
Abstract
Background:
The absorption of levothyroxine (LT4) is affected by many factors. Bariatric surgery is recommended in severely obese patients. The aim of this study was to determine the consequences of bariatric surgery on LT4 pharmacokinetic parameters, and to identify the regions of the gastrointestinal tract where LT4 is absorbed in patients with severe obesity before and after surgery.
Methods:
We studied 32 severely obese nonhypothyroid patients who underwent sleeve gastrectomy (SG; n=10), Roux-en-Y gastric bypass (RYGBP; n=7), or biliopancreatic diversion with long limbs (BPD-LL; n=15). Before surgery, from 8:00 a.m., blood samples were collected before and every 30 minutes after the oral administration of a solution of 600 μg of LT4. The same procedure was repeated 35 days after surgery. We estimated the pharmacokinetic parameters of LT4 before and after surgery, including the area under the curve (AUC), the peak thyroxine concentration (C max), and the time to peak thyroxine concentration (T max).
Results:
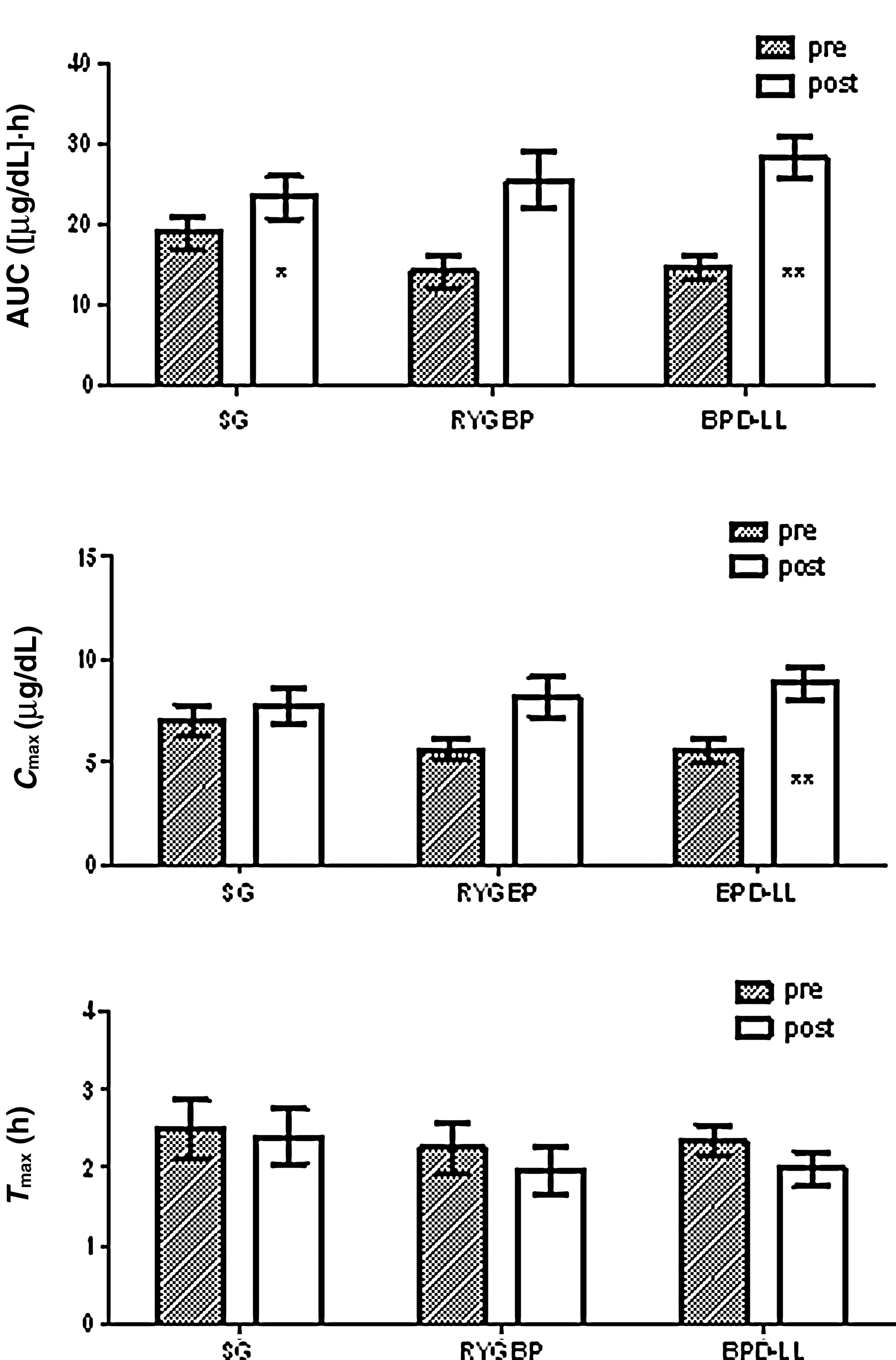
Following surgery, in the SG group, the mean AUC was higher than it was before surgery (18.97±6.01 vs. 25.048±6.47 [μg/dL]·h; p<0.01), whereas the values of C max and T max were similar to those before surgery. In the RYGBP group, mean AUC, C max, and T max were similar before and after surgery. In the BPD-LL group, mean AUC and C max were higher after surgery than before (14.18±5.64 vs. 25.51±9.1 [μg/dL]·h, p<0.001; 5.62±1.34 vs. 8.16±2.57 μg/dL, p<0.001, respectively), whereas T max was similar.
Conclusions:
The pharmacokinetic parameters of LT4 absorption are improved following SG and BPD-LL types of bariatric procedures. We conclude that the stomach, the duodenum, and the upper part of the jejunum are not sites for LT4 absorption, because in the above-mentioned bariatric procedures these are bypassed or removed.
Introduction
Bariatric surgery has gained acceptance as one treatment of choice for severely obese patients, especially in those with comorbidities such as diabetes mellitus type 2 (8). In the United States, the number of bariatric procedures performed annually increased from ∼16,000 in the early 1990s to ∼103,000 in 2003 (9).
It has been reported that severely obese patients require higher replacement or suppressive doses of LT4 owing to their higher lean body mass (10), as well as their greater blood volume and/or delayed gastrointestinal absorption of LT4 (11). Case reports have shown that the dose of LT4 required in hypothyroid patients increases after bariatric surgery (12,13).
In the several types of bariatric procedures, such as sleeve gastrectomy (SG), Roux-en-Y gastric bypass (RYGBP), and biliopancreatic diversion with long limbs (BPD-LL), different parts of gastrointestinal tract are bypassed or removed, and this could affect LT4 absorption. Studies in patients before and after surgery would provide information regarding the sites of LT4 absorption, based on these differences.
The aim of the study described herein was to study the effects of bariatric surgery on the pharmacokinetic parameters of LT4 in severely obese patients, and to study the gastrointestinal sites of LT4 absorption.
Materials and Methods
Patients
We studied 32 severely obese patients, who underwent several types of bariatric surgery. The participants had no history of endocrine disease or any comorbidities related to obesity, and they were not receiving any medication. They all had negative antibody titers for Helicobacter pylori. The participants were divided into three groups on the basis of the type of surgery received. The SG group consisted of 10 patients, aged 32.5±6.49 years (range 18–50 years) with a body–mass index (BMI) of 42.12±2.1 kg/m2, who underwent SG. The RYGBP group consisted of 7 patients, aged 35.86±7.6 years (range 18–50 years) with a BMI of 44.1±2.47 kg/m2, who underwent RYGBP. The BPD-LL group consisted of 15 patients, aged 32.8±11.03 years (range 18–50 years) with a BMI of 52.96±7.1 kg/m2, who underwent BPD-LL (Table 1).
SG group: patients who underwent sleeve gastrectomy; RYGBP group: patients who underwent Roux-en-Y gastric bypass; BPD-LL group: patients who underwent biliopancreatic diversion with long limbs. Values are expressed as mean±SD.
BMI, body–mass index; T4, thyroxine; T3, triiodothyronine; TSH, thyrotropin; AUC, area under the curve; C max, peak T4 concentration; T max, time to peak T4 concentration; ns, not significant.
Informed written consent was obtained, and the study protocol was approved by the Ethics Committee of our hospital.
Study design
All participants visited our outpatient clinic for their initial screening examination. A complete medical history was obtained and a physical examination was performed, as well as a biochemical count and determination of serum triiodothyronine (T3), T4, thyrotropin (TSH), and anti–thyroid peroxidase antibodies (TPOAbs). One month before the scheduled surgery, all participants underwent an LT4 absorption test (as described previously) (10). Briefly, 8:00 a.m. after an overnight fast, blood samples were collected 0.5 and 0.25 hours before the oral administration of a solution of 600 μg of LT4. The oral solution was prepared by diluting sodium LT4 powder (Faran Co., Athens, Greece) with 95% absolute alcohol, and then diluting with water to a final concentration of 600 mg of LT4 per 240 mL. Further blood samples were collected at 0.5, 1, 1.5, 2, 2.5, 3, and 4 hours post–administration of LT4. No food or liquids other than water were allowed per os during the period of sample collection. Blood samples were centrifuged immediately and stored at −20°C until assayed. All patients favorably tolerated the administration of 600 μg of the LT4 solution. Baseline values were considered to be the mean of the values obtained at the 0.5, 0.25, and 0 hour time points. The same procedure was repeated 35 days after bariatric surgery (after the washout period). All operations were performed by the same experienced surgeon.
Types of bariatric surgery
As noted, the three types of bariatric surgery were SG, RYGBP, and BPD-LL. During SG, the greater curvature of the stomach was divided from the left crus of the diaphragm to the distal antrum. Dissection of the stomach began 3 cm from the pylorus, close to a 33-Fr bougie, and preceded up to the incisura angularis. The use of a 33-Fr bougie corresponds to a sleeve volume of 50–60 mL. The main outcomes of the RYGBP procedure included a small gastric pouch of 15±5 mL, a biliopancreatic limb of 50 cm, and an alimentary limb of 150 cm. The BPD-LL was a variant of BPD and was the procedure of choice for the super-obese patients (BMI>50 kg/m2) (14). The main outcomes of the BPD-LL procedure were (i) a gastric pouch of 60 mL, (ii) a common limb of 100 cm, (iii) an alimentary limb that was almost always equal to 400 cm, and (iv) the remainder of the small intestine as the biliopancreatic limb.
Cholecystectomy was performed during every bariatric procedure, with the addition of appendectomy in the BPD-LL procedure.
Assays
Serum T3, T4, TSH, and TPOAbs were measured by chemiluminescence immunoassays (E170 Module for Modular Analytics; Roche Diagnostics GmbH, Mannheim, Germany). The samples were assayed in a single large batch. The intra-run and inter-run coefficients of variance were 1.5%–3.1% and 1.3%–1.7% for T3, 1.1%–3.0% and 3.7%–4.5% for T4, and 3.4%–4.2% and 3.3%–7.2% for TSH, respectively.
Statistics
All values are expressed as mean±SD. Statistical significance was set at a p-value of <0.05. The pharmacokinetic parameters of area under the curve (AUC) from the baseline to 4 hours, peak T4 concentration (C max), and time to peak concentration (T max) were estimated to evaluate the extent and the rate of absorption of LT4, in accordance with U.S. Food and Drug Administration (FDA) recommendations (15). To avoid misinterpretation of the LT4 values owing to the endogenous production of T4, researchers generally use three methods to correct the AUC and C max (16) and another one proposed by Eisenberg et al. (17). In the first method (method A), it is assumed that there is no suppression of the release of endogenous T4 and TSH and that the endogenous production of T4 remains constant throughout the sampling period following the administration of a large exogenous dose of LT4. In the second method (method B), it is assumed that the endogenous production of T4 is suppressed completely. In the third method (method C), it is assumed that there is no suppression of endogenous T4, but the calculation takes into account the diurnal variation in T4 levels. The three methods of mathematical correction yield similar results for the key bioequivalence parameters of AUC, C max, and T max (18). We used the first method of correction and evaluated the AUC and C max as follows: we subtracted the baseline T4 value from the T4 concentration at every time point after the administration of LT4 (18). Also, we estimated the AUC and C max using the above-mentioned Eisenberg method (17). To compare the mean values pre- and postsurgery in the same group, we performed a paired-samples t-test, whereas we used one-way analysis of variance (ANOVA) to compare the mean values among the groups.
We calculated the pre- and postsurgery plasma volume (PV) in all patients as follows. First, we calculated the blood volume index (inBV) according to the formula, which estimates the blood volume in obese and morbidly obese patients: inBV=70/√(BMI/22) (19). Second, we multiplied inBV by the body weight to determine the total blood volume. Third, taking into account the individual hematocrit of each patient, we calculated the PV.
The data were analyzed using SPSS version 17 (SPSS, Inc., Chicago, IL).
Results
At baseline, body weight and BMI were higher in the BPD-LL group (one-way ANOVA, p<0.001) and T4 was higher in the RYGBP group than in the other two groups (one-way ANOVA, p<0.01), whereas the mean age and the mean serum concentrations of T3 and TSH were similar among the groups (Table 1).
We chose to analyze our data in accordance with FDA recommendations by using the method widely accepted in the literature, method A (15,16). The pharmacokinetic parameters of LT4 were similar among the groups (Table 1).
In the SG group, the mean AUC postsurgery was higher (18.97±6.01 vs. 25.048±6.47 [μg/dL]·h, paired t-test: p<0.01), whereas mean body weight, BMI, and T3 were lower (paired t-test: p<0.001, p<0.001, p<0.001, and p<0.01, respectively) compared with presurgery values. In addition, there was a trend toward C max being higher postsurgery (paired t-test: p=0.07) compared with presurgery, whereas mean T4, TSH, and T max were similar (Table 2; Figs. 1 and 2).
Pre- and postbariatric surgery pharmacokinetic parameters in the three groups of patients. SG group: patients who underwent sleeve gastrectomy; RYGBP group: patients who underwent Roux-en-Y gastric bypass; BPD-LL group: patients who underwent biliopancreatic diversion with long limbs. Values are expressed as mean±SD.
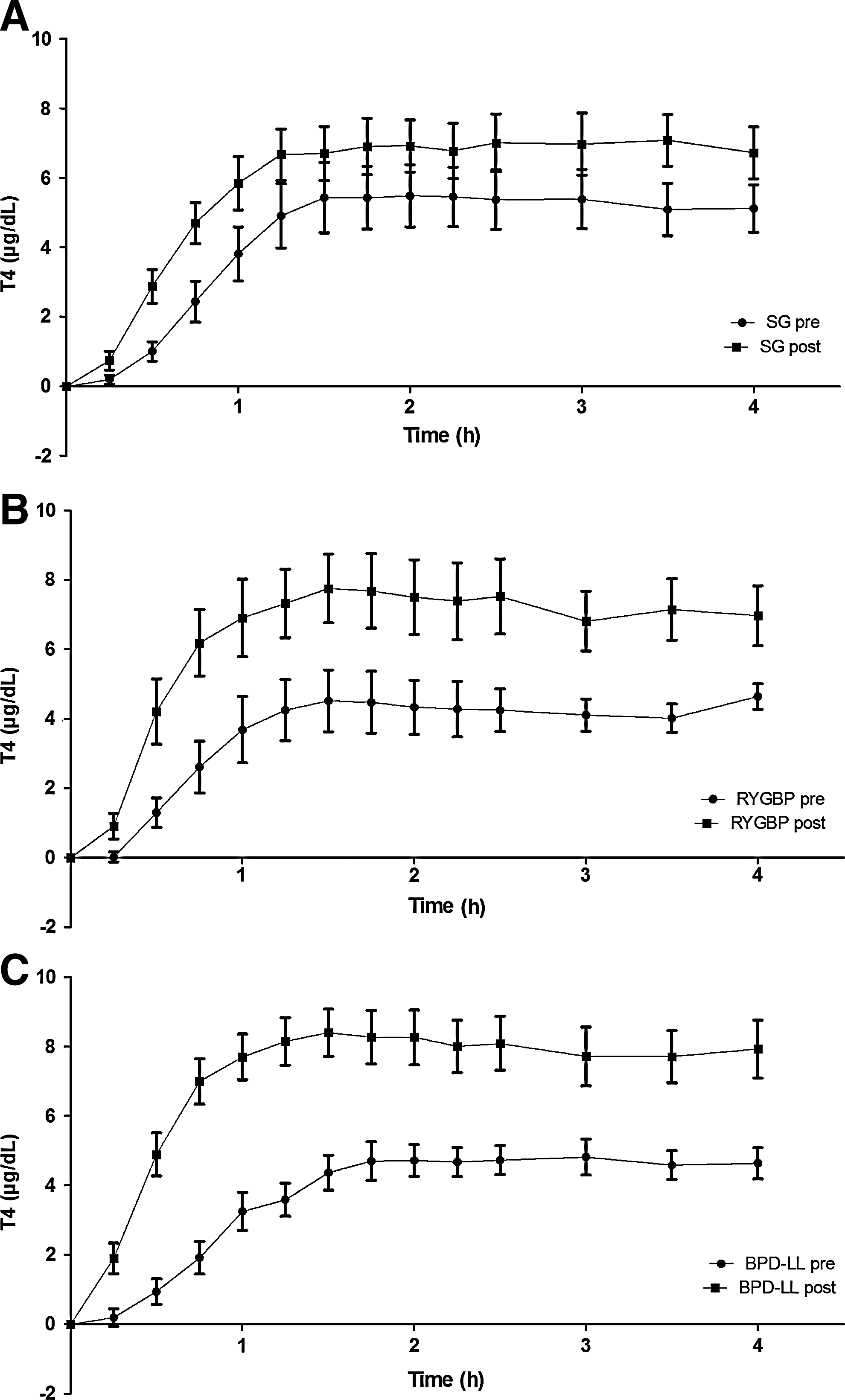
Pre- and postbariatric surgery corrected mean serum thyroxine (T4) concentrations postadministration of the oral solution of 600 mg LT4 in the three groups of patients.
Values are expressed as mean±SD.
p<0.001; b p<0.01; c p<0.05.
PV, plasma volume.
In the RYGBP group, the mean AUC and C max had a statistically insignificant tendency to be higher postsurgery than presurgery (paired t-test: p=0.07 and p=0.07, respectively), whereas the mean values of T4, TSH, C max, and T max were similar, and mean body weight, BMI, and T3 were lower (paired t-test: p<0.001, p<0.001, p<0.001, and p<0.05, respectively; Table 2 and Figs. 1 and 2).
In the BPD-LL group, the mean AUC and C max were higher postsurgery than presurgery (paired t-test: p<0.001 and p<0.001, respectively), whereas the mean body weight, BMI, and T3 were lower (paired t-test: p<0.001, p<0.001, p<0.001, and p<0.001, respectively). The mean values of T4, TSH, and T max were similar (Table 2 and Figs. 1 and 2).
Using Eisenberg's method (17), we found no difference in AUC and C max pre- and postsurgery in the SG and RYGBP groups (AUC: SG 19.07±6.01 vs. 23.42±8.25 [μg/dL]·h, RYGBP 14.33±5.60 vs. 25.53±9.03 [μg/dL]·h; C max: SG 7.03±2.32 vs. 7.81±2.73 μg/dL, RYGBP 5.67±1.33 vs. 8.19±2.58 μg/dL), whereas both parameters were higher postsurgery in the BPD-LL group (AUC: 14.84±5.92 vs. 28.28±9.75 [μg/dL]·h, p<0.001; C max: 5.61±2.07 vs. 8.89±3.02 μg/dL, p<0.001).
PV remained similar pre- and postsurgery in all groups (Table 2).
The pharmacokinetic parameters and the levels of thyroid hormones and TSH were similar among the groups postsurgery (Table 3).
Values are expressed as mean±SD.
Discussion
We noted that, in the patients with severe obesity who underwent different types of bariatric surgery, the pharmacokinetic parameters of LT4, such as AUC and C max, were not decreased after bariatric surgery, but, in fact, were increased in the SG and BPD-LL groups. Patients who undergo restrictive or malabsorptive bariatric surgery are characterized by almost total functional absence of the stomach. In the SG procedure, ∼90% of the stomach is removed, but the rest of the gastrointestinal tract remains intact. In RYGBP, the remaining gastric pouch is extremely small (15±5 mL), the duodenum and a small part of the jejunum are bypassed, and the food encounters the biliopancreatic secretions in a common limb. In BPD-LL, a small gastric pouch is also created, the alimentary limb is two to three times longer than in RYGBP, and the duodenum, the jejunum, and a part of the ileum are bypassed. The food eventually encounters the biliopancreatic secretions ∼1 m before the ileocecal valve. Therefore, since the postsurgery increments of LT4 pharmacokinetic parameters were observed in SG and BPD-LL procedures, we conclude that the main sites of absorption of LT4 were the lower part of the jejunum and the ileum, whereas the role of the stomach is restricted to the process of dissolution of LT4.
We used method A, a method that is recommended by the FDA to estimate the pharmacokinetic parameters AUC, C max, and T max for LT4 (15), to avoid misinterpretation of the LT4 values due to endogenous T4 production. The main finding of our study was the postsurgical increment of AUC and C max. This increment was significant in the SG and BPD-LL groups. In addition, using Eisenberg's method, both parameters were higher postsurgery in the BPD-LL group. Given that the AUC represents the extent of absorption and the C max represents the rate of absorption of LT4, it is noteworthy that the absorption of LT4 is increased postoperatively, as estimated by these pharmacokinetic parameters.
These findings are not easy to explain. In humans, data on the physiology and the sites of LT4 absorption in the gastrointestinal tract are limited to a small number of observations (7,8). Case reports have shown that a greater number of patients require LT4 replacement therapy after bariatric surgery than before (12,13). However, these studies were based on a small number of patients and were characterized by methodological flaws. In a recently published clinical study on the use of LT4 tablets in morbidly obese patients who had undergone RYGBP, the opposite result was reported (20). The authors commented that “it is tempting to bring forward a hypothesis that the new configuration of the gut after Roux-en-Y bypass, with the jejunoileal segment placed immediately below the gastric pouch, might create a new situation favorable to LT4 absorption.” Our findings confirm these results using the same correction method for the pharmacokinetic parameters. However, this study (20) has several limitations, including the fact that the same patients were not compared before and after their bariatric surgery, and the fact that the patients who participated suffered from different diseases of the thyroid.
It seems paradoxical that, in the patients who had undergone various types of bariatric surgery, the conventional pharmacokinetic parameters of LT4 were not decreased, but rather were increased. These findings could be attributed to several factors. Postsurgical changes in biliopancreatic secretions may affect absorption of LT4. The LT4 solution administered traverses the alimentary limb in the absence of biliopancreatic secretions following the malabsorptive procedures of RYGBP and BPD-LL. In the patients who have undergone the BPD-LL procedure, the LT4 solution encounters biliopancreatic secretions 1 m before the ileocecal valve. This common limb is much longer in the patients who have undergone the RYGBP procedure. These changes in patients who have undergone RYGBP or BPD-LL mean that LT4 passes the main sites of absorption without encountering biliopancreatic secretions. It is documented that the biliary secretions contain bilirubin linked with glucuronides, cholesterol, and cholesterol esters, together with fatty acids, lecithin, and bile salts. We hypothesize that the decreased availability of bile—especially of glucoronides, including glucoronized T4—enhances the absorption of LT4. It has been postulated that T4 penetrates the bowel mucosa by an active transport mechanism and is glucoronized subsequently, because the intestinal mucosal cell membrane is impermeable to glucoronized T4 (21). In addition, it is known that several drugs induce hepatic glucoronization, which leads to decreased serum levels of T4 (22 –24). Given that the biliary secretions are reduced, the enhanced absorption of LT4 under these conditions may be due to the reduction in glucoronized T4. However, a number of authors report that glucoronized T4 is absorbed as effectively as T4 (24). An additional mechanism that could explain our results is the cell proliferation that has been observed in the jejunal mucosa after RYGBP (25). Also, changes in gut microbiota after bariatric surgery have recently been reported (26,27). It is known that the stomach contributes to LT4 absorption by enhancing the solubility of T4 tablets, a result of the acidic pH (28). Moreover, T4 is more soluble in either acidic or basic solutions than in neutral solutions. We could speculate that the absence of stomach acids did not neutralize the administered basic LT4 solution. Another factor contributing to the observed increase of LT4 postsurgery pharmacokinetic parameters is the reduced binding of LT4 to the proteins normally present in the stomach and duodenum. It has been reported that LT4 tablet absorption is increased in dumping syndrome after Billroth 2 surgery and decreased when accompanied by a significant amount of albumin (29,30). More studies are needed to confirm the assumptions described previously.
We also found that the mean level of serum T3 decreased in all groups after bariatric surgery. For the first month after bariatric surgery, all patients consumed a low-calorie diet (800 kcal/day), and they lost a significant amount of their initial body weight. It is known that fasting induces alterations in the hypothalamic–pituitary–thyroid axis, and this is a model of the nonthyroidal illness syndrome (31 –33). We considered that the low values of serum T3 observed postsurgery could be attributed to fasting.
In conclusion, LT4 absorption was not decreased after three different bariatric surgery procedures as assessed by studying the LT4 pharmacokinetic parameters. Rather, LT4 absorption appears to increase after the SG and BPD-LL procedures as assessed by AUC and C max pharmacokinetic parameters. We conclude that because the stomach, duodenum, and upper part of the jejunum are bypassed or removed in these procedures, it appears that LT4 is absorbed primarily in the lower part of the jejunum and the ileum. These findings are not consistent with previous reports of studies in patients with hypothyroidism after bariatric surgery. Thus, we conclude that the stomach and the duodenum are not sites for the absorption of LT4.
Footnotes
Disclosure Statement
The authors have nothing to disclose.