
Abstract
Background:
Agents such as aflibercept, which target the angiogenic pathway, are of great interest as candidates for the management of metastatic differentiated thyroid cancer. Here, we report a patient who developed a hemorrhagic abdominal pseudoaneurysm shortly after being started on this drug.
Patient Findings:
The patient was a 67-year-old woman being treated with single agent aflibercept (VEGF-Trap) for metastatic thyroid cancer. She had no history of intra-abdominal pathology or vascular disease but had been previously treated with sorafenib. Twelve days after receiving her second dose of aflibercept, she developed vague abdominal pain, which increased in severity and was accompanied by nausea and vomiting. Her symptoms progressed along with a decline in her hematocrit and signs of internal hemorrhaging. An angiogram identified an occluded celiac artery with increased collaterals and a bleeding pseudoaneurysm in the inferior pancreaticoduodenal artery. After the pseudoaneurysm was coiled, the patient stabilized.
Summary and Conclusions:
Anti-angiogenic agents, usually well tolerated, can disrupt the delicate balance of normal endothelium, leading to hemorrhagic and thrombotic complications. The hemorrhage of aberrant vasculature should be included in the differential diagnosis in patients presenting with vague complaints while being treated with anti-angiogenic agents.
Introduction
Patient
A 67-year-old woman with papillary thyroid carcinoma metastatic to the lung and skin presented with severe nausea and generalized pain. The patient was receiving aflibercept at 4 mg/kg every two weeks on a clinical trial. The patient had a 6-year history of thyroid cancer, initially treated with a total thyroidectomy and radioactive iodine and, later, with external beam radiation therapy. She developed metastatic disease to the lung, skin, and lymph nodes, but no known abdominal disease. She was then treated with sorafenib for 7 months until progression of the disease, which occurred 4 months before admission. The patient was subsequently started on a phase II protocol with aflibercept and received her second dose of drug 12 days before admission. Her past medical history included chronic sinus disease, headaches, and depression. She had no known history of abdominal surgery. The patient was a former smoker with a 10 pack-year history.
The patient presented with generalized pain, nausea, and vomiting. The physical exam was unremarkable, with a soft, non-tender abdomen and bowel sounds present, and the laboratory values at admission were unremarkable. She was admitted for pain management. She was treated with intravenous hydration and dexamethasone and had symptomatic improvement. On hospital day 4, the patient developed excruciating pain in her sternum radiating to her breast and abdomen with the new onset of abdominal bloating and cramping. A computed tomography scan of the chest, abdomen, and pelvis with intravenous and oral contrast demonstrated a new high-density fluid collection in the upper abdomen consistent with an intraperitoneal hemorrhage (see Fig. 1). There was no free air to suggest perforation. The patient had no peritoneal signs on physical exam.
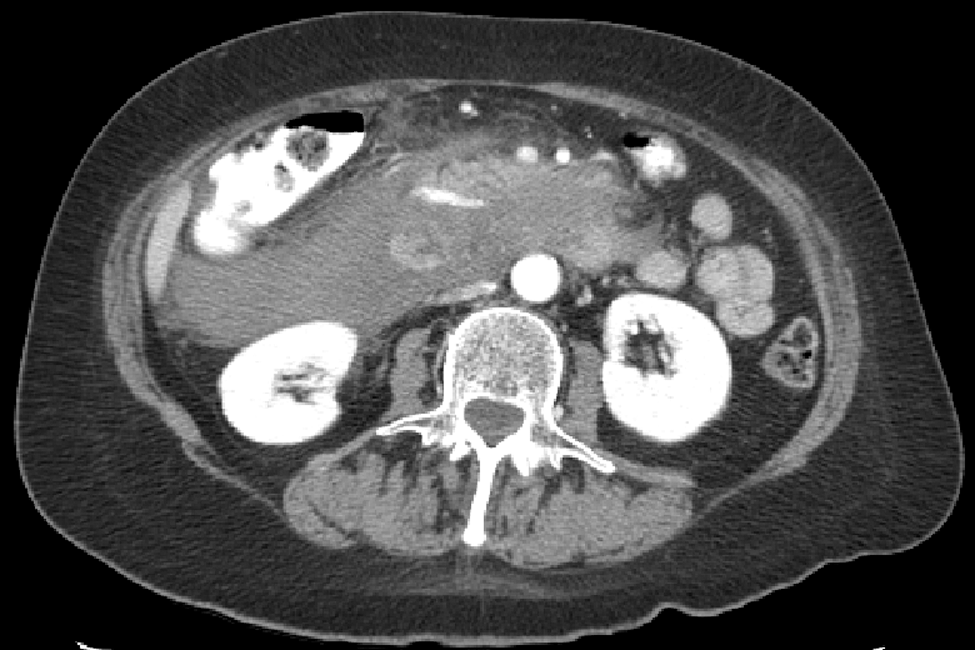
Axial computed tomography image of hematoma.
Over the next 24 hours, the patient was hemodynamically unstable and had a corresponding drop in hemoglobin from 11.7 g/dL to 8.4 g/dL. The platelet count and coagulation studies remained stable over this time. Given the persistence of hypotension and ongoing transfusion requirements, an emergent exploratory laparotomy was performed. Intraoperatively, she was found to have an extensive retroperitoneal hematoma, but no clear source of the bleed was identified. Postoperatively, the patient continued to require transfusions, and an angiogram was performed. The angiogram revealed an occluded celiac artery with increased blood flow through the inferior pancreaticoduodenal artery (IPDA) via collaterals (see Fig. 2). The source of bleeding was discovered to be a pseudoaneurysm that had developed in the IPDA. The lumen of the IPDA had abnormal scalloping consistent with a more diffuse wall abnormality, possibly vasculitic in appearance. This vessel abnormality seemed to be limited to this collateral flow; other blood vessels visualized during the angiography looked normal. The celiac artery was angioplastied to facilitate blood flow, and coils were placed around the pseudoaneurysm (see Fig. 3). After coiling, the transfusion requirements diminished, and the blood pressure stabilized. She had no further hemorrhage. The patient was taken off study. Her hospital course was further complicated by a thrombotic cerebrovascular accident (CVA). The patient has recovered well and has no significant neurological sequelae of the CVA.
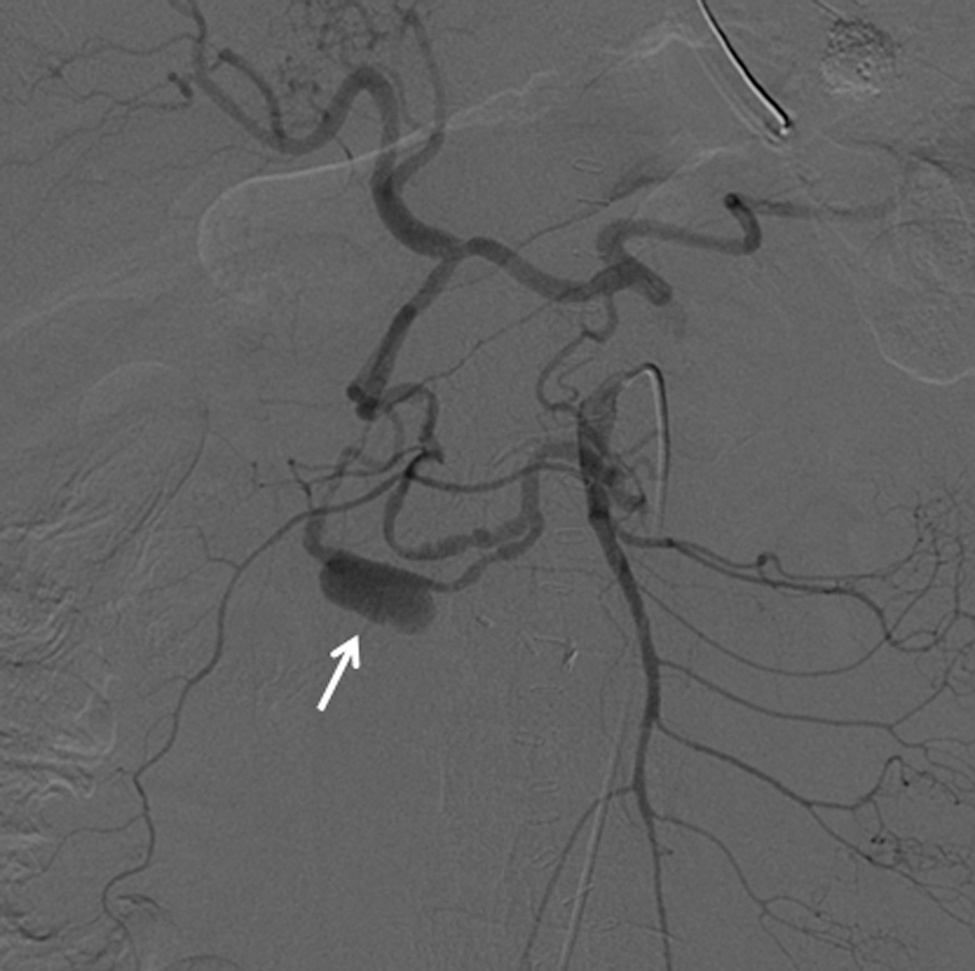
Angiogram of celiac artery. Arrow: Pseudoaneurysm in the collateral artery.
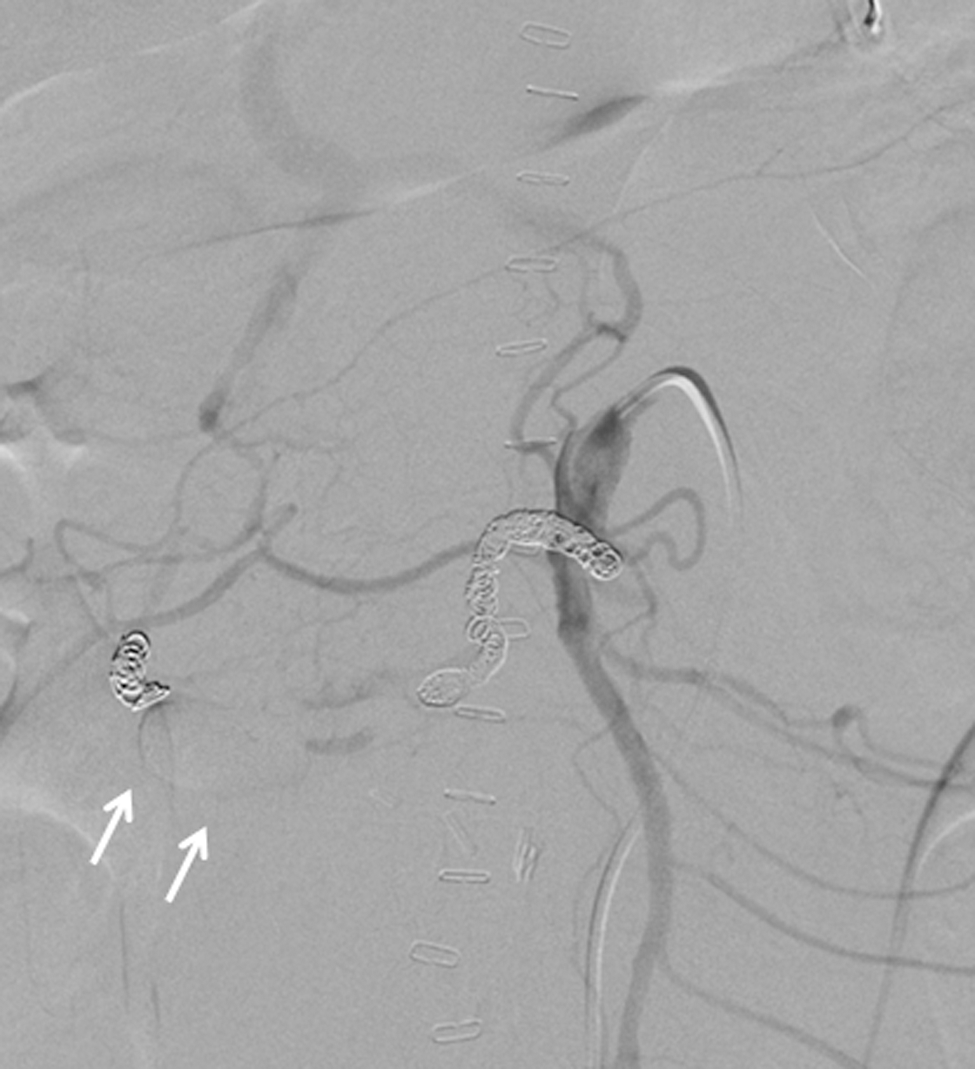
Angiogram of celiac artery post coiling. Arrow: Pseudoaneurysm in the collateral artery after coiling.
Discussion
Aflibercept is a fusion protein composed of the extracellular domain of VEGF1 and VEGF2 receptors bound to the Fc constant region of IgG1. Aflibercept acts a decoy binding VEGF with a high affinity, preventing it from binding with VEGF receptors expressed in various tissues (3). Aflibercept is one in a growing class of anti-angiogenic-targeted therapies that generally have acceptable side effects. However, toxicities such as serious thrombotic and hemorrhagic events have been reported to varying degrees with anti-angiogenic therapies and likely result from a disruption in the normal delicate balance of hemostasis. The varying mechanisms of VEGF inhibition have differing impacts on the normal physiologic properties of endothelial cells.
The prevalence of arterial thrombosis reported in clinical trials varies by anti-angiogenic agents with a prevalence of 3.3% (95% confidence interval [CI] 2.0–5.6) and a relative risk (RR) of 2.08 (95% CI 1.28–3.40) reported with bevacizumab and a prevalence of 1.7% (95% CI 1.1–2.4) and RR of 3.10 (95% CI 1.22–7.85) with sorafenib. The risk of arterial thrombosis is not elevated in trials of sunitinib with a prevalence of 1.3% (95% CI 1.0–1.6) and an RR of 2.39 (95% CI 0.12–49.41) (7,8). While the prevalence of grade 3 or higher venous thromboembolic disease on bevacizumab was 6.3% (95% CI 4.8–8.3) with an RR of 1.38 (95% CI 1.12–1.70), neither sunitinib nor sorafenib increased the RR of venous thromboembolic disease (9,10).
In a recent meta-analysis of randomized controlled trials of anti-angiogenic agents across multiple solid tumor sites, the rates of grade 3–5 hemorrhage were reported in 2.8% (95% CI 2.1–3.8) with an RR of 1.6 (95% CI 1.2–2.2) in patients treated with bevacizumab and 2.4% (95% CI 1.6–3.9) with an RR of 1.2 (95% CI 0.7–1.92) in patients treated with either sorafenib or sunitinib (11,12). Hemorrhage, in the setting of VEGF inhibition, is potentially attributed to the non-physiologic apoptosis of endothelial cells, which can lead to loss of integrity of blood vessels. Tumor vasculature is likely more susceptible due to its dependence on VEGF (13). We report a case of severe hemorrhage from a nonmalignant blood vessel.
Celiac artery stenosis is not a rare finding, occurring in about 7% of the population (14). The etiology is not well understood, and it generally remains asymptomatic in most patients. When celiac artery stenosis is present, the pancreaticoduodenal arteries serve as the major collateral routes from the superior mesenteric artery (15). Usually both the anterior and posterior systems develop as collator pathways, but as seen in this patient, occasionally one system can develop and serve as a single dominant pathway. The formation of collaterals is a normal physiologic response to arterial occlusion and results in angiogenesis, a process dependent on the VEGF pathway (16). Typically, this aberrant vasculature remains undetected, but in this patient being treated with anti-angiogenesis therapy, the stressed IPDA arcade provided the location for a potentially life-threatening grade 4 hemorrhage.
The toxicity of long-term or sequential use of anti-angiogenic therapy is not well understood. Earlier studies have found that concurrent anti-VEGF therapy can cause significant vascular damage. This patient developed this toxicity only 12 days after the second dose of aflibercept, but she had earlier received 7 months of sorafenib therapy. It raises the concern that the duration, the mechanism of VEGF inhibition, or both could be important in patients, especially those who are susceptible due to aberrant blood vessels. The number of agents in this class of anti-cancer therapies is growing along with indications for use. Similar to hypertension and proteinuria, hemorrhage is a class effect of this drug, and the potential toxicity of sequential administration should be considered in the differential for patients presenting with vague abdominal symptoms.
Footnotes
Acknowledgments
The study drug was provided by the Cancer Therapy Evaluation Program (CTEP). The study was funded by Grant N01 CM 62206 and the Overman Fund. A special acknowledgment goes to Alice Chen at CTEP for review of this article.
Disclosure Statement
The authors declare that no competing financial interests exist.