
Abstract
Background:
Ectopic thyroid tissue is a relatively rare condition and a developmental anomaly characterized by the aggregation of thyroid tissue. Usually, it occurs along the path of descent of the developing thyroid primordium from the foramen caecum, the most common being in the anterior midline of the neck at or below the level of the hyoid bone. Surgical removal of ectopic thyroid tissue is usually accomplished through an external incision in the neck. However, this procedure inevitably results in a neck scar.
Methods:
We report the case of a 30-year-old woman with ectopic thyroid tissue. We implemented a modified approach to ectopic thyroid tissue removal through a frenotomy incision of the mouth using an endoscope system.
Results:
A modified approach to ectopic thyroid tissue removal was used in this patient. The total operative time was 50 minutes, and the patient remains free of disease 15 months after excision.
Conclusion:
Resection of ectopic thyroid tissue can be performed by a transoral endoscope-assisted approach through a frenotomy incision of the mouth.
Introduction
Surgical excision is the treatment of choice for symptomatic or clinically apparent ectopic thyroid tissue. However, just observing the patient is another treatment choice for asymptomatic or nonclinically apparent ectopic thyroid tissue, unless the ectopic thyroid tissue is confirmed as a carcinoma.
Considering that many patients who undergo surgical resection are women, it is desirable to develop a surgery for the removal of ectopic thyroid tissue that avoids external scarring of the neck. Thanks to advancements in medical technology, we were able to develop a modified endoscope-assisted approach through a frenotomy incision of the mouth (4). This method reduced the risk of damage to the mouth floor structure, since we used anatomical dehiscence through the frenotomy incision.
Additionally, this was an endoscopic surgical procedure through a natural opening in the human body, otherwise known as natural orifice transluminal endoscopic surgery (NOTES). We developed this technique taking into consideration that it could also be applied to transoral thyroid and parathyroid surgery. In this report, we describe this new technique in detail, as well as the surgical outcome.
Patient and Methods
A 30-year-old female patient was admitted for the chief complaint of a mass at the anterior part of the neck, detected six months before her visit. The size since the initial detection had gradually increased, and she found swallowing uncomfortable due to the sensation of a lump in her throat. During palpation, a painless, movable, soft mass 1.5 cm in diameter was located between the hyoid bone and thyroid gland. The mass moved upon tongue protrusion and swallowing. Laryngoscope examination revealed no protruding mass at the base of the tongue. The medical history of the patient was unremarkable, and she had no history of thyroid disease.
Computed tomography (CT) imaging of the neck documented that the thyroid was in the normal location. With contrast enhancement, there was a solid mass below the hyoid bone, approximately 1.5 cm×1.5 cm in size (Fig. 1). Aspiration cytology and CT scans suggested a thyroid nodule in the thyroid gland of the pyramidal lobe. The thyroid function tests were normal. The patient was a young woman, and she did not want a surgical scar remaining in the neck area. Therefore, the surgery was performed by a transoral approach using an endoscope.
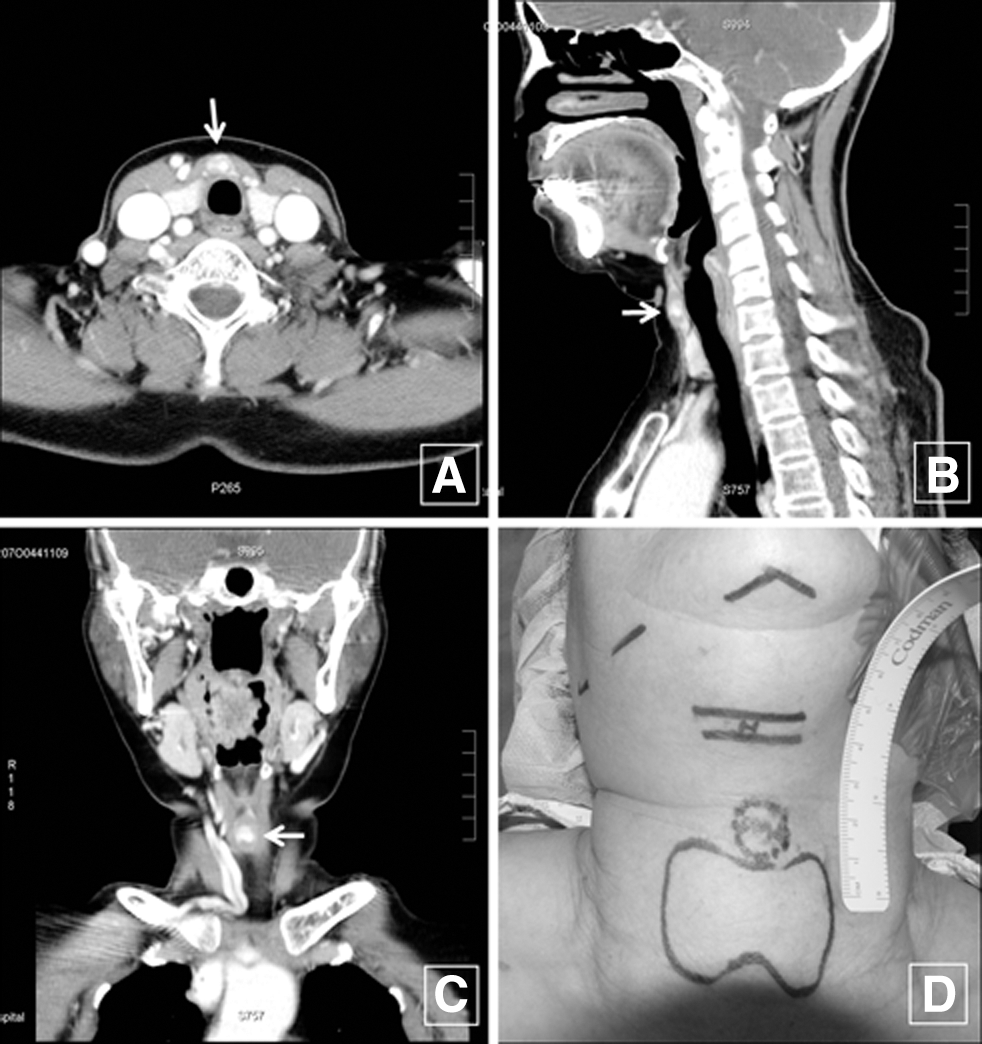
Computed tomography (CT) scan confirmed a 1.5 cm mass (arrow) that was found between the hyoid bone and the thyroid inferior to the level of the hyoid bone.
With the patient under general anesthesia, the mouth was opened, and the tongue was tracted to the upper position. An incision of ∼2 cm was made in the oral mucosa including the frenulum (Fig. 2A). After careful dissection of the soft tissue in the floor of the mouth, we found the genioglossus muscles (Fig. 2B), separated them in the midline, and retracted them bilaterally (Fig. 2C). With the aid of an endoscope (rigid, 10 mm, 0°; Olympus, Tokyo, Japan), after retraction of the genioglossus muscles, we found the hyoid bone and the strap muscles (Fig. 2D). We transected the strap muscles with ultrasonic scissors (Harmonic scalpel 300, Ethicon Johnson & Johnson Co., Cincinnati, OH) ∼0.5 cm away from the hyoid bone. We then cut the body of the hyoid bone out with an Osteo Punch Rongeur (1 mm, 40°; Koros USA, Inc., Moorpark, CA) ∼0.5 cm (Fig. 2E and F). The remnant hyoid bone was retracted bilaterally, and then we went downward and were able to identify a dark solid mass at the anterolateral side of the thyroid cartilage (Fig. 2G). The mass was easily dissected from the adjacent tissue (Fig. 2H), and the remnant hyoid bone did not restrict this procedure (Fig. 2I). After removal of the mass, the strap muscles and thyroid cartilage were present below (Fig. 2J). The operation field was irrigated, a drain was inserted through the floor of the mouth, and it was sutured to the edge of the opened mucosa. Afterward, the genioglossus muscles were sutured with 4-0 Vicryl, and the opened oral mucosa was sutured. The total operation time was ∼50 min. The drain was removed on postoperative day 2. We encouraged frequent oral gargling with 0.02% chlorhexidine and allowed a normal diet on postoperative day 3. The patient was discharged home on postoperative day 5. Fifty months after the operation, there had been no special findings on the patient, including thyroid function and articulation. She is currently under follow-up observation at our outpatient clinic. The patient was quite satisfied with the surgical outcome. The mass was confirmed as an ectopic thyroid nodule by pathological examination.
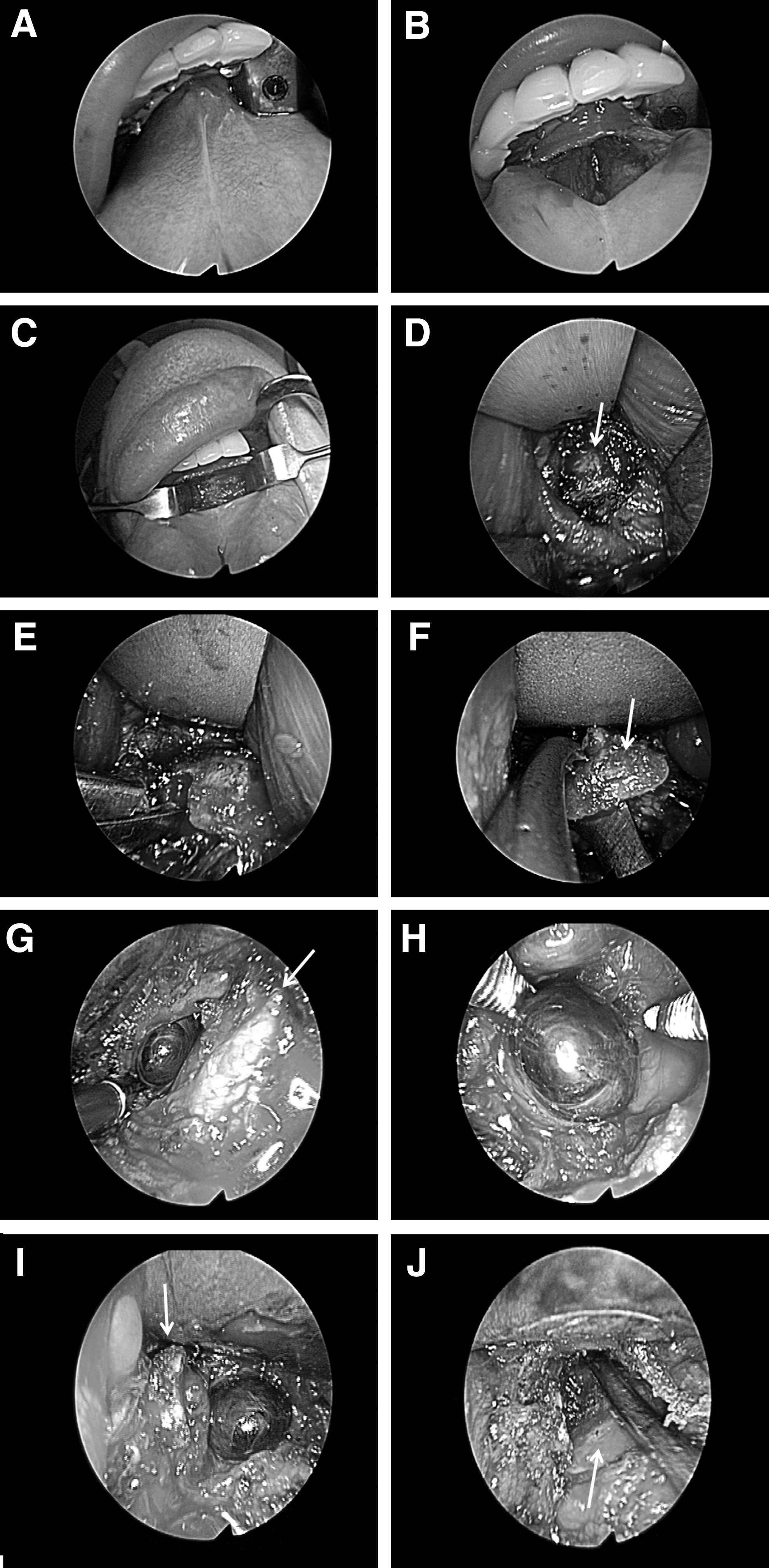
Transoral approach through a frenotomy incision of the mouth.
Discussion
Ectopic thyroid tissue is defined as thyroid tissue that is not located anterolaterally to the second through fourth tracheal cartilages (1). It may be found anywhere along its embryological path of descent. The thyroid primordium originates from the posterior floor of the embryonic pharynx during the fourth week of embryonic development. Eventually, the gland anlage descends through the tongue into the neck, passing anteriorly to the hyoid bone and thyroid cartilage to reach its final position anterolateral to the superior part of the trachea in the seventh week of embryonic development. During its migration, the thyroid gland is attached to the foramen caecum by a narrow tube called the thyroglossal duct. This duct is normally obliterated, and it eventually disappears.
The treatment for ectopic thyroid depends on the location, size, and presence of symptoms or complications (5,6). Therefore, an accurate diagnosis greatly reduces posttreatment complications.
In the neck, an ectopic thyroid is primarily a cosmetic issue while secondary ulceration, hemorrhage, and malignant degeneration are the major complications (7). The treatment for an isolated ectopic thyroid occurring in the midline of the neck along the route of descent of the thyroglossal anlage is surgical excision. However, this operation requires a transcervical approach, which results in external scarring of the neck (4,8). Therefore, many surgeons wish to achieve scar-free surgery using the oral cavity. However, there is a major obstacle in the pathway from the mouth to the thyroid—the hyoid bone. In contrast to the external surgical removal of an infrahyoid neck mass, transoral removal must pass through the hyoid bone.
Generally, thyroglossal duct cyst (TGDC) surgery should include the removal of the TGDC and hyoid bone (4,8 –15). This means the middle part of the hyoid bone must be removed. Therefore, we cut the hyoid bone and approached the ectopic thyroid tissue below the hyoid bone. Previously, the authors published a paper on cutting the hyoid bone and excising the TGDC through the oral cavity (4,8).
The authors reported in that paper about the safe excision of a dermoid cyst and TGDC by cutting the hyoid bone using a frenotomy incision. It showed that a transoral hyoid bone excision was technically feasible with the advancements in the endoscope system (4,8,15).
This surgical approach passed through the midline incision in the floor of the mouth and used the natural midline dehiscence present between the genioglossus muscles (4,15). This area has been shown to be a relatively avascular dissection plane. When the space between the genioglossus muscle was spread out using a tractor, the mylohyoid muscle was reached. When we traced the posterior line of the mylohyoid muscle, the hyoid bone was reached.
When we reached the hyoid bone, we dissected the suprahyoid muscles attached to the middle portion of the hyoid bone (0.5 cm in width). We used ultrasonic scissors to remove a cuff of tissue in the middle portion of the hyoid bone. This method was concordant with the Sistrunk operation (14,15,17 –19). We then cut the hyoid bone and resected the ectopic thyroid tissue placed below the hyoid bone. The patient was quite satisfied with the surgical outcome.
The transoral approach is straightforward. Moreover, it has the advantages of minimizing the access trauma and allowing for improved preservation of the adjacent structures (4). Thanks to the development of the endoscope and other medical instrument technologies, the ectopic thyroid tissue located inferior to the hyoid bone can be removed with the intraoral approach without any complications.
This method is not only technically possible, but it could also provide an appropriate surgical field. Thus, it is believed that this method could be used for patients with ectopic thyroid tissue manifested as a central midline neck mass. The satisfaction level of our patient after the operation was good, and significant swelling or bleeding was not observed. Since neck exploration is associated with the risk of turning an aseptic operation into a potentially infectious surgical procedure by spreading the oral flora, postsurgical infection has to be managed carefully. Therefore, we used antibiotics and an oral gargle, and the drain was removed two days after the operation.
Follow-up observation was carried out for 15 months postoperatively, and there were no noteworthy recurrences or complications observed. However, we need to secure long-term stability through continuous reporting of cases.
This report suggests a new surgical method to approach an anterior neck mass through the floor of the mouth. Therefore, ectopic thyroid tissue can be resected through an intraoral approach.
Footnotes
Author Disclosure Statement
No financial or material support has been received for this work. Moreover, the authors declare no financial interests in companies or other entities that could have an interest in the information within this contribution. None of the authors have any conflict of interest, financial or otherwise.