determine whether other associations exist and what their relative importance are, perhaps also discriminating patients with nonthyroidal illness, although the likelihood of this seems low. Third, it should be kept in mind that direct analog FT4 immunoassays are usually reliable but may be suboptimal in certain settings, being influenced by abnormalities in protein binding, nonthyroidal illness, and certain drugs. Lastly, we did not measure thyroid autoimmunity, which, if it had been done, may have offered further insights. The strengths of our study include the large healthy population surveyed and the careful measures taken to minimize confounding variables.
In conclusion, FT4 levels were inversely associated with coronary artery calcification in euthyroid men. In euthyroid women, we could not establish whether there was an association between FT4 and CACS, probably because of the low prevalence of coronary calcification in women in this study. Further studies are needed to validate whether subjects with low normal FT4 levels are at a high risk for CVD with poor CV outcomes.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.