
Abstract
Background:
Patients with goiter often complain of compressive symptoms, which may contribute to symptoms of obstructive sleep apnea (OSA). However, the impact of thyroid enlargement on these symptoms is not clear. Therefore, we sought to evaluate whether symptoms of sleep apnea resolved after thyroidectomy by using a validated questionnaire.
Methods:
The Berlin Questionnaire, a validated sleep apnea assessment tool, was provided to patients at a single academic institution before and after thyroidectomy. Patients who admitted to symptoms of snoring were asked to complete the questionnaire before and 8 weeks after surgery to assess for improvement in symptoms. The questionnaire uses 3 categories of questions to determine risk of sleep apnea. Two symptom categories must be positive for a patient to be considered high risk for sleep apnea.
Results:
Forty-five patients completed both pre- and postoperative questionnaires. The average age of patients completing the questionnaire was 53±2 years, and 78% of patients were female. Average body mass index was 33.3±1.4 kg/m2. Based on their preoperative questionnaire score, 71% of patients were considered to be high risk for OSA, and this decreased to 51% after surgery (p=0.002). Overall scores significantly improved after surgery (mean 2.0 vs. 1.6, p<0.0001). Specifically, patients noted a significant decrease in snoring frequency after surgery (p=0.002), as well as a significant decrease in whether or not their snoring bothered others (p=0.004). The frequency of nodding off during the day also significantly decreased after surgery (p=0.02). Among patients with ≥25% improvement compared with those with <25% improvement in scores, the only significant difference found was a higher preoperative thyrotropin among patients with <25% improvement (p=0.03). No significant difference was found between age, gender, presence of compressive symptoms, gland weight at resection, presence of thyroiditis, or the largest dimension of the gland at resection.
Conclusions:
Thyroid surgery appears to significantly improve symptoms of OSA in patients who screened positive for symptoms before surgery. Evaluation of patients with OSA should include evaluation of thyroid disease, as symptoms of sleep apnea may improve with thyroidectomy.
Introduction
Patients considered to be at high risk for OSA include those with obesity (body mass index [BMI] >35), type 2 diabetes, pulmonary hypertension, congestive heart failure, atrial fibrillation, treatment refractory hypertension, and patients who have had a stroke. Increased neck circumference (>17 inches in men and 16 inches in women) has also been associated with increased risk of OSA (5). The gold standard for a diagnosis is overnight polysomnogram. Home testing with portable monitors have been used in the evaluation of patients with suspected OSA (6). Validated questionnaires have also proven effective in determining patients at high risk of OSA, including the Epworth Scale and the Berlin Questionnaire. The Berlin Questionnaire, created in 1996 by pulmonary and primary care physicians, was designed to focus on a limited number of known risk factors for sleep apnea, including snoring behavior, wake-time sleepiness or fatigue, and the presence of obesity or hypertension. The questionnaire accurately detects patients who ultimately meet or exceed respiratory disturbance index used in diagnostic classifications of the OSA syndrome (3). Standard treatment of sleep apnea is continuous-positive airway pressure (CPAP), and alternative treatments include behavioral therapy, oral appliances, adjunctive therapies, or surgery. Surgical options include upper airway procedures or tracheostomy (6).
Untreated hypothyroidism is associated with OSA, mainly due to upper airway narrowing related to thickening of the pharyngeal walls (7). These changes are reversible with correction of the hypothyroid state. The presence of a large goiter, independent of thyroid function, has also been associated with an upper airway obstruction due to tracheal deviation. Small case series have demonstrated improvement in symptoms of sleep apnea after thyroid surgery in patients with goiter. Preoperatively, flow–volume curves demonstrated an expiratory plateau, suggestive of an intrathoracic upper airway obstruction. After thyroidectomy, some patients required a lower CPAP airway pressure or were able to discontinue CPAP due to complete resolution of their OSA (8 –12). However, most studies have limited their evaluation to patients with large goiters.
Compressive symptoms from goiter include orthopnea, dysphagia, cough, and hoarseness. Substernal goiters are most commonly due to multinodular goiter, large follicular adenomas, and chronic Hashimoto's thyroiditis (13). Although orthopnea is a known complication of an enlarged thyroid gland, and small case series have reported improvement in OSA after thyroidectomy for goiter, it remains unclear what symptoms due to OSA improve after thyroid surgery, and if patients with thyroid disease not due to goiter have improvement in symptoms of sleep apnea after thyroid surgery. OSA is not currently identified as an indication for thyroid surgery, and a diagnosis of OSA does not always prompt an evaluation for thyroid disease.
Therefore, the relationship between thyroid disease and OSA remains unclear. In this study, we sought to evaluate whether symptoms of sleep apnea resolved after hemithyroidectomy or total thyroidectomy, regardless of surgical indication, by using a validated questionnaire.
Materials and Methods
This was an Institutional Review Board–approved, prospective study performed at a single academic institution from March 2010 through June 2011. Patients undergoing thyroid surgery (lobectomy or total thyroidectomy) for any reason were asked to complete a survey as part of their preoperative evaluation. Indications for surgery included a variety of conditions including: nodules/goiter (diffuse enlargement with substernal extension, airway compromise, cosmetic concerns, and nodule size > 4 cm), fine-needle aspiration biopsy results consistent with cancer or suspicious for cancer, presence of compressive symptoms (dysphagia, difficulty breathing, or pressure in their neck), and hyperthyroidism.
Surgery was performed by one of the two endocrine surgeons at our institution. All patients were asked if they snored. If patients answered yes to snoring, they were asked to complete an additional survey, the Berlin Questionnaire, before surgery and 8 weeks postoperatively.
The Berlin Questionnaire is a validated sleep apnea assessment tool. It consists of 10 questions in 3 categories that determine risk for obstructive sleep apnea. In category 1, high risk was defined as persistent symptoms (>3–4 times per week) in two or more questions about their snoring volume, frequency of snoring, whether or not snoring bothered others, and frequency of witnessed apneic episodes. In category 2, high risk was defined as persistent (>3–4 times per week) wake-time sleepiness, drowsy driving, or both. In category 3, high risk was defined as a history of high blood pressure or BMI>30. To be considered at high risk, a patient had to qualify for at least two symptom categories (3,14). Patient symptom severity is based on self-report. (See Supplementary Data, available online at
A statistical analysis was performed using Microsoft Excel (2003 for Microsoft Windows, Microsoft, Redmond, WA). Results are expressed as the mean±SEM. Throughout the statistical analysis, the significance level was set as p≤0.05.
Results
During the study period, 235 patients underwent a thyroidectomy of which 24% (n=56) screened positive for snoring symptoms and completed the preoperative questionnaire. Forty-five patients completed the postoperative questionnaire for an 85% response rate. The average age of patients completing the questionnaire was 53±2 years, and 78% of patients were female. Average BMI was 33.3±1.4 kg/m2 (range 18.6–68.9 kg/m2). The average thyroid gland weight at surgical resection was 39.8±6.4 g. Twenty-nine patients (64%) admitted to compressive symptoms at their preoperative visit. Indications for surgery were as follows: goiter (n=13, 29%), compressive symptoms (n=6, 13%), nodules > 4 cm (n=14, 31%), thyroid cancer (n=10, 22%), and Graves' disease (n=2, 4%).
Surgical treatment consisted of a total thyroidectomy in 33 (73%) patients and a thyroid lobectomy in 12 (26%) patients. Of the 33 patients who underwent total thyroidectomy, the overall score improved significantly (mean preoperative score 18.1±0.9 and mean postoperative score 15.3±0.9, p=0.008). Seven patients had known sleep apnea and used CPAP machines at home at night preoperatively, and one patient no longer required CPAP after surgery, although they did not undergo formal repeat sleep evaluation. The average gland weight of patients undergoing total thyroidectomy was 44.7±7.9 g (median 27.4 g and range 7.3–200 g).
Of the patients who underwent hemithyroidectomy, the average weight of their thyroid lobe at resection was 28.3±11.0 g (median 12.7 g and range 3.2–138.6 g). This group's overall scores also improved significantly (mean preoperative score 17.9±1.8 and mean postoperative score 13.8±1.4, p=0.03). Two of the patients who underwent hemithyroidectomy had confirmed sleep apnea by polysomnography and were using CPAP machines at home at night preoperatively.
Based on their preoperative questionnaire score, 71% of patients of the entire cohort were considered to be high risk for OSA, this decreased to 51% after surgery (p=0.04). Overall scores significantly improved after surgery (17.5±0.7 preoperatively vs. 14.9±0.8 postoperatively, p=0.003, Fig. 1). Symptoms in all three categories significantly improved after surgery (mean 2.0 vs. 1.6, p<0.0001) (Table 1). Specifically, patients noted a significant decrease in snoring frequency after surgery (p=0.002), as well as a significant decrease in whether or not their snoring bothered others (p=0.004). The frequency of nodding off during the day also significantly decreased after surgery (p=0.02). Patients with compressive symptoms before surgery (n=29, 64%) had an average improvement in the overall score of 2.2±0.8, while those without compressive symptoms had an average improvement in the overall score of 3.4±1.8. These scores were not significantly different (p=0.99).
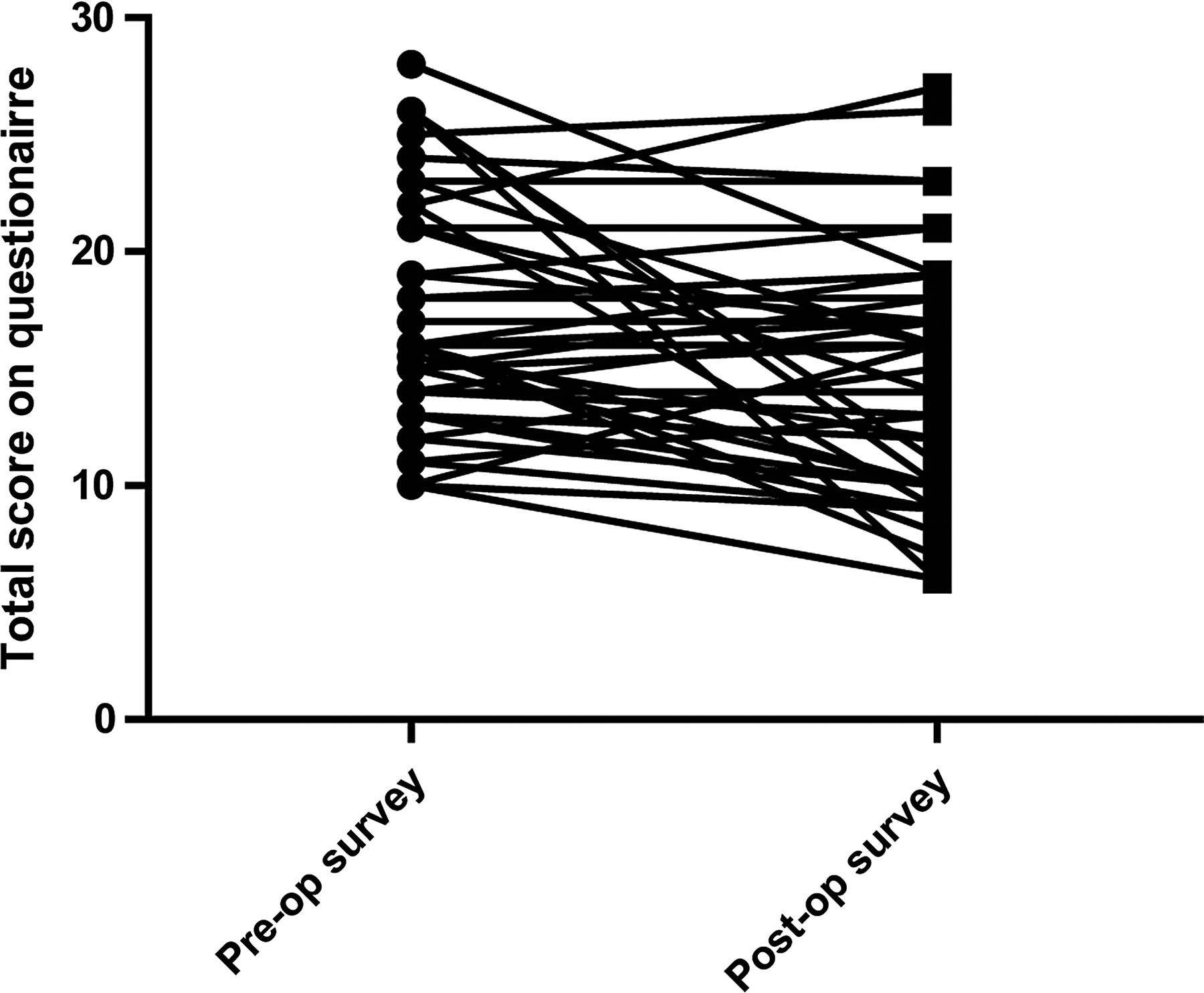
Individual data points for preoperative and postoperative scores.
Bolded p-values indicate statistical significance (p<0.05).
A 25% or greater improvement in the overall score after surgery was seen in 29% of patients (Table 2). Interestingly, the only significant difference between patients with ≥25% improvement and patients with <25% improvement was the preoperative thyrotropin (TSH) value (1.4±1.8 vs. 2.0±1.5 mIU/L, p=0.03). Surprisingly, there was no significant difference in the weight of the thyroid tissue removed between patients with ≥25% improvement in scores (37.2±12.1 g) and patients with <25% improvement in scores (40.9±7.7), p=0.51, or in the largest dimension of the thyroid tissue removed (p=0.79). The presence of thyroiditis, defined having thyroid antibodies or findings of autoimmune thyroid disease on final pathology, did not differ between patients with ≥25% improvement in scores (31% patients had thyroitidis) versus patients with <25% improvement in scores (33% patients had thyroiditis) (p=0.88). Also, there was no significant difference in age (p=0.89), percent female patients (p=0.36), presence of compressive symptoms preoperatively (p=0.43), or average BMI (p=0.31) between the two groups.
Bolded p-value indicates statistical significance.
TSH, thyrotropin; BMI, body mass index.
Discussion
Our study demonstrated a significant improvement in the overall score after thyroid surgery using a validated OSA screening questionnaire (p<0.01). Patients in this study underwent thyroid surgery for compressive symptoms, thyroid cancer, thyroid nodular disease, goiter, and Graves' disease. Specific symptoms that significantly improved postoperatively included snoring frequency (4.1±0.2 vs. 3.2±0.2, p=0.002), how bothersome snoring was to others (0.7±0.1 vs. 0.4±0.1, p=0.004), and whether or not a patient nodded off (0.2±0.1 vs. 0.1±0.0, p=0.02). At least a 25% improvement in the score was observed in 13 patients (29%). Interestingly, age, gender, BMI, gland weight, presence of compressive symptoms, and the largest dimension of the gland were not significantly associated with whether or not patients had a significant improvement in their score (see Table 2).
OSA is typically diagnosed with polysomnography. Previous studies have found the Berlin Questionnaire responses accurately detect patients who will meet or exceed respiratory distress indices values used in diagnostic classification of the OSA syndrome (3,4,15). Thus, the Berlin Questionnaire is a useful tool in the clinic setting to screen for the presence of obstructive sleep apnea. This is the first study in the literature using the Berlin Questionnaire to identify patients at high-risk of sleep apnea before and after thyroid surgery.
Previous studies have reported improvement in symptoms of compressive symptoms after thyroidectomy. Compressive symptoms include symptoms of neck pressure, dysphagia, dyspnea, neck pain, snoring, and hoarse voice. These symptoms are attributed to compression of the goiter on the trachea or esophagus (16,17). Deegan and colleagues describe 2 patients with a large goiter and OSA. Both patients were able to come off CPAP after hemithyroidectomy (8). Many physicians consider compressive symptoms to be related only to the size of the thyroid; however, other factors such as the presence of thyroiditis may also cause these symptoms. Studies have demonstrated improvement in compressive symptoms related to Hashimoto's thyroiditis after thyroid surgery (18,19). In our current study, there was no significant difference in the percentage of patients with thyroiditis among those with ≥25% improvement versus those with <25% improvement in symptoms (p=0.88).
Interestingly, a significant difference in preoperative TSH was found between patients with ≥25% improvement in scores (1.4±1.8 mIU/L, median 0.8, and range 0.01–6.2 mIU/L) versus those with <25% improvement (2.0±1.5 mIU/L, median 1.5, and range 0.33–7.0), p=0.03. Patients with overt hypothyroidism have an increased prevalence of OSA, which is thought to be related to pharyngeal narrowing from soft tissue infiltration by mucopolysaccharides and proteins (7). However, a study by Kapur and colleagues evaluated unrecognized hypothyroidism in 336 patients undergoing polysomnography for suspected OSA (20). In their study, 5.1% had pre-existing hypothyroidism, and only 4 new cases of hypothyroidism were diagnosed, translating to an odds ratio of 1.47. Thus, the authors recommended against testing for hypothyroidism in patients with OSA. Although we found a significant difference in TSH values between patients with at least 25% improvement in scores and those with <25% improvement, both groups had an average TSH within the normal reference range.
We used the Berlin Questionnaire to identify patients at high risk of OSA before undergoing thyroid surgery. Other methods of identifying risk of OSA or tracheal compression in patients undergoing thyroidectomy include computed tomography (CT), flow–volume loops (FVLs), and polysomnography. A case series by Agrama reviewed 8 patients with euthyroid goiter with evidence of tracheal compression and moderate to severe OSA who underwent thyroidectomy. Tracheal compression was confirmed with CT and OSA with polysomnography. Polysomnography was repeated 3 months after surgery, and 7 patients had evidence of postoperative improvement in their apnea-hypopnea index (10).
FVLs have been used to demonstrate the presence of upper airway obstruction in patients with goiter (11). A case report by Meysman and colleagues used FVLs in 2 patients with goiter and demonstrated positional changes in FVL (9). Both patients demonstrated an upper airway flow limitation in the recumbent posture, but normal FVLs in the upright posture. FVLs can be a useful tool to determine the presence of positional upper airway obstruction from goiter.
In contrast to these studies, we did not limit our study to only patients with goiter, but instead screened based upon the presence of snoring symptoms. Thyroid enlargement is not the only factor that can lead to the presence of compressive symptoms, and therefore, our data are more representative of the greater population of patients with thyroid disease undergoing thyroidectomy. While we did not use objective measurements of improvement, such as formal sleep studies, we did use a well-established and validated questionnaire that was given preoperatively as well as postoperatively so that matched pair comparisons could be made. While this questionnaire is validated, the self-reporting nature of this survey is a limitation, as patients are asleep when their snoring occurs. However, most patients did have a spouse or family member with them at their pre- and postoperative visits who assisted the patient with the completion of the questionnaire. Since we do not routinely obtain CT preoperatively, we were unable to assess the degree of tracheal compression and thus determine whether or not imaging could predict who would benefit the most from thyroidectomy for symptoms of sleep apnea. Another limitation of this study was the small number of patients enrolled. However, despite the relatively small number and the mixed patient population, we did find statistically significant differences between our groups. Therefore, if we were to expand our study or to focus in on a narrower subset of patients, these differences would likely be even greater. Also, this is the largest study to date evaluating symptoms of snoring in patients undergoing thyroid surgery. By 8 weeks after surgery, most patients had resolution of their postoperative swelling, but before that time, postoperative swelling may have actually exacerbated some patient symptoms as witnessed by the rise in scores in some patients in the postoperative period.
Our study demonstrated improvement in symptoms of sleep apnea before and after thyroid surgery using the Berlin Questionnaire. While our results are interesting, further studies are needed to determine the mechanism behind this improvement and to better define which group of patients will benefit most from thyroid surgery. Evaluation for thyroid disease should be included when evaluating a patient with symptoms of obstructive sleep apnea, as symptoms of sleep apnea may improve with thyroidectomy.
Footnotes
Disclosure Statement
No competing financial interests exist for any of the authors.