
Abstract
Background:
Although functioning thyroid cancer metastases have been reported, they have almost never been reported for the clear cell variant of papillary thyroid carcinoma (PTC). Here we describe a patient with disseminated lung metastases of the clear cell variant of PTC who presented in the euthyroid state despite discontinuance of levothyroxine after total thyroidectomy.
Patient Findings:
A 49-year-old woman underwent total thyroidectomy for the clear cell variant of PTC in March 2002. Levothyroxine replacement was initiated after total thyroidectomy, but the patient was lost to follow-up 5 years after the operation. She did not take any levothyroxine for 4 years. Upon presentation to our institution, her initial thyroid function tests were a serum thyroid-stimulating hormone (TSH) of 4.51 mIU/L (0.30–5.00), total triiodothyronine of 82 ng/dL (60–181), and free thyroxine of 1.21 ng/dL (0.89–1.76). The results of workups, including thyroid ultrasonography, chest computed tomography (CT) scan, and fluorine-18 fluorodeoxyglucose positron emission tomography (18F-FDG PET)/CT, revealed that she had multiple metastases in the cervical lymph nodes and both lungs. She received 0.9 mg of recombinant human TSH (rhTSH) for 2 consecutive days followed by administration of 200 mCi 131I. A therapeutic whole body scan after 131I administration demonstrated intense uptake in the whole lung fields, suggesting functioning lung metastases.
Summary:
It is extremely rare for metastatic PTC, even though it is a well-differentiated thyroid carcinoma, to produce a sufficient amount of thyroid hormones to result in euthyroid state after total thyroidectomy. To our knowledge, this is the first report of functioning lung metastases of the clear cell variant of PTC after total thyroidectomy that produced enough thyroid hormone to restore a euthyroid state.
Conclusion:
Functioning metastases from recurred PTC, particularly of the clear cell variant, are very rare. When they occur, rhTSH is required to prepare these patients for treatment with ablative doses of radioactive iodine (131I).
Introduction
There are many histological variants in PTC; these are described in a recent edition of the World Health Organization (WHO) classification of PTC (13). Among them, the clear cell variant of PTC is rare, accounting for 0.06% of all PTCs (14). Here we describe a patient with metastatic clear cell variant of PTC who presented in the euthyroid state despite her having discontinued levothyroxine after having a total thyroidectomy.
Patient
A 49-year-old woman presented with cough and mild dyspnea. She had undergone a total thyroidectomy 9 years previously, in March 2002. In the thyroidectomy specimen, a 1.5-cm tumor in the left lobe was noted. The tumor was predominantly (>50%) composed of cells showing clear cytoplasm and nuclear features of PTC. The tumor's histological appearance was consistent with the clear cell variant of PTC. The tumor invaded the capsule of the thyroid gland and extended into the surrounding soft tissue (Fig. 1A). The patient refused 131I remnant ablation therapy. Levothyroxine replacement (200 μg daily) was started after total thyroidectomy. The patient was lost to follow-up 5 years after surgery. She took levothyroxine during the follow-up period of 5 years after total thyroidectomy. However, she did not take any levothyroxine for 4 years after follow-up loss, until her first visit to our institution.

Histopathological and immunocytochemical findings.
On presentation to our institution, her initial thyroid function tests were a serum thyroid-stimulating hormone (TSH) of 4.51 mIU/L (reference range [RR] 0.30–5.00), total triiodothyronine (T3) of 82 ng/dL (RR 60–181), and free thyroxine (T4) of 1.21 ng/dL (RR 0.89–1.76). Her serum thyroglobulin (Tg) concentration was elevated to 986.61 ng/mL. Anti-Tg antibody, antithyroid stimulating hormone receptor antibody (TRAb), and microsomal antibody were all negative. Repeat thyroid function tests one week later were a TSH of 4.46 mIU/L, total T3 of 96 ng/dL, and free T4 of 1.09 ng/dL. These tests were consistent with the euthyroid state or very mild primary hypothyroidism. She was started on levothyroxine of 100 μg daily. On this dose here serum TSH was suppressed to 0.15 mIU/L.
A chest X-ray showed multiple bilateral tiny nodules, suggestive of metastatic disease (Fig. 2A). These findings were better defined by a computed tomography (CT) scan of the chest (Fig. 2B). Fluorine-18 fluorodeoxyglucose positron emission tomography (18F-FDG PET)/CT showed hypermetabolic masses (SUVmax=1.1) in both lung fields, suggesting metastases of thyroid cancer (Fig. 2C). Thyroid ultrasonography (US) revealed multiple enlarged lymph nodes, ranging from 0.7 to 1.0 cm, in the central compartment and left level III. US-guided fine needle aspiration (FNA) of a left level III lymph node showed metastatic PTC (Fig. 1B). On immunocytochemistry for a cell block section, the tumor cells were strongly immunoreactive for Tg (Fig. 1C).
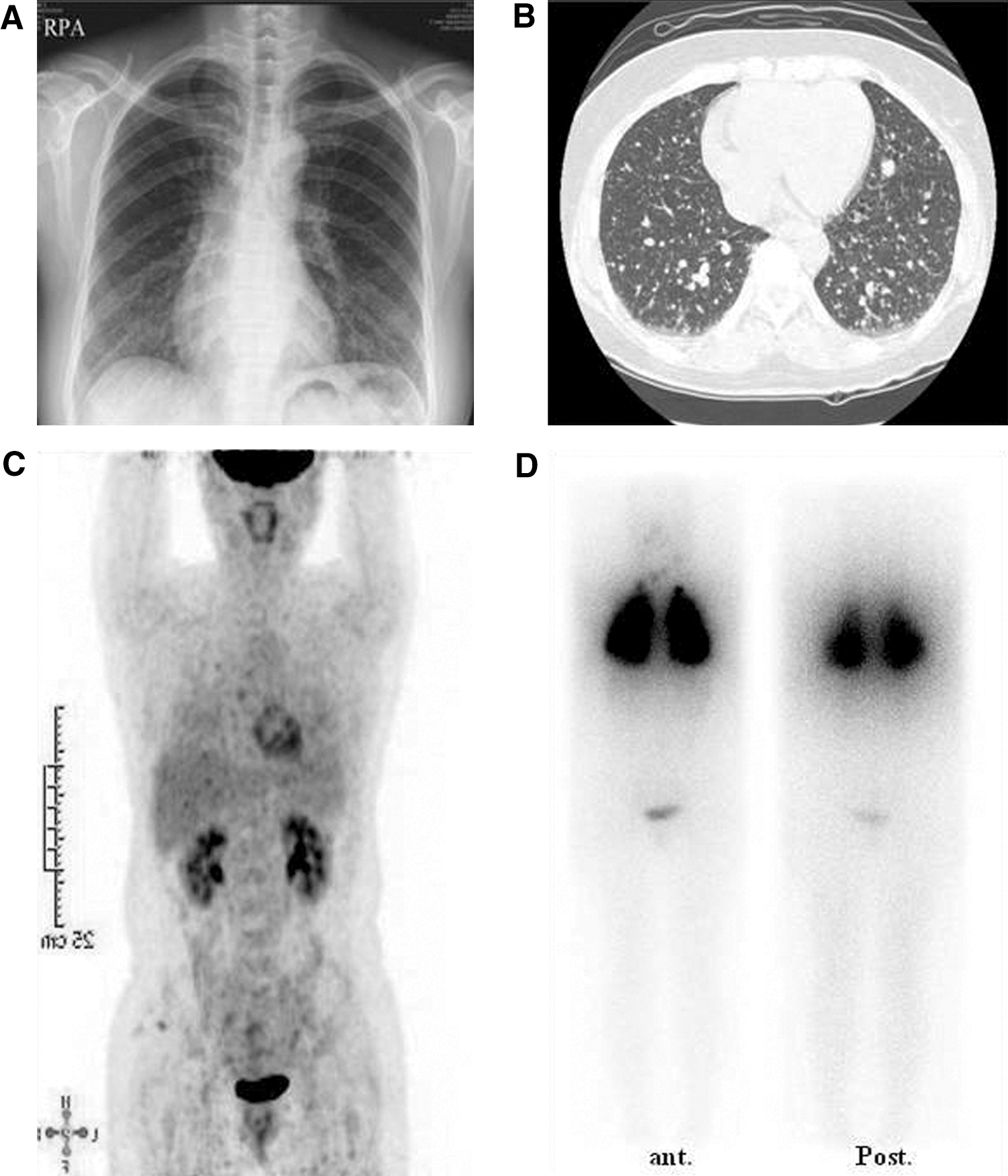
Imaging studies of the metastatic tumor.
After a low-iodine diet for 2 weeks, the patient received 0.9 mg of recombinant human TSH (rhTSH; Thyrogen®; Genzyme Corporation, Cambridge, MA) for 2 consecutive days followed by administration of 200 mCi 131I. The serum TSH, T3, and free T4 measured on the day after the second rhTSH injection were >150 mIU/L, 121 ng/dL, and 1.01 ng/dL, respectively. The serum Tg and anti-Tg antibody measured 3 days after the second rhTSH injection were 3108.4 ng/mL and 81.4 IU/mL (RR 0–60), respectively. A therapeutic whole body scan (TxWBS) 5 days after 131I administration showed intense uptake in the lung fields (Fig. 2D). Seven days after 131I administration, the patient's dry cough and dyspnea worsened. Radioactive iodine therapy–induced pulmonary damage could not be ruled out; therefore, she was treated with prednisolone. Her symptoms improved. A follow-up chest CT scan 3 months after 131I ablation therapy showed decreases in the numbers and sizes of the lung metastases. The serum Tg level on levothyroxine also decreased to 360.3 ng/mL.
Discussion
Hyperthyroidism or euthyroidism resulting from hyperfunctioning metastases of differentiated thyroid carcinoma is a rare entity (1). Follicular thyroid carcinoma is the most common type associated with this kind of hyperthyroidism (3 –11). However, there are only a few reports of hyperthyroidism caused by metastatic PTC (12,15). Basaria and Salvatori described a 74-year-old man with conventional PTC with functional lung metastases causing severe hyperthyroidism complicated by Graves' disease (15). Girelli et al. noted a case of hyperthyroidism with a functioning pelvic metastasis of PTC (12). In all the cases reported to date the appearance of the functional metastases preceded or occurred simultaneously with the diagnosis of thyroid cancer.
There are several histological variants of PTC (13). Among them, the clear cell variant of PTC is rare and is characterized histologically by cells showing clear cytoplasm and nuclear features of PTC (16). To the best of our knowledge, this is the first reported case in which lung metastases from the clear cell variant of PTC produced enough thyroid hormone to meet or almost meet thyroid hormone requirements.
There are several potential mechanisms that might be involved in the rare situations where physiological or supraphysiological amounts of thyroid hormone are produced by metastatic thyroid cancer. Metastatic thyroid cancers may function autonomously to produce thyroid hormone (5,7,10,12). In addition, the TSH receptor in the metastatic tumor may induce the formation of TRAb, favoring the production of even greater amounts of thyroid hormone by the metastatic tissue (6,9,11,15). Finally, some metastases from follicular thyroid carcinoma express 5′-iodothyronine deiodinase activity. If patients with these tumors receive levothyroxine, there could be an increase in the conversion of this to T3 in the metastatic tumor tissue (17,18). Our patient's thyroid status was maintained in the euthyroid or near euthyroid state in the absence of thyroid hormone replacement. Notably, the patient had intense uptake in the metastatic lesions in the TxWBS but there was no 131I activity in the thyroid bed in this test nor did US show regrowth of thyroid tissue. Of note, she did not have TRAb.
Therapy for differentiated thyroid carcinoma with hyperfunctioning metastases aims to treat both the hyperthyroidism and the neoplastic lesions. In most reported cases, 131I ablation therapy is effective in normalizing thyroid hormone values and reducing the size of metastases (9). In our patient, treatment with 200 mCi 131I by the oral route was effective in reducing her metastases, as confirmed by the chest X-ray and chest CT that demonstrated a decrease not only in the size but also the number of visualized metastases.
In previous studies, survivors with functioning metastases had significant reductions of thyroid hormone levels after administration of therapeutic doses of radioiodine. Of note, the overall survival of patients with functioning metastases from differentiated thyroid carcinoma does not differ from that of euthyroid patients with metastatic differentiated thyroid carcinoma (1). In addition, the clear cell variant of PTC behaves similarly to conventional PTC (19).
The clear appearance of the cytoplasm of the clear cell variant of PTC may mimic metastatic carcinoma, particularly from the kidney (20). In this patient, there was no evidence of renal cancer on 18F-FDG-PET/CT, and the immunocytochemical staining for Tg and cytokeratin19 was strongly positive. Therefore, we excluded the diagnosis of metastatic carcinoma of kidney.
In conclusion, we report an unusual case of a patient with the clear cell variant of PTC with disseminated lung metastases who presented in the euthyroid state despite discontinuing levothyroxine after total thyroidectomy. Although functioning metastases of thyroid cancer are rare, clinicians should be aware of the possibility that PTC with massive metastases may produce sufficient thyroid hormone to maintain the euthyroid state, even after total thyroidectomy.
Footnotes
Disclosure Statement
The authors have no financial conflicts of interest to disclose.