
Abstract
Background:
Carcinoma showing thymus-like elements (CASTLE) is a rare malignant neoplasm of the thyroid gland, morphologically and immunohistologically similar to a thymic carcinoma, whose histogenesis is still debated. Hypotheses include an origin from ectopic thymic tissue, vestige of the thymopharyngeal duct, or branchial pouch remnants from which solid cell nests (SC-nests) originate. The diagnosis of CASTLE may be treacherous due to its rarity and its propensity to mimic other poorly differentiated tumors such as squamous cell carcinoma.
Methods:
We present a case of CASTLE in a 58-year-old man initially diagnosed as a poorly differentiated squamous cell carcinoma both on fine-needle aspiration cytology (FNAC) and on biopsy, arising in close association with SC-nests. A thorough literature review, with special emphasis on its diagnosis and histogenesis of CASTLE, was also conducted.
Results:
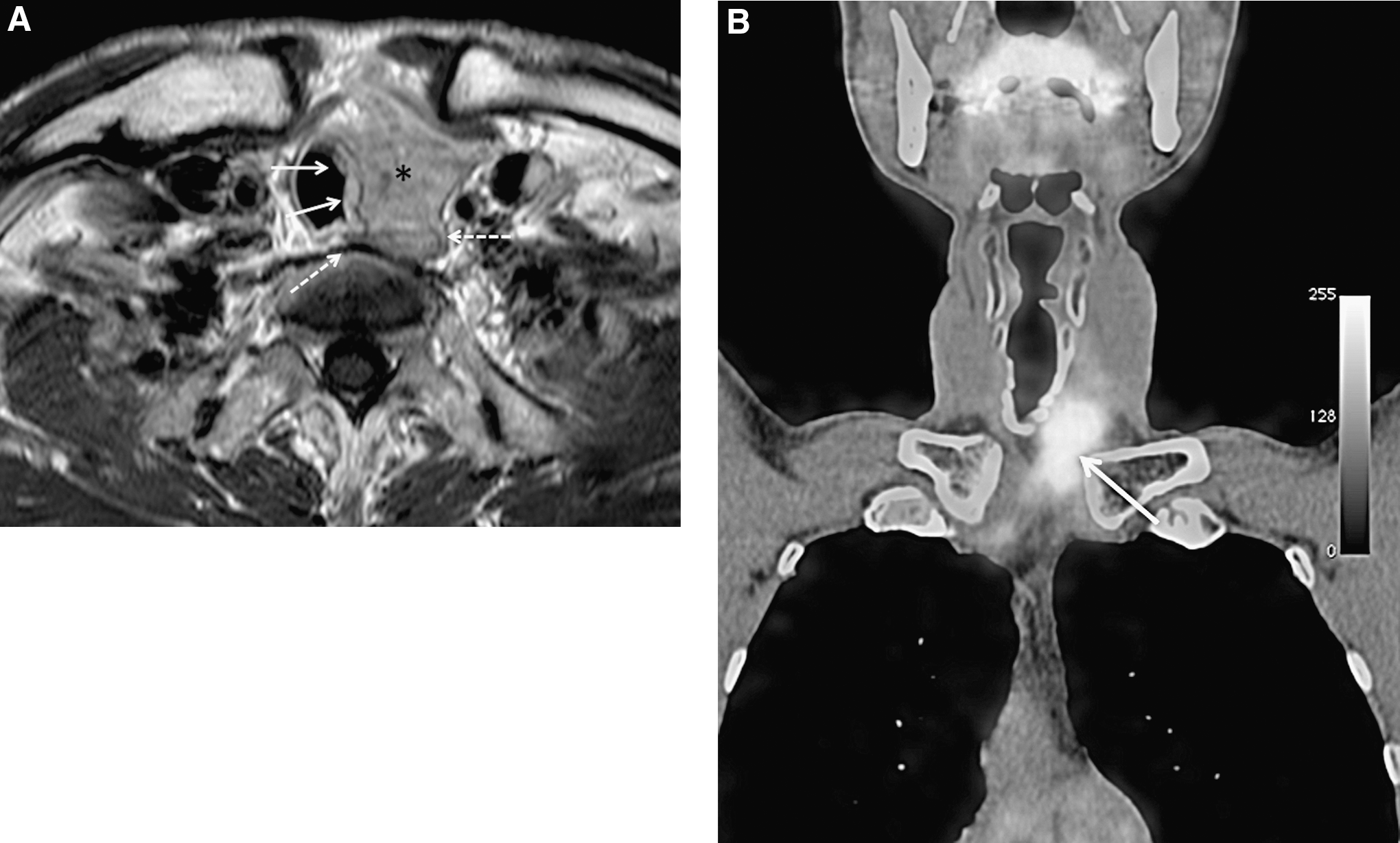
Magnetic resonance images revealed a 4.0-cm cervical mass on the left side of the trachea, involving the lateral middle/inferior portion of the left lobe of the thyroid gland. FNAC was performed with a diagnosis of “malignant cells, consistent with squamous cell carcinoma.” A histological evaluation of the resected specimen revealed a malignant proliferation of cells, focally exhibiting a squamoid appearance, which were immunopositive for CD5 and p63. A diagnosis of CASTLE was made. The tumor was located in direct continuity with SC-Nests, and the cell morphology of both the SC-nests and CASTLE was very similar with merging. Moreover, the immunohistochemical expression profiles of most markers useful in the diagnosis of CASTLE were identical in the SC-nests.
Conclusions:
The inclusion of CASTLE in the differential diagnosis of poorly differentiated tumors of the thyroid region and the use of ancillary studies are essential to diagnose this rare entity associated with a relatively favorable prognosis. The close association of CASTLE with SC-nests opens the way to a new scenario for studies of its histogenesis.
Introduction
Most CASTLE occurs in the thyroid gland, with a particular predilection for the middle to lower part, but the tumors often extend to extrathyroidal soft tissue (1,2). Similarly, thyroid SC-nests are predominantly found in the middle third of the lateral thyroid lobes (5). Nevertheless, a direct spatial and temporal morphologic continuum between SC-nests and CASTLE has not been described.
Comparative immunohistochemical features of both SC-nests and CASTLE (from separate patients) have been reported in a recent study (4). The positive immunochemical markers in this study included p63, carcinoembryonic antigen (CEA), high–molecular-weight cytokeratins (HMWK), and CD5 markers (4). There was a similar profile in the two patients, one with SC-nests and the other with CASTLE, except for CD5, which was found in CASTLE and is known to be a critical marker of CASTLE. Thus, this study suggests that CASTLE is closely related to SC-nests and that it may originate from SC-nests due to their similar immunohistochemical profile (4). Additionally, Veits et al. have shown using comparative genomic hybridization that CASTLE is characterized by chromosomal imbalances similar to those found in thymomas and thymic carcinomas, indicating a similar sequence in tumor development (10).
Here we describe a unique case of CASTLE arising in close association with SC-nests, suggesting that SC-nests may potentially be a precursor lesion due to its topographic, morphological, and immunohistological similitudes with CASTLE. We also review the difficulties in the diagnosis of this rare entity and in elucidating its histogenesis.
Materials and Methods
The materials obtained from the fine needle aspiration cytology (FNAC) of the cervical mass were rinsed in an ethanol-based fixative system (BD CytoRich™. Red Preservative, BD Diagnostics, Burlington, NC) and thin-layer slides were then prepared and stained (Papanicolaou) using an automated BD PrepStain™ Slide Processor. Materials were available for the cell block preparation, which was performed, sectioned, and stained by H&E.
All surgical specimens (open biopsy and resection) were fixed in 10% buffered formalin and routinely processed. The mass was extensively sampled. Hematoxylin and eosin stains were performed on 3-μm-thick sections of formalin-fixed paraffin-embedded tissue.
Immunohistochemistry was conducted using the following antibodies and conditions, and the Envision Plus detection System (Dako, Carpinteria, CA): CK903 (Dako; clone 34βE12; 1:100 dilution); p63 (Dako; clone 4A4; 1:200 dilution); galectin 3 (BD Bioscences, Franklin Lakes, NJ; clone B2C10; 1:50 dilution); CEA (Dako; clone Fo/11-7; 1:100 dilution); CD117 (KIT) (Dako; 1:100 dilution); calcitonin (Dako; clone 1–32; 1:20 dilution); Thyroid transcription factor (TTF-1) (Dako; clone 8G7G3/1; 1:100 dilution); CD5 (Novocastra, Newcastle upon Tyne, United Kingdom; clone 4C7; 1:20 dilution); Ki-67 (Dako; clone Mib-1; 1:200 dilution). Antigen retrieval (microwave pretreatment: CK903; galectin 3; CEA; CD117; calcitonin; pressure cooker: p63; TTF-1; CD5) was used. Appropriated positive and negative controls were used throughout.
Results
Case presentation
A 58-year-old man presented with a 1-year history of dysphonia and occasional dysphagia. The patient was an ex-smoker with a remote history of gastric adenocarcinoma for which a total gastrectomy was performed in 1995. Clinical examination showed palsy of the left vocal cord and a lower neck mass. Magnetic resonance images revealed a 4.0-cm cervical mass on the left side of the trachea, involving the lateral middle/inferior portion of the left lobe of the thyroid gland (Fig. 1A). FNAC was performed showing medium-sized elongated cells with poorly defined borders, the eosinophilic cytoplasm, and organoid architecture. Nuclei were atypical, vesicular, and sometimes nucleolated. In the background, small lymphocytes were present. The cell block preparation showed a group of cohesive cells in a vaguely squamoid arrangement (Fig. 2A). Immunocytochemically, the cells were positive for p63 and cytokeratin, but did not express TTF-1, calcitonin, or thyroglobulin. A diagnosis of “malignant cells, consistent with squamous cell carcinoma” was rendered. Presuming a thyroid metastasis or a direct extension to the thyroid from a primary malignancy in the head and neck area, a complete panendoscopy was performed as well as a whole-body positron emission tomography–computed tomography scan, which showed a very high-glucose metabolism of the tumor (Fig. 1B), but did not identify any other abnormality. An open surgical biopsy of the mass was then performed to better specify the nature and origin of the neoplasia; the diagnosis was “poorly differentiated squamous cell carcinoma infiltrating the thyroid and perithyroid soft tissue.” Surgical resection (left thyroid lobectomy with lumpectomy and partial tracheal resection) was performed. The patient had adjuvant radiotherapy (66 Gy) and was disease-free 22 months after surgery.
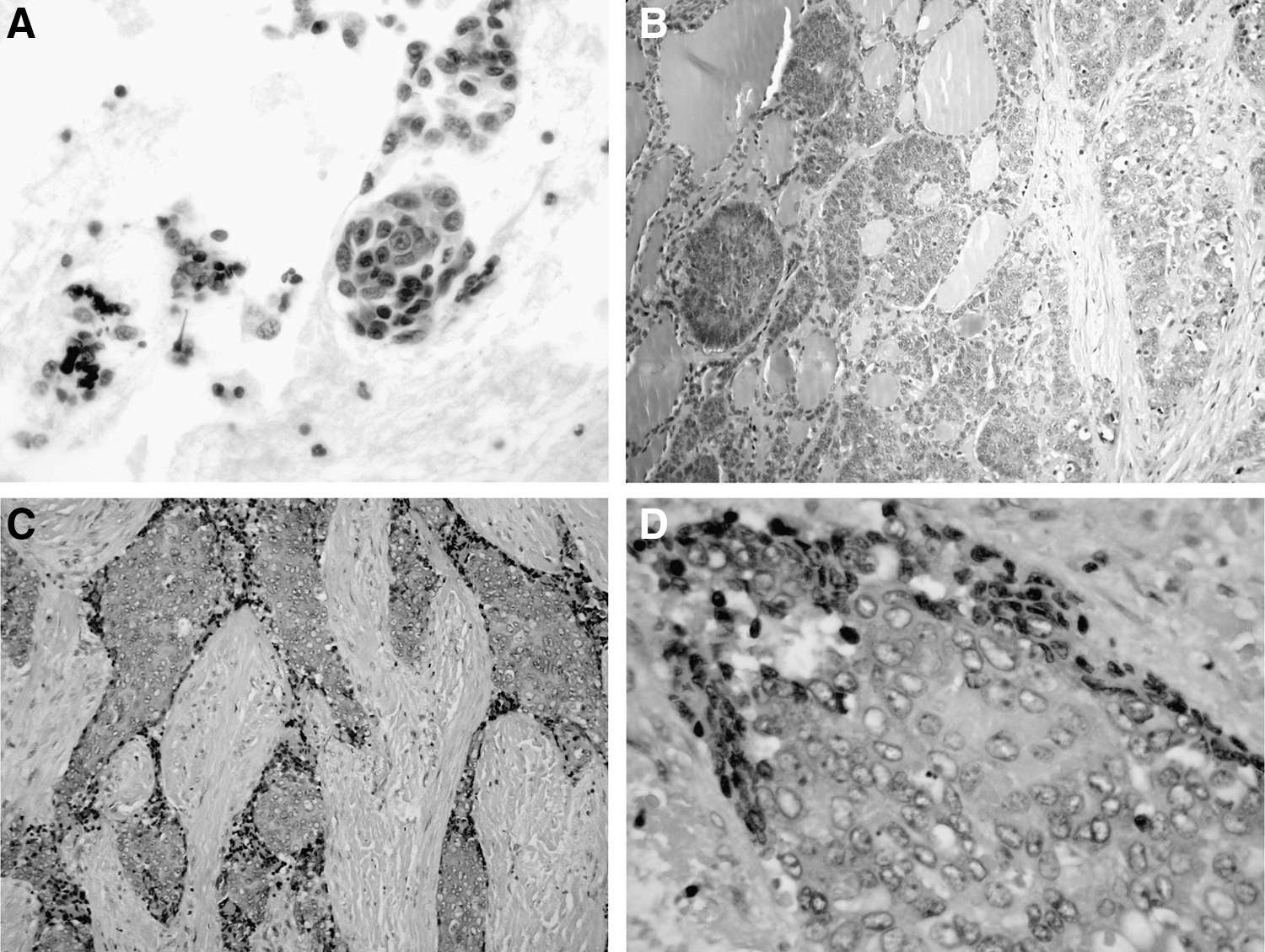
Gross examination of the surgical specimen showed a solid, firm, lobulated, grayish-white tumor, 3.2 cm × 2.7 cm × 2.0 cm, originating from the lateral middle part of the left thyroid lobe and infiltrating the lateral surrounding soft tissue (mainly squelettal muscle) and the external portion of the trachea (Fig. 3). The mass was extensively sampled and had a uniform microscopic appearance. The neoplasm was composed of islands and cords of medium-sized cells admixed with small lymphocytes and separated by dense fibrous septa (Fig. 2C). The tumor cells were ovoid to spindle-shape with an indistinct cell border, and contained abundant pale cytoplasm and large vesicular nuclei with a prominent nucleoli (Fig. 2D). Focally, the cells exhibited a squamoid appearance, with more distinct cell borders, but without a discernable intercellular bridge or keratinization. Mitoses were rare and no necrosis or calcifications were identified. One regional lymph node metastasis was found.
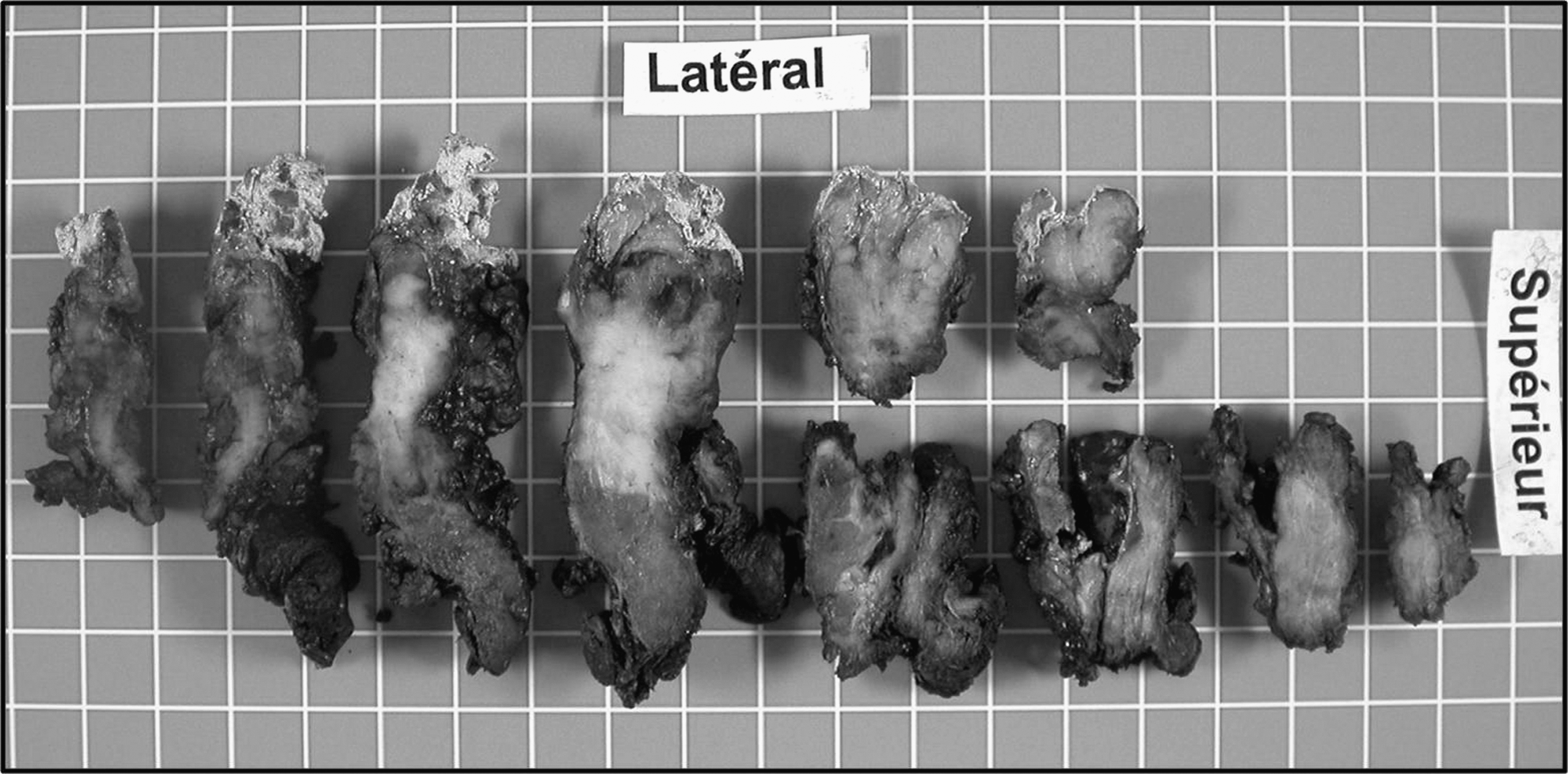
Horizontal sections of the surgical specimen (formalin-fixed) show a white tumor infiltrating thyroid parenchyma and perithyroidal soft tissues up to the surgical margin.
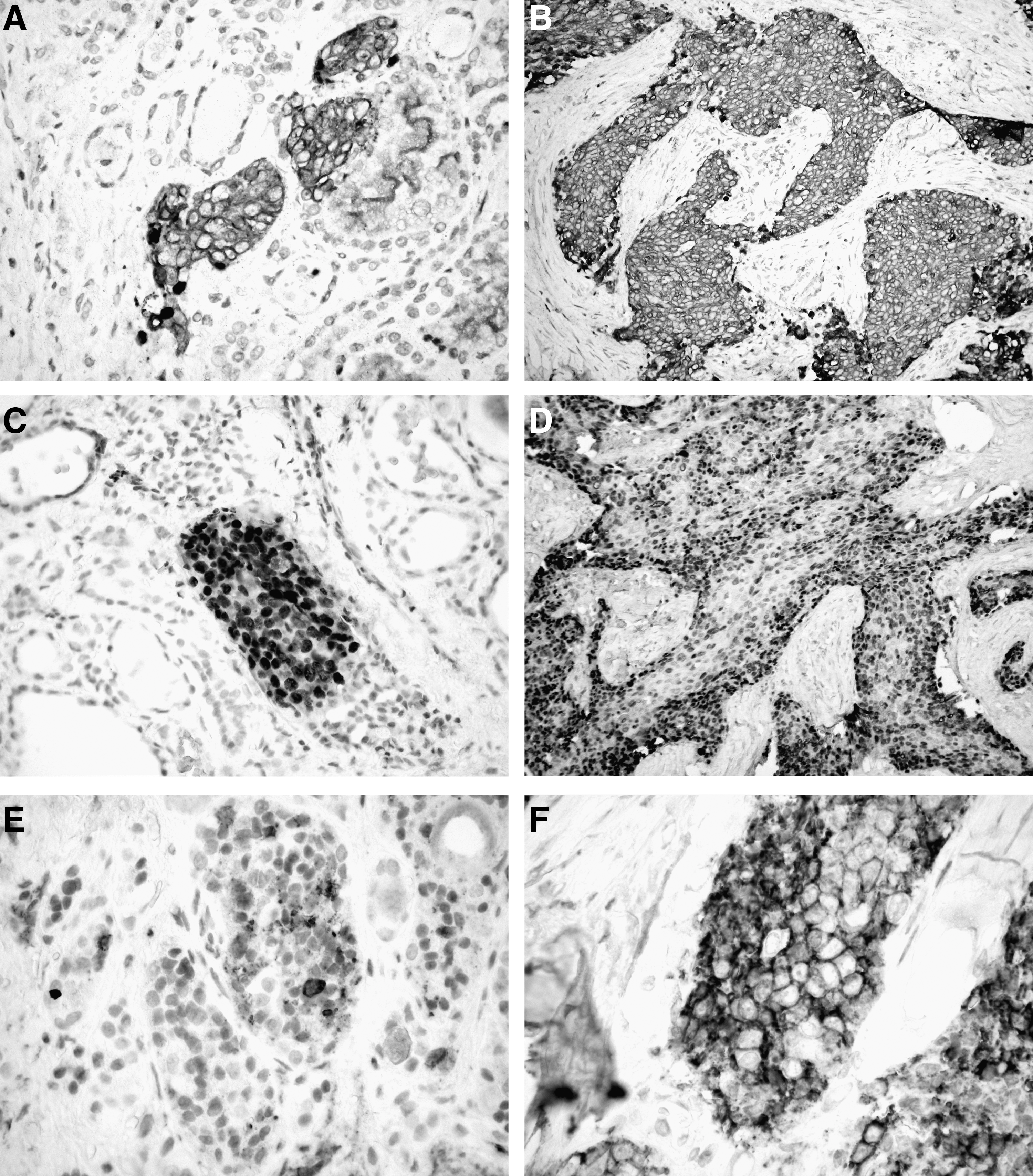
Notably, SC-nests were identified into the adjacent thyroid parenchyma. These SC-nests had a direct continuity with the tumor mass without any intervening capsule or fibrous septa (Fig. 2B). Additionally, the cell morphology of the SC-nests was very similar to the tumor cells. In both the tumor and the SC-nests, the cells exhibited a similar immunoreactivity (Fig. 4). Namely, all cells expressed diffusely and strongly cytokeratin 903 and p63 (Fig. 4A–D); focally galectin 3, CEA, and KIT (CD117). Conversely, calcitonin and TTF-1 showed no reactivity. Although the tumor cells revealed diffuse membranous CD5 staining (Fig. 4F), SC-nests were weakly and focally positive for CD5 (Fig. 4E). The proliferative index (Ki-67/MIB-1) reached focally 25%.
Discussion
This case illustrates two major issues about CASTLE: its diagnosis and its origin. From a diagnostic point of view, an accurate diagnosis was not made in this case preoperatively, thus illustrating the diagnostic difficulties in cases of such a poorly-known and rare entity. While it did not affect the clinical management in this patient, a correct diagnosis on FNAC or incision biopsy is still important because CASTLE usually has a much better prognosis than other tumors, which enter into its differential diagnosis, including a primary or secondary epidermoid carcinoma of the thyroid gland. A correct diagnosis may prevent unnecessary investigations and increase the likelihood of a surgical resection. The FNAC features of CASTLE have not been extensively described in the literature and there are no reliable cytological criteria. In the literature, a diagnosis of “malignant tumor” or “suspicious for malignant tumor” is made in the majority of cases. Although one case was correctly diagnosed by FNAC, the remaining cases had unusual features not typical for a papillary, follicular, medullary, squamous, or undifferentiated carcinoma (4,10 –12).
In the largest series available, Hirokawa et al. (13) described the cytological features of eight cases of CASTLE. They were all diagnosed as “malignant tumors,” except for one case in which only the necrotic material was aspirated. Among them, poorly differentiated carcinoma was most frequently considered (six of eight cases) and CASTLE was suggested as one differential diagnosis only in two cases. Of note, immunocytochemistry (e.g., CD5) was not performed on those cases. Five of them showed squamous differentiation (including acidophilic keratinization) and six of them contained a small to moderate number of lymphocytes and plasma cells in the background. The latter being a helpful morphological clue to suggest CASTLE, although by no means specific.
The inclusion of CASTLE in the differential diagnosis of any poorly differentiated tumors of the thyroid region (“to think about it”) and the use of immunohistochemistry (including p63 and CD5), when feasible, are probably the best ways to promote the correct preoperative diagnosis of this rare neoplasm.
Since its initial description in 1985, several hypotheses have been proposed to explain the histogenesis of CASTLE, including ectopic thymic tissue, vestiges of the thymopharyngeal duct, or branchial pouch remnants, such as SC-nests (4). This case, in which there was merging of CASTLE and SC-nests cells, raises the possibility that SC-nests may have been the precursor lesion. There is topographic, morphological, and immunohistochemical evidence in this case and in the literature that suggests that SC-nests may be a source of some cases of CASTLE.
Topographically, the tumor was located in the lateral middle to lower part of the thyroid (Figs. 1 and 3), reflecting the localization reported in the literature (1 –3,14). This topography also reflects the localization of the SC-nests, which are predominantly found in the middle third of the thyroid lateral lobes (5). SC-nests can be found in most (>60%) thyroid specimens if the search is meticulous. In contrast, ectopic thymic tissue, another candidate for CASTLE histogenesis, is rarely found in the thyroid gland (1.4%) (15).
Histologically, the SC-nests were readily discernable and numerous in this case and were merging with the neoplasm without there being any intervening fibrous septa, capsule, or thyroid follicle (Fig. 2B). Of note, the immunoreactivity for CD5 was much fainter in the SC-nests than in CASTLE cells, arguing against a subtle nested-like infiltration of the thyroid parenchyma by CASTLE cells that mimicked SC-nests.
Immunohistochemically, the expression profile of most markers useful in the diagnosis of CASTLE (p63, HMWK −CK903, CEA, KIT −CD117) were identical in CASTLE and SC-nests (Fig. 4A–D). The only notable difference was CD5 as previously noted (Fig. 4E–F).
CD5 immunoreactivity was present in neoplastic cells, as described in most cases of CASTLE and of primary thymic carcinoma, but very weak or absent in SC-nests, as has also been reported (4,16,17). This similar morphology and immunoprofile of CASTLE and thymic carcinoma has been used previously as an argument to support a thymic differentiation and/or origin of CASTLE and/or a possible ectopic thymus derivation, a hypothesis that was proposed in the first report of the disease (2,4,16,17). Moreover, observation of a histologic continuity from orthotopic thymic tissue to this neoplasm as been described (18). However, an SC-nests origin may be more likely than an ectopic thymus derivation of CASTLE for the following reasons. First, SC-nests, which are very small, could have been easily overgrown by the tumor in most cases of CASTLE, including the case described by Kakudo et al. (18), preventing their recognition. Second, SC-nests show an immunohistochemical expression profile most similar to thymic tissue, supporting a similar embryonal derivation of these tissues from the branchial pouch (4). Finally, considering the usual location of most cases of CASTLE and the much higher prevalence of SC-nests compared to the ectopic thymic tissue in the thyroid, as mentioned earlier, it is easier to explain an SC-nests origin for most CASTLE cases rather than an ectopic thymic tissue origin. Although we support the concept of an SC-nests derivation of CASTLE, this does not exclude the possibility that some cases of CASTLE, including the rare purely extrathyroid form, could develop from ectopic extra- or intrathyroid thymic tissue, as SC-nests are only located inside the thyroid gland. Hence, a dual origin, from SC-nests and also from ectopic thymus tissue, may occur.
To the best of our knowledge, this is the first report of CASTLE closely associated with SC-nests. Additional studies are needed to determine if our patient is unusual with regard to SC-nests as the site of origin for his CASTLE, or if this is more common but difficult to detect without meticulous investigations. These studies would be aided if they included mutually exclusive markers for thymic tissue and SC-nests.
Footnotes
Disclosure Statement
The authors disclose that no competing financial interests exist.