
Abstract
Background:
The pyramidal lobe is an accessory lobe of the thyroid gland. The prevalence of the pyramidal lobe in thyroid glands and its features have been studied in autopsy series but there is little information regarding its parameters in patients or normal subjects. The purpose of the current study was to assess the frequency, location, and size of the pyramidal lobe using computed tomography (CT) of the neck.
Methods:
From January to December 2010, 327 patients who underwent neck CT for trauma, thyroid cancer, pharyngolaryngeal malignancy, a palpable neck mass, cervical lymphadenopathy, and vocal cord paralysis were enrolled in the study. Their neck CTs were retrospectively analyzed by a single radiologist. Small pyramidal lobes (<9 mm) were not included in the study.
Results:
A pyramidal lobe was present in 41.3% (135/327) of the patients; some pyramidal lobes showed complete separation from the thyroid gland (12.6%, 17/135). There was no difference in the frequency of pyramidal lobe detection by gender (p>0.05, Fisher's exact test). The pyramidal lobe predominantly originated from the left thyroid gland in 54.1% (73/135) of patients. There were two patients in whom the pyramidal lobe was located bilaterally (one case from both the right and left sides of the thyroid gland and one case from the left side and midline of the thyroid gland). The average length and volume of the pyramidal lobes were 25.0 mm and 129.4 mm3, respectively. The upper margin of the pyramidal lobe was most commonly located at the level of the thyroid cartilage.
Conclusion:
The prevalence of the pyramidal lobe in the left lobe of the thyroid gland is somewhat greater than 50% using the criteria employed in this study. Neck CT is useful for detecting the presence, size, configuration, and location of the pyramidal lobe.
Introduction
The pyramidal lobe is an accessory lobe of the thyroid gland and has been reported to be present in various frequencies from 15% to 75% in previous studies that were performed on cadavers (7 –12). Studies in patients or healthy populations regarding the prevalence or size of the pyramidal lobe have not been performed using computed tomography (CT). Pyramidal lobes separated from the main thyroid gland have the greatest potential to remain after total thyroidectomy because surgeons remove the thyroid gland based on visual inspection. Remnant pyramidal lobes can be an undesirable target for RI ablation and may be the focus of recurrence (13). Therefore, the purpose of this study was to assess the presence, location, size, and the upper end of the pyramidal lobe in randomized patients undergoing neck CT.
Materials and Methods
Patients
This study was approved by the Institutional Review Board (IRB) before subject selection began (IRB: 11-090). From January 2010 to December 2010, CT scans of the neck were performed in 1015 patients (513 women and 502 men; age 13–91 years; average age, 44.5 years) in our hospital. Exclusion factors for this study included neck CT showing previous thyroidectomy or other neck operations, inappropriate CT protocol, or poor image quality. Ultimately, 327 patients (221 women and 106 men; age 19–82 years; average age, 51.0 years) were enrolled in this study. The patients underwent neck CT for the following reasons: trauma (n=1), thyroid malignancy (n=180), pharyngolaryngeal malignancy (n=36), palpable neck mass (n=54), cervical lymphadenopathy (n=44), and vocal cord palsy (n=12).
Neck CT scanning
Neck CT scans were conducted using contrast medium (slice thickness, 3 mm; reconstruction increment, 3 mm) using a 64-channel multidetector CT scanner (Aquilion One; Toshiba Medical Systems, Otawara, Japan) or a 128-channel multidetector CT scanner (LightSpeed; General Electric Medical Systems, Milwaukee, WI). Nonenhanced axial, contrast-enhanced axial, and contrast-enhanced coronal reformatted CT images were acquired in all cases.
Image analysis
Using a picture archiving and communication system, image analysis was carried out by a single radiologist (Dong Wook Kim) with 9 years of experience in head and neck CT interpretation. In the neck CT, the pyramidal lobe was defined as longitudinally arranged thyroid tissue protruding from the upper margin of the thyroid gland proper on three or more serial axial images. Superficial cervical veins can be differentiated from the pyramidal lobe because they show greater longitudinal arrangement, uniform size, small diameter, and different attenuation than the thyroid gland in the neck CT (Fig. 1). As a result, small pyramidal lobes less than 9 mm in length were not included in this study. However, differentiation between Delphian node and the pyramidal lobe is not difficult in the neck CT because Delphian node shows a short segment, bean or ovoid shape, low attenuation, and mild enhancement in comparison to the pyramidal lobe. The location of the pyramidal lobe was classified in accordance with its origin, for example, right, left, midline, or bilateral. The volume of the pyramidal lobe was calculated using an ellipsoid formula, length×anteroposterior diameter×transverse diameter×0.52. The pyramidal lobe was classified into four categories according to the location of the upper end: tongue base, hyoid bone, thyrohyoid membrane, and thyroid cartilage. The separation of the pyramidal lobe was considered to be nonvisualization of the pyramidal lobe on one or more axial images between the pyramidal lobe and main thyroid gland. The presence, location, length, volume, and upper end of the pyramidal lobe and its separation or continuity with the main thyroid gland were investigated. In addition, the anteroposterior diameter of the main thyroid (i.e., the mean of the largest anteroposterior diameter measured at both thyroid lobes) was measured.
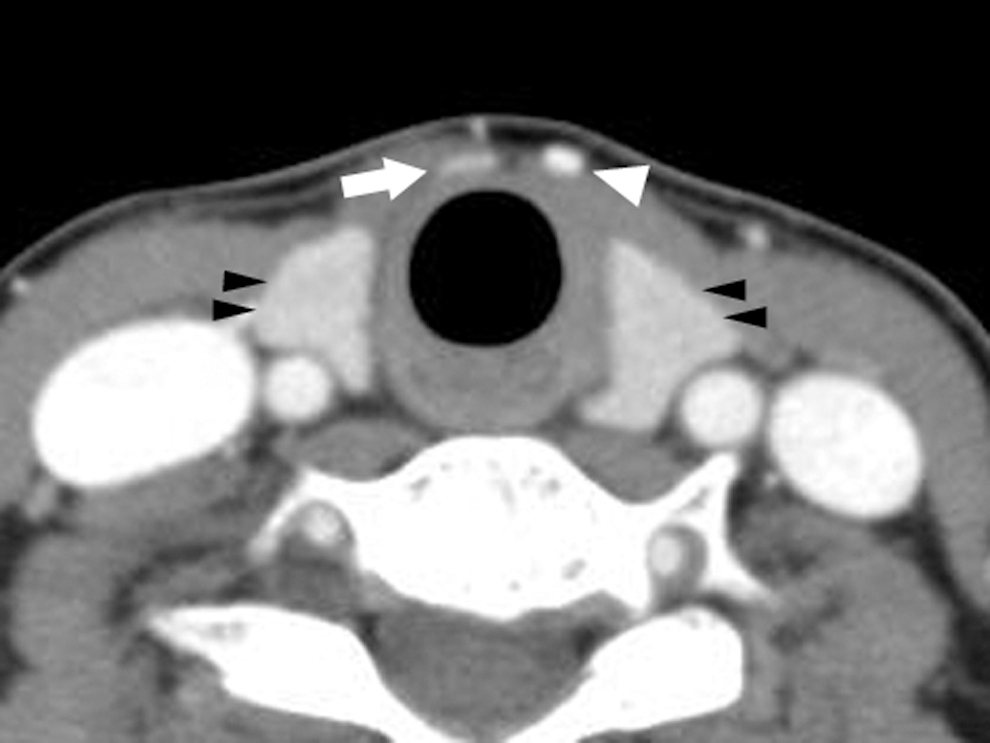
Computed tomography (CT) differentiation between the pyramidal lobe and superficial cervical vein. While the pyramidal lobe (arrow) shows the same enhancement with the main thyroid gland (black arrowheads) at contrast-enhanced axial CT image, superficial cervical vein (white arrowhead) shows uniform size and strong enhancement like internal jugular vein.
Statistical analysis
All data were compared using Fisher's exact test, chi-square test, or t-test and p<0.05 was considered statistically significant. Statistical analyses were performed using SPSS for Windows (version 17.0.1; SPSS, Inc., Chicago, IL).
Results
Data for patient age, and the presence, location, and separation or continuity of the pyramidal lobe are summarized in Table 1. The pyramidal lobe was observed in 135 patients (99 women and 36 men; age 19–82 years; average age, 49.9 years) with 41.3% frequency (35/106 men, 100/221 women) (Fig. 2), and there was no difference in the frequency or patient age of pyramidal lobe detection between the men and women (p>0.05, Fisher's exact test). The patients with a pyramidal lobe underwent neck CT for the following reasons: trauma (n=0), thyroid malignancy (n=77), pharyngolaryngeal malignancy (n=21), palpable neck mass (n=24), cervical lymphadenopathy (n=11), and vocal cord palsy (n=2). Significant differences were not found in the prevalence of the pyramidal lobe among the groups with different clinical reasons for neck CT scanning (p>0.05, chi-square test). In seven patients, differentiation between the pyramidal lobe and the superficial cervical vein on neck CT was difficult because of its thin caliber, longitudinal arrangement with termination in the main thyroid and infrahyoid neck, and similar attenuation to the thyroid gland; these cases were interpreted as absence of the pyramidal lobe. The locations of the pyramidal lobes were right (n=34), midline (n=26), left (n=73), right/left (n=1), and midline/left (n=1). Pyramidal lobes originating from the left side of the thyroid were most common, and the difference was statistically significant (p<0.05, Fisher's exact test). The number of pyramidal lobes showing separation from the main thyroid gland was 17 (2 men, 15 women) and the remaining cases (n=118) showed continuity with the main thyroid gland (34 men, 84 women); there was no difference in continuity or separation of the thyroid gland between men and women (p>0.05, Fisher's exact test).
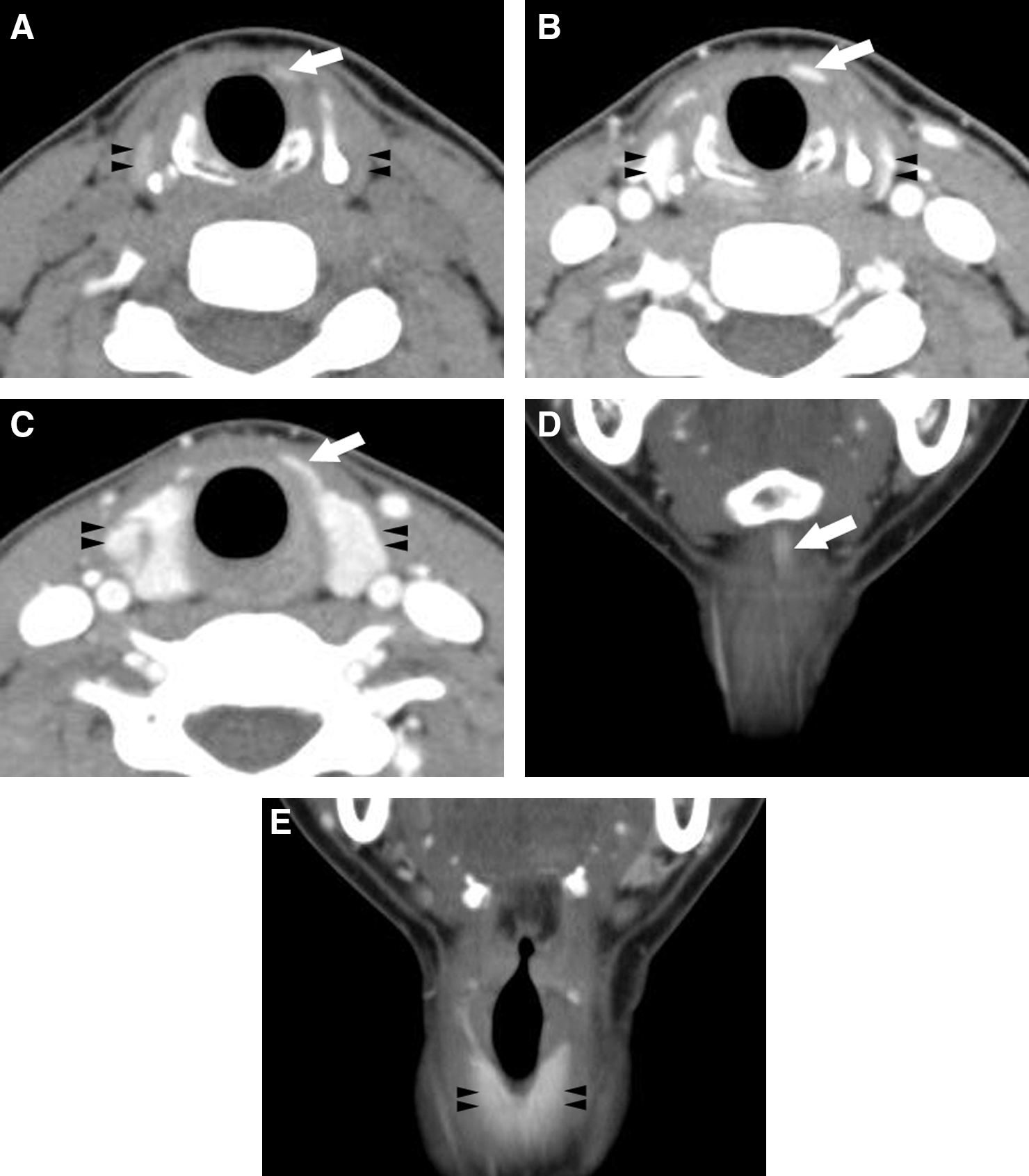
Thirty-one-year-old woman with a left pyramidal lobe.
Data for the size and upper end of the pyramidal lobe are summarized in Table 2. The average length was 25.0 mm, 24.3 mm in women and 26.0 mm in men, with no difference between the genders (p>0.05, Fisher's exact test). The average volume of the pyramidal lobe was 129.4 mm3. The volume was 142.7 mm3 for women and 92.9 mm3 for men; this difference was statistically significant (p<0.05, Fisher's exact test). The levels of the upper end of the pyramidal lobes were 23 at the hyoid bone, 1 at the tongue base, 43 at the thyrohyoid membrane, and 68 at the thyroid cartilage. There were no differences in the location of the upper end between genders (p>0.05, Fisher's exact test). Ectopic thyroid was not observed in this study.
Data presented in parentheses are the percentage of each item.
p Value in each item is difference between men and women.
The anteroposterior diameter of the main thyroid was measured in contrast-enhanced axial CT, but an increase in the anteroposterior diameter due to thyroid nodules was excluded. The mean anteroposterior diameter of the main thyroid in patients with and in those without a pyramidal lobe was 19.7 mm (range, 11.2–34.1 mm; standard deviation, 3.69 mm) and 19.3 mm (range, 11.9–31.8 mm; standard deviation, 3.51 mm), respectively. There was no difference in the anteroposterior diameter of the main thyroid between patients with and those without a pyramidal lobe (p>0.05, t-test).
Discussion
The thyroid gland is an important endocrine organ, located in the frontal and inferior cervical area between the fifth cervical vertebra and the second thoracic vertebra. Among the anatomical anomalies or variants of the thyroid gland, there are ectopic thyroids, pyramidal lobes, accessory thyroids, and retrotracheal extensions. The thyroid gland has around 120 Hounsfield units in CT scans due to its high iodine concentration, which can be affected by diverse conditions such as Graves' disease, Hashimoto thyroiditis, adenoma, or malignancy (14). The pyramidal lobe reflects the inferior part of the thyroglossal duct, which is formed during the descent of the thyroid diverticulum from the floor of the pharynx (15,16).
The frequency of pyramidal lobe existence has been reported to vary from 15% to 75% (7 –12). In previous studies that were not based on a radiological modality, it has been reported that most pyramidal lobes were attached to the left side of the isthmus and reached the level of the hyoid bone (12,15,17). In the current study, the pyramidal lobe was observed in 41.3% of the patients, was somewhat more common in the left thyroid gland (54.1%, 73/135), and was separated from the main thyroid gland in 12.6% of the cases. In two cases, the pyramidal lobe originated bilaterally from the thyroid gland (2/135, 1.5%). The bilaterality rate of the pyramidal lobe in this study was lower than those in previous reports obtained anatomically on cadavers, ranging from 3.3% to 10% (9 –11). The low bilaterality rate in this study maybe related to the inclusion criteria that small pyramidal lobes less than 9 mm in length were excluded. The average length and volume of the pyramidal lobe were 25.0 mm and 129.4 mm3, respectively, indicating that a pyramidal lobe may be difficult to detect in routine ultrasonography without significant attention. The upper end of the pyramidal lobe most commonly terminated at the level of the thyroid cartilage (50.4%, 68/135). Although removal of a pyramidal lobe at the level of the thyroid cartilage during total thyroidectomy is generally possible, a higher or separated pyramidal lobe may remain after a routine thyroidectomy.
In preoperative evaluation of the thyroid gland, neck CT is valuable in identifying the presence of calcification, cysts, necrosis, or hemorrhage of the nodules; in determining the margin of the lesion and invasion to adjacent organs; and in assessing lymph node metastasis to the neck or mediastinum (18). When lymph node metastases are suspected at preoperative ultrasonography, neck CT, or cytology in a patient with thyroid cancer, total thyroidectomy with extensive lymph node dissection is mandatory. However, total or partial thyroidectomy without lymph node dissection is performed according to the patient's tumor staging or risk factors when lymph node metastases are not detected at preoperative image or cytology. If lymph node metastases are identified or the patient belongs to a high-risk group in the latter situation, postoperative RI ablation is subsequently performed (19). RI ablation therapy is more efficient when remnant thyroid tissue is minimal or absent because the radioisotope has a higher affinity for normal thyroid cells than for malignant cells (6). Therefore, surgeons try to remove all normal thyroid tissue when performing a total thyroidectomy if this is to be followed by RA ablation. However, significant thyroid tissue, such as a pyramidal lobe, ectopic thyroid, or other variants, may remain without proper preoperative evaluation, such as a neck CT. Therefore, determining the presence and location of pyramidal lobes, ectopic thyroid, or other variants may be necessary in patients with thyroid cancer and this can be accomplished with preoperative neck CT.
There are several limitations to our study. First, patients underwent neck CT scanning for various reasons, including head and neck abnormalities; thus, they do not represent the general population. Furthermore, young patients less than 18 years old were not included in this study and neck CT images were analyzed by a single radiologist. Therefore, large-scale multicenter studies are recommended. CT was the only one used in this study and the results of neck CT were not compared to other modalities such as ultrasonography. Finally, a neck CT protocol involving 3-mm slice thicknesses was employed in this study, although a more accurate analysis may have been possible with lesser slice thicknesses.
In conclusion, our study indicates a high prevalence of the pyramidal lobe in thyroid glands and the usefulness of preoperative neck CT in the detection and characterization of the pyramidal lobe.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.