
Abstract
Background:
The cribriform-morular variant of papillary thyroid carcinoma (cmvPTC) is rare. There are few if any studies of the ultrasonographic (US) features of cmvPTC. The aim of this study was to determine the characteristic US and clinical features of the cmvPTC.
Methods:
A retrospective review of the US and clinical features was performed on 18 surgically confirmed cmvPTCs in five patients who were seen at our institution between January 2000 and December 2010.
Results:
All patients were female with a mean age of 28 years (range, 19–46 years). Two patients presented with palpable lesions, and the other patients were incidentally detected during screening US. On US, the majority of nodules had well-defined, oval to round shapes, and were hypoechoic and solid without calcifications. However, 6 (33.3%) of 18 nodules did have a cystic change. The size of the lesions varied from 0.3 to 3.0 cm (mean, 1.11 cm). None of the nodules were diagnosed as malignant based on the US criteria, but all except one patient had a cytology of their thyroid nodules that was read as malignant, without revealing the subtype of their PTC. Two of the five patients had familial adenomatous polyposis (FAP), and they had bilateral multiple nodules. No metastatic lymph nodes or extrathyroidal extension were identified. To date, none of the patients has had recurrence or metastasis during their mean follow-up of 25 months after thyroidectomy.
Conclusion:
It appears that most cases of cmvPTC do not have features of malignancy on US and that they are indolent tumors as far as their clinical and histological features are concerned.
Introduction
The cytological, clinical, and pathologic features of cmvPTC have been the subject of many reports. In contrast, there is little published information regarding the ultrasonographic (US) features of cmvPTC. The purpose of this study was to determine and record the characteristic imaging and clinical features of cmvPTC.
Methods
Patients
The Institutional Review Board approved this retrospective study, and the need for informed consent was waived. The medical record database at our institution was queried for patients diagnosed with cmvPTC between January 2000 and December 2010. Five female patients (age range, 19–46 years; mean age, 27.6 years) with 18 nodules were diagnosed with cmvPTC based on the histopathological diagnoses made after thyroid surgery. The sonographic findings of these thyroid nodules were retrospectively reviewed, and clinical information was obtained from the medical records.
Ultrasonography
Experienced radiologists scanned the thyroid gland with HDI 5000, or iU22 scanners (Philips Medical Systems, Bothell, WA) equipped with a commercially available 7- to 12-MHz linear transducer. A retrospective review of the US images was performed in consensus by two radiologists (J.H.S. and B.K.H.) with 7 and 12 years of thyroid imaging experience, respectively. They determined the US characteristics of nodules, including the shape (ovoid to round, taller-than-wide, or irregular), margin (circumscribed, spiculated, or ill-defined), echogenicity (markedly hypoechoic when a nodule is hypoechoic relative to the adjacent strap muscle, hypoechoic when a nodule has the same echogenicity as that of the strap muscle, mildly hypoechoic when a nodule is hypoechoic relative to the thyroid parenchyma, and is echogenic relative to the strap muscle or isoechoic when a nodule has the same echogenicity as that of the thyroid parenchyma), echotexure (homogeneous or heterogeneous), presence of a hypoechoic halo (thin rim of decreased echogenicity surrounding the nodule), calcifications, or cystic change. The size of the nodules was recorded according to previous US reports. Color Doppler imaging was not routinely used. US contrast media was not used in the study.
The radiologists made a final diagnosis for each nodule as being malignant, indeterminate, or benign based on widely accepted US criteria for a malignancy. US characteristics of a malignant finding were defined as a taller-than-wide shape with a spiculated margin, marked hypoechogenicity, and the presence of microcalcifications or macrocalcifications (9,10). The lesion was diagnosed as malignant if at least one of these findings was present. The inclusion criteria for a benign nodule included cyst, predominantly cystic nodule (≥90% cystic), and a spongiform (or honeycomb) nodule. Ultrasonographically indeterminate nodules were defined as having neither benign nor malignant features.
Cytopathology
All five patients underwent a US-guided fine-needle aspiration (US-FNA). US-FNAs were performed by one of the six experienced radiologists using 23-gauge needles with or without local anesthesia. The aspirates were expressed onto frosted-end glass slides and then immediately fixed in 95% alcohol and stained with hematoxylin and eosin and the Papanicolaou stain. The final results were determined on the basis of the cytology and pathology reports. The number of nodules was ascertained based on the lesions that were seen on US images being correlated with the pathology findings.
Results
Clinical and imaging features are charted in Tables 1 and 2. Two patients presented with a palpable mass or neck swelling. The other nodules were detected during screening US in one patient with FAP, one patient with breast cancer, and one patient without a remarkable medical or family history.
FNA, fine-needle aspiration; FAP, familial adenomatous polyposis; F, female; PTC, papillary thyroid carcinoma; TT, total thyroidectomy; CND, central neck dissection; Rt, right; Lt, left.
All specimens were found to have circumscribed margins.
All specimens were heterogeneous in echotexture.
US, ultrasonographic; Bilat, bilateral; Calc., calcification; Indet, indeterminate.
Two of the five patients also had FAP. The APC (adenomatous polyposis coli) gene mutation was identified in one of the two patients. Another patient with FAP refused mutational analysis of the APC gene because her family illness had been recognized to her satisfaction. The remaining three patients were sporadic FAP; one was negative for the APC mutation and two did not have an APC gene analysis, but they had no family history of polyposis.
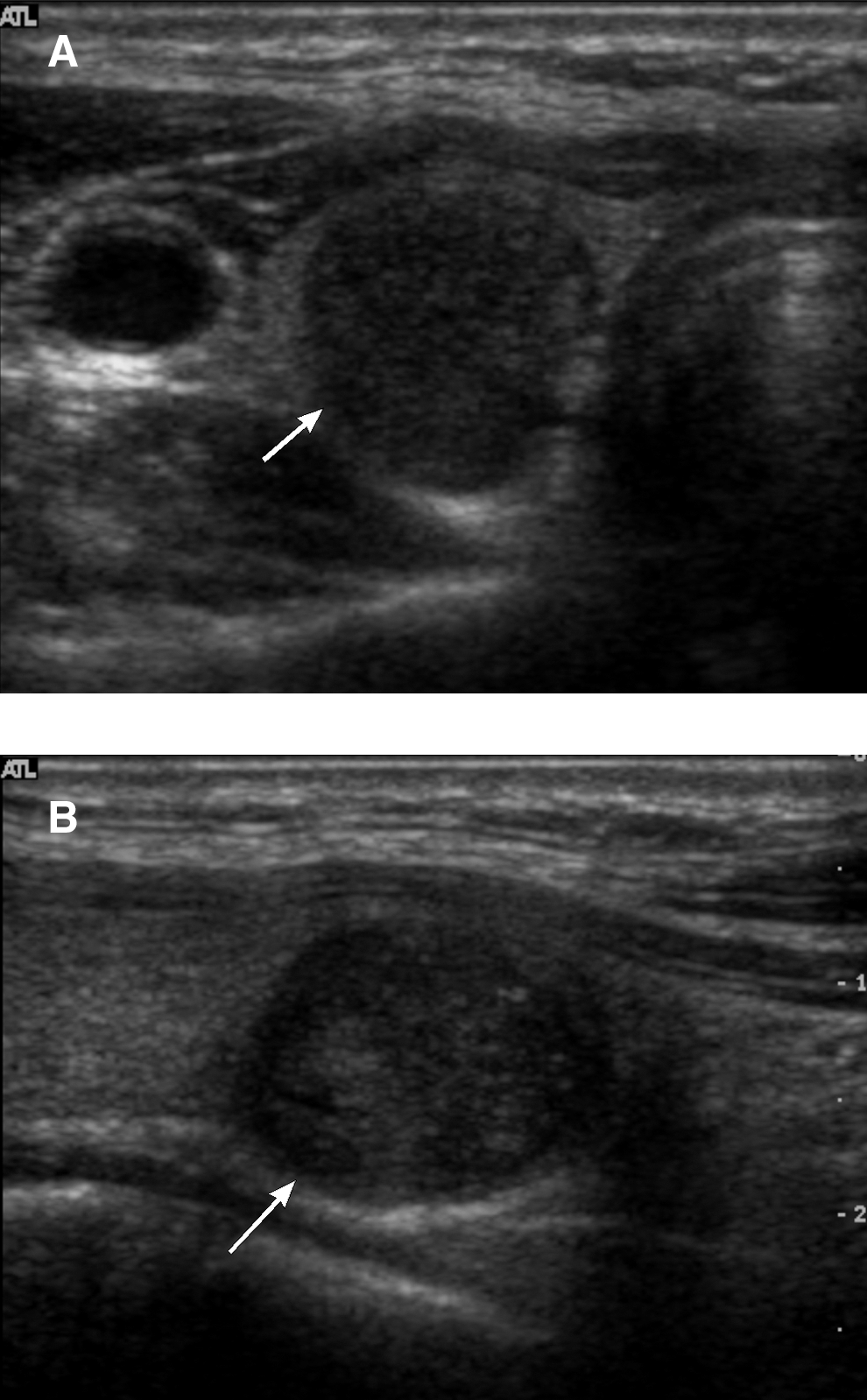
The size of the lesions varied from 0.3 to 3.0 cm (mean, 1.11 cm). The most common US features of cmvPTC were solid (17/18), oval to round (18/18), circumscribed (18/18), hypoechoic (18/18), heterogeneous (17/18), no hypoechoic halo (17/18), and no calcifications (18/18) (Fig. 1). Uncommon findings included homogeneous (1/18), hypoechoic halo (1/18), and cystic change in solid nodule (5/18) (Fig. 2). A predominantly cystic nodule was found in only one case (Fig. 3). There was no case diagnosed as a malignant nodule on US, but 17 nodules (17/18) were considered as indeterminate. Only the predominantly cystic nodule (1/18) was diagnosed as a benign lesion on US.
Case 3: cmvPTC in a 30-year-old woman. Transverse

Case 2: cmvPTC in a 46-year-old woman. Transverse
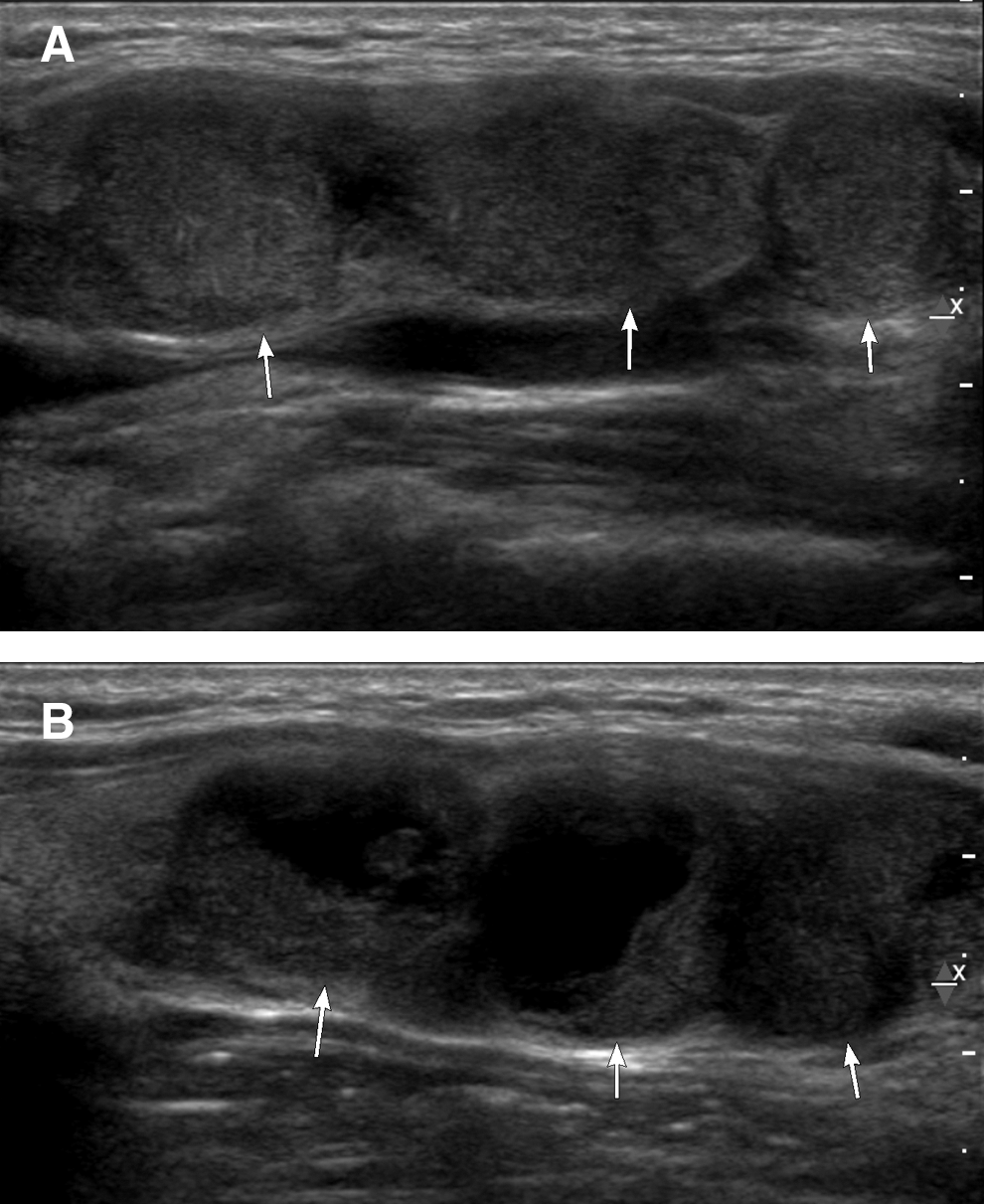
Case 4: Multifocal cmvPTC in a 23-year-old woman. Longitudinal
US-FNA was performed for 6 out of the total 18 nodules (for one nodule in four patients, and two nodules in one patient). All aspirates were adequate for cytological examination. Cytology showed PTC in five out of the six nodules and suspicious for neoplasm (PTC or thymic origin tumor) in one nodule.
A BRAF mutation analysis from aspiration specimens was performed in one patient, but a mutation was not detected.
A β-catenin protein test was performed in three of the patients. In tumor cells, β-catenin is often found in the cytoplasm and nucleus, participating in the pathway of oncogenesis. An abnormal localization and accumulation of β-catenin have been reported for various types of cancer: thyroid, colon, prostate, uterus, and liver (11). In all of the three cases, β-catenin was positive in tumor cells, with nuclear and cytoplasmic staining.
All patients underwent total thyroidectomy with central neck dissection. Tumors were located in the left lobe (n=2), the right lobe (n=1), and bilaterally (n=2). No lymph node metastases were documented histologically at the time of thyroidectomy or in the preoperative imaging. All patients were free from extrathyroidal extension on final pathology. All five patients were followed up with US and did not have recurrent disease or metastases when followed after surgery (range 12–43 months; mean period, 25 months).
Discussion
The results of this study suggest that cmvPTC usually does not meet the currently accepted US criteria for a thyroid malignancy, especially PTC. However, indeterminate US features in a nodule larger than 1 cm mandate FNA to exclude malignancy. The most common US features of cmvPTC were oval, circumscribed, heterogeneous, hypoechoic solid nodule(s) without a hypoechoic halo, or calcification. The clinical presentation of cmvPTC in our study includes early age of onset (age range, 19–46 years; mean age, 27.6 years), female predominance, and multiplicity when associated with FAP.
Although three of the five patients had incidentally found thyroid nodule(s) on screening US, it was difficult to diagnose this specific type of PTC with US features and cytology only in the preoperative state. Although the prevalence of cmvPTC is low, it should be included in the differential diagnosis in young women with a diagnosis of PTC by cytology, and well-defined hypoechoic solid nodule(s) on US. Inquiry should also be made regarding a history of colonic polyposis in these patients. After a patient is diagnosed with cmvPTC, it is critical to perform colonoscopic evaluation for early colon cancer detection and to provide genetic counseling.
About 112 patients with coexisting diagnoses of FAP and thyroid carcinoma have been reported. There is a distinct female predominance with a female-to-male ratio of 17:1, and the age of onset (mean age, 27.65 years) is relatively young (2,4). As was the case for our patients, those with FAP in combination with cmvPTC were younger than patients with sporadic cmvPTC. Since thyroid carcinoma may be the first clinical manifestation in patients who are destined to develop clinically evident FAP, diagnosed 4–12 years before the development of polyposis in 30% of the cases, ongoing screening is essential in patients with cmvPTC.
Clinical presentations of thyroid carcinoma associated with FAP other than female predominance and early age of onset are tumor multicentricity and early lymph node involvement. Fortunately, the recurrence rate after adequate resection is low, and the 5-year and 20-year survival rates of 90% and 77%, respectively, are relatively high (6,12,13). All of our five patients who had follow-up with US did not have recurrent disease or metastasis after their thyroid surgery (mean follow-up time; 25 months). Recently, Ito et al. reported, consistent with our results, that all of their 32 patients with cmvPTC did not have extrathyroidal extension and were node-negative (14). They recommended total thyroidectomy for patients with cmvPTC who also had FAP, but did not think that extensive lymph node dissection was necessary.
Our study has several limitations. The number of patients or nodules was relatively small due to the rarity of the disease. In addition, the two patients that were classified as sporadic cmvPTC did not have analyses for a mutation in the APC gene. Therefore, the possibility that they may have been predisposed to FAP cannot be ruled out.
In conclusion, even though cmvPTC is a form of thyroid cancer, it generally does not have features of malignancy seen on US. In terms of clinical and histological features, it is also relatively indolent.
Footnotes
Disclosure Statement
No competing financial interests exist.