
Abstract
Background:
The strong predilection for thyrotoxic periodic paralysis (TPP) to occur in males suggests androgen may contribute to its pathogenesis. We therefore sought to determine if serum total and free testosterone (TT and FT) concentrations differed among patients with TPP during episodes of paralysis, patients with TPP between episodes of paralysis, and patients with Graves' disease (GD) not having TPP.
Methods:
A total of 105 Chinese men were included in the study, and were divided into three groups. Group 1 consisted of men with TPP who were studied during episodes of paralysis; group 2 consisted of men with TPP who were studied between episodes of paralysis; group 3 consisted of men with GD not having TPP. Patients in each were different persons. Serum electrolytes, free triiodothyronine (FT3), free thyroxine (FT4), TT, and FT were measured. Multiple regression analyses and analysis of covariance were performed to analyze the relationship of serum parameters, group status, and age.
Results:
One multiple regression analysis was used to determine if serum TT concentrations were associated with age, FT3, FT4, or group status. This analysis indicated that age, FT4 level, and group status were significantly and independently associated with serum TT concentrations. With regard to group status, patients in group 1 had serum TT concentrations 0.92 ng/mL higher than patients in group 3 (p=0.033). As to FT4 level, TT concentrations increased by 0.016 ng/mL for each additional pmol/L of FT4 (p=0.002). Another multiple regression analysis was used to determine if serum FT concentrations were associated with age, FT3, FT4, group status, or serum TT concentrations. This analysis revealed that serum TT concentrations and group status were significantly and independently associated with serum FT concentrations. In terms of group status, patients in group 1 had serum FT concentrations of 2.11 pg/mL greater on average than patients in group 3 (p=0.006).
Conclusions:
We infer that episodes of paralysis in Chinese men with TPP are associated with elevated serum testosterone. We also found serum TT and FT concentrations of men with GD are both affected by group status; serum TT rather than FT concentrations are associated with thyroid function.
Introduction
As early as 1966, potassium transportation to the intracellular compartment was shown to be the cause of hypokalemia in TPP (10,11). Na+, K+-ATPase, as an important enzyme for intracellular potassium influx, has been found to be centrally involved in TPP, and increases in enzyme mass and activity implicated in the process (12,13). In TPP, this is induced by an excess of thyroid hormones (14 –17) and/or β-adrenergic stimulation (18 –20). Some studies have reported that Na+, K+-ATPase activity may also be increased by androgens (21 –23). It has also been speculated that estradiol and testosterone are involved in protecting against and facilitating episodes of paralysis in patients with TPP, respectively (8). This may possibly occur through alteration of gene expression for Kv4.3 potassium channels (24).
Since almost all patients with TPP are male, who obviously have higher levels of androgens than females, it is reasonable to consider the hypothesis that the sex difference in the prevalence and incidence of TPP is due to sex differences in androgen levels. However, only a small fraction of Asian or other men with thyrotoxicosis develop TPP. Therefore, we hypothesized that the relatively high androgen levels in those patients contribute to the occurrence of TPP.
As far as we know, to date there are only two studies of total testosterone (TT) concentrations in patients with TPP: one published in English (25), and the other one published in Chinese (26). In both studies, serum TT concentrations were higher in patients with TPP than in patients with Graves' disease (GD) not having TPP. However, in Wang's study, patients were not studied during episodes of paralysis (25), and in Tian's study, although patients were studied during episodes of paralysis, no information about the age difference between patients with TPP and patients with GD not having TPP was provided. Furthermore, although free triiodothyronine (FT3) levels of the two groups were found to be significantly different, this was not taken into consideration when analyzing the difference in TT concentrations between the two groups (26). Neither of the two research studies measured free testosterone (FT) concentrations. In the present study, both serum TT and FT concentrations were examined in Chinese men with TPP during episodes of paralysis, in Chinese men with TPP between episodes of paralysis, and in Chinese men with GD not having TPP.
Materials and Methods
Subjects
A total of 105 Chinese men with GD at the West China Hospital of Sichuan University, both outpatients and inpatients, were recruited for the study. GD was diagnosed by its clinical symptoms and signs, ophthalmopathy or palpation of a symmetrically and diffusely enlarged thyroid, and laboratory tests showing a decreased thyrotropin (TSH) level with elevated free thyroxine (FT4) and FT3 levels. All patients were questioned specifically on the occurrence of periodic paralysis. Periodic paralysis was diagnosed if: (i) they had acute onset of weakness in their extremities that was severe enough to prevent unassisted walking or standing, or rising from a lying or sitting position, which fully resolved over hours to days; or (ii) they came to the hospital during the acute onset of weakness in their extremities that was severe enough to prevent unassisted walking or standing, or rising from a lying or sitting position, and were found to be hypokalemic with other diseases involving hypokalemia excluded. Special care was taken to exclude the following diseases: (i) family periodic paralysis, which is characterized by a family history; (ii) thyrotoxic myopathy, which is a long-standing weakness of muscles in hyperthyroid patients; (iii) other diseases involving hypokalemia, such as renal tubular acidosis and hyperaldosteronism. This study was approved by the Ethics Committee of West China Hospital, and written informed consent was obtained from each patient.
Subjects were divided into three groups: patients with TPP who were studied during episodes of paralysis (group 1; n=24); patients with TPP who were studied between episodes of paralysis (group 2; n=33); and patients with GD without a history of TPP (group 3; n=48). Tests for anti–thyroid peroxidase or antithyroglobulin antibodies were not a mandatory requirement for inclusion but were obtained in 65% of the subjects (20 of 24 patients in group 1, 22 of 33 patients in group 2, and 27 of 48 patients in group 3). Patients in group 1 were all inpatients at the time they were studied; group 2 included both inpatients and outpatients, and none of them had had an episode of paralysis within at least one month prior to the evaluation; group 3 included both inpatients and outpatients. Patients in each group were different persons. All patients in group 1 were thyrotoxic when evaluated, while some patients in groups 2 and 3 were euthyroid, even hypothyroid (14 euthyroid and 2 hypothyroid in group 2, 19 euthyroid and 7 hypothyroid in group 3) due to the medication or other treatment for GD, and were required to provide their initial reports of thyroid function for diagnosis of GD.
Samples and data collection
Blood samples were drawn once in each group at enrollment—that is, during episodes of paralysis in group 1, during intervals between episodes of paralysis in group 2, and on any random day in group 3. FT3, FT4, TSH, TT, FT, and electrolyte values were tested in all blood samples. Furthermore, for group 1, their last electrolyte values before they left hospital were tracked and recorded, as were their electrolyte reports during intervals between episodes of paralysis; for group 2, we recorded their initial reports of thyroid function (FT3, FT4 and TSH) for diagnosis of GD, and they were also required to supply the electrolyte reports during their episodes of paralysis they had experienced before, if they had any (24 out of 33 patients in group 2 had records showing that they had hypokalemia during their episodes of paralysis); for group 3, their initial reports of thyroid function for diagnosis of GD were also recorded. See Figure 1 for the details of the flow of data collection.
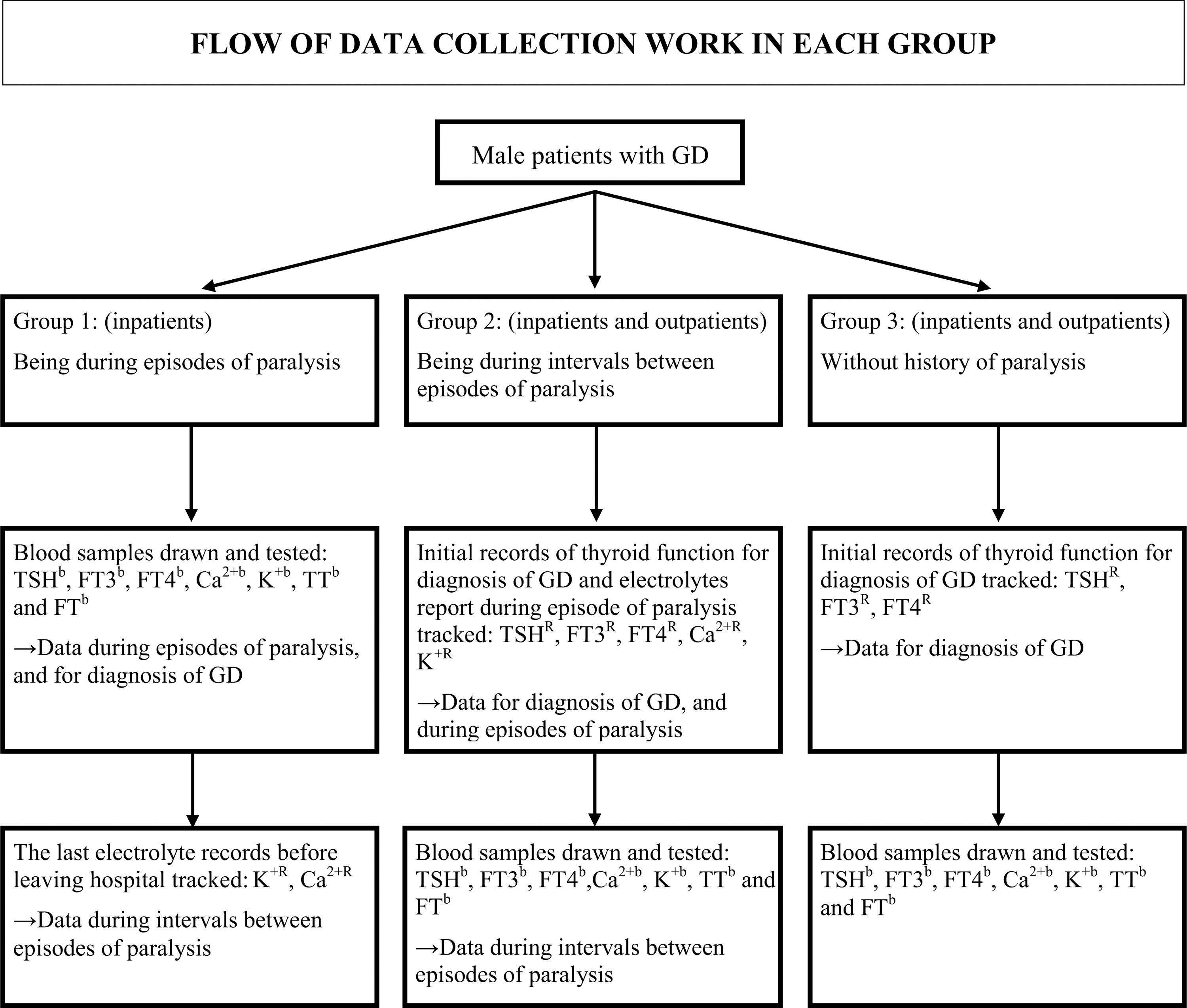
Flow of data collection work in each group. bData obtained by testing the blood samples; Rdata obtained by tracking records.
Test methods
FT3, FT4, and TSH were determined by electro-chemiluminescence immunoassay (ECLIA Elecsys and Cobas e immunoassay analyzer; Roche). TT was measured using a Testosterone Radioimmunoassay Kit (Beijing North Institute of Biological Technology). FT was tested with a DSL-4900 ACTIVE® Free Testosterone Coated-Tube Radioimmunoassay (RIA) Kit (Diagnostic Systems Laboratories, Inc.). Blood electrolytes were tested by ion selective electrode method (Roche/Hitachi 900 analyzer; Roche).
All thyroid function reports and blood electrolyte reports, including those offered by patients or tracked by us or tested at enrollment, were from the same laboratory at the West China Hospital using the same testing system and kits.
Statistical analysis
Clinical features were compared using one-way analysis of variance (ANOVA; for three groups) or independent samples t test (for two groups). The correlations between TT and FT concentrations and relevant clinical features (age, FT3 level, FT4 level, potassium during episodes of paralysis and between episodes of paralysis, and calcium during episodes of paralysis and between episodes of paralysis) in our study were assessed using Pearson correlation analysis. Analysis of covariance (ANCOVA) was used to assess the difference in serum TT and FT concentrations among three groups, with age, FT4 level, and FT3 level included as covariates for the analysis of serum TT concentrations, and age, FT4 level, FT3 level, and serum TT concentrations included as covariates for the analysis of serum FT concentrations respectively. Multiple regression analyses were used to predict serum testosterone concentrations (TT and FT) on the basis of age, FT3 level, FT4 level, and group status. Serum TT or FT concentration was a dependent variable. Age, FT3 level, FT4 level, and group status were independent variables. Serum TT concentration also was an independent variable to predict FT concentration. Since the group status is a categorical variable, dummy variables were used in the regression analyses: whether TPP patients were studied during episodes of paralysis (group 1=1, otherwise=0) or whether TPP patients were studied between episodes of paralysis (group 2=1, otherwise=0). Group 3 was a basic group. Analyses were performed using SPSS version 13.0 statistical software. A two-tailed α level of 0.05 was the cutoff used to indicate statistical significance.
Results
The clinical features of patients in the three groups (mean±SD) are shown in Table 1. Serum TT concentrations, serum FT concentrations, age, FT3 level, and FT4 level when the samples were collected were all significantly different among the three groups. Patients in group 1 and group 2 were significantly younger than those in group 3 (p<0.001). Thyroid function tests (both FT3 and FT4) and testosterone levels (both TT and FT) were significantly higher in group 1, who were studied during episodes of paralysis, than in group 2, who were studied during intervals between episodes of paralysis, or in group 3 (p<0.001). There were no significant differences between group 2 and group 3 in these parameters. No significant differences in blood potassium levels were detected either during episodes of paralysis between group 1 and group 2, or during intervals between episodes of paralysis among the three groups. Since the calcium channel gene CACNA1S is reported to be involved in TPP, we also compared blood calcium levels among the three groups, but observed no significant differences (27).
Blood samples for groups 1 and 2 were drawn during episodes of paralysis and during intervals between episodes of paralysis, respectively.
p<0.01, ** p≤0.001 vs. group 2; † p≤0.001 vs. group 3.
Data were obtained aby tracking records or patients providing records, or bby testing the blood samples.
TT, total testosterone; FT, free testosterone.
A significant negative correlation between age and serum TT concentrations (r=−0.417; p<0.01), serum FT concentrations (r=−0.413; p<0.01) was found. There was also a positive correlation between FT3 level and serum TT concentrations (r=0.395; p<0.01), serum FT concentrations (r=0.415; p<0.01), and between FT4 level and serum TT concentrations (r=0.445; p<0.01), serum FT concentrations (r=0.479; p<0.01) respectively. No significant correlation was found between serum TT concentrations, serum FT concentrations, and the other clinical parameters.
The serum FT and TT concentrations (mean±SE) after accounting for age, FT3 level, and FT4 level (plus serum TT concentrations when analyzing serum FT concentrations) are provided in Figure 2. Serum FT concentrations were significantly different between the three groups (p=0.023). The serum FT concentrations in group 1 (20.50±0.64 pg/mL) were significantly higher than in group 2 (18.37±0.49 pg/mL; p=0.009) and group 3 (18.53±0.43 pg/mL; p=0.018). Although a similar tendency was observed in serum TT concentrations, which were 0.92 ng/mL higher in group 1 than in group 2 and group 3 respectively, no significant difference in serum TT concentration was observed between the three groups (p=0.062).
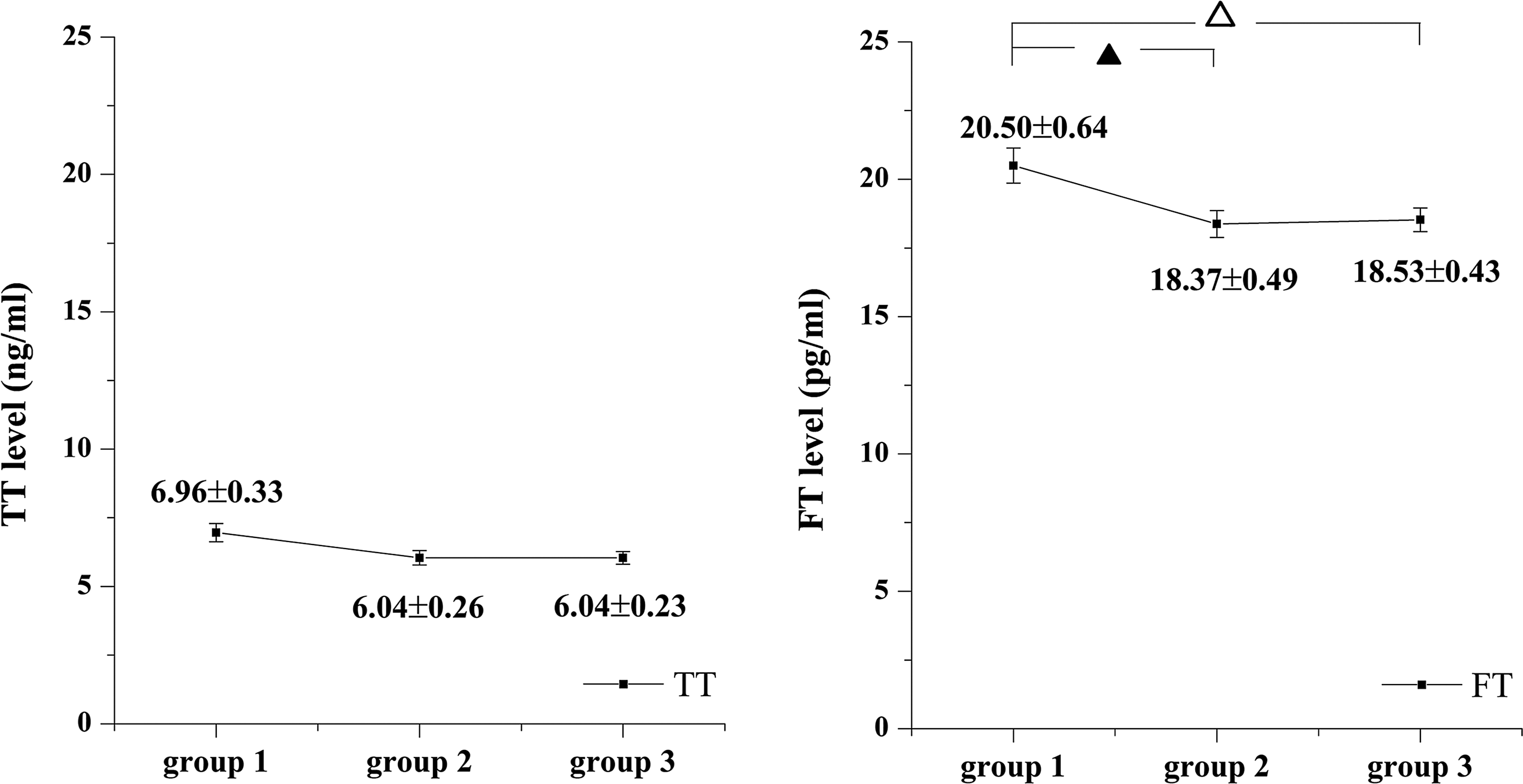
Comparisons of serum total and free testosterone (TT and FT) concentrations (mean±SE) among three groups, adjusted for age, free triiodothyronine, and free thyroxine levels (plus serum TT concentrations when analyzing serum FT concentrations). ▴ p=0.009 vs. group 2; ▵ p=0.018 vs. group 3.
Two multiple regression analyses were performed. One was used to determine if serum TT concentrations were associated with age, FT3 level, FT4 level, or group status (Table 2). In this multiple regression analysis, serum TT concentration was the dependent variable; age, FT3 level, FT4 level, and group status were the independent variables. This multiple regression analysis indicated that age, FT4 level, and group status were significantly and independently associated with serum TT concentration. With regard to group status, serum TT concentrations were different between groups 1 and 3. The mean serum TT concentration in group 1 was 0.92 ng/mL higher than that in group 3 (p=0.033). With respect to FT4 levels, for each additional pmol/L of FT4, there was a 0.016 ng/mL increase in serum TT concentrations (p=0.002). Another multiple regression analysis was used to determine if serum FT concentrations were associated with age, FT3 level, FT4 level, group status, or serum TT concentrations. In this multiple regression analysis, serum FT concentration was the dependent variable; age, FT3 level, FT4 level, serum TT concentration, and group status were the independent variables. This analysis revealed that serum TT concentrations and group status were significantly and independently related to serum FT concentrations (Table 2). In terms of group status, serum FT concentrations were different between groups 1 and 3. The mean serum FT concentration in group 1 was 2.11 pg/mL higher than in group 3 (p=0.006). The FT4 level, however, was not shown to be independently associated with serum FT concentrations.
Adjusted R 2=0.303.
Adjusted R 2=0.756.
B, unstandardized coefficients; SE, standard error for unstandardized coefficients; CI, 95% confidence interval; β, standardized coefficients.
Discussion
We asked whether the testosterone level differs (and how it differs) between patients with TPP during episodes of paralysis, patients with TPP between episodes of paralysis, and patients with GD not having TPP to test the pathogenic androgen hypothesis. A total of 105 patients were included and categorized into three groups. As shown in Table 1, a younger age during an episode and uncontrolled thyroid function of group 1 are characteristics of TPP: it frequently occurs in the third and fourth decades and is typically associated with uncontrolled thyrotoxicosis as a prerequisite for its occurrence and recurrence. It is the difference in age and FT3 and FT4 levels among the three groups that necessitates the consideration of the factors influencing testosterone levels when analyzing the difference in testosterone concentrations.
Many factors could affect testosterone concentrations in males. Age has been shown to be one factor (28). Furthermore, thyroid function status is revealed to affect gonadal steroids, including estrogens and androgens in males. There are studies showing that thyrotoxic males have a higher serum or plasma TT and estradiol-17β (E2) level than normal males (29,30). In patients with hyperthyroidism, the pretreatment concentrations of serum or plasma TT and E2 are significantly higher than those found posttreatment, while the opposite occurs in hypothyroid men, suggesting that the normalization of thyroid function would simultaneously normalize TT and E2 levels in both hyperthyroidism and hypothyroidism (30 –32). In males with hyperthyroidism, the correlation between TT concentrations and thyroid function, including triiodothyronine (T3) and thyroxine (T4) level, or the change of TT concentrations and the change of FT3 and FT4 levels, has been observed, while a correlation between E2 concentrations and T3 or T4 level was not observed (30,32). When it comes to FT levels, the results of studies vary. In some studies, no significant difference was found between the serum FT concentrations of patients with GD and those of normal males, or between the pretreatment concentrations and posttreatment concentrations of FT in patients with hyperthyroidism (29,32). However, in other studies, pretreatment concentrations of FT in patients with hyperthyroidism were lower than posttreatment concentrations, while in patients with hypothyroidism, the opposite occurred (31). Unbound E2 was reported to be higher in thyrotoxic males than normal males, especially in those with gynecomastia (29,33).
The results of ANCOVA and multiple regression analyses showed that TT and FT concentrations were elevated in patients in group 1, independent of age and thyroid functional status. This finding is interesting because we expected similar testosterone levels in patients who develop TPP, including patients in group 1 during episodes of paralysis and patients in group 2 during intervals between episodes of paralysis, whereas only those in group 1 exhibited a significantly higher level of TT and FT. We infer that episodes of paralysis in Chinese men with TPP are associated with elevated testosterone levels, including TT and FT. Assuming that groups 1 and 2 represent patients with TPP in different phases, we also speculate that the higher testosterone levels in group 1 may possibly indicate a process of testosterone fluctuation, rising from and falling back to a common level in male patients with GD, and this fluctuation may possibly be involved in the pathophysiologic process of episodes of paralysis. However, the time span of the fluctuation process could not be determined, given our study design.
In normal men, 2% testosterone is free, 44% is bound to sex hormone binding globulin (SHBG), and 54% is bound to albumin and other proteins (34). It is well known that, in hyperthyroid patients, the TT concentrations increase, non-SHBG-binding testosterone concentrations decrease, and FT concentrations decrease or remain normal. These changes are thought to be caused by an increase of SHBG. SHBG, which is positively correlated with thyroid functional status, increases in hyperthyroidism. This leads to an increase in SHBG-bound testosterone and a decrease in non-SHBG-bound testosterone, and results in a decrease in the metabolic clearance rate of testosterone and thereafter increased TT concentrations (29,31,32,35,36).
In our study, however, the increase in TT concentrations in group 1 during episodes of paralysis is independent of FT3 levels, FT4 levels, and age, and therefore cannot be explained by the foregoing mechanism. To discover the underlying mechanism, future studies should focus on the following three candidates during episodes of paralysis: increased production rate of testosterone, decreased metabolic clearance rate of testosterone, and increased conversion rate of other hormones to testosterone, especially the extra portion that is not explained by FT3 levels, FT4 levels, and age.
To our knowledge, this study is the first to demonstrate higher serum FT concentrations in patients with TPP during episodes of paralysis. This is interesting, since the higher serum FT concentrations we observed in patients during episodes of paralysis are independent of FT3 levels, FT4 levels, serum TT concentrations, and age. It may involve a direct increase of FT resulting from either an increase of production or a decrease in the metabolic clearance rate, with or without an indirect increase in FT caused by testosterone's shift from a protein-bound form to a free (active) form.
Li et al. (25) also observed higher TT concentrations in patients with TPP compared to patients with GD not having TPP. However, details in that report were inadequate—it is unknown whether the patients with TPP were in episodes of paralysis or not when the blood samples were drawn for testosterone concentration tests. After contacting them for details about their group division, we were informed that the group division was based on history of TPP and the blood samples were drawn when hypokalemia totally resolved (one week or more after paralytic attacks). It seems that patients with TPP in their study represent those during intervals between episodes of paralysis, so their result is different from ours in terms of whether TT concentrations of patients with TPP between episodes of paralysis are significantly higher than that of patients with GD not having TPP. However, considering that high testosterone concentrations need time to fall back to baseline levels after episodes of paralysis, it is possible that some of the patients with TPP in the study by Li et al. after episodes of paralysis may still be in a state of declining testosterone concentrations (25), which could explain the discrepancy in results.
Few studies have ever examined the factors influencing testosterone concentrations of men with hyperthyroidism within one model, while our study included age, FT3 levels, FT4 levels, as well as group status into one analysis model, and explored what their respective and independent effects on serum testosterone concentrations were when pooling them together. The relationship between thyroid function and testosterone concentrations in men with GD revealed by our regression analyses was in accordance with previous findings of higher TT levels and normal FT levels in men with hyperthyroidism but lower TT levels in men with hypothyroidism, in that the TT level is affected by thyroid function while the FT level is not. We observed a linear relationship between FT4 and TT levels when FT4 ranges from 0.005 pmol/L to 99.22 pmol/L. However, seven patients in group 1, five patients in group 2, and four patients in group 3 had thyrotoxicosis too severe to obtain accurate FT4 values, with values above the upper limit of reference (100 pmol/L). From their data, it is suggested that when FT4 increases in a range higher than 100 pmol/L, the increase of TT level does not follow the linear relationship we observed in this study.
There is a deficiency in our study in that we did not adopt the gold standard method (tandem mass spectrometry method and the equilibrium dialysis assay) for TT and FT assays. The radioimmunoassay we used for measuring TT concentrations was reported to have limited accuracy, especially when the testosterone level is low, indicating the unacceptable reliability of this method for measuring TT concentrations in women and children (37). Since the TT level of hyperthyroid male adult patients is known to be higher than that of normal or euthyroid male adults (29 –31), the accuracy of the radioimmunoassay used for TT measurement in our study should not be compromised severely. Furthermore, the study design was to compare the TT and FT concentrations between three groups by applying the same assay method to each group. If any systematic bias exists in either of the assay methods, the bias would not influence the results of comparisons. For the FT assay, the accuracy and specificity of the analog-based method has been a concern, and an analog-based kit for FT was reported to actually test TT levels rather than FT levels (38,39). However, it is important that the difference of serum FT concentrations between three groups in our study is shown after adjustment for serum TT concentrations in both ANCOVA and multiple regression analysis.
Considering that group 1 and group 2 represent patients with TPP in different phases, we could not exclude the possibility that the higher level of testosterone in those during episodes of paralysis may suggest a process of its fluctuation in the same patient, and it is based on this rationale that we make our hypothesis of the possible fluctuation of testosterone levels in those male patients with GD who developed TPP. But it should be noted that group 1 having higher serum testosterone concentrations than group 2 does not definitely prove to be the result of a process of testosterone rising in the same TPP patient, since groups 1 and 2 are two distinct groups without any subject simultaneously included in both groups. Hence, this uncertainty could weaken our inference. It is one of the limitations of our study design, which can be perfected in the future by having the same patients' serum testosterone concentrations tested before, during, and after episodes of paralysis. It should also be noted that if testosterone concentrations were tested only once in each phase—i.e., respectively before, during, and after episodes of paralysis—the data would not be adequate to confirm the fluctuation of testosterone concentrations and its role in the pathophysiological process either, since the time span of intervals between episodes of paralysis in patients with TPP varies from hours to months and the onset of TPP is unpredictable, which makes it hard to ensure that the selected monitoring time points are around the episodes of paralysis. Whether the elevation of testosterone levels triggers or induces the episodes of paralysis should be examined by regularly recording the testosterone concentrations in men with GD until several episodes of paralysis are covered.
In our study, ANCOVA failed to show an increase in serum TT concentrations attributable to group status (p=0.062), while the trend is shown by multiple regression analysis. The relatively small sample size, which is a limitation of the present study, may be the reason for this.
Our study addresses the question of whether testosterone level differs among three groups of patients and how it differs, and the question of which among those candidate factors are independently associated with testosterone levels in men with GD. To be more convincing, future research should adopt the gold standard methods for the testosterone assay and amplify the sample size. It should be noted that our study design did not enable us to determine whether fluctuation of testosterone levels around episodes of paralysis exists, what the time span is for the fluctuation, or whether the elevation of testosterone levels triggers paralysis attacks. These issues need to be resolved by modifying the study design, as discussed above. Notwithstanding its limitations, our study does suggest that episodes of paralysis in Chinese men with TPP are associated with higher serum testosterone concentrations (including TT and FT), and this may offer some insight into the underlying mechanism.
Footnotes
Author Disclosure Statement
No competing financial interests exist.