
Abstract
Background:
Thyroid remnant ablation (RA) with 30 mCi of radioactive iodine (131I) in patients thyroidectomized for treatment of low-risk differentiated thyroid carcinoma (DTC) has a success rate of 64% to 84%. Lithium increases the residence time of 131I in the thyroid tissue. The aim of this study was to determine if lithium treatment added to 30 mCi 131I would enhance the success rate of this treatment compared with 30 mCi 131I alone in patients who were thyroidectomized for treatment of low-risk DTC.
Methods:
This was a randomized study with endpoint at one year. Sixty one consecutive patients were enrolled and randomized into two groups: group A (n=32) treated with 30 mCi 131I; group B (n=29) treated with 30 mCi 131I plus an oral dose of lithium 900 mg/day, for 7 days. All patients were evaluated by whole body scan (WBS) with 123I and had serum TSH, thyroglobulin (Tg), and anti-Tg antibodies (TgAb) determined when they were hypothyroid on no thyroid hormone. Patients were reevaluated after one year with serum TSH, Tg, and TgAb determinations and WBS with 123I. The criteria for defining a successful outcome was a negative WBS and a serum Tg of <1.
Results:
Group A was composed of 28 women and four men (ages 25–71 years) with 2 having follicular thyroid carcinoma (FTC), 22 having papillary thyroid carcinoma (PTC) of 1–4.5 cm, and 8 having micro PTCs (mPTC) of 0.3–0.8 cm. Group B was composed of 26 women and 3 men (ages 20–63 years) with 3 having FTC, 15 having PTC of 1.2–3.5 cm, and 11 having mPTC of 0.2–0.8 cm. All patients had a history of a WBS after their post-therapeutic 131I dose that showed uptake in the cervical region. After one year, 22 patients from group A had a negative WBS (68.75%) and in group B, 27 patients had a negative WBS (93.1%). The successful rates for the follow-up WBS were significantly different (p=0.017). There were 19 patients in Group A in whom the initial Tg was positive. Of these, 14 had a negative follow-up Tg (73.7%). Group B had 9 patients with a positive initial Tg and all of them had a negative follow-up Tg (100%).
Conclusion:
The addition of lithium to treatment with 30 mCi 131I in thyroidectomized patients with low-risk DTC improved the efficacy of thyroid RA and therefore might be a better alternative than using higher doses of 131I for remnant ablation in these patients.
Introduction
For most of the cases of DTC a dose of radioactive iodine (131I) is administered after thyroidectomy and tumor resection to ablate thyroid remnants (remnant ablation, RA). The main reason for RA in low-risk DTC is to macroscopically destroy normal thyroid remnants to increase the specificity and the positive predictive value of the whole body scan (WBS) and serum Tg determination, methods for evaluating postsurgical persistence or recurrence of thyroid cancer. Additionally, RA may destroy microscopic foci of tumor remnants that escape surgical resection (3). The success of RA is enhanced by (i) a low-iodine diet (4), (ii) administration of a greater dose of 131I, (iii) TSH stimulation, and (iv) greater retention of the 131I dose in thyroid tissue.
The 131I dose required for RA is not well established; it varies from ∼30 to 100 mCi or more. In many regions, a dose of 30 mCi is the maximum allowed for administration to ambulatory patients who are not hospitalized in isolation after the treatment. In recent years, there have been several reports that low doses of ∼30 mCi are as efficient as 100 mCi for RA, with success rates of about 70%–80% (4 –8). However, Hackshaw et al., in a metanalysis, concluded that it is not possible to know if the success rate with these low doses of RA is similar to that obtained with high doses of ∼100 mCi (9).
It is known that lithium increases the residence time of radioactive (and stable) iodine in thyroid tissue (10,11) and it has an adjuvant action in the therapy of Basedow-Graves' (BG) disease with 131I (12,13). Two studies have demonstrated that lithium leads to an increase in the half-life of tracer doses of radioactive iodine in metastasis from DTC and in thyroid remnants in patients who have had surgery for DTC (14,15). However, to date, there are no studies of the influence of concomitant lithium administration on the efficacy of RA.
In this context, we hypothesized that lithium can have an adjuvant role in RA. The objective of this study was to evaluate, by comparing a group of patients who received 30 mCi 131I with another group that received lithium in addition to 131I for RA, if lithium improves the efficacy of RA in patients having surgery for low-risk DTC.
Methods
Patients
A total of 61 consecutive patients with low-risk DTC who had been treated with total thyroidectomy were studied. They were being followed up from January 2004 to December 2009 at the ambulatory clinic for thyroid diseases at Hospital São Paulo (Universidade Federal de São Paulo–Escola Paulista de Medicina). The inclusion criteria were tumors restricted to the thyroid, without extra-thyroid invasion according to microscopy, without lymph node involvement observed during surgery or by ultrasound (US), and without evidence of local and distant metastasis.
The protocol was approved by the Ethics Committee from Hospital São Paulo–Universidade Federal de São Paulo and all patients, after being informed, signed a document allowing their participation in the study.
Study protocol (Table 1)
All prospective patients in the study were taking L-thyroxine at the time of their first medical appointment for the study. At this time serum samples were collected for the determination of TSH, Tg, and anti-Tg antibodies (TgAb) and an US was obtained to exclude the presence of cervical adenopathy. Eligible patients were then randomly assigned to groups A and B by a simple randomization method.
WBS, whole body scan; LC, lithium carbonate.
Patients from both groups were individually oriented about the low-iodine diet they were to take. After stopping L-thyroxine treatment and taking a low-iodine diet for 30 days a screening dose of 5 mCi of 123I was administered to patients in group A. Thyroid scintigraphy, cervical uptake, and WBS-1 were performed 6 hours later. After 5 days, a blood sample was collected for TSH measurement and Tg measurement (Tg-1), and a therapeutic dose of 30 mCi 131I was administered. A new WBS image was obtained after 6 days.
The same procedures that were performed in patients in group A were performed in patients in group B. In addition, they also received an oral dose of 300 mg lithium carbonate every 8 hours for 7 days. This was started and ended respectively, 3 days before and 3 days after the administration of 30 mCi 131I. After the therapeutic dose of 30 mCi 131I, all patients were maintained on L-thyroxine at a dose sufficient to suppress serum TSH, but maintaining normal serum T4 levels.
One year after the therapeutic dose of 30 mCi 131I, all patients were reevaluated by performing a new WBS (WBS-2) with 5 mCi 123I after stopping their dose of L-thyroxine for 30 days. In addition, a cervical US and serum levels of TSH, Tg (Tg-2), and TgAb were determined. After the WBS-2, L-thyroxine was started again and the patients were followed up every 6 months at our outpatient service. RA was considered successful if there was disappearance of any visible area of uptake in the thyroid bed, cervical uptake of <1%, and no detectable serum Tg (<1 ng/mL).
Laboratory determinations
The concentration of serum TSH was measured using a third generation immunofluorimetric assay, having the sensitivity of 0.05 mL U/L, developed in our laboratory (16). The measurement of serum Tg was done using an immunofluorimetric assay (Delfia® Perkin Elmer Life and Analytical Sciences, Wallac Oy, Finland), having the sensitivity of 1.0 ng/mL. The measurement of serum TgAb was done by an immunofluorimetric assay with a functional sensitivity of 40 mU/mL. This was also developed in our laboratory (17). The concentration of serum lithium was measured by an ion-selective method.
Thyroid US
All US examinations were performed by the same professional, using the Phillips equipment, model Envision with a multifrequency linear transducer of 3–12 MHz associated to color doppler.
WBS using radioactive iodine 123 and 131
For WBS the Forte MDC (ADAC Laboratories) equipment was used and, for the planar images of the neck and mediastinum, the Tyrus camera (ADAC Laboratories) was used.
The WBS images were analyzed by two experienced professionals who did not have access to the patients' clinical data and who also did not exchange information about the image analysis either with each other or with any other person. It was their task to determine if the result was positive or negative for each image in the two moments. When there was any discrepancy, a third professional was consulted.
Statistical analysis
The statistical test used for the evaluation of the categorical data was the chi-square (χ 2 ) and, when not possible to use it, Fisher's exact test was used. The numeric variables were tested in relation to data normality, and in positive cases, groups were compared by the T-test.
A statistically significant difference was considered when p<0.05. The statistical software Minitab version 16.1 was used.
Results
The clinical characteristics (age, gender, and histological type) were similar between the groups (Table 2). In group A, 4 out of 32 patients had a negative WBS-1, but all had a postablative dose WBS positive for thyroid remnants and Tg-1 was positive in 19 cases.
PC, papillary carcinoma; PMC, papillary microcarcinoma; FC, follicular carcinoma.
In group B, 4 out of 29 patients had a negative WBS-1, all had a postablative dose WBS positive for thyroid remnants and the Tg-1 was positive in nine.
Success rate evaluated by the WBS (Fig. 1)
At the one-year endpoint, in the 32 patients in group A, 22 had a negative WBS-2 (68.75%). In the 29 patients in group B, 27 had a negative WBS-2 (93.1%). The percentage of patients that had successful ablation was significantly higher in group B than in group A (p=0.017). When the eight patients (four in each group) with negative WBS-1 were removed from the analysis, the successful RA was also significantly higher in group B (92%) than in group A (64.2%, p=0.022).
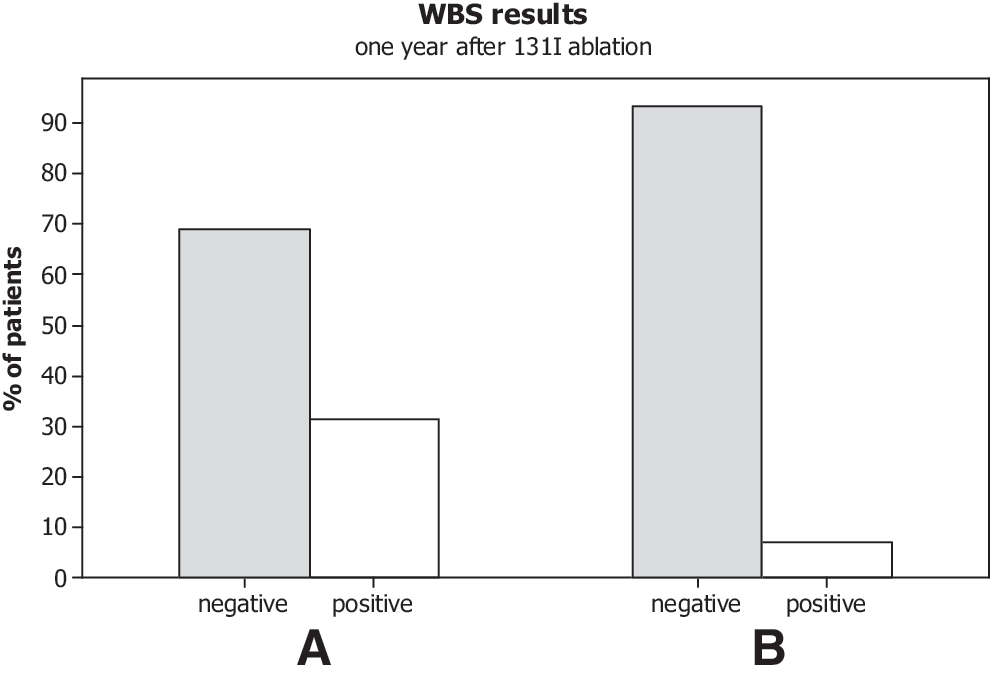
Success rate of RA (%) evaluated by WBS-2 in patients from group A and B. RA, remnant ablation; WBS, whole body scan.
Success rate evaluated by Tg (Fig. 2)
Of the 19 patients in group A with a positive Tg-1, 14 had a negative Tg-2 (73.7%) after one year. Of the 9 patients of group B with positive Tg-1, all of them had a negative Tg-2 (100%). This difference was not statistically significant (p=0.14). Tg levels, TgAb, and WBS-2 of positive Tg-1 patients are shown in Tables 3 and 4. Of the 33 patients with indetectable Tg-1 levels, four had a positive TgAb test (one in group A and three in group B).
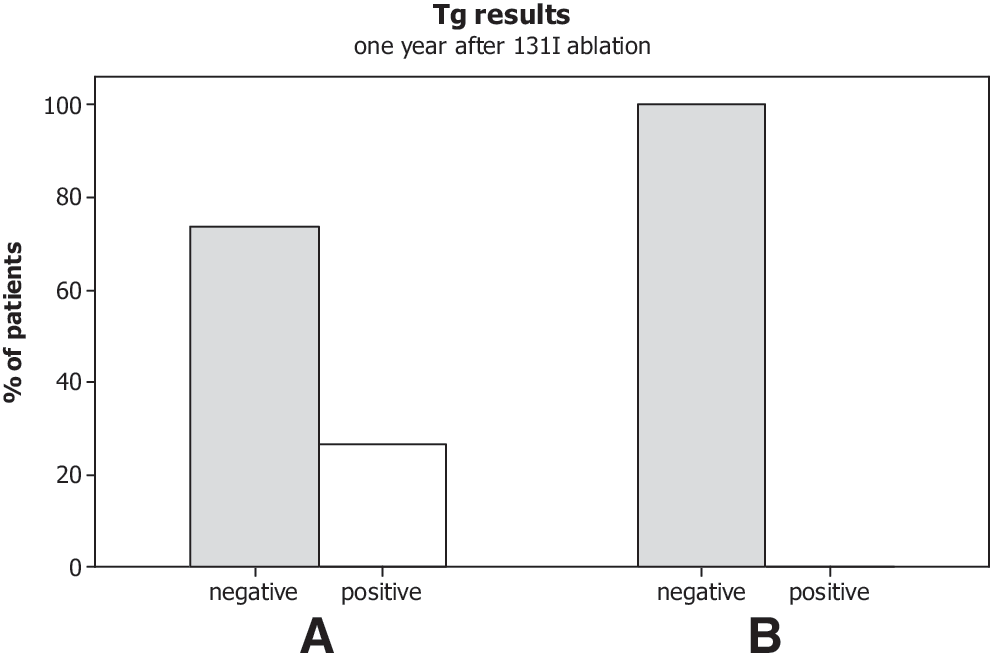
Success rate of RA (%) evaluated by Tg-2 for patients who showed a positive Tg-1 in groups A and B.
Pos, positive; Neg, negative.
The serum lithium concentration was determined for 19 patients in group B and ranged from 0.09 to 1.77 mEq/L (0.52±0.47). Therapeutic lithium concentrations for psychiatric patients range from 0.6 to 1.2 mEq/L. Ten patients (52.6%) had lithium levels below 0.6 mEq/L, eight patients (42.1%) had levels ranging from 0.6 to 1.2 mEq/L, and one patient (5.2%) had a serum lithium level greater than 1.2 mEq/L.
We did not observe any complication or serious adverse effect in any of the patients from group B, the lithium-treated group. One of the patients had dizziness and malaise, which was controlled with oral hydration and oral dimenhydrinate, 50 mg every 8 hours for 2 days, without the need for hospitalization. This last patient had a serum lithium concentration of 1.77 mEq/L.
Discussion
The goal of RA with 131I, when performed after the thyroidectomy to obtain surgical removal of DTC, is to destroy normal thyroid tissue that was not removed by thyroidectomy so as to obtain greater specificity for the followup tests, namely WBS and serum Tg, to detect persistence or recurrence of thyroid cancer. Another goal is to destroy microscopic foci of DTC that were not detected by WBS or other image methods (3).
There are controversies regarding RA using 131I, some studies considering it a procedure that decreases the recurrence rate after DTC (2,18) and others not showing benefits, mainly in low-risk cases (1,19). However, RA is still widely performed for low-risk DTC, if only to enhance followup procedures but removing normal thyroid tissue that would compete with cancer tissue in WBSs and potentially act as a misleading source of serum Tg.
It is to be expected that the likelihood of RA would be influenced by the duration of residence of the administered 131I in the thyroid tissue (15,20). It has been noted that oral lithium carbonate increases iodine retention in the thyroid and acutely decreases the release of the thyroid hormone in euthyroid and thyrotoxic patients (10,11).
Lithium also increases the retention of 131I in DTC metastasis (14,15,21,22) and in thyroid tissue remnants as confirmed, in small groups of patients, by Pòns et al. and Koong et al. (14,15).
In the present study, our objective was to verify if lithium could be used as an adjuvant for RA in patients having surgery for low-risk DTC, comparing a group that received 30mCi 131I (group A) and another in which lithium was administered in conjunction with 30 mCi 131I therapy (to group B). Patients in group A had a success rate for RA of 68.75%, in accordance with other reports in the literature, where the rate varied 64% to 84% (5,7 –12) using the 30 mCi 131I dose to hypothyroid patients. In contrast, the lithium-treated group (Group B) had a success rate of 93.1%. This was significantly greater than that noted in Group A (p=0.017). Even after excluding the eight patients with a negative WBS-1, the success rate of RA with lithium was significantly higher than in the group that did not receive lithium (p=0.022).
To date, there are no comparative randomized trials similar to ours. Barbaro et al. showed that the reduction of the iodine pool by the removal of L-thyroxine and by the use of furosemide had significant effect on the success rate of RA, but lithium did not change this rate. This finding was attributed by the author to the low dose (450 mg/day for 3 days) of lithium carbonate used (23). A double-blind, multicenter study titled “The Effects of Lithium Carbonate on Low Dose Radioiodine Ablation in Early Thyroid Cancer Treatment” is now in phase II in the United States, but it has not been published (information available at
Within our case set, only one patient had relatively mild symptoms, including dizziness and malaise. This favorably responded to oral rehydration and oral dimenhydrinate with hospitalization not being required. In this regard, Bogazzi did not note any significant adverse effects in patients who received lithium (900 mg/day for 12 days) as an adjuvant for 131I therapy for BG disease (13).
The mechanism of action of lithium in the thyrocyte is not well known. One of the hypotheses is that it inhibits adenylate cyclase and blocks the translocation of the thyroid hormone mediated by cyclic adenosine monophosphate, the latter being responsible for the inhibition of thyroid hormone release (24).
With regard to using serum Tg measurements to assess the success of RA, we noted a success rate of 73.7% for the group that did not receive lithium and 100% for the group that received lithium. This difference appears impressive but was not significant, probably because the power of the study was not sufficient.
In conclusion, lithium can be used as an adjuvant in RA with 30 mCi of 131I in patients who have had thyroidectomy for low-risk DTC. This may be an acceptable alternative to administering higher doses of 131I in an effort to enhance the success rate of this relatively low dose.
Footnotes
Disclosure Statement
The authors declare that no competing finantial interests exist.