
Abstract
Background:
Endoscopic thyroidectomy is gaining popularity, particularly in Asian countries, as an alternative to conventional cervical thyroidectomy. Multiple large case series have been published that confirm the feasibility and safety of this procedure compared to conventional methods. However, no data are available that demonstrate long-term oncologic outcomes or complications.
Patient Findings:
A patient who underwent transaxillary gas insufflation thyroidectomy for a follicular neoplasm presented to the authors with a mass along the operative tract 31 months after her first surgery. The mass was found to be a recurrence of the thyroid neoplasm.
Summary:
Since this is a relatively new procedure, the potential complications differ from those of conventional cervical thyroidectomy. Further studies are needed to determine size limitations on nodules considered for endoscopic resection.
Conclusion:
When performing these procedures, care should be taken to ensure that the specimen is removed entirely and in one piece. Long-term outcomes data for endoscopic thyroidectomy are warranted prior to this becoming an acceptable standard of care for thyroid surgery.
Introduction
Thyroidectomies have classically been performed through a cervical incision. Recently, endoscopic techniques have been introduced for thyroidectomy that utilize either a direct or remote approach (Fig. 1) (5). Direct techniques involve placement of access ports in the cervical region. Remote techniques, such as the transaxillary or bilateral breast areola and ipsilateral axillary (BBIA), utilize various combinations of axillary, breast, and anterior chest access ports to tunnel along fascial planes and visualize the thyroid bed (6 –9). These techniques avoid a neck incision allowing for improved cosmesis. Furthermore, robotic and “gasless” remote techniques are additional variants that are currently being used with reportedly good results by some highly experienced centers (10,11).
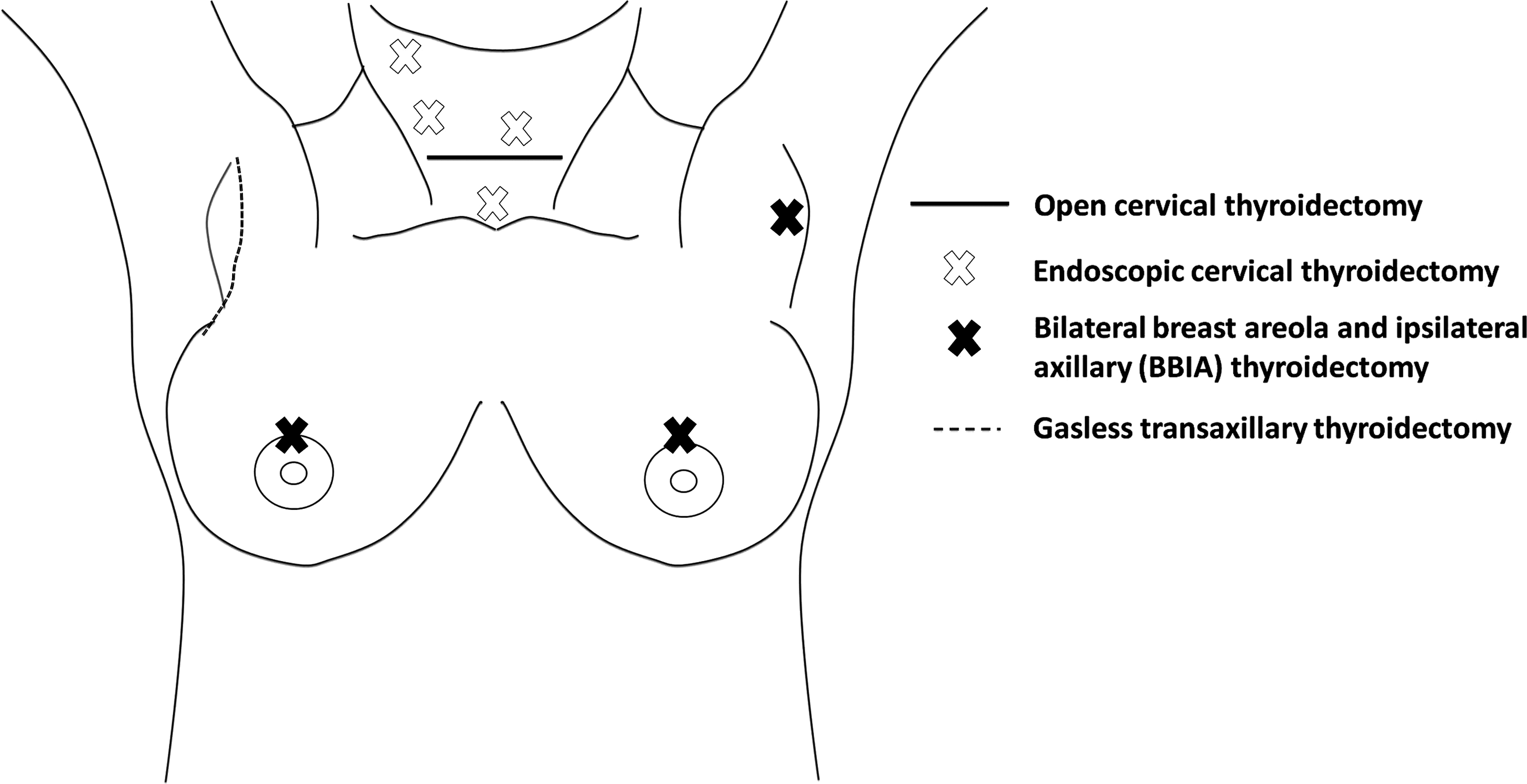
Diagram showing common locations for incision and port placements for traditional open and endoscopic thyroidectomy.
Several groups have shown that endoscopic thyroidectomies provide similar oncologic resections and perioperative complication rates compared with conventional open thyroidectomies (12 –14). However, since these procedures are relatively new, there are no studies available that have documented the long-term outcomes and complications for resection of both benign and malignant disease.
Here we present a patient who presented with tumor recurrence in the operative bed 31 months after undergoing an endoscopic transaxillary gas insufflation hemithyroidectomy for a follicular neoplasm.
Patient
A 31-year-old woman presented to a tertiary referral center for evaluation of a palpable nodule on the right anterior chest wall. Three years prior, she sought evaluation at an outside institution for two nodules in the right lobe of the thyroid and one nodule in the left lobe. Records from the outside institution were obtained and revealed the following details about her presentation, evaluation, and treatment. She denied dysphagia, dysphonia, or hoarseness at the time of presentation and had no history of radiation or prior thyroid disease. Physical exam revealed a soft midpole nodule in the right thyroid lobe and a normal thyroid gland on the left with no cervical lymphadenopathy. Thyroid function studies including serum thyrotropin (TSH), triiodothyronine (T3), and free thyroxine (fT4) were normal. Ultrasound revealed a 2.6-cm heterogeneous nodule in the midpole of the right thyroid lobe, a 1.6-cm nodule in the right upper pole, and a 0.5-cm nodule in the left lobe of the thyroid. FNA of both the 2.6-cm and 1.6-cm nodules revealed follicular cells with Hürthle cells present. The 0.5-cm left lobe nodule was not biopsied.
The patient elected to undergo an endoscopic gas insufflation transaxillary right hemithyroidectomy. Three incisions were made along the mid-axillary line on the right for trocar placement. The pectoralis fascia was elevated from lateral to medial until the sternocleidomastoid and thyroid bed were visualized. The dissection was carried out from the inferior pole to the superior pole of the thyroid and care was taken to preserve the recurrent laryngeal nerve and parathyroid glands. A 3-cm smooth-surfaced nodule in the right lobe of the thyroid was identified. Due to the mass effect of the nodule, the right lobe was divided into two pieces that were removed separately. Of note, no endoscopic retrieval bag was used when removing the specimen. She did well postoperatively and made an unremarkable recovery.
The specimen on final pathology revealed a dominant 3.4-cm thinly encapsulated nodule. The nodule lacked any significant cytologic atypia and lacked the nuclear features of papillary thyroid carcinoma. The entire capsule was evaluated and there was no evidence of capsular or vascular invasion consistent with the diagnosis of follicular adenoma. The remaining thyroid showed nodular hyperplasia. An endocrine pathologist at our institution who confirmed the above outside pathologic diagnosis reviewed the entire case.
Thirty-one months after her first surgery, she presented to our clinic with a palpable nodule in the anterior chest below the clavicle along the tract of the prior transaxillary gas insufflation hemithyroidectomy. The nodule was noted to be 1–2 cm in size and nontender and was freely mobile on the right anterior chest wall. Since she had not received any follow-up imaging of the left thyroid lobe nodule, repeat ultrasound revealed slight enlargement to 0.9 by 0.6 by 0.7 cm.
The patient underwent an excisional biopsy of the right anterior chest wall mass and ultrasound-guided FNA of the left thyroid nodule. The anterior chest mass was adherent to the underlying tissue and was excised en bloc with the surrounding tissue. She did well postoperatively and had an uneventful recovery.
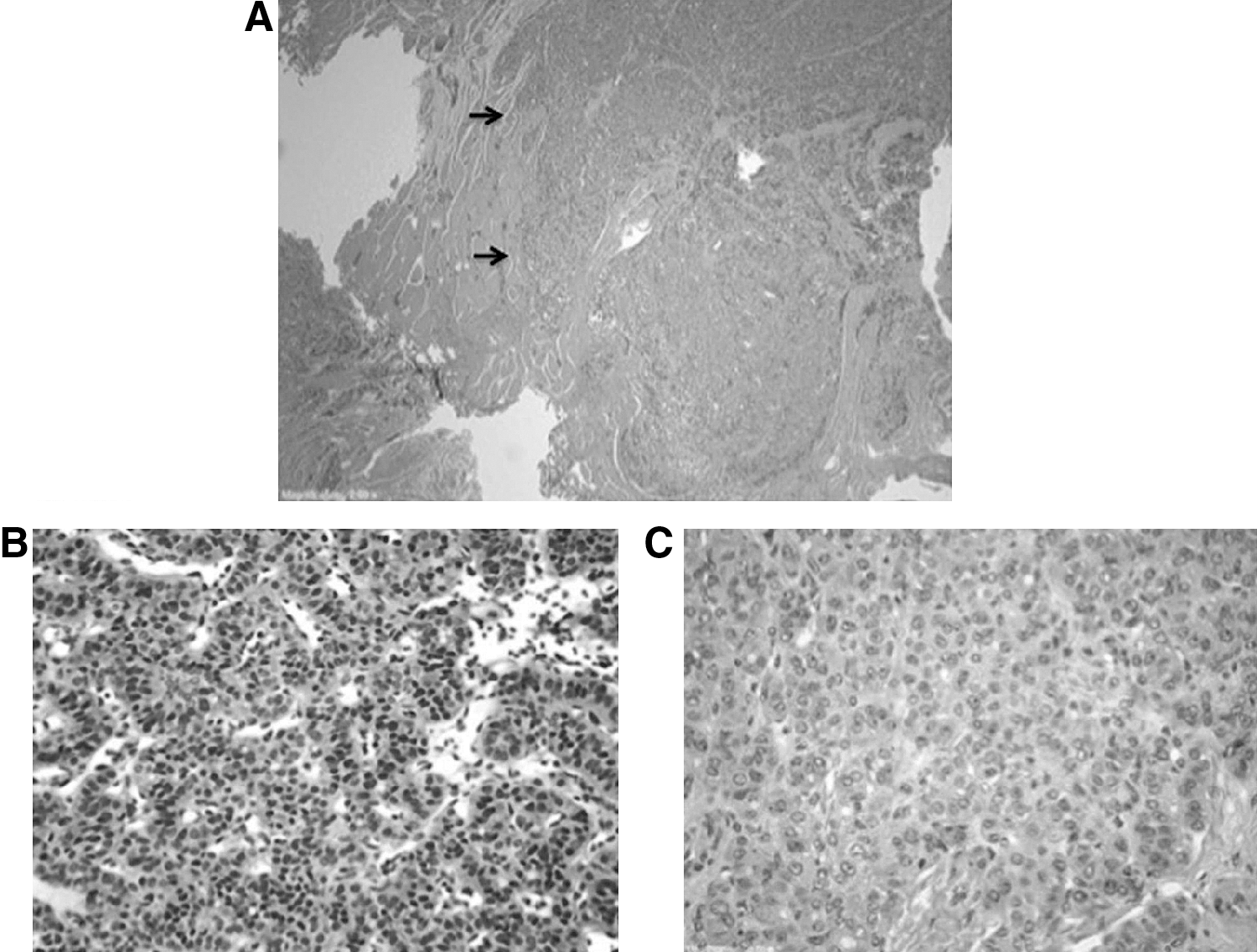
On final pathology, the chest wall specimen showed a follicular patterned lesion infiltrating adjacent fibromuscular tissue (Fig. 2A). The tumor cells showed diffuse staining for thyroglobulin and TTF-1, confirming thyroid origin of the tissue. The current lesion was compared to the pathology of the previous hemithyroidectomy specimen and was histologically similar (Figs. 2B, 2C). Immunohistochemical stains for HBME-1 and Galectin-3 were negative and CK19 was focally positive. A Ki-67 immunostain showed a low proliferation index (<5%). Based on the histologic and immunohistochemical findings, the lesion was regarded as a low-grade thyroid neoplasm most consistent with displaced follicular adenoma from the previous surgery. The FNA of the left-sided nodule was consistent with a follicular neoplasm.
Discussion
Transaxillary thyroidectomy has been established as a common technique at several large-volume centers in Asia that perform over 100 endoscopic or robotic thyroidectomies for thyroid cancer each year (10,14,15). The complication rates of these groups are comparable to conventional cervical thyroidectomy (<1% risk of permanent recurrent laryngeal nerve injury, <1% risk of hematoma) (10). However, this technique also carries the unique risks of brachial plexus injury, Horner's syndrome, and chyle leaks, each of which have been reported to occur in <1% of cases (10,13,15). This case documents an additional risk—that of tract recurrence following transaxillary thyroidectomy.
There are two previously reported cases of tract site recurrence following endoscopic thyroidectomy utilizing a breast approach (16,17). The first case occurred in a 25-year-old woman who underwent a BBIA endoscopic hemithyroidectomy for initially benign adenomatous hyperplasia but returned 14 months later with multiple sites of low-grade papillary thyroid cancer along the thyroid bed and anterior chest tracts. The second case involved a 61-year-old woman who also underwent a BBIA endoscopic hemithyroidectomy for a follicular adenoma and returned 31 months later with several large, hard masses at the sternal, anterior neck, and anterior chest wall subcutaneous tunnels made during the previous operation. All of these masses were excised and were determined to be either follicular carcinoma or papillary carcinoma on final pathology.
Port-site recurrence has been known to occur infrequently following laparoscopic abdominal surgeries for other common cancers such as colorectal, kidney, and prostate cancers (18,19). The cause of these events is probably multifactorial but appears to be related to intraoperative details such as the extent of tumor manipulation, the use of tumor morcellation to facilitate extraction, the method of specimen removal, or the use of pneumoperitoneum and the potential for a “chimney effect” (20). Fortunately, as the collective experience with laparoscopic techniques has increased, the risk of incisional implantation has decreased and now is considered equivalent to that of open surgery (18,21 –23).
In laparoscopic surgery for cancer of the colon and rectum, multiple prospective trials have shown no difference in long-term outcomes in regards to oncologic adequacy of resection, recurrence, and disease-free survival (18,23). Because of its recent adoption, there are not yet any studies evaluating long-term oncologic outcomes of endoscopic and robotic surgery for thyroid cancer. Since recurrence in thyroid cancer can occur 20 years after surgery and there are so few centers performing large numbers of endoscopic thyroidectomies, it will likely be many years before prospective long-term outcomes data are available.
Although there are no universally recognized size criteria for performing transaxillary thyroidectomy, some centers advocate a size restriction of no larger than 5.0 cm for follicular neoplasms and no larger than 2.0 cm for FNA-confirmed well-differentiated thyroid carcinomas (10,13). A potential cause of tract seeding in this patient could have been that the thyroid lobe had to be divided intraoperatively and removed piecemeal. Furthermore, the use of gas insufflation or even the lack of use of an endoscopic retrieval bag may have contributed to tract seeding, although to date there are no trials that have investigated either in endoscopic thyroidectomies.
Interestingly, the operative tract recurrence identified here occurred following excision of a presumably benign follicular adenoma. Determining the true nature of the recurrence, however, presents a unique challenge. The chest-wall lesion had similar histologic features when compared with the original follicular adenoma and did not have any characteristic findings expected in papillary thyroid cancer such as nuclear grooves, intranuclear inclusions, and psammoma bodies. In this case evaluation of the classic histologic features required to diagnose malignancy in a thyroid follicular neoplasm (the presence of capsular/vascular invasion) were not possible. Therefore, it is very difficult to know whether the observed infiltration into the surrounding fibromuscular tissue truly represents an indication of malignancy.
In conclusion, while transaxillary procedures are at the forefront for advancements in surgical technique, one must always keep in mind that new methods may bring unforeseen complications. Although several authors have demonstrated the safety and feasibility of transaxillary thyroidectomies, there remains little information on long-term outcomes. Even in surgery for benign lesions, every effort should be made to remove the specimen entirely and in one piece, and to potentially utilize an extraction device to help avoid operative site seeding. Using gasless techniques versus insufflation may also minimize the risk of seeding. Further studies are also needed to help develop standardized limitations for lesion size when utilizing these techniques. Ultimately, long-term outcomes data for endoscopic thyroidectomy are warranted prior to this becoming an acceptable standard of care for thyroid surgery.
Footnotes
Acknowledgment
The authors received grant support from the Dancers Care Foundation.
Disclosure Statement
No competing financial interests exist.