
Abstract
Background:
While radioiodine (RAI) therapy remains the most effective treatment modality for RAI-avid distant metastatic follicular cell–derived thyroid cancer, the therapeutic utility of empiric RAI therapy in patients with structurally identifiable distant metastases that demonstrate RAI avidity only on the post-therapy scan (negative diagnostic whole-body scan [DxWBS]) remains uncertain.
Methods:
We report a retrospective assessment of the structural response to RAI therapy in 27 patients (median age 54 years, 59% male) with metastatic thyroid cancer (45% classical papillary thyroid cancer, 21% poorly differentiated, 15% tall-cell variant, 15% follicular variant, and 4% Hurthle cell carcinoma) with structurally identifiable distant metastases (86% pulmonary metastases) in whom a properly conducted DxWBS was negative, and the post-therapy scan showed RAI-avid metastatic lesions at the time of RAI remnant ablation.
Results:
In response to the initial RAI ablation, none of the selected patients demonstrated structural disease regression, and no patient was rendered free of disease. However, 12 patients (44%) demonstrated stable lesions on serial structural imaging after an RAI ablation. Structural disease progression was seen in the remaining 56% (15/27), a median of 6 months after ablation. Unfortunately, additional RAI therapies given to 12/15 patients with progressive disease and 5/12 patients with stable lesions failed to cause structural disease regression, cure, or conversion from progressive to stable disease in any patient. All of the disease-specific deaths (7/27) were in patients who had structural disease progression (n=15) in response to RAI ablation. None of the patients with persistent but stable lesions on structural imaging (n=12) have died of thyroid cancer over a median follow-up period of 3.7 years.
Conclusions:
While 44% of patients with the DxWBS-negative/post-therapy scan-positive macroscopic distant metastasis will have stable cross-sectional imaging after RAI remnant ablation, the other 56% will demonstrate structural disease progression that cannot be effectively treated with repeated empiric RAI activities. Furthermore, the high disease-specific mortality rate seen within the first few years of remnant ablation in this small subset of patients with persistent progressive disease despite a positive post-therapy RAI scan argues that treatments other than repeated empiric RAI dosing be strongly considered.
Introduction
The use of empiric radioiodine (RAI) therapy for either localization or therapeutic purposes in Tg-positive/diagnostic whole-body scan (DxWBS)–negative patients without structurally identifiable disease remains controversial. As our ability to detect non-RAI-avid disease has improved through the use of neck ultrasonography, high-resolution cross-sectional body imaging, and fluorodeoxyglucose (FDG)–positron emission tomography (PET) scanning, the use of empiric RAI as a localization study is being used much less commonly. However, many clinicians continue to use empiric RAI in Tg-positive/DxWBS-negative patients as a therapeutic tool.
Recommendation 75 of the 2009 ATA thyroid cancer management guidelines note that “empiric radioactive iodine therapy (100–200 mCi) might be considered” in patients with elevated or rising serum Tg levels “in whom imaging has failed to reveal a potential tumor source” since the post-therapy scan will identify a discrete metastatic lesion in up to 50% of the patients (5,8 –11). Furthermore, recommendation 76 indicates that additional empiric RAI therapies should only be repeated if there is “objective evidence of significant tumor reduction” in which case RAI therapy should be repeated “until the tumor has been eradicated or the tumor no longer responds to treatment” while balancing the risk of repeated RAI treatments against “uncertain long term benefits” (11).
Some argue that empiric treatment with RAI is likely to provide an objective benefit, since radioiodine uptake on the post-therapy scan reflects at least a partial ability of the tumors to concentrate iodine. In support of this hypothesis, several studies have demonstrated a significant reduction in Tg levels and resolution of radioiodine uptake on the post-therapy scan in patients with microscopic Tg-positive/DxWBS-negative disease who received repeat empiric RAI therapies (8,10,12 –14). In a recent meta-analysis, up to 62% of these patients demonstrated a decrease in Tg levels in the years after RAI therapy (15). However, it has now become apparent that observation and levothyroxine suppression without additional RAI therapy can be associated with a slow decline in the serum Tg over many years in many Tg-positive/DxWBS-negative patients (10,14,16 –18). These observations make it difficult to ascertain whether the fall in Tg after empiric RAI therapy is caused by a tumoricidal effect of RAI or whether the Tg would have spontaneously decreased over time with observation and continued TSH suppressive therapy.
Since empiric RAI therapy for Tg-positive/DxWBS-negative patients was largely focused on using the post-therapy scan to localize metastatic foci, patients with structurally identifiable disease were usually excluded. The exception was a report by Fatourechi et al., who described continued disease progression despite additional RAI therapies in one patient with macroscopic distant metastases who was negative on the DxWBS and positive on the post-therapy scan (19). In our referral practice, we are occasionally faced with the clinical dilemma of a patient with structurally identifiable distant metastases on cross-sectional imaging in whom a properly done DxWBS is negative. In this clinical scenario, the inability to visualize structurally identifiable metastatic disease on DxWBS suggests that the metastatic lesions have significantly impaired ability to trap and retain RAI. Since individual lesional dosimetry studies are not a diagnostic option for most patients, we hypothesized that the absence of visible RAI uptake on diagnostic RAI scanning in macroscopic metastatic lesions could be used a surrogate marker of lesional dosimetry to identify metastatic lesions that are very unlikely to have an objective response to additional RAI therapy even if the metastatic lesions were RAI avid on the post-therapy scan.
Therefore, the goal of this study was to retrospectively evaluate the impact of repeat RAI therapies in a cohort of patients with metastatic, follicular cell–derived thyroid cancer with structurally identifiable distant metastases in whom a properly conducted DxWBS was negative, and the post-therapy scan showed RAI-avid metastatic lesions at the time of initial RAI remnant ablation. Specifically, we aimed to study the ability of repeat RAI therapy, defined as any RAI therapy after RAI ablation, to shrink or resolve persistent lesions in distant metastatic sites. Without an untreated control group, we cannot determine whether or not the initial RAI ablation dose caused subsequent stable disease or whether the patient would have stable disease even without RAI. Additionally, it is not possible to determine if repeated RAI doses had any impact on maintaining stable disease over time. Therefore, the primary endpoints of the study focused on objective measures of either disease progression or regression on cross-sectional imaging after repeated RAI therapies. To our knowledge, this is the first study to address short-term and long-term disease-specific clinical outcomes of repeat RAI therapy in patients with structurally identifiable distant metastatic thyroid cancer presenting with a negative diagnostic/positive post-therapy scan at time of RAI ablation.
Materials and Methods
Subjects
After obtaining the Institutional Review Board's approval, we retrospectively reviewed the electronic medical records of 364 consecutive subjects with metastatic FCDTC who had RAI scanning or therapy at Memorial Sloan-Kettering Cancer Center (MSKCC) between 1990 and 2011. In 58/364 patients, a negative DxWBS (obtained 48–72 hours after 5 mCi 131I) was associated with a positive postablation scan (obtained 5–10 days after ablative RAI therapy, more than 90% of the structurally identifiable disease was RAI avid). The median-administered activity of 131I was 150 mCi (range 73–300 mCi). Iodine contamination through contrast load was excluded by careful history, and all patients were placed on low-iodine diet 7–10 days before scanning. Urinary iodine measurements are not routinely obtained. At the time of ablation, RAI activity was determined empirically in 22 patients, with only 5 patients having whole-body and blood radioactive iodine clearance.
After excluding patients with no corresponding structural disease on the post-therapy scan (n=18), those with inadequate follow-up imaging (n=10), 1 patient with chronic noncompliance with levothyroxine suppression therapy, 1 patient with 30% uptake in the thyroid region at the time of scanning, and 1 patient with false-positive uptake in bronchiectasis; 27 patients were available for evaluation.
Subjects of all ages with metastatic thyroid carcinoma were included, except those with histological diagnosis of anaplastic or medullary thyroid carcinoma. All studied patients received TSH suppressive therapy for the duration of the study.
Laboratory studies
All Tg levels were measured at MSKCC. Between 1990 and 1997, various Tg assays were used with functional sensitivities of ∼1 ng/mL. Starting in 1998, all Tg values were measured using the Dynotest-TgS immunoradiometric assay (Brahms, Inc.; functional sensitivity 0.6 ng/mL normalized to CRM 457). We excluded subjects with interfering thyroglobulin antibodies (TgAbs) from the Tg analysis (n=5).
Follow-up
A minimum of 1-year follow-up after radioiodine ablation was required for entry in this study unless one of the clinical endpoints (recurrence, thyroid cancer-related death) was reached earlier. Appropriate serial follow-up included unstimulated Tg and TgAb measurements and cross-sectional imaging of the involved organ 6–18 months after each radioiodine therapy.
Clinical endpoints
Objective outcome to therapy (change in Tg and/or structurally evident disease) was assessed after initial RAI ablation and then again after any subsequent RAI therapy. Patients achieving an undetectable suppressed Tg level and no structural evidence of disease were classified as having no evidence of disease (NED). Patients were classified as having structurally progressive disease if the maximum size of any metastatic lesion increased more than 20%, or there was an increase in the number of metastatic foci on follow-up cross-sectional imaging. Likewise, structural disease regression was defined as a decrease in the maximum tumor size of 30%, or a decrease in the number of metastatic lesions by at least 30% on follow-up cross-sectional imaging. Patients not meeting criteria for structural progression or regression were classified as having structurally stable lesions. Similarly, a 20% increase in suppressed Tg was defined as biochemical progression, and a 20% decrease was classified as biochemical regression, and Tg values±20% of the baseline suppressed Tg value just before remnant ablation were considered to have stable biochemical evidence of disease.
Results
Patient characteristics
The clinical description of 27 thyroid cancer patients with structurally evident distant metastases that were negative on DxWBS and positive on post-therapy scanning at the time of RAI remnant ablation is given in Table 1. The median age at diagnosis was 54 years (mean 50±20; range 9–77 years). At the time of diagnostic RAI scanning, the percent neck uptake ranged between 0.064% and 7.4% (median 0.49%). Pulmonary metastases accounted for the majority of the distant metastases (86%), with 70% (16/23) of those with micronodular pattern (the metastasis size range between 3 and 7 mm). Two patients had bone metastasis alone (both >1 cm), and 2 had mixed bone and lung metastasis. Lesion-specific dosimetry was not available in this patient cohort. Only 45% of the tumors were classic papillary thyroid cancers, while the remainders were either poorly differentiated (21%), tall-cell variant papillary thyroid cancer (15%), follicular variant of papillary thyroid cancer (15%), or Hurthle cell cancer (4%). The nonstimulated Tg values were quite variable with a median Tg on levothyroxine before ablation of 5.4 ng/mL (range <0.6–10,090). Before ablation, 55% of the nonstimulated Tg values were <10 ng/mL, 40% were between 11 and 93 ng/mL, and 10% were between 280 and 10,090 ng/mL. None of the patients demonstrated interfering anti-TgAbs.
Tg, thyroglobulin; rhTSH, recombinant human thyroid-stimulating hormone; FDG, fluorodeoxyglucose; PET, positron emission tomography.
When performed (n=12), the PET scan showed FDG-avid distant metastases in 83% (10/12). Out of these 10 patients, 3 had PET-positive bone metastasis, and 5 had PET-positive lung lesions >1 cm in size. RAI remnant ablation was performed using the recombinant human thyroid-stimulating hormone (rhTSH) in 52% (14/27). The median administered activity was 150 mCi (range 75–300). As would be expected, these patients often received additional RAI therapies (median-2 RAI treatments, range 1–9) and had a median cumulative RAI administered activity of 426 mCi (see Table 1). The median follow-up duration after remnant ablation was 3.7 years (range 1.1–17 years).
Objective outcomes after RAI
When evaluating the objective benefits of the distant metastases to RAI remnant ablation, disease progression was noted in 56% (n=15), while 44% (n=12) had persistent stable lesions on serial cross-sectional imaging studies (see Table 2). None of the patients demonstrated objective structural evidence of disease regression in response to RAI ablation, and none of the patients were rendered NED from thyroid cancer by this initial administered activity of RAI. In the 15 patients who demonstrated structural disease progression, the median time to progression was 6 months (mean 9.5±8 months; range 6–36 months).
RAI, radioiodine.
As can be seen from Table 3, patients demonstrating structural disease progression after RAI remnant ablation were older, more likely to have aggressive histologies (Hurthle cell carcinoma, poorly differentiated thyroid cancer, and tall-cell variant papillary thyroid cancer), more likely to have an abnormal FDG-PET scan, and were also prescribed larger administered activities of RAI for ablation than patients demonstrating structurally stable lesions. None of the following differed significantly between the groups: gender, method of preparation (rhTSH vs. thyroid hormone withdrawal), size of the primary tumor, percent uptake in the thyroid bed at the time of ablation, or duration of follow-up.
PTC, papillary thyroid carcinoma; FV, follicular variant; HCC, Hurthle cell carcinoma; PDTC, poorly differentiated thyroid cancer; TCV, tall cell variant.
After RAI remnant ablation, Tg levels were generally stable or slowly declined over time in patients with stable persistent lesions (see Fig. 1). However, the Tg response was more variable in patients with structural disease progression, showing an increase in 6 patients, and a decrease in 3 patients.
Changes in suppressed thyroglobulin (Tg) values in response to radioiodine remnant ablation.
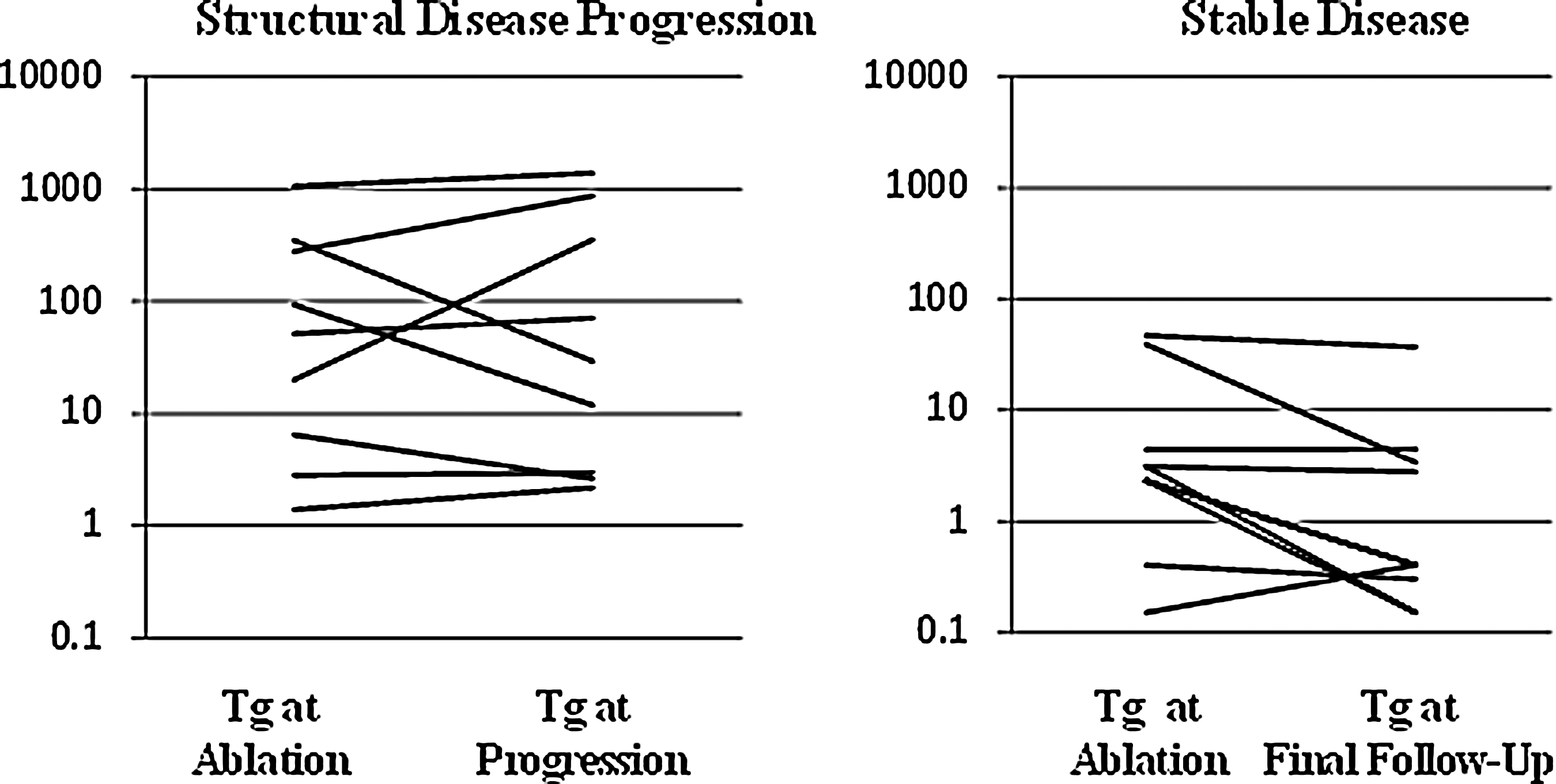
Not surprisingly, additional RAI treatments were given to 12/15 patients with progressive disease and 5/12 patients with stable lesions (see Fig. 2). Patients with initially progressive disease continued to have disease progression despite additional RAI therapy. In no patient did additional RAI therapy appear to slow the rate of disease progression on serial cross-sectional imaging studies. Furthermore, patients with stable lesions continued to have stable findings on serial cross-sectional imaging studies, with no patient showing disease regression (see Table 3).

Schematic of results.
At the time of final clinical follow-up, 30% of the patients were alive with continued disease progression; 41% were alive with persistent stable lesions; 26% had died from progressive thyroid cancer; and 3% (1 patient) died a nonthyroid cancer-related death with stable persistent biopsy-proven metastatic thyroid cancer. All of the disease-specific deaths were in the cohort of patients who had structural disease progression in response to RAI remnant ablation. None of the patients with stable persistent lesions at distant sites have died of thyroid cancer over this relatively short follow-up period (median 3.7 years).
Discussion
To our knowledge, this is the first study to examine the objective outcomes of repeat RAI therapy on structurally evident distant metastases that were negative on DxWBS and positive on post-therapy scanning at the time of RAI remnant ablation. Despite demonstrating RAI avidity on the post-therapy RAI scan, 56% of these patients demonstrated disease progression by a median of 6 months after ablation. Even though 44% of the patients had stable lesions after RAI remnant ablation, none of the patients had regression of the structural lesions, and none had complete resolution of lesions on cross-sectional imaging. Furthermore, additional RAI treatments were also ineffective in either causing disease regression or even in changing progressive disease to stable disease. These data suggest that while empiric RAI therapy in patients with diagnostic RAI scan-negative macroscopic distant metastases may provide localizing information, the lesional dosimetry achieved is nearly always below the threshold necessary to produce structural disease regression or cure.
In the absence of the control group of untreated patients with documented metastatic thyroid cancer, we cannot fully determine the impact of initial RAI ablation on overall disease progression in this cohort. Stability of lesions after RAI ablation may be explained by either natural history of otherwise nonprogressive RAI-insensitive disease, persistence of low-volume indolent disease versus scarring after adequate RAI response. It is possible that some these patients, if left untreated, may have presented with disease progression overtime. Nevertheless, since repeated doses were not associated with resolution of the structural lesions, it is likely that the risks associated with repeated empiric RAI therapies may outweigh any potential benefit in most of these patients with persistently stable lesions.
In addition to the lack of visualization of macroscopic metastatic lesions on the DxWBS, this cohort of patients also had several other clinical features that are often associated with poor response to RAI. As opposed to cohorts of younger patients with RAI avid, classical papillary thyroid cancer, this cohort of patients were older (median 54-year old at diagnosis), more likely to be male (59%), more likely to be FDG PET positive (83%), and enriched in more aggressive histological phenotypes (21% poorly differentiated, 15% tall-cell variant, and 4% Hurthle cell cancer). The clinical importance of these additional clinical features is emphasized by the observation that patients with structurally progressive disease were older and more likely to have an aggressive histological phenotype than patients with structurally stable disease (see Table 3). Furthermore, disease progression was seen in all of the patients with Hurthle cell cancer, poorly differentiated thyroid cancer, and tall-cell variant of papillary thyroid cancer despite the uptake of RAI visualized on the post-therapy scan.
Unlike patients with well-differentiated classical papillary thyroid cancer, the serum Tg values in this cohort of patients were much less reliable at either indicating the presence or likelihood of progression of the distant metastases. While patients with stable lesions generally had Tg levels that were stable or declining over time, the patients with progressive disease exhibited a pattern of Tg responses that ranged from increasing, to stable, to frankly declining. Therefore, serum Tg values cannot be relied upon to assess the extent or likelihood of structural disease progression in this cohort of patients with macroscopic distant metastases that are negative on the DxWBS/positive on the post-therapy scan.
Since more than half of the patients with macroscopic distant metastases who have a negative DxWBS/positive RAI scan at the time of remnant ablation will demonstrate structural disease progression early during follow-up, strong consideration should be given to repeat cross-sectional imaging 3–6 months after ablation to identify patients having early disease progression, especially in older patients with aggressive primary histologies. It is important to identify these patients with early disease progression who have failed RAI so that they can be considered for systemic therapies and clinical trials (with tyrosine kinase inhibitor therapy with or without RAI, combination chemoradiation therapy or chemotherapy alone) and not subjected to additional ineffective doses of RAI. Even over the relatively short period of follow-up in this study, the disease-specific mortality was 46% (7/15) in the patients with structurally progressive disease, further emphasizing the importance of strongly considering additional treatments beyond standard RAI therapy to this high risk cohort of patients.
In summary, repeat empiric RAI dosing in the small subset of patients with DxWBS-negative/post-therapy scan-positive macroscopic distant metastases is not associated with cure, regression of stable lesions, or conversion from progressive to stable disease. Even though the risks associated with repeat RAI activities are relatively small, the lack of demonstrable clinical benefit would argue that the risks of additional RAI therapies may outweigh the benefits in this clinical scenario. Furthermore, the high disease-specific mortality rate seen within the first few years of remnant ablation in patients with persistent disease progression argues strongly for an early referral to medical oncology for consideration of alternative systemic therapies, rather than repeating what are most likely to be ineffective treatments with RAI. In the near future, we anticipate using individual lesional dosimetry determined by 124I PET scanning in a routine clinical practice to be able to more specifically predict the responsiveness of metastatic lesions to additional therapeutic RAI (20,21).
Footnotes
Disclosure Statement
No competing financial interests exist for M.M.S., R.K.G., H.T., and S.M.L. R.M.T. is a consultant to, and receives honorarium for speaking from Genzyme Corporation.