
Abstract
Background:
The effectiveness of short-term 3,5,3′-triiodothyroacetic acid (TRIAC) therapy for the treatment of hyperthyroidism caused by thyroid hormone resistance (RTH) has been documented. Here, we report a 3-year course of TRIAC therapy in an RTH boy, with a quantitative evaluation of the therapeutic effects and pharmacological study of TRIAC.
Patient findings:
The gene encoding the thyroid hormone receptor beta (THRB) of the patient carries a P453T mutation. During treatment with up to 3.0 mg TRIAC per day, reduction in the thyroid volume, resolution of supraventricular arrhythmia, and decrease in thyroid-stimulating hormone (TSH) and free-thyroxine (FT4) levels were achieved. In addition, attention-deficit hyperactivity disorder (ADHD) symptoms improved, with a concomitant decline in the ADHD Rating Scale score.
Summary:
A TRIAC pharmacokinetic study, conducted using triiodothyronine level as a surrogate for TRIAC level, demonstrated that TRIAC disappears from the circulation rapidly and has a shorter duration of TSH secretion inhibitory effect in the RTH patient compared to that in the control subject. Studies of TSH and FT4 levels over a period of 3 years indicated that the TRIAC effect is dose dependent.
Conclusions:
TRIAC was effective and safe in ameliorating the effects of hyperthyroidism and ADHD symptoms in a child with known genetic RTH. Further, it was demonstrated that TRIAC has a short half-life and functions dose dependently.
Introduction
Patient report
The patient is a Japanese boy who was born without any complications at 37 weeks of gestational age. He weighed 2884 g (−1.6 standard deviation [SD]) at birth. He had an elder brother with childhood-type hypophosphatasia. Through fetal ultrasonography (US), the patient was found to have shortening of the extremities and was suspected to have hypophosphatasia. This diagnosis was later supported by elevated urinary excretion of phosphoethanolamine and by the identification of a common heterozygous mutation (c.1559delT) in the liver/bone/kidney alkaline phosphatase gene (ALPL). His motor development was slightly delayed; he could keep his head steady at 5 months, and he walked independently at 24 months. At 4 years, he suffered from right-sided Perthes' disease, which necessitated operative intervention. At this time, he was referred to us for evaluation of his short stature. Through the endocrinological work-up, the thyroid function tests showed unexpected results. The serum TSH level was 3.48 μIU/mL (reference range [RR]: 0.43–4.0 μIU/mL), the serum free-T3 (FT3) was 9.62 pg/mL (RR: 2.32–4.60 pg/mL), and the serum free-thyroxine (FT4) was 4.15 ng/dL (RR: 1.01–1.97 ng/dL). Clinical re-evaluation following the thyroid function tests revealed the presence of goiter. At this point, hyperthyroidism was not evident, except for mild tachycardia (heart rate, up to 102/min). RTH was suspected and was confirmed by the TR-β gene analysis that revealed a heterozygous P453T mutation.
From 5 years of age, tachycardia (heart rate, up to 120/min) was repeatedly recorded at outpatient visits. In addition, diaphoresis and repetitive diarrheal episodes had occurred. A child psychiatrist noted that he was hyperactive and impulsive despite normal intellectual development. Treatment with a β-blocker (propranolol, 0.5 mg/kg/day) was started under the diagnosis of PRTH, but it did not decrease the heart rate.
At 8 years of age, his parents sought a second consultation with the child psychiatrist, because the patient had exhibited recent disruptive behaviors such as frequent quarreling with classmates and throwing tantrums. According to the psychiatrist, he was maladaptive, and he presented with distinctive symptoms compatible with attention-deficit hyperactivity disorder (ADHD), such as hyperactivity, inattention, and impulsiveness. The extent of his ADHD symptoms was considered to be inconsistent to his reported intelligence quotient (IQ) of 79–89 (the method used for measuring the IQ is unknown). He did not show any symptoms indicative of autism.
TRIAC therapy was planned, and favorable effects were expected for both hyperthyroidism and ADHD symptoms. The patient was admitted for a short period for pretreatment endocrinological, cardiac, and metabolic evaluations. At the time of admission, he was 9 years old, 112.8 cm (−3.3 SD) tall, and weighed 20.8 kg (body mass index, 50th percentile). His blood pressure (BP) was 105/76 mm Hg, and body temperature was 36.0°C. His pulse rate (PR) was regular (80/min at rest), but it tended to increase frequently (up to 150/min) with light physical activity such as walking. Holter electrocardiography showed frequent supraventricular premature contraction (SVPC) during sleep. He was so hyperactive that he was not able to sit still. Excessive sweating was observed. The thyroid gland was diffusely enlarged and elastically soft on palpation. He did not show exophthalmia or finger tremor. He showed no pubertal development (Tanner stage: genital development 1 and pubic hair development 1), and his testicular volume was 2 mL on each side. Laboratory data were unremarkable, except for high TH levels (FT3=15.8 pg/mL, RR: 2.50–4.77 pg/mL; FT4=5.60 ng/dL, RR: 1.02–1.99 ng/dL) with nonsuppressed TSH (2.68 μIU/mL, RR: 0.46–4.4 μIU/mL). His total cholesterol level was 149 mg/dL (RR: 117–223 mg/dL), and his creatine phosphokinase level was 55 IU/L (RR: 53–283 IU/L). TRIAC was started at a dose of 0.2 mg/day, administered in two equally divided doses (at breakfast and supper). Except for transient nausea in the earlier phase of treatment, no severe adverse events were observed for the next 3 years with an increasing TRIAC dose. His last IQ, measured at 13 years of age, was reported to be 83.
Methods
Evaluation of TRIAC effectiveness
The therapeutic effects of TRIAC were initially monitored monthly and later every 3 months, in an outpatient setting. The patient usually visited in the evening, about 8 hours after administration of the morning TRIAC dose. After blood sampling, his BP and PR were recorded in the sitting position. TSH, FT3, FT4, T3, and thyroxine (T4) levels were measured at an in-house laboratory by electrochemiluminescence immunoassay (ECLIA). Holter electrocardiography and thyroid volume estimation by US were carried out annually. Any effects of the TRIAC treatment on ADHD symptoms were assessed based on the parents' observations. The ADHD Rating Scale-IV (22), translated into Japanese, was also scored by the parents. As the TRIAC dose was gradually increased, TSH and FT4 values were evaluated during each of the three periods during which he was given increasing doses of TRIAC in a stepwise fashion. During the initial 4 months, he received TRIAC, 0.7–1.0 mg/day. During the next 4 months, he was given TRIAC, 1.5–2.5 mg/day, and during the last 18 months, he was given TRIAC, 3.0 mg/day.
Spiked recovery test to determine if serum T3 levels reflect serum TRIAC levels
During TRIAC therapy, the values for the patient's serum T3 level increased to above the range of the T3 assay. We hypothesized that this was due to crossreactivity of TRIAC with T3 in the T3 ECLIA. To determine the extent to which serum T3 reflects the serum TRIAC level, we tested the recovery of added TRIAC in T3 assay. Increasing doses of TRIAC (5, 10, 20, 40, and 80 ng) were added to 10 mL of pooled serum. In each sample, concentrations of T3 and T4 were measured by ECLIA (Elecsys® T3 and T4; Roche Diagnostics, Tokyo, Japan) and chemiluminescent immunoassay (CLIA) (Chemilumi E-T3® and Chemilumi ACS-T4®; Siemens Healthcare Diagnostics, Tokyo, Japan). Antibodies used in ECLIA and CLIA were ovine polyclonal and murine monoclonal antibodies, respectively. The same procedure was performed using hypothyroid serum (T3 0.39 ng/mL and T4 0.76 μg/dL) instead of pooled serum. All assays were conducted in duplicate. The recovery rate was expressed as the percentage of the observed increment in T3 concentrations to the expected values. Table 1 summarizes the assay kits used in this report.
CLIA, chemiluminescent immunoassay; ECLIA, electrochemiluminescence immunoassay; T3, triiodothyronine; T4, thyroxine; TRIAC, 3,5,3′-triiodothyroacetic acid.
Pharmacokinetic study of single TRIAC dose
As a control for these studies, 1.0, 2.0, and 4.0 mg of TRIAC were administered to a normal adult male volunteer on separate occasions. Serum samples were obtained before and 1, 2, 3, 6, and 24 hours after the administration of TRIAC, and samples were assayed in the T3 ECLIA. For the sera, which showed readings for T3 above the measurable range, T3 was measured after dilution with hypothyroid serum, and the measured value was then converted appropriately. The TSH level in each sample was also determined. For determination of T3 and TSH levels, samples were assayed in duplicate. Our RTH patient also underwent this study for 3 years after the initiation of TRIAC, at which time he was 12 years old and weighed 29 kg. He received 1.5 mg of TRIAC in the morning, and serum samples were obtained 0, 1, 2, 3, 6, 12, and 24 hours later for T3 and TSH determination.
Statistical analysis
Statistical analysis was carried out using Microsoft Office Excel 2007® (Microsoft Corporation, Tokyo, Japan) and Statcel® (an add-in forms feature on Excel, 2nd edition; OMS Publishing, Tokyo, Japan). Values are expressed as mean±SD. Mean values of FT4 and T4 levels at the different TRIAC doses were compared by the Kruskal-Wallis test, followed by Bonferroni and Tukey-Kramer corrections. Results of the spiked recovery test were evaluated by linear regression analysis. Mean TSH levels before and 24 hours after single TRIAC administration were compared by Mann–Whitney U-test. p-values of less than 0.05 were considered to be significant.
Approval
The Ethics Committee of the Kanagawa Children's Medical Center reviewed and approved the study protocol. Written informed consent was obtained from the parents of the patient as well as from the volunteer who participated in the pharmacokinetic study.
Results
Clinical effectiveness of TRIAC
We aimed to maintain TSH levels, measured on clinic visits, below 3.0 μIU/mL, which was an arbitrarily set value. To achieve this target, we needed to raise the TRIAC dose gradually up to 3.0 mg/day (Fig. 1). Despite the gradual increase in the TRIAC dose, an occasional decrease in FT3 levels was noted, which was interpreted as inadequate patient compliance. Nevertheless, after TRIAC therapy, some favorable effects were noted. At first, shrinkage of the goiter was noticed at 3 months after TRIAC introduction. This was confirmed by consecutive US studies (Table 2). Although BP and PR did not vary significantly (data not shown), Holter electrocardiography demonstrated a decrease in the mean heart rate as well as the dissolution of SVPC (Table 2). Diaphoresis and diarrhea subsided soon after TRIAC therapy was started. Improvements in hyperactivity and impulsiveness were noticed by the parents around 6 months after TRIAC treatment was started. Disruptive behaviors were not reported thereafter. ADHD Rating Scale-IV showed a marked decrease in the scores over a 3-year period (Table 2). More than 85% of TSH values were below 3.0 μIU/mL, as originally aimed (Table 3). FT4 and T4 levels during the last 18 months (with TRIAC 3.0 mg/day) were significantly lower than those during the initial 4 months (with TRIAC 0.7–1.0 mg/day; Table 3).
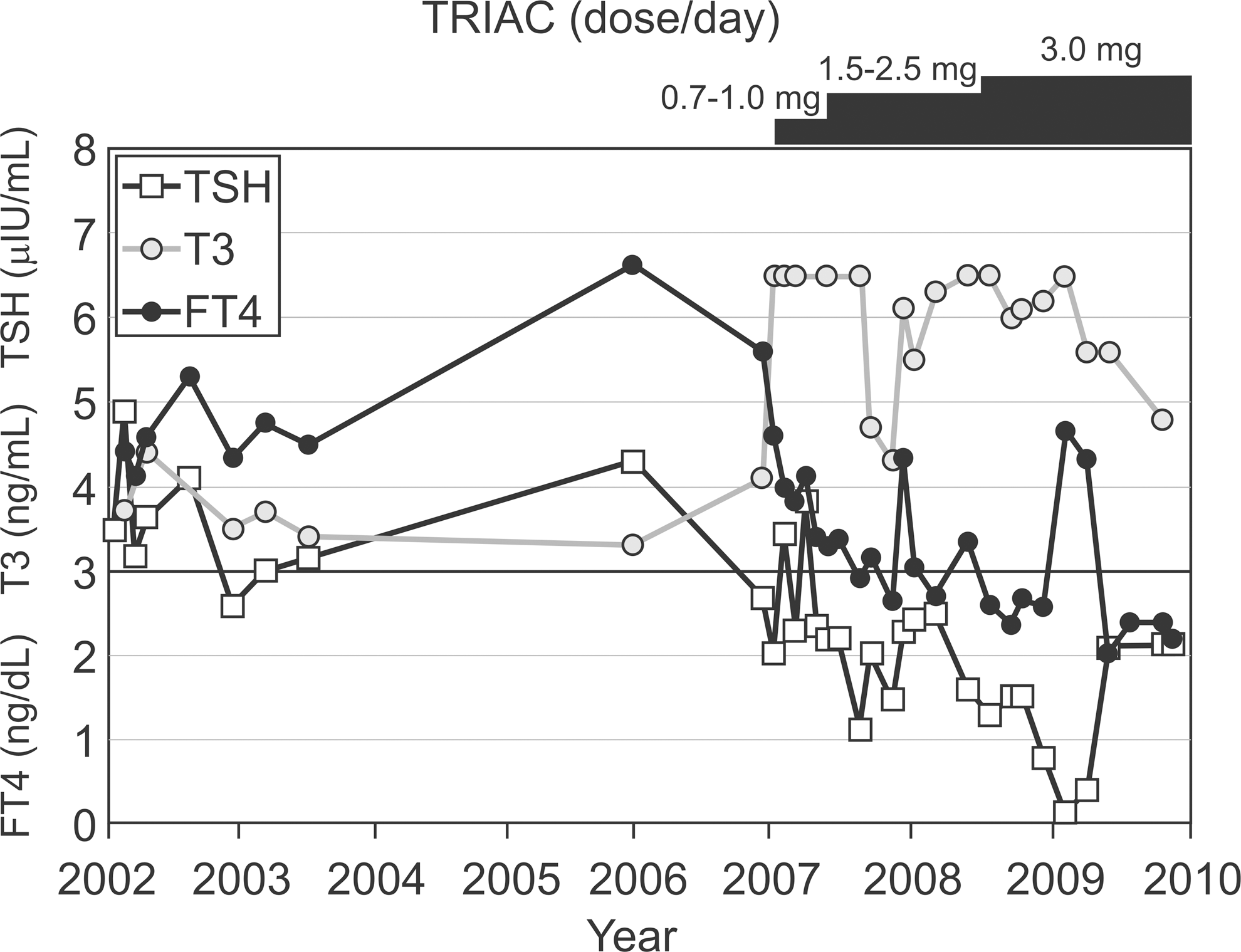
Thyroid function tests conducted on the patient before and during 3 years of TRIAC therapy. TRIAC, 3,5,3′-triiodothyroacetic acid; TSH, thyroid-stimulating hormone; FT4, free thyroxine; T3, triiodothyronine.
ADHD, attention-deficit hyperactivity disorder; SVPC, supraventricular premature contraction.
p<0.05, compared to TRIAC dose of 0.7–1.0 mg/day.
p<0.01, compared to TRIAC dose of 0.7–1.0 mg/day.
TSH, thyroid-stimulating hormone.
Spiked recovery test findings
Figure 2 shows the relationship between the added TRIAC dose and the recovered TRIAC dose inferred by the increment of T3 levels measured by both ECLIA (with ovine polyclonal anti-T3 antibody) and CLIA (murine monoclonal anti-T3 antibodies). The values determined by ECLIA were almost two times higher than those determined by CLIA at all points. However, a close linear relationship with TRIAC concentrations was observed irrespective of the measurement method (ECLIA or CLIA) and the medium (pooled serum or hypothyroid serum). TRIAC crossreactivity was calculated as 79.0% (ECLIA, hypothyroid sera), 61.6% (ECLIA, pooled sera), 37.9% (CLIA, hypothyroid sera), and 32.5% (CLIA, pooled sera). T4 levels, as measured by both ECLIA and CLIA, were not influenced by the TRIAC spike (data not shown).
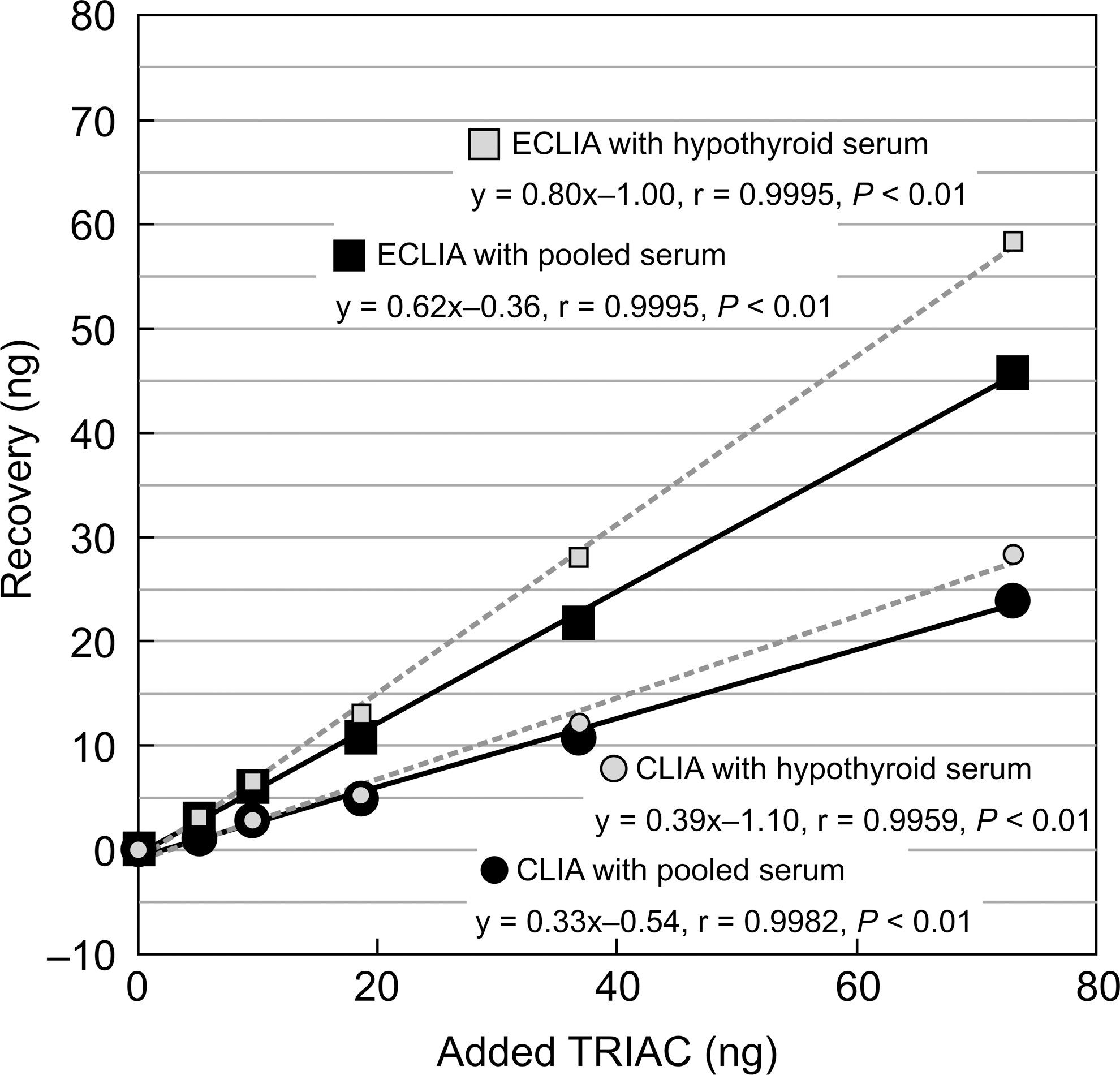
Results of the spiked recovery test for TRIAC. Black symbols with solid lines indicate data obtained using pooled sera as medium. Gray symbols with dashed lines indicate data obtained using hypothyroid sera. CLIA, chemiluminescent immunoassay; ECLIA, electrochemiluminescence immunoassay.
Pharmacokinetic study of single TRIAC dose
Based on the results of the spiked recovery test, changes in the serum TRIAC level after single administration of TRIAC were evaluated in a healthy adult volunteer using ECLIA T3 as a TRIAC surrogate. As depicted in Figure 3, T3 levels after treatment with 1–4 mg TRIAC peaked within 1–2 hours, and then returned to initial levels within 6 hours. In our patient, T3 levels peaked 1 hour after TRIAC ingestion. Serum TSH levels showed a continuous downward trend that lasted for 24 hours after TRIAC treatment in the healthy adult volunteer. In the patient, the TSH level was lowest at 6 hours after TRIAC treatment.
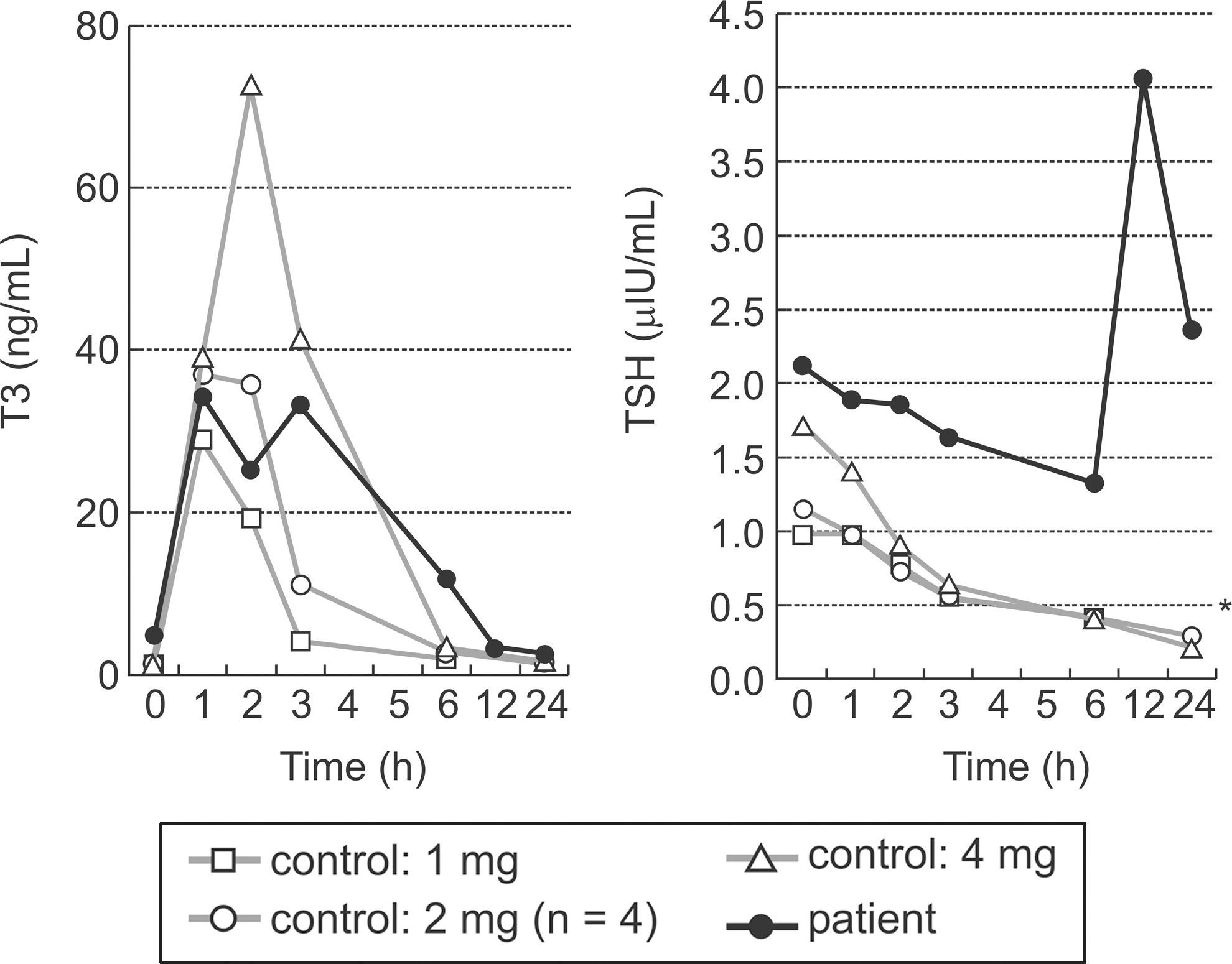
T3 (left panel) and TSH (right panel) changes following a single TRIAC dose in a healthy control and the patient. A healthy adult volunteer ingested 1–4 mg of TRIAC on six separate occasions, whereas the patient ingested 1.5 mg of TRIAC. *TSH at 24 hours (n=5, 1.21±0.43) in the healthy volunteer showed a significant decrease compared to TSH at 0 hour (n=6, 0.27±0.08) (p<0.01).
Discussion
The heterozygous P453T mutation in the gene encoding TR-β has been identified in four GRTH kindred (23 –26) and in one boy who was assumed to have hyperthyroidism (15). Our patient seemed to be in a hyperthyroid state based on his symptoms, which included diaphoresis, tachycardia, and repetitive diarrhea. Presentation of SVPC further supported this assumption, because atrial arrhythmia frequently occurs in hyperthyroid individuals (27). Although some RTH individuals have mixed symptoms of hyperthyroidism and hypothyroidism, our patient did not show any overt signs or biochemical indications of hypothyroidism. His short stature was considered to be due to hypophosphatasia. In addition, his cognitive ability did not seem to be severely impaired. Thus, our patient presented exclusively with the symptoms of hyperthyroidism, which was similar to the previously reported case of a boy with the same P453T mutation (15).
Effectiveness of TRIAC treatment in RTH patients has been investigated on a case-by-case basis with short treatment periods. Results include the alleviation of symptoms of hyperthyroidism in PRTH (15,16,18,19), suppression of TSH and/or T4 levels (10,13
–20), and the normalization of neurological symptoms, including nervousness, inattention, and hyperkinetic behaviors (15,17). TRIAC was shown to reduce the goiter size in non-RTH euthyroid individuals more effectively than
The close association between RTH and ADHD is well known, and the prevalence of ADHD in pediatric RTH has been estimated to be as high as 70%, 10 times higher than that in the general population (29). In such cases, the usual medication prescribed for ADHD in children, methylphenidate, for example, has been shown to be minimally effective. Our patient showed distinct symptoms indicating the presence of ADHD: according to the evaluation of the child psychiatrist, he had hyperactivity, inattention, and impulsiveness, which were inconsistent with his intellectual level. In addition, the presence of autism seemed unlikely. Although the absolute score of 21 in ADHD Rating Scale-IV before therapy was not grossly high, this discrepancy may be derived from the fact that the score was rated by the parents.
TRIAC therapy in our RTH patient resulted in amelioration of ADHD symptoms, as early as 6 months after initiation of treatment, with a decrease in ADHD Rating Scale-IV score (from 21 to 9). This improvement may in part be derived from factors other than TRIAC, including spontaneous improvement or maturity. Nevertheless, the effectiveness of TRIAC in ADHD has been demonstrated previously in pediatric patients, both in GRTH (17) and PRTH (15) cases. The findings in our patient support these previous reports. Although the effect of TRIAC on ADHD can be confirmed only after a placebo-controlled trial, the use of TRIAC to treat RTH children with overt ADHD symptoms seems to be justified at present.
Elevated T3 during TRIAC therapy, which was documented repeatedly (7,10,18,20), has been considered to be due to antibody crossreactivity with serum TRIAC. Through the spiked recovery test, we could demonstrate that the degree of crossreaction differs considerably according to the methods of measuring, probably due to the kind of antibodies used. However, a linear relationship was observed between the TRIAC added to the sample and the apparent T3 increment; this indicates that crossreactivity was constant at various TRIAC levels in each method, and thus T3 levels can be used as a surrogate for serum TRIAC levels. On the other hand, a difference of about 15%–20% in crossreactivity was observed depending on whether the medium was pooled or hypothyroid serum. A clear explanation for this is unknown, but it may indicate that the serum T3 level influences the degree of crossreactivity of TRIAC. Nevertheless, T3 levels were used as a TRIAC surrogate in the pharmacological study, because the study was conducted with constant T3 levels.
In accordance with a classic study on specific radioimmunoassay for TRIAC (30), TRIAC (T3 surrogate) disappeared from circulation rapidly in both normal subjects and patients. On the other hand, TRIAC showed a sustained TSH inhibitory effect, which also supports previous reports (30). However, we observed a substantial difference in this inhibitory effect between the healthy volunteer and our RTH patient: inhibition lasted for at least 24 hours in the former, whereas it lasted for <12 hours in the latter. Ueda and colleagues also described a reduced TSH inhibitory effect of TRIAC in RTH patients (31). Although the rationale for this phenomenon is unknown, TRIAC administered twice a day may be recommended in patients with hyperthyroidism due to RTH. Considering the discrepancy between the circulating TRIAC level and its pharmacological effect, TRIAC serum levels are not a suitable guide in deciding treatment dosage. However, it may be used as an indicator of the patient's compliance.
The long treatment period enabled us to evaluate the relationship between TRIAC dose and thyroid function, and we found that the effect of TRIAC on lowering T4 and FT4 seemed dose dependent. Therefore, in a therapeutic regimen, a stepwise increment of the TRIAC dose, guided by both clinical observations and TSH and (F)T4 levels, may be prudent. Table 4 presents a review of the hitherto-reported TRIAC therapy regimes, which may be helpful in TRIAC dose optimization.
M, male; F, female; PRTH, pituitary thyroid hormone resistance; GRTH, generalized thyroid hormone resistance; ↓, decrease; ↑, increase; PR, pulse rate; TC, total cholesterol; NA, not available
In conclusion, TRIAC therapy for 3 years for a boy with PRTH was safe and effective in ameliorating hyperthyroidism as well as ADHD symptoms. Although TRIAC showed a long TSH inhibitory effect despite its short half-life, TRIAC should be given using a divided dose regimen, considering the shorter drug effect in RTH patients. Because TRIAC seems to work dose dependently, its dose should be adjusted according to the clinical effects and laboratory findings.
Footnotes
Acknowledgments
We thank Prof. Keiichi Ozono (Department of Pediatrics, Osaka University Graduate School of Medicine, Osaka, Japan) and Dr. Toshimi Michigami (Department of Bone and Mineral Research, Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan) for the molecular diagnosis of hypophosphatasia by ALPL gene analysis.
Disclosure Statement
The authors declare that they have no commercial associations that might create an actual or potential conflict of interest in connection with the work described in the article.