
Abstract
Background:
Hürthle cell carcinoma (HCC) is regarded as an aggressive variant of follicular thyroid carcinoma based in part on its propensity to metastasize regionally and recur locally. The current treatment recommendation of formal regional lymph node dissection is largely based on the presumption of lymphatic dissemination to cervical lymph nodes as the main mechanism of regional spread. The purpose of this study was to better define the distribution of locoregional recurrence in HCC, and specifically to differentiate soft-tissue implants from true nodal metastases.
Methods:
The surgical pathology files of The Johns Hopkins Hospital were searched for cases of HCC with locoregional recurrences. The slides were reviewed to assess the histologic patterns of tumor spread, including the presence or absence of lymph node metastasis. Elastic staining was used to confirm vessel invasion.
Results:
Twenty-four cases from 19 patients were identified. Thirteen were men, and the patients ranged in age from 35 to 83 years (mean 66). All had total or near-total thyroidectomies, and 16 received postoperative radioactive iodine. The time from primary diagnosis to first recurrence ranged from 0 to 12 years (mean 5 years). The locoregional disease involved the lateral neck (n=16), central neck (n=18), and larynx/trachea (n=4). In all 24 cases, the dominant tumor nodule was present as a rounded nodule of carcinoma within the soft tissues and unassociated with lymphoid tissue. Of 22 cases evaluated by elastic staining, 13 had tumor nodules within veins. True lymph node metastases were present in only six (25%) cases, and in all but one case, the lymph node metastases were <0.5 cm.
Conclusions:
When HCC spreads in the neck, it usually does so as soft-tissue implants likely resulting from spread within venous channels. True lymph node metastases are not a major source of nodular recurrences in the neck. Resolving the pattern of tumor spread could help guide and refine the management of locoregional recurrence for patients with HCC.
Introduction
For patients with differentiated thyroid carcinoma where surgery is elected for the removal of locoregional metastases, the American Thyroid Association currently recommends comprehensive compartmental lymph node dissections rather than limited targeted removal of a tumor nodule (i.e., berry picking) (15,16). This recommendation was validated by a large experience with PTCs showing that (i) cervical lymph nodes are by far the most common site of recurrent disease, (ii) these cervical lymph node metastases are often more extensive than can be appreciated from imaging studies alone, frequently involving multiple lymph nodes in a lymph node chain (17 –19), and (iii) surgical clearance of a lymph node compartment with metastatic carcinoma can improve clinical outcomes and facilitate long-term follow-up (20).
While these observations have guided important therapeutic decisions for all patients with differentiated thyroid carcinomas, the conventional pattern of locoregional spread to cervical lymph nodes via a lymphatic plexus is more presumed than verified when it comes to HCC. The purpose of this study was to better define the pattern and distribution of locoregional spread of HCC. Potentially, a clear distinction between soft-tissue implants and true nodal metastases could help refine the surgical approach to locoregional recurrences.
Methods
Study approval was obtained from The Johns Hopkins Medical Institutions Internal Review Board. The electronic surgical pathology files of the Johns Hopkins Hospital were reviewed for all cases of HCC resected between 1985 and 2010. The term “hurthle cell carcinoma” was used as the diagnostic search term to identify all potential cases. The medical records including the surgical pathology reports were then reviewed to identify all cases of HCC that developed local and/or regional spread. The histologic slides were reviewed to confirm the diagnosis and to document the pattern of extra-thyroidal spread to the neck. Specifically, we noted the location of the HCC with respect to lymph nodes, blood vessels, and soft tissues, and the pattern of invasion (e.g., nodular vs. infiltrative). Elastic staining (Verhoeff's Van Gieson) was also performed to aid in the identification of blood vessels distended and obliterated by intra-luminal tumor nodules. Medical records were reviewed to document patient age, gender, clinical course, and treatment (e.g., nature and extent of thyroid surgery, surgical management of the neck, and use of radioactive iodine).
Results
Sixty-one primary HCCs were diagnosed at The Johns Hopkins Hospital from 1985 to 2010. The diagnosis of malignancy was based on the presence of tumor invasion into the tumor capsule and the presence of vascular invasion of intracapsular blood vessels. Three (5%) patients had histologically confirmed locoregional spread. In addition, we identified 16 patients with recurrent HCC in the neck whose primary HCC had been diagnosed elsewhere. These 19 patients underwent a total of 24 resections for locoregional spread of HCC. These cases are summarized in Table 1. Patient age ranged from 35 to 83 years (mean 65.9). The male-to-female ratio was 2.2:1. All 19 patients had total or near-total thyroidectomies, and 16 received postoperative radioactive iodine. In one case, there was regional spread at the time of initial thyroidectomy. In the remaining 22 cases, recurrent clinical disease in the neck was detected after initial thyroidectomies. The time from primary diagnosis to first recurrence ranged from 0 to 12 years (mean 4.8). The locoregional disease involved the lateral neck (n=16), central neck (n=18), and larynx/trachea (n=4).
L, left; R, right; LND, lymph node dissection; LN, lymph node; ST, soft tissue; NA, tissue block not available for elastic staining.
All cases manifested as grossly identifiable rounded nodules, ranging in size from 0.5 to 4.5 cm. On microscopic examination, the tumor implants exhibited a multinodular pattern of growth. The nodules tended to have a smooth, rounded interface with the surrounding tissues (Fig. 1). In all 24 cases, the dominant tumor nodules were present in extra-nodal sites, including fat and skeletal muscle (Fig. 1). These soft-tissue nodules lacked a peripheral zone of lymphoid tissue or a lymph node capsule to suggest involvement or replacement of a lymph node. Areas suspicious for carcinoma involving vascular channels were common. In 13 of the 22 cases where tissue blocks were available for elastic staining, at least some of the microscopic tumor nodules were surrounded by a contiguous zone of compressed elastic fibers consistent with the wall of a blood vessel (Fig. 2). The absence of a developed muscular wall surrounding these nodules indicated their venous rather than arterial nature. The involved vessels included small-, medium-, and large-caliber veins.
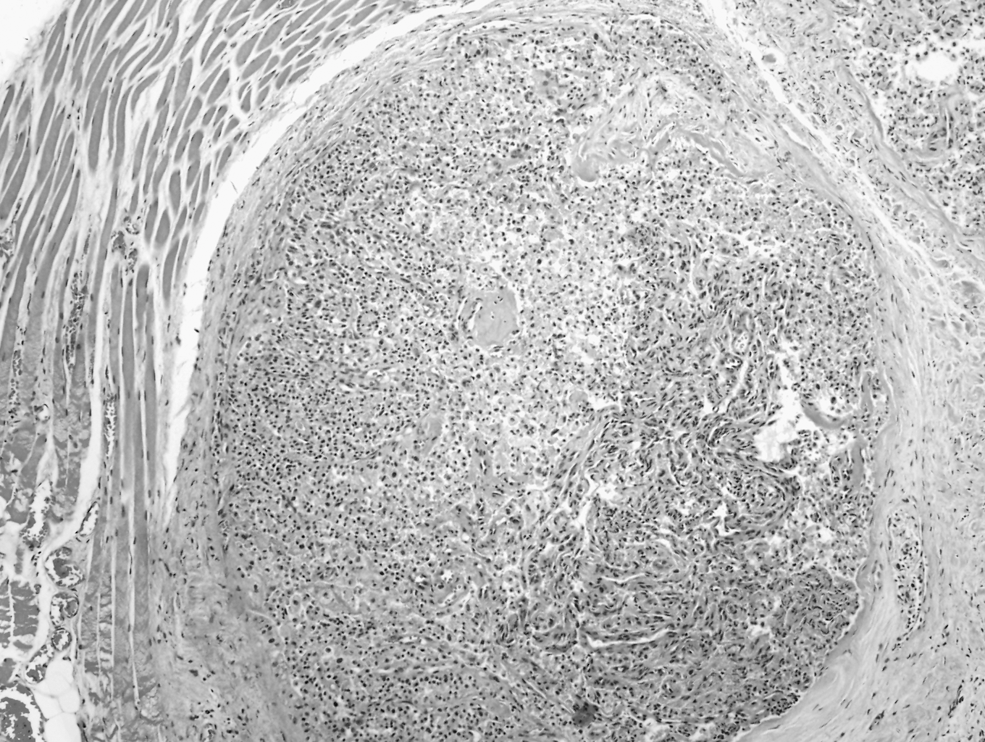
A rounded nodule of Hürthle cell carcinoma. The location of the tumor within skeletal muscle, along with the absence of a lymphoid cuff or lymph node capsule, indicates that this implant does not involve a lymph node (hematoxylin and eosin, ×100).
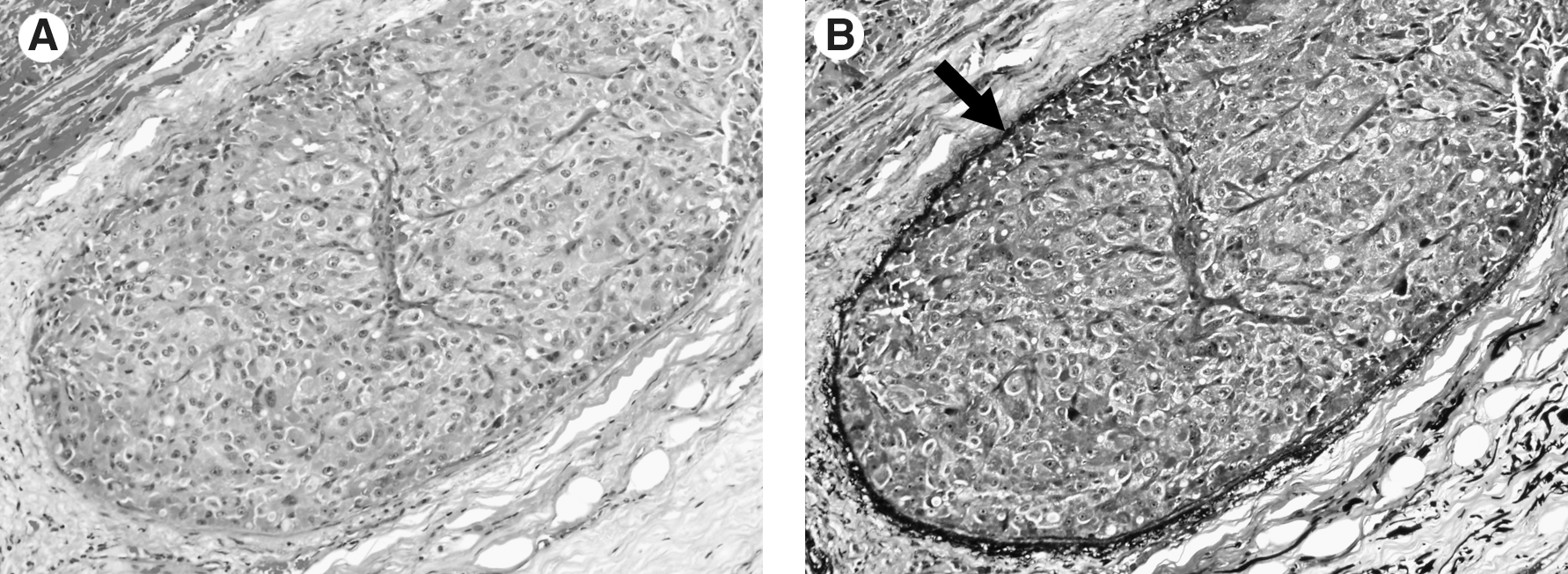
This nodule of Hürthle cell carcinoma comprises large, polygonal cells with granular, eosinophilic cytoplasm and prominent nucleoli (
True lymph node metastases were identified in six (25%) cases, but these tended to be small implants that were only apparent on microscopic examination. In five cases, these metastases were <0.5 cm and did not represent the dominant process. In the remaining case, two lymph node metastases, measuring 2.9 and 1.0 cm, were identified in a resection specimen with larger dominant soft-tissue implants.
Discussion
HCC is generally regarded as a more aggressive form of follicular thyroid carcinoma reflecting a lower likelihood of concentrating 131I and a higher likelihood of locoregional metastases (3 –6). Based on HCC's aggressive behavior, there have been recommendations for a more aggressive surgical approach, including total thyroidectomy with compartmental lymphadenectomy (12 –14). The strategy to remove lymph nodes en bloc is partially based on a presumption of spread to regional lymph nodes via the lymphatic plexus draining the thyroid gland. We found that in most cases of spread to the neck (74%), nodules of HCC were located not in lymph nodes but in soft tissues. In the cases where lymph node metastases were present, they were often microscopic (<5 mm) and occurred in a background of larger soft-tissue nodules that dominated the clinical and pathologic picture. Although these metastatic nodules could potentially represent replaced lymph nodes, there was no histologic evidence to support that interpretation. The metastatic nodules were not surrounded by any peripheral cuff of lymphoid tissue or a residual lymph node capsule. Instead, the majority of cases showed metastatic nodules surrounded by a thin zone of compressed elastic fibers consistent with elastic lamella of a vascular structure. Given the absence of a well-developed muscular wall, these structures most likely represent distended veins rather than arteries or arterioles. This venous distribution of these tumor emboli is not unexpected given well-known patterns of tumor invasion for follicular thyroid carcinomas, including the Hürthle cell variant. Follicular carcinomas escape the confines of the tumor capsule by accessing horizontal veins within the capsule, extending along thyroid outflow veins, and then reimplanting along the venous outflow tract as discrete nodules (21).
The relative infrequency of true lymph node metastases runs counter to the notion that lymph node metastases are common for HCCs. The actual evidence supporting tumor spread within the lymphatic chain, however, is not very compelling. First, many studies of HCC may take great care to document the presence and extent of capsular and/or vascular invasion of the primary tumor, but fail to document the precise distribution of tumor spread in the neck (3 –5,10,11,22,23). Even in those studies where nodal disease is purportedly supported at the histologic level, the distinction between true lymph node metastases and soft-tissue implants is not explicated by any detailed description or photomicrographic documentation (6 –9,24). Second, many studies of HCCs were undertaken before the description of oncocytic PTC (i.e., Hurthle cell PTC)—a variant of PTC that shares with conventional PTC a tendency to metastasize to cervical lymph nodes (25 –27). Some previously reported HCCs metastatic to lymph nodes were undoubtedly misclassified oncocytic PTCs (28). Third, assumption of lymph node spread may reflect a strong yet inappropriate tendency to generalize the behavior of one form of differentiated thyroid carcinoma to another form. The propensity of PTCs to metastasize to cervical lymph nodes is well documented, but this behavior may not necessarily be shared by other forms of differentiated thyroid cancer that are otherwise biologically and clinically distinct.
This practice of generalizing the behavior of one tumor type to another may be hazardous if erroneous assumptions are used to guide therapeutic decisions as they relate to specific therapeutic scenarios. As for current recommendations for the surgical management of locoregional spread to the neck, the American Thyroid Association recommends compartmental lymph node dissections rather than limited targeted removal of a tumor nodule based on a large experience with PTC (15,16). Although PTCs and HCCs may both spread to the neck, our findings indicate that the pattern and distribution of spread to the neck is quite different for HCCs. These differences should be carefully weighed when recommendations are made for the treatment of differentiated thyroid cancer, including when to target not just the tumor nodule but also the regional lymphatic network. Patients with HCC may not always require formal compartmental lymph node dissections, and in cases where there is clinically apparent locoregional spread of disease, wide excision of the nodules alone may provide local control similar to a compartmental lymphadenectomy.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.