
Abstract
Background:
Current management guidelines suggest that 6–12 months after total thyroidectomy and radioactive iodine remnant ablation (RAI-RA), patients with differentiated thyroid cancer should be re-evaluated with serum thyroglobulin (Tg) and neck ultrasonography to assess the efficacy of initial treatment and to guide subsequent management. However, if serum Tg levels can continue to decline for many years after RAI-RA, then an early assessment of response to therapy could lead to excessive evaluations and treatments in patients with low-level Tg values that are likely to resolve over time without additional therapies.
Methods:
Serum Tg concentrations in patients with differentiated thyroid cancer, who had been thyroidectomized (Tx), received RAI-RA, and who were receiving levothyroxine to suppress serum thyrotropin (suppressed serum Tg), were retrospectively analyzed. The study included 299 patients, 69% of whom were women with an overall median age of 46 years and who had a median follow-up of 7 years. The study was limited to patients who received no additional treatments beyond total Tx, RAI-RA, and levothyroxine therapy to suppress thyrotropin. The primary endpoints were the time required to achieve the lowest Tg (nadir Tg) and the time required to achieve a suppressed serum Tg<1 ng/mL.
Results:
The nadir –suppressed serum Tg was achieved by 6 months in 58% of the patients and by 12 months in 75% of the patients. The remaining 25% of patients required 18 months or longer to reach the nadir Tg. However, in the subgroup of patients that eventually reached a nadir suppressed serum Tg<1 ng/mL (n=223 patients), this goal was achieved by 6 months in 81%, by no more than 12 months in 91%, and by no more than 18 months in 94%. In patients with a 6-month suppressed serum Tg of 1–5 ng/mL, 54% eventually developed a suppressed serum Tg of <1 ng/mL without additional therapy.
Conclusions:
In patients selected for continued observation, serum Tg levels often continue to decline for several years after total Tx and RAI-RA. While a 6–12-month assessment of the response to initial therapy is useful in patient management, strong consideration should be given to continued observation without additional therapy in patients with well-differentiated thyroid cancer who have 6-month suppressed serum Tg values of 1–5 ng/mL without a structurally identifiable disease.
Introduction
In the setting of a negative neck ultrasound at the 6–12-month evaluation, it is the suppressed and stimulated thyroglobulin (Tg) values that have the largest influence on management recommendations (1). In this context, and for the purposes of this study, “suppressed serum Tg” refers to a serum Tg value obtained with a corresponding thyrotropin (TSH)<1 mIU/L, and “stimulated Tg” refers to a serum Tg value obtained either after thyroid hormone withdrawal (TSH>25 mIU/L) or recombinant human TSH stimulation. For example, if at the 6 month evaluation, the suppressed serum Tg value is >1 ng/mL or the stimulated Tg value is >2 ng/mL, then the ATA algorithm calls for the consideration of a diagnostic whole body RAI scan. Furthermore, if the stimulated Tg value is >5–10 ng/mL, then additional diagnostic studies (such as neck and chest computerized tomography [CT], neck magnetic resonance imaging [MRI], or fluorodeoxyglucose positron emission tomography [18F-FDG PET]/CT) and empiric RAI therapy are considered. Therefore, a strict interpretation of this algorithm could lead to extensive testing and potentially additional RAI therapy, as early as 6 months after RAI-RA, for any patient with suppressed serum Tg>1 ng/mL or stimulated Tg>5 ng/mL even in the absence of a structurally identifiable disease.
Since several studies have demonstrated that serum Tg levels can decline for many years after treatment with RAI (4 –13), it is important to determine the time course of the disappearance of Tg after initial therapy. A more precise understanding of the expected time to nadir Tg after initial therapy can help avoid unnecessary diagnostic testing and empiric therapies in patients who are likely to eventually develop undetectable Tg values with observation alone.
Based on our clinical experience, we hypothesized that in the absence of a clinically apparent structural disease, serum Tg levels often continue to decline for at least 18 months after initial therapy. Furthermore, we hypothesized that in the absence of a structurally identifiable disease, many patients with suppressed serum Tg<5 ng/mL at the 6-month point will eventually achieve an undetectable suppressed serum Tg during follow-up without additional therapy. If these hypotheses are correct, then extensive evaluations and empiric therapies for patients with low-level Tg values at the 6-month evaluation point may not be necessary.
Therefore, the goal of this study was to describe the time course of Tg changes over time after initial therapy with total Tx and RAI-RA and to determine whether Tg values at the 6-month point can be used to predict the likelihood of eventually achieving an undetectable suppressed serum Tg during follow-up.
Methods
After obtaining institutional review board (IRB) approval, we retrospectively reviewed the electronic medical records of 436 adult patients with differentiated thyroid carcinoma evaluated at the Memorial Sloan-Kettering Cancer Center (MSKCC) who had undergone total Tx and RAI-RA between October 1999 and November 2007. A minimum of 3 years of follow-up after initial therapy was required for inclusion in the study.
Since the objective of this study was to determine the time course of suppressed serum Tg in response to total Tx and RAI-RA, patients who received additional therapies during follow-up that could have influenced the serum Tg levels were excluded from analysis (n=125). This included 113 patients who received additional RAI therapy, 8 patients who had subsequent neck surgery, and 4 patients who received external beam irradiation. An additional 12 patients were excluded, because the presence of interfering antibodies made the Tg determinations unreliable. Therefore, the study cohort consisted of 299 thyroid cancer patients followed over time without any additional treatments beyond the initial total Tx and RAI-RA.
All patients were risk stratified using the 7th edition of the American Joint Committee on Cancer/Union for International Cancer Control tumor–node–metastasis staging system (AJCC/UICC TNM; Stages I, II, III, IVA, IVB, and IVC) and the ATA risk of recurrence stratification system (low, intermediated, or high risk of recurrence) (14,15).
The clinical status at the time of final follow-up was classified as previously described (15). Patients were considered as having no evidence of disease (NED) at final follow-up if they had suppressed serum Tg<1 ng/mL, no detectable anti-Tg antibodies, and no structural evidence of disease confirmed by biopsy, cytology or histology, cross-sectional imaging, ultrasound, CT, nuclear magnetic resonance, functional imaging, RAI scan, or 18F-FDG PET scan (TSH-stimulated Tg values were not available at the time of final follow-up in most patients and are not required in this definition of NED). Persistent disease was defined as the presence of Tg ≥1 ng/mL, stimulated Tg ≥2 ng/mL, or any evidence of disease on cross-sectional imaging, functional imaging, or biopsy at the time of final follow-up. A recurrence was defined as new biochemical (suppressed serum Tg ≥1 ng/mL, and/or stimulated Tg ≥2 ng/mL), structural, or functional evidence of disease that was detected after any period of NED.
For each patient, all suppressed serum Tg values associated with TSH<1 mIU/mL were recorded and analyzed. The nadir suppressed serum Tg value was defined as the lowest Tg value obtained during follow-up with a corresponding serum TSH value of <1 mIU/mL.
In addition to the time to nadir Tg, the time to achieve a suppressed serum Tg of <1 ng/mL was used as a secondary endpoint. This endpoint was selected based on the functional sensitivity of the assay used in the follow-up of the early patients and because a Tg cutoff of 1 ng/mL was used to guide patient management in the 2009 ATA guidelines (1).
Tg assays
Between 1994 and 1997, a variety of Tg assays were used with functional sensitivities of ∼1 ng/mL. After 1998, serum Tg values were measured with an immunoradiometric recovery assay (Brahms, Inc., Berlin, Germany, functional sensitivity 0.6 ng/mL normalized to CRM 457) (16). Patients with interfering anti-Tg antibodies were excluded.
Statistical analysis
All data are presented as mean±standard deviations with medians and ranges presented where appropriated. A p-value<0.05 was considered statistically significant. Statistical analysis was performed using SPSS software (Version 18.0.1: SPSS, Inc, Chicago, IL).
Results
The study cohort consisted of 299 patients with differentiated thyroid cancer that required no additional treatments beyond total Tx, RAI-RA, and levothyroxine suppressive therapy. The median age at diagnosis was 46 years (range 17–77 years), 69% were women, and 92% had either classic or a follicular variant of papillary thyroid cancer (See Table 1).
SD, standard deviation; T, tumor; N, node; M, metastasis; AJCC/UICC TNM, American Joint Committee on Cancer/Union for International Cancer Control tumor–node–metastasis staging system; rhTSH, recombinant human thyroid stimulating hormone; mCi, millicurie; ATA, American Thyroid Association; NED, no evidence of disease.
Trend in Tg values continues to decline over time with continued observation
As can be seen in Figure 1, the nadir suppressed serum Tg (lowest Tg value observed in each patient) was achieved by 6 months after RAI-RA in only 58% of the patients and by 12 months in 75% of the patients. In the remaining 25% of patients, the nadir Tg was achieved 18 months or longer after RAI-RA.
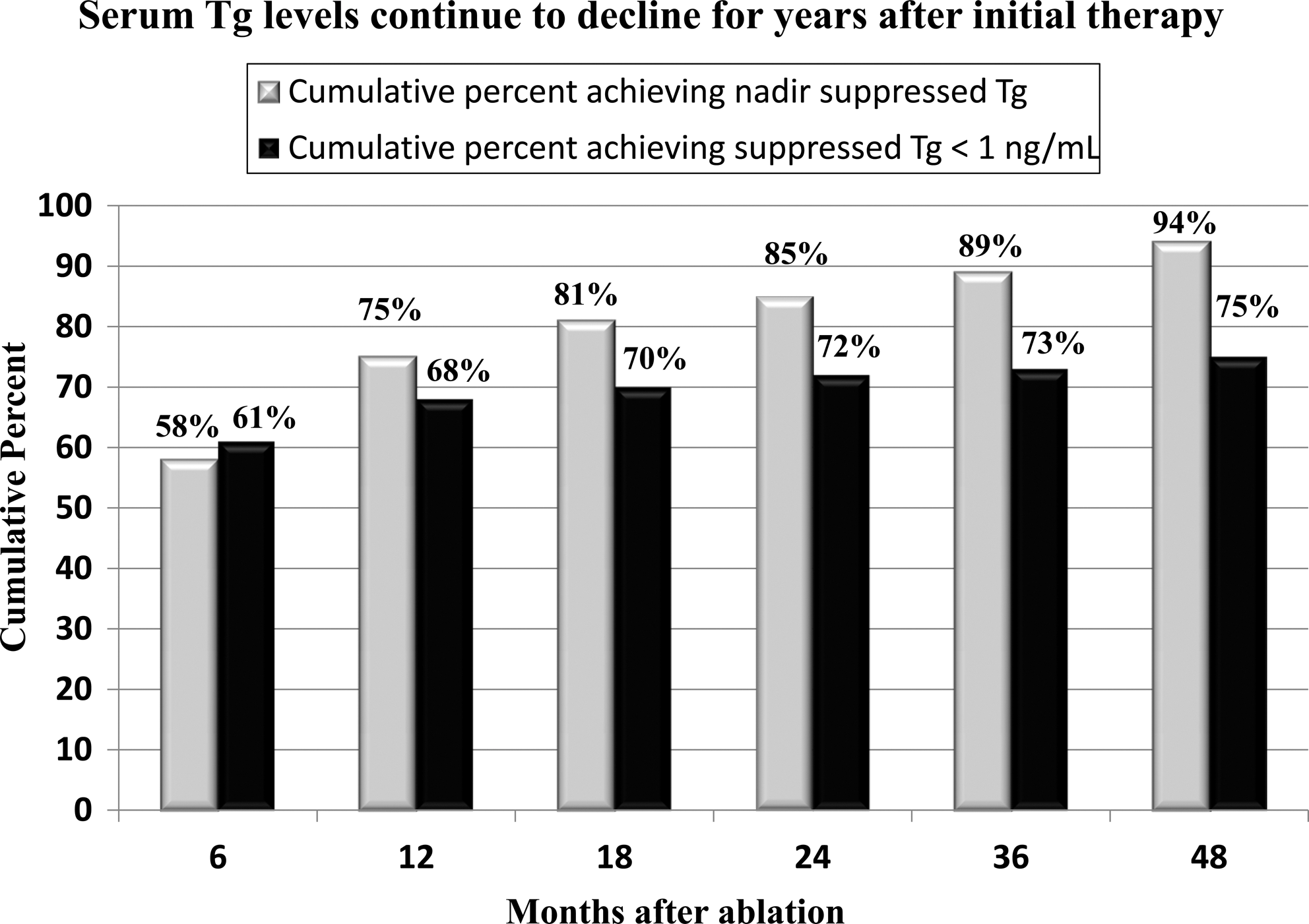
Cumulative percent of patients achieving nadir thyroglobulin (Tg) value (lowest Tg value without additional therapy) or suppressed serum Tg<1 ng/mL over time in the entire cohort (n=299).
Six months after RAI-RA, 61% (181/299) of the subjects had suppressed serum Tg<1 ng/mL. An additional 23% (69/299) had suppressed serum Tg levels from 1 to 5 ng/mL, 7% (21/299) had suppressed serum Tg levels between 5 and 10 ng/mL, and 9% (28/299) had suppressed serum Tg>10 ng/mL.
By 48 months after RAI-RA, 75% (223/299) of the cohort had achieved suppressed serum Tg<1 ng/mL while 25% (76/229) continued to have Tg values ≥1 ng/L (See Fig. 1). The percentage of patients achieving suppressed serum Tg<1 ng/mL gradually increased over time from 61% at 6 months to 75% at 48 months.
In patients who were destined to achieve suppressed serum Tg<1 ng/mL over time, 81% (181/223) had reached that nadir by 6 months (See Fig. 2). This percentage increased to 91% by 12 months, and to 94% by 18 months with a few patients achieving suppressed serum Tg<1 ng/mL after 24–48 months of observation.
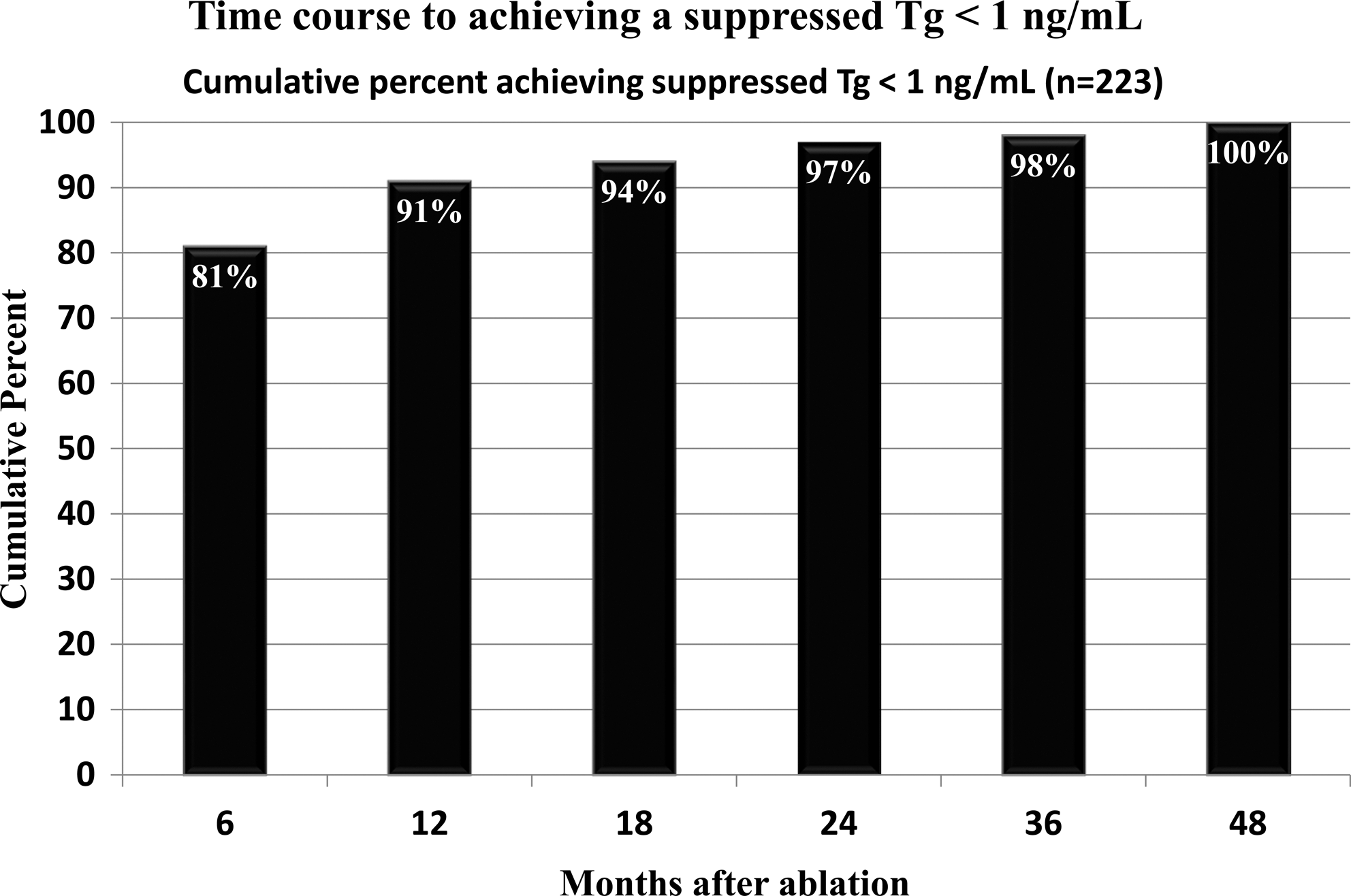
Time course for achieving a suppressed serum Tg<1 ng/mL in the 223 patients destined to reach this goal without additional therapy.
Clinical characteristics of patients who achieved suppressed serum Tg<1 ng/mL with continued observation
A comparison of the clinico-pathologic features between those patients who eventually achieved suppressed serum Tg<1 ng/L and those who maintained measurable Tg values of ≥1 ng/mL did not reveal any significant differences with regard to gender, histology, TNM stage, ATA risk stratification, age at diagnosis, size of primary tumor, method of preparation for RAI-RA, or administered activity of RAI (data not shown). However, patients who achieved suppressed serum Tg<1 ng/mL were less likely to have had N1b disease (20% vs. 29%, p<0.002) than those who had a nadir suppressed serum Tg of >1 ng/mL.
Furthermore, patients who achieved suppressed serum Tg<1 ng/mL in follow-up had significantly lower Tg values at the 6-month time point (median Tg<1 ng/mL) than patients who failed to develop Tg values of <1 ng/mL over time (median 3.0 ng/mL, p<0.002). When the suppressed serum Tg was <1 ng/mL at 6 months, 99% of the patients maintained suppressed serum Tg<1 ng/mL over the follow-up period (See Table 2). Interestingly, if the suppressed serum Tg was 1–5 ng/mL at the 6-month point, then 54% eventually achieved suppressed serum Tg<1 ng/mL during follow-up without additional treatments. Conversely, suppressed serum Tg values of >5 ng/mL at 6 months were seldom associated with the development of suppressed serum Tg values of <1 ng/mL over time with observation alone.
See text for definition of “suppressed serum Tg.”
Tg, thyroglobulin.
Tg outcomes in the 69 patients who had a 6-month suppressed serum Tg of 1–5 ng/mL
Further analysis of the 69 patients from Table 2 who had 6-month suppressed serum Tg values between 1 and 5 ng/mL did not identify any significant differences with regard to gender, histology, TNM stage, ATA risk stratification, age at diagnosis, size of primary tumor, method of preparation for RAI-RA, or administered activity of RAI between the patients who either did or did not subsequently develop suppressed serum Tg<1 ng/L (data not shown). However, patients within this group who achieved suppressed serum Tg<1 ng/mL with continued observation had significantly lower 6-month suppressed serum Tg values (median 2, mean 3.2±1.8) than patients who did not achieve this goal (median 4, mean 4.4±2, p=0.02).
In patients who achieved suppressed serum Tg<1 ng/mL, the decline in Tg that occurred during follow-up often did not follow a simple linear pattern (See Fig. 3). While a rapid linear decline to Tg levels of <1 ng/mL at the 12-month follow-up point was seen in 59% (22/37), nonlinear patterns of decline that often included mild elevations in suppressed serum Tg values were seen in 41% (15/37) of the patients who ultimately achieved suppressed serum Tg<1 ng/mL with continued observation.
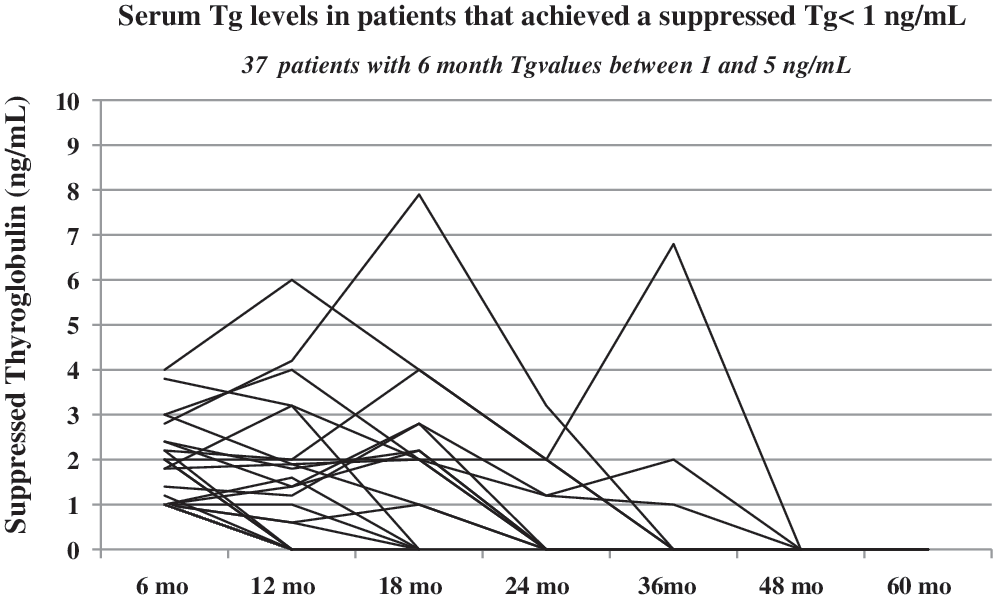
Time course for the development of a suppressed serum Tg<1 ng/mL in the 37 patients who had 6 months of Tg values of 1–5 ng/mL. Tg values <1 ng/mL were graphed as zero.
In the patients who had Tg levels of 1–5 ng/mL at 6 months and who did not eventually achieve Tg of <1 ng/mL without additional therapy, serial Tg values over 12–48 months of follow-up were quite stable with median Tg values of 2 ng/mL (range 1–5 ng/mL) at 6 months, 1.1 ng/mL (range 1–6.2 ng/mL) at 12 months, 1.0 ng/mL (range 1–5.8 ng/mL) at 24 months, and 1.4 ng/mL (1–10.6 ng/mL) at 48 months.
Discussion
In a cohort of 299 patients selected for continued observation after total Tx and RAI-RA, serum Tg levels continued to decline for years with only 75% of patients achieving their nadir Tg by 1 year after initial therapy. The remaining 25% demonstrated a nadir Tg more than 1 year after RAI-RA. In addition, the cumulative percentage of patients achieving a suppressed serum Tg value of <1 ng/L also increased with continued observation for approximately 48 months after RAI-RA. These findings are consistent with previous studies which have demonstrated that serum Tg values often continue to decline for several years after RAI administration (4 –13).
In addition to the completeness of the total Tx and the effectiveness of the RAI-RA, the percentage of patients who eventually achieve suppressed serum Tg<1 ng/mL is also dependent on initial risk stratification. As previously shown, suppressed serum Tg<1 ng/mL is achieved by 2 years after RAI-RA in 84% of ATA low-risk patients, 74% of ATA intermediate-risk patients, and only 39% of ATA high-risk patients (15). Since two thirds of the cohort described in this current article were either ATA intermediate or high risk, it is not surprising that only 75% of the cohort eventually achieved suppressed serum Tg<1 ng/mL without additional therapy.
Since additional interventions during follow-up could have had an impact on serum Tg levels, it is not possible to determine what the time to untreated nadir Tg would have been in patients who received additional surgery or RAI therapy. Therefore, these data regarding the time to nadir Tg and time needed to achieve suppressed serum Tg<1 ng/mL during follow-up are most applicable to patients with persistently elevated Tg levels without the structural evidence of persistent/recurrent disease who were selected for continued observation rather than early retreatment.
Since the percentage of patients who achieve nadir Tg and suppressed serum Tg<1 ng/mL continue to increase over time, it seems reasonable to resist giving additional therapies for at least 12–18 months in patients with persistently low-level Tg values without the structural evidence of disease. This is particularly important in the patients who had a suppressed serum Tg between 1 and 5 ng/mL at the 6-month follow-up, as 54% of these patients will eventually achieve suppressed serum Tg<1 ng/mL with continued observation alone. Cautious observation can avoid additional RAI therapies in a substantial number of patients with persistently low-level Tg values without structural evidence of disease after initial therapy.
However, patients with suppressed serum Tg values of >5 ng/mL at 6 months of follow-up are more likely to benefit from additional imaging in order to identify clinically significant disease, as the likelihood of identifying structural disease increases in patients with significant Tg elevations (16). However, if additional imaging fails to identify structural disease, then a substantial number of these patients will have a continued slow decline in suppressed serum Tg values over several years of follow-up. In the absence of structurally evident disease, there appears to be little need for urgent retreatment with RAI in patients with persistent, stable, and biochemical evidence of disease, as the 10-year survival in this group of patients is nearly 100% (17,18). Therefore, cautious observation over 12–24 months may be prudent in order to identify those patients who are going to have a continued decline in serum Tg levels over time without additional therapies. Additional interventions could be reserved for those patients who demonstrate a significant, sustained rise in serum Tg values over time, as a progressive increase in Tg levels over time is associated with an increased risk of structural disease progression (7,9,17).
One of the challenges of continued observation is the variability in Tg levels within the same patient over time. Even in patients who eventually achieved suppressed serum Tg<1 ng/mL, serum Tg levels often increased slightly before declining to undetectable levels. These data indicate that continued observation is appropriate even with low-level Tg fluctuations that do not demonstrate a consistent increase over time. Some of the variations in these Tg levels could have been due to minor variations in TSH levels, as all Tg values associated with a TSH of <1 mIU/L were included in the analysis. Alternatively, the presence of Tg antibodies that were not detected in our assay is another potential cause of artifactual changes in serum Tg levels (19).
These data are also directly relevant to the management of patients who have persistently elevated Tg levels without the structural evidence of disease in the setting of a negative diagnostic whole body scan. Since the natural history for many of these patients will be a slow decline in serum Tg values over time, simply showing decreasing Tg values after an empiric RAI therapy should not be considered evidence of therapeutic effectiveness. Multiple studies of Tg positive/RAI scan negative patients have shown that serum Tg levels often decrease over time whether or not additional empiric RAI therapy is given (4,8,10,12,13,20). As with our data, the likelihood of achieving undetectable Tg levels over time with continued observation was higher in patients who had the lowest Tg levels after initial therapy (5,12). These studies support a cautious observation approach to these patients rather than the routine empiric administration of additional RAI for patients with stable, persistently low level serum Tg values in the absence of a structrually identifiable disease.
In conclusion, in the absence of structural disease, serum Tg levels continue to decline for many years after total Tx and RAI-RA. The continued decline in serum Tg is of most clinical relevance to the patients who have suppressed serum Tg values in the 1–5 ng/mL range with a negative neck US at the 6-month evaluation afterRAI-RA. Since more than 50% of these patients will develop suppressed serum Tg<1 ng/mL without additional therapy, continued observation should be recommended for these patients rather than early empiric therapy. Furthermore, since suppressed serum Tg levels show considerable variability within an individual patient over time, additional imaging and therapy should be reserved for those patients demonstrating a consistent rise in serum Tg demonstrated by at least two consecutive Tg measurements over time. A conservative approach to patients with biochemical evidence of disease in the absence of structurally evident disease has the potential to decrease the likelihood that an empiric therapy will be given to a patient who is very likely to have an excellent late response to initial therapy.
Footnotes
Disclosure Statement
R.P., E.R., and M.B. have nothing to declare. R.M.T. is a consultant to and has received honoraria from the Genzyme Corporation.