
Abstract
Background:
Iodine-131 (131I) total-body scintigraphy is a commonly used post-thyroidectomy imaging procedure in the management of differentiated thyroid cancer (DTC), in particular in patients with an intermediate or high risk of persistent or recurrent disease, in combination with serum thyroglobulin (Tg) determinations and ultrasonography of the neck. It can show the persistence of residual thyroid tissue after thyroidectomy and local and distant metastases. Although this is a highly sensitive method for detecting normal and pathologic thyroid tissue, especially when performed after an ablative dose of 131I, false-positive scans (i.e., uptake in the absence of residual thyroid tissue or metastases) can occur in different situations.
Patient Findings:
We report a case of a 42-year-old woman with recurrent chest infections and bronchiectasis, who had a total thyroidectomy and 131I treatment because of a papillary thyroid carcinoma. She presented with marked bilateral 131I uptake in the lungs mimicking metastatic involvement of the lungs by thyroid cancer, but interpreted as nonspecific bilateral uptake by her bronchiectatic bronchial tree.
Summary:
Our case, as well as others reported in the literature, calls attention to the fact that 131I lung uptake may be related to chronic inflammatory lung disease, thus representing a potential diagnostic pitfall in patients with DTC.
Conclusions:
131I uptake should be interpreted on the bases of clinical context, imaging, and laboratory findings (serum Tg). Recognition of potential false-positive 131I scans is critical to avoid unnecessary exposure to further radiation from repeated therapeutic doses of 131I with possible side effects and even worsening of lung disease itself.
Introduction
131I total-body scintigraphy after 131I ablation is a commonly used post-thyroidectomy imaging procedure in the management of DTC. The main diagnostic tools in the follow-up of these patients are serum thyroglobulin (Tg) determinations (during suppressive therapy or after recombinant human TSH [rhTSH] administration) and ultrasonography of the neck, whereas a diagnostic 131I total-body scintigraphy is not routinely performed, but can be useful notably in patients with intermediate or high risk of persistent or recurrent disease. It can show the persistence of residual thyroid tissue after total thyroidectomy and local and distant metastases. Although this is a highly sensitive method for detecting normal and pathologic thyroid tissue, even more when performed after 131I ablation, iodine uptake can be seen in other organs possessing the sodium–iodide symporter (NIS). Besides normal physiological uptake in salivary glands, the stomach, choroid plexus, and lactating and nonlactating breast tissue, atypical uptake of 131I can be due to a wide spectrum of physiological processes and nonthyroidal disease conditions, simulating metastases from DTC.
A proper understanding of the causes of these potentially misleading artifacts is essential for an accurate interpretation of the images to avoid diagnostic errors that may lead to unnecessary administration of 131I therapeutic doses or surgical procedures.
Patient
A 42-year-old woman, with recurrent chest infections and bronchiectasis, had a total thyroidectomy because of a thyroid nodule in the right thyroid lobe. This was diagnosed as papillary thyroid carcinoma (PTC) by fine-needle aspiration biopsy. A preoperative ultrasonography evaluation did not show involvement of the lymph nodes of the neck.
The histological examination confirmed the diagnosis of PTC of the right thyroid lobe, 13 mm in diameter, without infiltration of the thyroid capsule or involvement of the lymph nodes of the central compartment.
The patient then had a 131I treatment with 3700 MBq after 6 weeks of L-thyroxine withdrawal (TSH=89.2 mUI/L). The post-therapeutic dose total-body scan showed a residual iodine uptake in the thyroid bed attributable to thyroid remnant, compatible with the Tg serum level (Tg=6.5 ng/mL), and a low bilateral uptake in the lung fields (Fig. 1). A test for anti-Tg antibodies (TgAb) was negative.
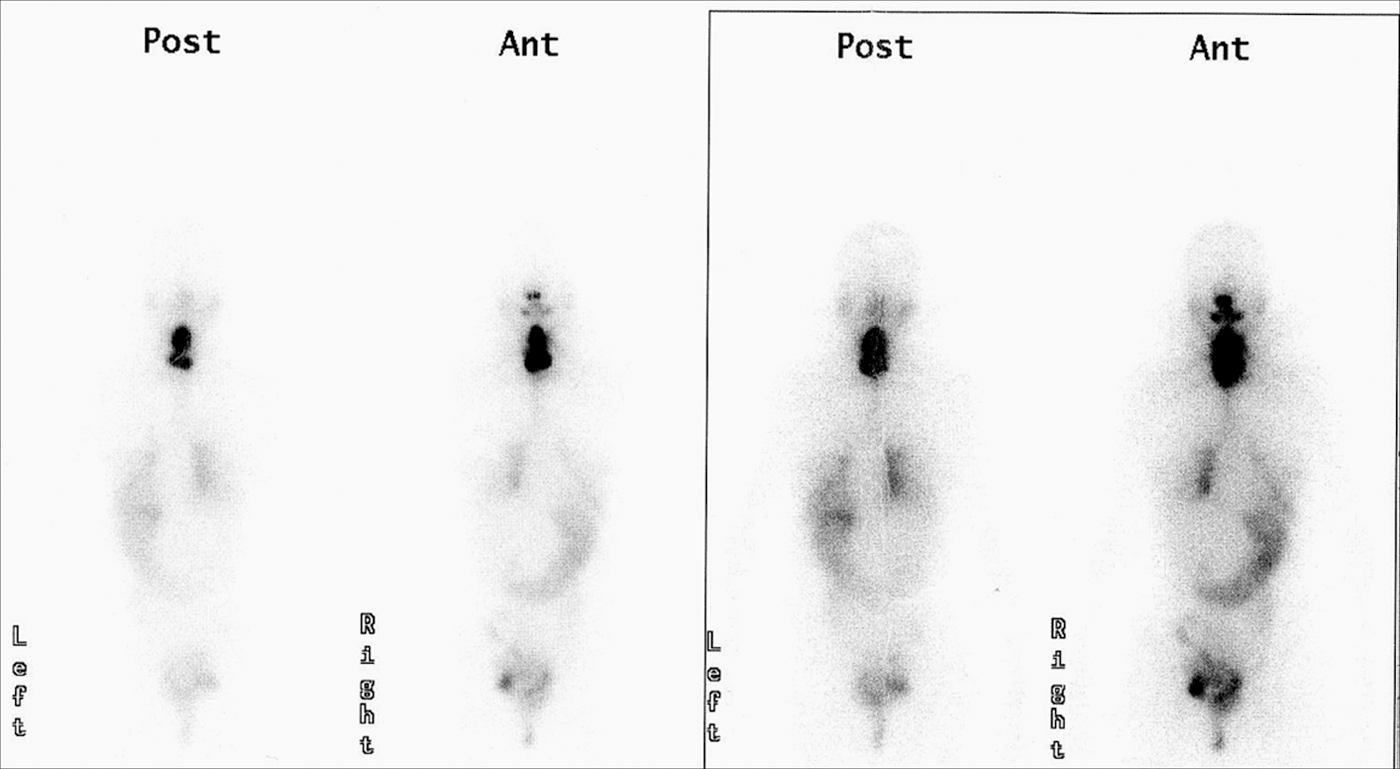
131I total body scintigraphy shows a residual iodine uptake in the thyroid bed caused by thyroid remnant and a low bilateral uptake in the lung fields.
In consideration of the lung uptake, it was decided to perform a 131I total-body scan (185 MBq) after rhTSH administration. This was done 4 months after she received the therapeutic dose of 131I. The scan showed diffuse marked uptake in the lungs. At that time, the serum Tg was below the detection levels, and the TgAb test was negative (Fig. 2).
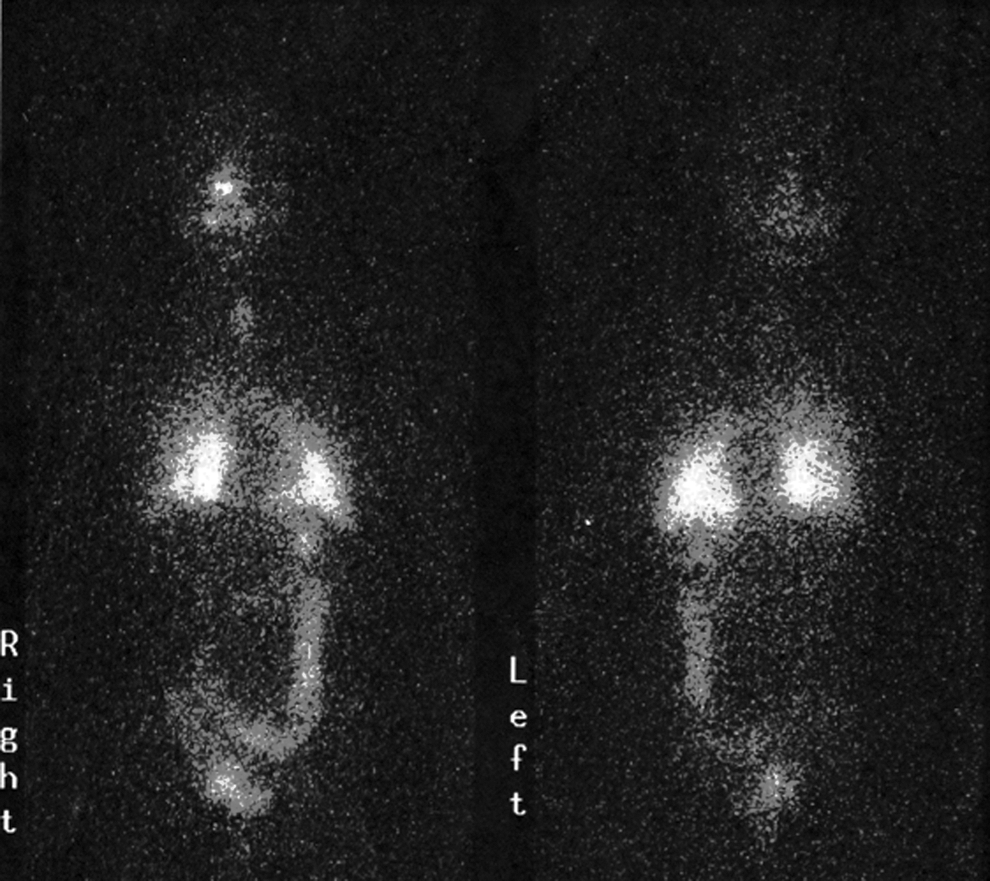
131I total-body scintigraphy performed 4 months later shows a marked and diffuse lung uptake.
A computed tomography (CT) of the chest confirmed the bronchiectatic appearance of the bronchial tree, with no metastatic involvement of the lungs. No further therapeutic dose of 131I was administered, considering that the lung uptake was attributable to the bronchiectasies. A neck ultrasonography evaluation did not show involvement of cervical lymph nodes.
The patient was then followed with periodic neck ultrasonography and serum Tg level and TgAb determinations during TSH-suppressive treatment, according to the guidelines for the management of thyroid cancer (1,2). Two years later, however, in consideration of this being an unusual case, even though the Tg was undetectable, it was decided to perform another 131I scan after rhTSH. It showed the same picture of diffuse uptake of 131I in the lungs (Fig. 3), with undetectable stimulated serum Tg and negative TgAb, whereas another CT of the chest confirmed the presence of bronchiectasies with no other lesions consistent with metastatic involvement of the lungs (Fig. 4).
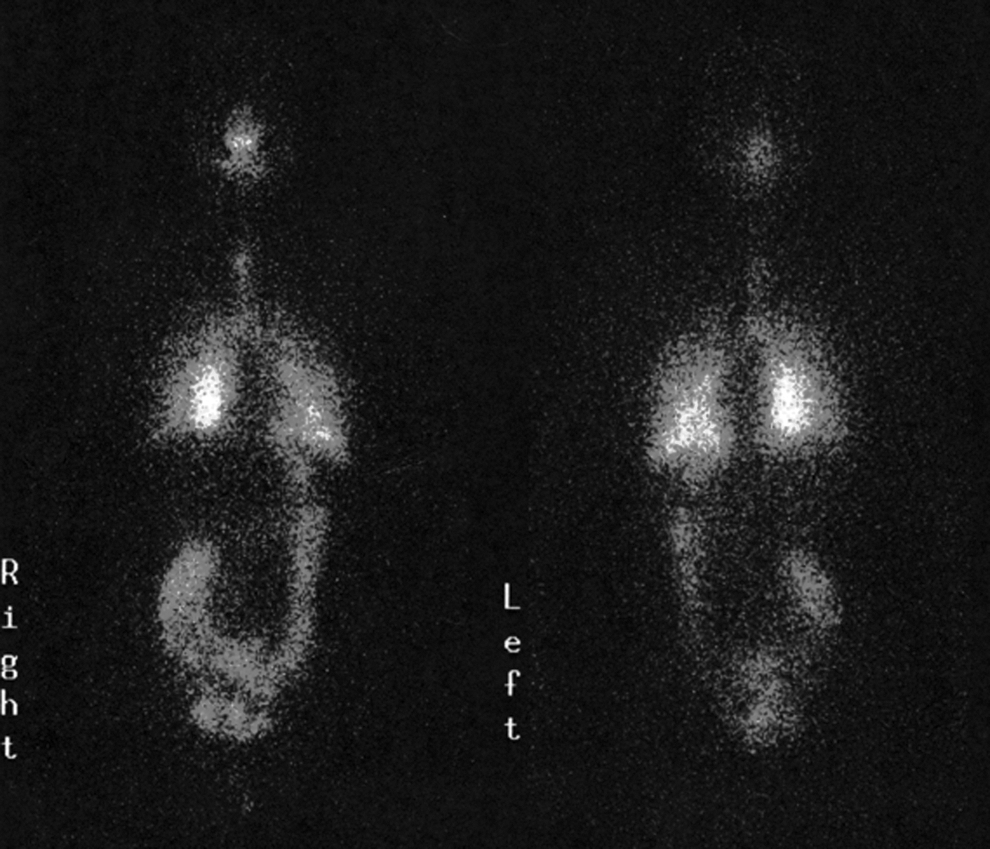
131I scan performed 2 years later shows the same picture of diffuse lung uptake.
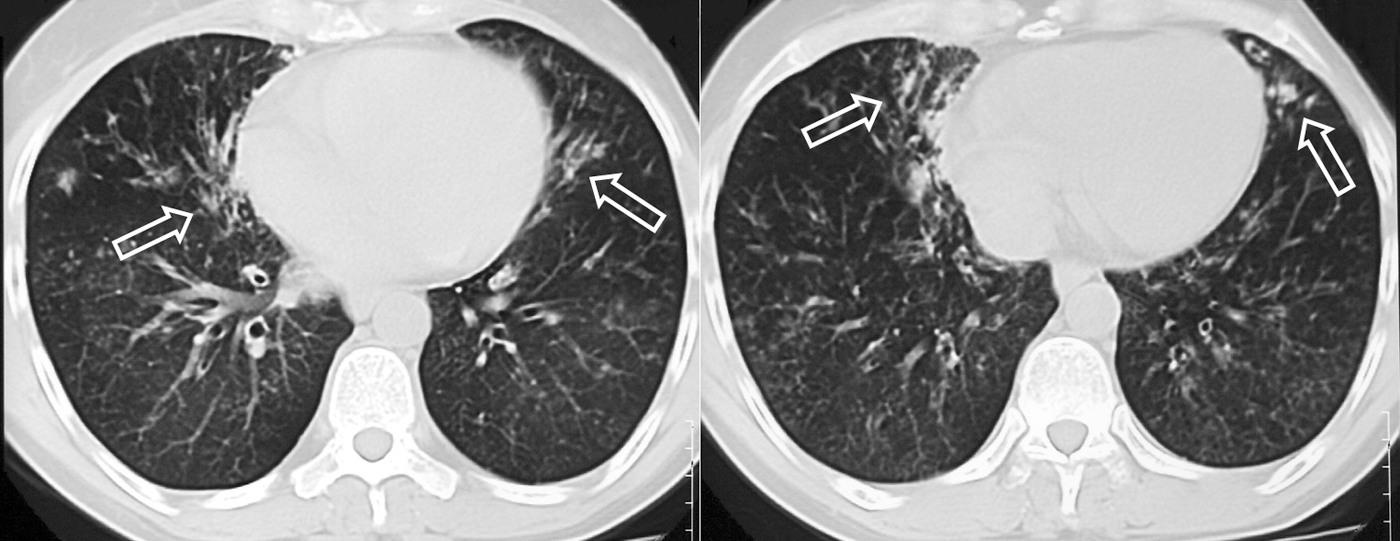
Chest computed tomography transverse scan confirms the presence of bronchiectasis (arrows), with no other lesion referable to metastatic involvement of lung parenchyma.
Discussion
Although 131I activity detected outside the thyroid bed is usually attributed to metastatic disease, false-positive localization of 131I has been described in the absence of residual thyroid tissue or metastases from DTC, and may be a potential pitfall that can lead to unnecessary 131I therapy or surgical procedures.
The mechanisms involved are usually one of several. 131I uptake can be related to NIS expression in ectopic thyroid tissue localized at the base of the tongue, along the course of the thyroglossal duct or laterally in the neck, as well as in the mediastinum or the subdiaphragmatic organs. This is due to developmental defects at early stages of thyroid embryogenesis and occurs during its passage from the floor of the primitive foregut to its final pretracheal position. In some cases, an orthotopic thyroid coexists with thyroid ectopy (3). Another rare condition involving NIS expression in thyroid tissue is struma ovarii (4,5).
The second mechanism is the iodine uptake in nonthyroidal tissues that express NIS. Normal physiological uptake occurs in the salivary gland, lacrimal gland, nasopharynx, the stomach, the choroid plexus, and lactating breast tissue. NIS can be even overexpressed in diseases involving these organs (6,7). Abnormally located gastric mucosa may retain NIS function, explaining iodine uptake by hiatal hernia (8), Meckel's diverticulum (9), and metaplastic gastric mucosa in Barrett's esophagus (10).
Neoplasms arising from tissues normally expressing NIS can retain NIS function, therefore having 131I uptake. These include gastric adenocarcinoma (11), Warthin's tumor (12), teratomas (13), breast malignancies (14), and adenocarcinoma of the lungs (15).
In some instances, foci of 131I activity are not related to the presence of NIS. This is the case for contamination artifacts due to physiological secretions (16 –18), such as saliva, nasal secretions, sweat, urine, and vomitus.
Artifacts can also be related to retention of 131I in physiological secretions accumulated in dilated ducts or cavities. This is the case for urinary tract anomalies, such as diverticuli, fistulae, and hydronephrosis (19), gastrointestinal anomalies, such as Zenker's diverticulum, esophageal motility disorders, achalasia of the cardia (20,21), or salivary ductal pathology (stones, tumors, etc.) (22). Other false-positive scans can be due to accumulation of 131I in pleural, pericardial, and peritoneal effusions (23,24).
In addition, various inflammatory conditions can cause false-positive 131I uptake because of their increased vascularity and capillary permeability. Examples of this are cholecystitis, sebaceous cyst (25,26), infective and inflammatory diseases of the lungs, such as bronchiectasis, fungal lung infections, tuberculosis, and rheumatoid arthritis-associated lung disease (27 –32). 131I lung uptake in case of chronic inflammatory lung disease could be related to the ability of the inflamed bronchial epithelium to take up and secrete iodine in the mucus and inflammatory exudate (27 –32), representing a potential diagnostic pitfall in patients with DTC, giving the fact that lungs are the most frequent sites of DTC distant metastases.
In some cases, the mechanism for 131I uptake remains unknown. This is the case for uptake in the thymus, which is frequently reported when iodine trapping by Hassal's bodies occurs (33,34).
Conclusions
This report draws attention to false-positive results of an 131I scan in patients with DTC who are also affected by infective and inflammatory diseases of the lungs, such as bronchiectasis, fungal lung infections, and tuberculosis. (27 –32). It emphasizes the importance of interpreting the 131I uptake with consideration of the clinical context, imaging, and laboratory findings (serum Tg).
Recognition of false-positive cases, in fact, is of capital importance to avoid further 131I therapeutic doses that are not only devoid of beneficial effects and expensive but also not indicated and potentially associated with side effects such as sialadenitis, gastritis, other malignancies, and even worsening of the pulmonary disease with lung fibrosis. Furthermore, an imprudent diagnosis of lung metastasis, and even an unnecessary exposure to 131I therapy can cause emotional trauma for the patient and may lead to legal disputes.
Footnotes
Disclosure Statement
No disclosure to declare.