
Abstract


Meeting Program
Wednesday, October 26, 2011
Registration Open 12:00 pm–9:00 pm
Chair: Susan Mandel
Why Lymph Nodes Matter Jennifer Sipos
Ultrasound Surveillance of the Neck Susan Mandel
Parathyroid Ultrasound Stephanie Fish
Cytology Nicole Massoll
Ultrasound Practicum 3:30 pm–5:30 pm
Preceptors: Stephanie Fish, Jennifer Sipos, Stephanie Lee, and Robert Levine
Gregory A. Brent, Richard T. Kloos, Anthony Hollenberg, and Martha Zeiger
Session Chairs: Anthony Hollenberg and Martha Zeiger
Thursday, October 27, 2011
Registration Open 6:00 am–6:00 pm
Chair: Stephanie Lee
Ultrasound Mira Milas
Dosimetry for the Clinician James Hennessey
Other Thyroid Imaging Pearls J. Woody Sistrunk
Introduction: Martha Zeiger
Speaker: Margaret Pepe
Chair: P. Reed Larsen
Mechanisms of Thyroid Hormone Action: Perspective and Application Kevin Phillips
What We Have Learned About Thyroid Hormone Receptor Action From Mouse Models Fredric Wondisford
Resistance to Thyroid Hormone: The Receptor and Beyond Samuel Refetoff
• I-131 Radiation Safety: Practice Recommendations of the ATA David Rosenthal and Charlene Edinboro
• Treatment of Hypothyroidism and Hyperthyroidism in Children Catherine Dinauer
• Role of Deiodinases Brian Kim
• Cofactors in Thyroid Hormone Receptor Action Ronald Cohen
Chairs: Martha Zeiger and Cheryl Ann Fassler
Abstracts # 1, 2, 3 and 4
Chairs: Anthony Hollenberg and Christine Spitzweg
Abstracts # 5, 6, 7 and 8
Introduction: Frances Carr
Navigating the “Club”—Mentors are the Key to Moving Ahead Honey Reddi
(all meeting attendees are welcome to attend and bring their own lunch)
Introduction: Paul Ladenson
The Medical Treatment of Hyperthyroidism: Past, Present, and Future David S. Cooper
Chairs: Anne Cappola and Emad Kandil
Abstracts # 9, 10, 11 and 12
Chairs: Frances E. Carr and Sissy M. Jhiang
Abstracts # 13, 14, 15 and 16
Chair: Patrizio Caturegli
• Induction of Antigen-Specific Tolerance in Autoimmune Thyroiditis Leonard Moise
• Modeling BRaf-Dependent Thyroid Cancer in the Mouse David McFadden
• Defining the Immune Response to Papillary Thyroid Cancer: Regulatory T Cells, T Cell Exhaustion and Disease Jena French
Chair: Gilbert Cote
• MicroRNAs Marina Nikiforova
• Gene Expression or Single Cell Arrays Thomas Fahey
• Epigenetics, SNPs, Splice Variants, Mutations, etc. Christopher Umbricht
• New Approaches to Thyroid Surgery Julie Ann Sosa
• Pediatric Thyroid Cancer Andrew Bauer
• Thyroid Hormone Transporters Heike Heuer
(for ATA Active members only)
Friday, October 28, 2011
Registration Open 6:00 am–6:00 pm
Chair: Richard Kloos
Molecular Diagnosis of Medullary Thyroid Cancer Gilbert Cote
Surgery for Medullary Thyroid Cancer Douglas Evans
Novel Drug Therapies Douglas Ball
Introduction: R. Michael Tuttle
Speaker: Pat Zanzonico
Chair: Sylvia Asa
• Challenging Thyroid FNA: Indeterminate Lesions and the Role of Ancillary Tools in Patient Management Scott Boerner
• Controversies in Thyroid Pathology: Follicular-Patterned Lesions Virginia LiVolsi
• Role of Molecular Diagnostics in Thyroid Pathology: Practical or Esoteric? Jennifer Hunt
Chair: Frances Carr
• Endocrine Disruption of Vertebrate Development: Lessons from Amphibian Metamorphosis Yun-Bo Shi
• Disruption of Cytoplasmic Signaling by TR Beta Impairs Synapse Development in Mouse Hippocampus David Armstrong
• Pesticide Exposure Is Linked to Thyroid Disease in Women Whitney Goldner
• Surgical Management of DTC Lisa Orloff
• The Role of the Subspecialist in the Patient-Centered Medical Home Carol Greenlee
• Thyroiditis Mary Samuels
• Review of the Literature on Molecular Studies in Thyroid Nodule Diagnosis Bryan Haugen
Chair: Barry Inabnet
• Safe Implementation of New Technology in the Operating Room Nancy Perrier
• Video of a Transaxillary Thyroidectomy Emad Kandil
• Overview of Robotic Thyroidectomies Performed Around the World Ronald Kuppersmith
Chair: Mingzhao Xing
• Novel Aspects of PI3K Signaling in Thyroid Transformation Antonio Di Cristofano
• BRAF and Thyroid Cancer Sareh Parangi
• PAX8-PPARgamma Fusion Protein in Thyroid Cancer Ronald Koenig
Introduction: Jerome Hershman
Thyroid Hormone Action: Mechanisms of Specificity and Crosstalk With Other Signaling Pathways Gregory A. Brent
Chairs: Kathryn G. Schuff and John A. Copland
Abstracts # 92, 93, 94, 95, 96 and 97
Chairs: Francesco S. Celi and Yuri E. Nikiforov
Abstract #98, 99, 100, 101, 102 and 103
Chair: Jorge Mestman
Hormone in Development Joanne Rovet
Clinical Trials in Pregnancy John Lazarus
Guidelines Debate: Leslie De Groot, Alex Stagnaro-Green, and Scott Sullivan
Saturday, October 29, 2011
Chair: Orlo Clark
Pros and Cons of Prophylactic Central Neck Dissection for Well Differentiated Thyroid Cancer Gerard Doherty vs. Gregory Randolph
Management of Recurrent Differentiated Thyroid Cancer Kenneth Burman
Management of Advanced Differentiated Thyroid Cancer Ashok Shaha
Speaker: Announced Onsite During Lecture
Chair: Terry F. Davies
• Autoimmunity and the TSH Receptor Sandra McLachlan
• Defining the Three Dimensional Epitopes of Thyroid Stimulating Antibodies Terry F. Davies
• Graves' Ophthalmopathy Terry Smith
Chair: Anne Cappola
• Genetic Determinants of Thyroid Function Robin Peeters
• Genetic and Epigenetic Mechanisms in Thyroid AutoimmunityYaron Tomer
• Genetic Variants in Pathogenesis of Thyroid Cancer James Fagin
Chairs: Elizabeth N. Pearce and Sara I. Pai
Short Call (SC) Abstracts 1, 2, 3, 4, 5 and 6
Introduction: Alan Farwell
Speaker: E. Chester Ridgway
Chairs: Sylvia L. Asa and Eren Berber
Abstracts # 174, 175, 176, 177, 178 and 179
Chairs: Basil Rapoport and Salvatore Benvenga
Abstracts # 180, 181, 182, 183, 184 and 185
Chair: Gerard Burrow
• Will Efforts to Reduce Dietary Sodium Jeopardize Iodized Salt Programs to Control Iodine Deficiency? Michael Zimmermann
• KI Distribution Around Nuclear Facilities Elizabeth Pearce
• Iodine Intake in Infants Angela Leung
Chair: Paul Ladenson
• How Thyroid Hormones Regulate Metabolism V. Krishna Chatterjee
• Development of Novel Thyroid Analogues to Treat Metabolic Disorders Thomas Scanlan
• Treatment of Thyroid Disease, Obesity and MetabolismFrancesco Celi
Introduction: Joel Ehrenkranz
Speaker: Valerie Anne Galton
• Pharmacological and Nonpharmacological Aspects of T4 Malabsorption Salvatore Benvenga
• Surgical Management of Advanced Thyroid Cancer Ralph Tufano
• Brown Fat Antonio Bianco
• Iodine Nutrition and the Impact of Environmental Toxicants, Especially Perchlorate in Turkey Aysel Özpınar
Sunday, October 30, 2011
Chair: Gregory Brent
ATA Anaplastic Thyroid Cancer Guidelines Robert Smallridge
ATA/AACE Hyperthyroidism Guidelines Rebecca Bahn
Pazopanib Trial for Differentiated Thyroid Cancers Keith Bible
E 7080 Trial for Differentiated Thyroid Cancer Maria Cabanillas
Thursday, October 27, 2011
Pediatrics, The Hospital for Sick Children, Toronto, ON, Canada
Thyroid and Development Thursday Oral Clinical 11:45 AM
The hippocampus is critically involved in remembering one's own personal memories, known as autobiographical memory (AM), and it is particularly vulnerable to early thyroid hormone (TH) deficiency. Despite animal evidence showing enhanced synaptic activity in hippocampi of rats exposed to maternal hypothyroidism during pregnancy (Gilbert and Sui, 2006), no study has as yet investigated hippocampal activation during AM retrieval in offspring of hypothyroid women (HYPO). This study sought to determine whether severity of maternal TH insufficiency during pregnancy predicts hippocampal activation during an AM retrieval task in their children.
Participants were 34 right-handed children aged 9 to 11 years, 15 HYPO and 19 typically developing controls. All underwent a 1-hour MRI session in a 1.5 T magnet that included fMRI testing. The fMRI paradigm included an individually programmed AM retrieval task containing yes/no questions about each child's past personal memories for specific events and a control condition containing yes/no questions assessing general semantic memory facts. The critical contrast was the difference in activations between AM and semantic fact retrieval conditions. For this study, multiple regressions were conducted in the HYPO group only using Statistical Parametric Mapping-5 software with a region-of-interest analysis (within the hippocampus), small volume correction at p<.10 uncorrected, and 5 contiguously active voxels restriction.
After controlling for total hippocampal volumes and accuracy, maternal TSH levels during first trimester of pregnancy significantly predicted hippocampal activations during AM versus fact retrieval. Higher maternal first-trimester TSH values significantly predicted greater left (p=.002) and greater right hippocampus activity (p=.042).
These results suggest that the hippocampi of children exposed to more severe maternal TH deficiency during early pregnancy worked harder and compensated more when later recalling past personal memories. These results provide critical new insight into the long-term specific effects of maternal TH deficiency on child hippocampal functioning and highlight the importance of maternal TH for normal hippocampal development.
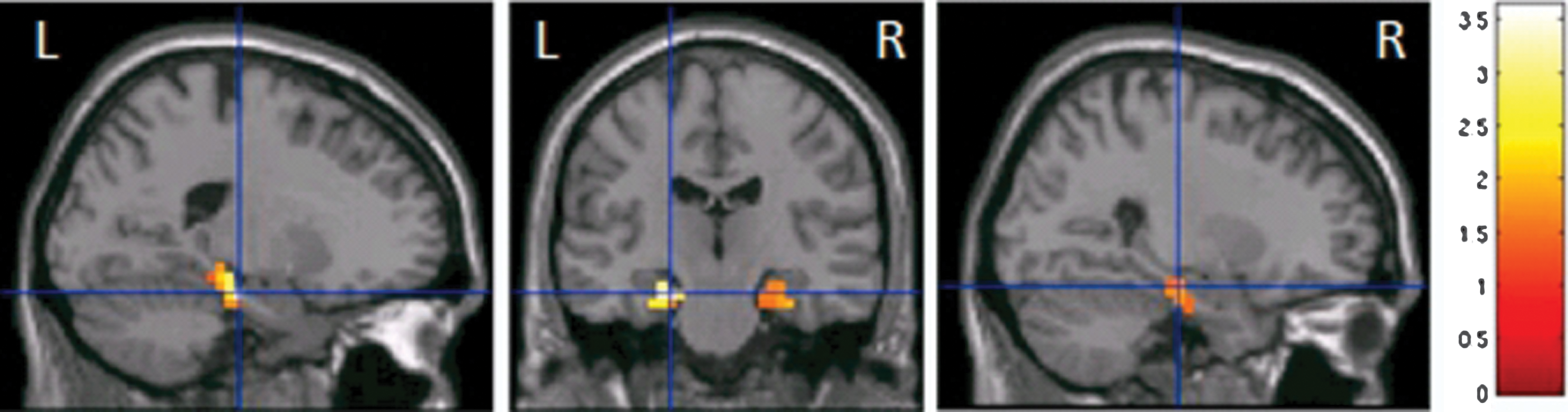
Significant correlations between first trimester maternal TSH levels and activations for autobiographical memory recall in child.
Thyroid Imaging Thursday Oral Clinical 12:00 PM
Benign-appearing enlarged cervical lymph nodes (ECLN)>1cm are easy to assess during an ultrasonographic evaluation for suspicious thyroid nodules, but their clinical significance regarding the thyroid cancer risk is not clear. We hypothesize that if ECLN are identified on ultrasound there is a greater chance of the patient having thyroid cancer.
The charts of 257 consecutive patients' referred for surgical evaluation of suspicious thyroid nodules and underwent comprehensive neck ultrasound were obtained. Demographics, pathology and operative reports were reviewed.
257 consecutive patients were included in the analysis. The mean age (SD) was 49.9 years±14.04. 192 patients were female (75%). Of the 257 patients that underwent ultrasounds, only 198 required surgical intervention. Fifty-nine of the patients were evaluated and did not meet the criteria for thyroidectomy. Of these 59 patients, 7 (11.8%) had ECLN identified on comprehensive neck ultrasound. Only patients that had postoperative pathology reports of papillary thyroid cancer or benign thyroid pathology were included in the study, which was a total of 198 patients, 46 of which had papillary cancer on postoperative pathology report. ECLN was found in 30 of the surgical patients. ECLN was present in 18 (39.1%) of the thyroid cancer patients compared to only 12 (8.4%) of patients with benign thyroid pathology (p<0.001). The presence of ECLN on ultrasound had a PPV of 60% and a NPV of 82.4% in predicting thyroid cancer with a sensitivity of 39.1% and a specificity of 91.6%.
Assessment of ECLN by ultrasound is feasible and should be studied further to determine the exact clinical and pathologic implications of ECLN found on preoperative ultrasound. In our cohort the presence of ECLN increases the predictive value in diagnosing thyroid cancer in suspicious thyroid nodules.
Oncology, Eisai Inc, Woodcliff Lake, NJ
Thyroid Cancer Thursday Oral Clinical 12:15 PM
Lenvatinib is an oral tyrosine kinase inhibitor targeting VEGFR1–3, FGFR1–4, RET, KIT and PDGFRβ. In phase I studies of lenvatinib partial responses (PR) were observed in thyroid as well as melanoma, endometrial, and renal cancers.
Between Oct 2, 2008 and Feb 5, 2010, patients (pts) with advanced, RAI-refractory DTC (papillary, follicular or Hurthle cell) and disease progression demonstrated by RECIST during the prior 12 months were enrolled. Pts may have received prior VEGFR targeted therapy. Pts were treated until disease progression or development of unmanageable toxicities. Primary end point was Response Rate (RR) by RECIST.
58 pts were enrolled (med age: 62; M: 59%, F: 41%) and confirmed PRs were observed in 50% (95% CI: 37–63) based on investigator assessment and 45% by independent radiographic review performed with 9 mo minimum follow-up. Correlation of clinical outcomes (RR, maximum tumor shrinkage (MTS) and PFS) with pharmacokinetic parameters, circulating cytokine and angiogenic factors (CAFs) and tumor gene mutation status were also performed. Lenvatinib concentration 2 hours post-treatment (Cmax) 29 days post-therapy weakly correlated with tumor shrinkage (r=−0.21, p=0.15). A panel of 43 serum CAFs was evaluated in serum samples collected pre-treatment (baseline), 8 and 36 days post-treatment. Lower baseline angiopoietin-2 (ANG-2) levels (r=0.309, p=0.033) and increase in FGF-2 (r=−0.347, p=0.021) and IL-10 (r=−0.38, p=0.020) levels 8 days post-treatment correlated with greater tumor shrinkage. A panel of 33 genes with a total of 443 mutations was examined in archival tumor tissue obtained from 23 pts. Mutations in 10 different genes in 16 pts were identified. Mutations in Ras (N- or K-) were found to be significantly associated with MTS (p=0.022) and RR (p=0.007). Ras mutation was also associated with longer PFS (p=0.027, HR=0.20 (CI:0.04–0.95)).
Tumor gene mutation status and serum CAF profiling may be informative in identifying patients who achieve greater tumor shrinkage and prolonged PFS with lenvatinib treatment. Further examination of these associations will be undertaken in an ongoing Phase III study of lenvatinib in patients with RAI-refractory DTC.
Department of Nuclear Medicine and Endocrinology, Institut de Cancérologie Gustave Roussy, Villejuif, France
Thyroid Cancer Thursday Oral Clinical 12:30 PM
This study supported only by the French National Institut du Cancer compared four strategies of postoperative radioiodine ablation (RAI).
This randomized, controlled, phase III trial performed in 24 French centers compared 4 strategies for postoperative RAI in a 2*2 factorial design: each strategy combined a TSH stimulation method (either thyroid hormone withdrawal (THW) or rhTSH (Thyrogen®, Genzyme)) and an activity of 131I (either 1.1 GBq or 3.7GBq). Study patients met the following criteria: age >18 yrs; total thyroidectomy for differentiated thyroid carcinoma performed 30–120 days before, treatment with LT4 for at least 30 days; TNM stage pT1<1cm, N1, pT1>1cm (any N) or pT2, N0; absence of distant metastasis. The primary endpoint was the rate of ablation at 6–10 months, which was assessed with neck-US and rhTSH-stimulated Tg determination (or whole-body scan in the presence of Tg antibodies). The four strategies were compared using an equivalence framework, with two-side α=0.05.
752 patients with written informed consent were included between April 2007 and February 2010: 79% were female, mean age was 49 years, 91% had papillary cancer; 30% of tumors were pT1N0, 18% were pT1N1, 39% were pT1,Nx and 12% were pT2,N0. 65 patients were excluded from the final analysis: 27 patients for persistent disease at ablation, 20 for consent withdrawal and 18 for incomplete follow-up. Among the remaining 687 patients, neck-US was normal in 655 patients (95%), stimulated Tg level was ≤1.0 ng/mL in 652 (95%) and thyroid ablation was complete in 633 patients (92%). The ablation rate was equivalent both for the I31I activity (difference 1.1 GBq / 3.7 GBq=−2.1%, IC=[−5.4%; 1.3%]) and for the TSH stimulation method (difference rhTSH/THW=−1.5%, IC=[−4.9%; 1.9%]). Among the other 54 patients, 18 had persistent disease, 25 had a normal subsequent work-up and 11 are still being followed.
These results validated the use of rhTSH and 1.1 GBq for ablation in low-risk patients.
Endocrinology, MSKCC, New York, NY
Thyroid Cancer Thursday Oral Basic 11:45 AM
A subpopulation of patients with BRAFV600E derived PTCs progress to more advanced stage disease, including to metastatic poorly differentiated thyroid cancers (PDTC) and anaplastic thyroid cancers. Understanding the biological processes that are associated with more aggressive disease in BRAFV600E PTCs is important for the development of successful therapeutic strategies in these patients.
We used models of BrafV600E activation in the thyroids of transgenic mice in combination with genetic approaches to deplete tumor-associated macrophages (TAMs) in order to examine the functional role of TAMs on PTC initiation and progression.
During acute activation of Braf in thyroids, expression of the macrophage chemoattractants colony stimulating factor-1 and CCL-2 is increased >1000-fold and 4-fold, respectively. This is accompanied by a dense infiltration of TAMs, which interdigitate with cancer-associated myofibroblasts (CAMs) to form a dense stroma within and surrounding the thyroid. Using diphtheria toxin receptor (DTR) targeted CCR2 mice (CCR2-DTR), we selectively depleted TAMs in PTCs with diphtheria toxin (DT). This was accompanied by a reduction in tumor size, and a more well-differentiated tumor phenotype with a lower mitotic index. Moreover, we observed a significant reduction in stromal CAM density. During PTC progression in Tg-braf/CCR2-DTR mice, PTCs are densely infiltrated with TAMs, are invasive, develop prominent tall cells and foci of PDTC. Following treatment with DT, TAM-depleted PTCs were 1) significantly smaller [0.018 g vs. 0.033 g in controls, p=0.0001]; 2) had fewer mitotic cells [0.54% vs. 0.77%/mm2 , p=0.04]; 3) had decreased total tumor cell volume 4) had a near absence of tall cells with less prominent papillae and more colloid and 5) had fewer foci of PDTC.
In summary, TAMs play key roles in PTC initiation and on PTC progression. To our knowledge, this is the first demonstration of a functional link between TAMs and CAM recruitment, activation and/or proliferation in any cancer type. Moreover, the impact of TAM depletion on tumor maintenance and progression identifies TAMs as a potentially important therapeutic target in patients with advanced, radioiodine refractory PTCs.
School of Clinical and Experimental Medicine, University of Birmingham, Birmingham, United Kingdom
Thyroid Hormone Metabolism and Regulation Thursday Oral 12:00 PM
Within the basolateral membrane of thyroid follicular epithelial cells, two transporter proteins are important for thyroid hormone (TH) biosynthesis. Initially, sodium iodide symporter (NIS) delivers iodide from the bloodstream into the thyroid and, following biosynthesis, monocarboxylate transporter 8 (MCT8) mediates secretion of TH from the thyroid gland. NIS-mediated radioiodine uptake is also critical in the treatment of thyroid tumours and metastases. We have previously demonstrated that PTTG-binding factor (PBF), a proto-oncogene upregulated in thyroid cancer, binds NIS and modulates its subcellular localisation, impacting on its ability to uptake iodide. We have now investigated a potential relationship between PBF and MCT8.
Protein interactions were assessed using GST-pulldown and co-immunoprecipitation assays. Immunofluorescent studies were performed both on cell lines and frozen sections of mouse thyroid gland. MCT8 expression levels were quantified using real-time PCR and Western blot analysis.
A physical interaction between PBF and MCT8 was demonstrated in vitro. Further, immunofluorescent studies demonstrated a shift in subcellular localisation, with increased staining of MCT8 within intracellular vesicles following PBF over-expression in vitro. Within these vesicles, colocalisation between PBF and MCT8 was observed. A significant reduction in the amount of MCT8 at the plasma membrane was determined by cell surface biotinylation assays. Colocalisation between PBF and MCT8 was also observed in vivo in a mouse model of thyroid-specific PBF over-expression (PBF-Tg). Thyroidal MCT8 mRNA and protein expression were comparable with wild type mice. PBF-Tg mice developed significantly enlarged thyroid glands with both increased follicular diameter and thyroidal TH levels. Interestingly MCT8-KO mice also share this phenotype.
These data show that PBF binds and alters the subcellular localisation of MCT8. In vivo evidence suggests this may result in reduced TH secretion via MCT8. Overall, these studies identify PBF as a novel interacting partner of MCT8 and, alongside NIS repression, indicate PBF may regulate TH biosynthesis and secretion.
Medicine, Intermountain Healthcare, Murray, UT
Thyroid Hormone Action Thursday Oral Basic 12:15 PM
Animal and human studies conducted between 1923 and 1930 showed that thyroxine affects circulating cholesterol levels. More recent experiments have demonstrated that the effects of both T3 and thyroid hormone analogues on lipid metabolism are mediated by the nuclear receptor TR β. Several observations also suggest that the thyroid-mediated reduction in cholesterol involves the LDL receptor. 3,5 diiodo thyronine (T2), a naturally occurring iodothyronine, lowers plasma cholesterol levels in animals and humans; however T2's site of action is thought to be non-genomic.
We undertook a series of studies in wild type and Ldlr−/− mice to characterize the lipid-lowering effects of T2, define the role of the LDL receptor as a mediator of thyroid hormone effects on lipids, and compare the effects of T2 to those of T3 on lipid metabolism. Adult mice were placed on a western diet one week prior to receiving therapy. Animals then received 0.75 mg/kg T3, 12.5 mg/kg T2 or by oral gavage for 1 week after which the animals were sacrificed. Plasma and lipoprotein cholesterol and triglyceride levels were determine before and after treatment.
Administering T2 and T3 led to significant (∼70%) and parallel reductions in circulating cholesterol in Ldlr-/- and wild type animals. The reduction in cholesterol was associated with a reduction in both apoB100- and apoB48- containing lipoproteins, a result that suggests no change in apoB RNA editing. This was due almost exclusively to a reduction in VLDL and LDL; HDL levels did not change significantly. The decrease in circulating cholesterol levels was not associated with increased protein or mRNA expression of the alternative hepatic lipoprotein receptors: LDL receptor related protein (LRP1), VLDL receptor, scavenger receptor-B1, or syndecan 1, or increased expression of either hepatic lipase or lipoprotein lipase.
T2 and T3 decrease serum cholesterol and plasma apoB-lipoprotein levels through a mechanism which does not involve the LDL receptor pathway. Targeting this pathway with thyroid hormone agonists could represent a new treatment approach for patients with genetic defects in the LDL receptor.
Molecular, Cellular & Developmental Biology, The Ohio State University, Columbus, OH
Thyroid Cancer Thursday Oral Basic 12:30 PM
PI3K/Akt activation, including copy gain and activating mutations in the PIK3CA gene or PTEN inactivating mutations, is associated with benign follicular thyroid adenoma (FTA) and malignant follicular thyroid carcinoma (FTC). We and others have shown that PI3K and Akt1/2 inhibitors increase Na+/I- Symporter (NIS)-mediated radioactive iodide (RAI) uptake in cultured thyroid cells. In this study, we examined NIS-mediated RAI influx and retention in thyroids of mouse models manifesting aberrant PI3K/Akt signaling pathways.
Thyroidal RAI accumulation, shown as percentage of injected dose (%ID), was acquired by SPECT imaging at 1 hr (RAI influx) and at 24 hr (RAI retention) post-injection of Na123I in mice. Thyroid volume was measured by ultrasound imaging and further calibrated by visual volumetric measurements of excised thyroid/trachea. RAI accumulation per anatomic unit was shown as %ID/mm3. RAI retention index was %ID at t24 divided by %ID at t1.
Thyroid tumors of 2 month old TPO-Cre; PTENL/L mice (a mouse model of FTA) had reduced RAI influx (0.42±0.20%ID/mm3 vs. 0.70±0.18%ID/mm3, p=0.052) and reduced RAI retention index (1.78±0.43 vs. 3.68±1.29, p<0.05) as compared to PTENL/L littermates. Thyroid tumors of 9 month old TPO-Cre; PTENL/L mice had a greater extent of reduction in RAI influx (0.10±0.02%ID/mm3 vs. 0.25±0.07%ID/mm3, p<0.01) and RAI retention index (4.13±2.82 vs. 20.46±3.36, p<0.05), showing temporal dynamics of RAI influx and RAI retention with age and/or accumulated mutations. Thyroid tumors of 3–4 month old TRβPV/PV mice (a mouse model of FTC, in which both PI3K activity and TSH levels are increased) also had a mild reduction in RAI retention. However, thyroid tumors of 3–4 month old TRβPV/PV; Akt1-/- mice had increased RAI influx (4.08%ID/mm3 vs. 1.52±1.13%ID/mm3) and RAI retention index (3.28 vs. 2.07±0.78), compared to same age of TRβPV/PV mice.
This is the first report demonstrating that PI3K/Akt pathway inhibits thyroidal iodide influx and retention in living mouse models. The data suggests pharmacological inhibition of PI3K/Akt may have clinical benefit in increasing iodide influx and retention in thyroid cancer patients treated with 131I.
Dept of Science and Medico-Surgical Biotechnologies, “Sapienza” University of Rome, Latina, Italy
Disorders of Thyroid Function Thursday Oral Clinical 2:15 PM
An efficient absorption of oral T4 is key to optimal and individually-tailored thyroxine treatment. However, a number of patients fail to attain the proper TSH level, requiring both additional diagnostic monitoring and often larger doses of levothyroxine sodium. Aim of this study has been to analyze the impact of occult gastrointestinal disorder on T4 treatment.
A total of 2018 sequentially examined adult patients (16–60 yrs) were treated with oral sodium levothyroxine (one brand) and followed for at least 24 months. All patients agreed to take thyroxine in fasting conditions, waiting at least one hour before eating or drinking. Patients who were pregnant, who used cosmetics, food and substances containing iodine or drugs interfering with T4 absorption were excluded.
The expected serum TSH has been obtained in the “responder” patients at a median thyroxine dose of 1.54 μg/kg/day in semi-suppressive mode(SM)(TSH=0.1–0.4 mU/l) and 1.31 μg/kg/day in replacement mode(RM)(TSH=0.4–2.5 mU/l). However, 335 patients (17%) still failed to reach the expected serum TSH. Once excluded the subjects still under investigation and those with poor compliance, 245 patients (12.1%; 222F/ 23M) were classified as “poor-responder”. These underwent an algorithm to diagnose gastrointestinal disorders. A gastric disease has been diagnosed in 152 patients (62%) (H.pylori infection or autoimmune gastritis), while an intestinal disorder (celiac or parasitic disease, lactose intolerance etc) has been detected in 47 patients (19%). The cause of malabsorption remained unknown in 46 patients. In patients with gastric disorders, the median therapeutic T4 dose required was increased by 30%(in RM) and by 37%(in SM)(1.73 vs 1.31μg/kg/day and 2.14 vs 1.54μg/kg/day). In patients with intestinal disorders, the median T4 dose was similarly higher (1.85 and 2.0μg/kg/day) than in reference group (+39%in RM and +28%in SM). Upon treatment of gastrointestinal disorders, the effect was reversed in 1/3 of patients.
We observed: •malabsorption or pseudomalabsorption of oral thyroxine in 1 out 5 treated patients; •most of T4 treatment failures were due to defined gastrointestinal disorders; •T4 malabsorption was reversible in about 1/3 of these patients.
Division of Endocrinology, Stanford University School of Medicine, Stanford, CA
Disorders of Thyroid Function Thursday Oral Clinical 2:30 PM
Hypothyroidism in pregnancy can lead to adverse maternal and fetal outcomes. Although screening of high risk women is advocated, universal screening for autoimmune thyroid disease (AITD) remains controversial. The objective of this study was to compare the cost-effectiveness of universal screening of pregnant women for AITD with screening of high risk women only and with no screening.
We developed a state-transition Markov model to compare the incremental cost per quality-adjusted life-year (QALY) between universal screening, high risk screening, and no screening. Screening occurred in the 1st trimester of pregnancy with anti-thyroid peroxidase (anti-TPO) antibodies and thyroid-stimulating hormone (TSH). It was followed by further testing if the screen was positive and treatment of hypothyroid women. The model accounts for adverse outcomes of miscarriage, preterm labor, postpartum thyroiditis, and progression to overt hypothyroidism. We performed a lifetime analysis taking a societal perspective. Using data from the literature, we made base-case assumptions regarding age of pregnancy (25 years), disease prevalence (11.2% for anti-TPO antibody positivity), cost of screening ($21 for anti-TPO and $25 for TSH), annual levothyroxine cost ($170) and other variables. We used data from randomized controlled trials to obtain probabilities for adverse obstetrical outcomes. All variables were varied in sensitivity analyses.
Universal screening was cost-effective relative to risk-based screening, with an incremental cost-effectiveness of $7,258/QALY. Risk-based and universal screening were both more cost-effective relative to no screening, with incremental cost-effectiveness ratios of $6,753/QALY and $7,119/QALY respectively. Screening remained cost-effective across a wide range of parameters varied, and even when we assumed that only overt hypothyroidism had adverse obstetrical outcomes. When we assumed that untreated maternal hypothyroidism decreased child IQ, while levothyroxine treatment prevented this, universal screening was cost-saving.
Universal screening of pregnant women in the 1st trimester for AITD is cost-effective not only compared with no screening, but also compared with screening of high risk women.
Screening consisted of TSH and anti-TPO antibodies. QALY: quality-adjusted life year, C-E: cost-effectiveness.
Department of Medicine, University of Manitoba, Winnipeg, MB, Canada
Iodine Uptake and Metabolism Thursday Oral Clinical 2:45 PM
Increased thyroid hormone requirements during pregnancy rely heavily upon adequate maternal intake of dietary iodine. Studies in regions considered iodine sufficient, including the United States, have shown median urine iodine levels below the World Health Organization recommended range for pregnancy (150 to 249 ug/L). Iodine deficiency during pregnancy can lead to goiter and hypothyroidism and is associated with neurologic and intellectual impairment in the fetus, the extreme form of which is cretinism. Little is known about the current status of iodine nutrition in Canada. OBJECTIVE: To evaluate the status of iodine nutrition in a sample of pregnant women presenting for routine antenatal care, by determining the median urine iodine concentration (UIC) of this population.
A cross-sectional, observational study of 150 pregnant patients in the ambulatory obstetrical department at Mount Sinai Hospital in Toronto, Ontario, Canada. Each participant provided a spot urine sample; urine iodine concentration was measured by spectrophotometry using a modification of the method of Benotti et al.
150 pregnant women (mean age 33.8±4.4SD years, mean gestational age 29.0±8.1SD weeks) were recruited from 4 low-risk antenatal clinics. The median UIC was 227.1 ug/L; values ranged from 25.9 ug/L to 1812.7 ug/L. 42 (28%) women had urinary iodine levels below 150 ug/L and 6 (4%) were below 50 ug/L, consistent with iodine deficiency. After excluding the 8 women with a UIC above 800 ug/L due to the possibility of unrecognized contamination, the median UIC was 221.3 ug/L.
The median UIC of this population is within the recommended range for pregnancy, suggesting adequate iodine nutrition. The lower rates of iodine deficiency compared to those previously reported by U.S. centers may be due to universal salt iodization in Canada and/or other dietary and lifestyle factors. The status of iodine nutrition during pregnancy requires continued surveillance in Toronto and merits investigation in other regions of Canada.
Section of Endocrinology, Diabetes, and Nutrition, Boston University School of Medicine, Boston, MA
Iodine Uptake and Metabolism Thursday Oral Clinical 3:00 PM
Breastfed infants are reliant on maternal iodine for thyroid hormone production required for neurodevelopment. Dietary iodine among U.S. women of childbearing age may be insufficient. Perchlorate (ClO4), a competitive inhibitor of the sodium/iodide symporter (NIS), is ubiquitous in the U.S diet. Thiocyanate (SCN), from cigarette smoke and the diet, is a weaker NIS inhibitor. Environmental ClO4 and SCN exposures could decrease breastmilk iodine uptake by competitively inhibiting NIS in the lactating breast, thus impairing infants' iodine availability. They could also inhibit infants' thyroidal NIS to directly affect infant thyroid function.
Iodine, ClO4, and SCN levels in breastmilk, maternal and infant urine, and infant serum TSH and FT4 levels were cross-sectionally measured in Boston-area women and their 1–3 month-old breastfed infants. Univariate and multivariable analyses were performed to assess relationships between iodine, ClO4, SCN, log-transformed TSH, and FT4 levels.
64 mothers (mean age 28.7 yrs±7.9[ SD], 69% Black, 61% foreign-born, 6% smokers) and their breastfed infants (mean age 1.6 mos±0.5 [SD]) were recruited. Median (range) urinary iodine levels were 101.9 μg/L (27–570) in mothers and 197.5 (40–785) in infants (p<0.01). Levels of infant urinary iodine were positively correlated with breastmilk iodine (r=0.56, p<0.01) and maternal urine iodine (r=0.35, p<0.01). Median (range) ClO4 concentrations were 4.4 μg/L (0.5–29.5) in breastmilk, 3.1 μg/L (0.2–22.4) in maternal urine, and 4.7 (0.3–25.3) in infant urine. Breastmilk iodine was positively correlated with breastmilk ClO4(r=0.26, p=0.04) and SCN (r=0.51, p<0.01) and maternal urine iodine (r=0.35, p<0.01) levels. There were no significant correlations between infant TSH or FT4 and iodine, ClO4 and SCN levels in breastmilk, maternal urine, and infant urine. In multivariable analyses, only maternal urine SCN concentrations were positively associated with infant serum FT4 levels (p=0.04).
Boston-area mothers and their breastfed infants are generally iodine-sufficient. Although environmental ClO4 and SCN are ubiquitous, these results do not support the concern that maternal and infant ClO4 and SCN exposures affect infant thyroid function.
PBF Abrogates P53 Function and Causes Genetic Instability in Thyroid Cancer
Thyroid Cancer Thursday Oral Basic 2:15 PM
PBF is overexpressed in thyroid cancer and can transform cells in vitro. Moreover, subcutaneous expression of PBF elicits tumors in nude mice. Given the established role of ionizing radiation in thyroid tumorigenesis, we investigated the relationship between PBF, p53 and genetic instability.
In vitro studies performed in TPC-1 thyroid papillary carcinoma cells; Co-IP assays were used to determine the PBF:p53 interaction; HDM2 luciferase assays and oligo-pulldown assays to assess the effects of PBF on p53 gene activation; p53 half-life assays and MG-132 ubiquitin assays to determine p53 stability; MTT cell viability assays to investigate cell survival; and Fluorescent inter-simple sequence repeat-PCR (FISSR-PCR) to measure the index of genetic instability from murine thyroid DNA.
Co-IP assays revealed direct binding of PBF to p53 in TPC-1 cells, with a marked increase in binding after treatment with gamma-irradiation. PBF also repressed p53-mediated gene regulation through HDM2 promoter assays by approximately 30% (p<0.0001). Furthermore, PBF repressed p53 binding to the p21 promoter in specific oligo-pulldown assays. p53 showed strong affinity for the p21 promoter; however, in the presence of recombinant PBF protein, p53 binding was reduced in a dose dependent manner. Transient overexpression of PBF in TPC-1 cells resulted in a significant decrease in p53 protein levels compared to controls (75±2.5% decrease after 90 minutes, p<0.028, n=4). This result correlated with increased ubiquitination of p53. Additionally we observed a significant reduction of cell viability in mock-transfected TPC-1 cells after treatment with gamma-irradiation compared to untreated controls (17.9±0.008% decrease, p<0.016, n=4). Critically, overexpression of PBF abrogated this observed decrease of cell viability (0.2±0.007% decrease, p=NS, n=4). Finally in vivo, murine thyroids overexpressing PBF displayed higher levels of genetic instability compared to wild-type thyroids (18.75%, n=4).
These findings highlight a novel mechanism of thyroid tumorigenesis whereby PBF binds to p53 and inhibits its function, resulting in increased cell survival after DNA damage in vitro, and significantly elevated genetic instability in vivo.
Microbiology&Immunology, University of Illinois at Chicago, Chicago, IL
Thyroid Cancer Thursday Oral Basic 2:30 PM
Anaplastic thyroid cancer (ATC) has a very poor prognosis that may not be significantly altered by the current treatment regimens. Therefore there is a compelling need to identify potential new therapies. TNF-related apoptosis inducing ligand (TRAIL) induces apoptosis selectively in cancer cells and may be useful in the management of ATC. IG20/MADD is highly expressed in thyroid cancer and confers TRAIL resistance; therefore, we aimed to investigate the effects of IG20/MADD knockdown on TRAIL induced-apoptosis.
A shRNA expressing lentivirus was used to selectively knockdown IG20/MADD in the human ATC cell lines: C643, CAL62 and HTh7 ATC-cell lines with RAS mutation, and the 8505C cell line with BRAF mutation. Cells were treated with TRAIL alone or in combination with kinase inhibitors targeting the two main pro-survival pathways, MAPK, and/or PI3K/Akt, in thyroid cancer. Apoptosis was assessed by detection of activated caspase-3 by flow-cytometry.
C643, CAL62 and HTh7 cells were sensitive to TRAIL induced apoptosis, while 8505C cells were resistant to even high doses of TRAIL (100 ng/ml). Combination of TRAIL with select Akt/mTOR (perifosine and everolimus) and/or MEK inhibitors (PD-0325901) showed an antagonistic effect on TRAIL-induced apoptosis in C643 cells, but had no effect on 8505C cells. Upon knockdown of IG20/MADD, C643 cells had increased sensitivity to TRAIL induced apoptosis (p=0.022) and rendered previously resistant 8505C cells sensitive to TRAIL (p=0.009).
IG20/MADD knockdown in TRAIL treated cells enhanced apoptosis in sensitive ATC cells and induced significant cytotoxicity in resistant ATC cells. This effect was not enhanced significantly in the presence of various inhibitors of the MAPK/PI3K/Akt signaling pathways. TRAIL treatment combined with IG20/MADD knockdown may be a potential therapeutic modality for anaplastic thyroid cancer.
Oral Health Research, University of Kentucky, Lexington, KY
Thyroid Cancer Thursday Oral Basic 2:45 PM
Thyroid cancer is the fastest increasing incidence cancer amidst all cancers in both sexes. Nonmedullary (NMTC) accounts for ≈94% of cases and 3–6% of these appear familial (FNMTC). Alterations of the telomere-telomerase complex have been reported in association with several malignancies including thyroid cancer. Capezzone et al (JCEM 93:3950, 2008) reported short telomeres, hTERT gene amplification & increased telomerase enzymatic activity in their Italian cohort of FNMTC and we sought to replicate these findings in a different patient population.
We evaluated, in triplicate analyses, mean relative telomere length (RTL), telomerase gene copy number (TGCN) in 36 FNMTC (26 Papillary & variants, 10 Follicular & variants; 21 kindreds), 53 sporadic NMTC cases (43 Papillary & variants, 10 follicular & variants) and 24 healthy volunteers, utilizing DNA obtained from peripheral blood mononuclear cells. We assessed RTL using multiplex quantitative real-time PCR (qPCR; LightCycler®480, Roche) and TGCN by standard qPCR, analyzed as a ratio (Pfaffl's method; Nucl Acids Res 29:2002, 2001) to results for reference single-copy genes (albumin & Colony Stimulating Factor 1 Receptor) with a ratio >2 considered demonstrative of gene amplification.
Data analysis shows no significant difference in RTL between the FNMTC samples and those of healthy volunteers (p=0.537, one-way ANOVA, adjusted for age and sex). On the other hand, the sporadic NMTC samples revealed a longer mean RTL (1.56) that was significantly different from the FNMTC samples and nearly significantly different from those of healthy volunteers (p=0.035 and p=0.068, respectively). We could not find any evidence for hTERT gene amplification in any of these subjects.
These results differ from the findings of Capezzone et al who found significantly shorter RTL in their FNMTC cohort than in their healthy volunteers and sporadic cases, rather than our finding of increased RTL in sporadic NMTC cases. Also, contrary to the report of Capezzone et al, there was no evidence of hTERT gene amplification in our FNMTC cohort. Our findings call into question whether the telomerase gene plays any role in producing a familial risk for nonmedullary thyroid carcinomas.
Dept. of Internal Medicine II, Ludwig-Maximilians-University, Munich, Germany
Thyroid Cancer Thursday Oral Basic 3:00 PM
In contrast to radioiodine-refractory differentiated (DTC) and anaplastic thyroid cancer (ATC), radioiodine-sensitive DTC can be efficiently treated by the application of radioiodine based on the expression of the sodium iodide symporter (NIS). Due to limited therapeutic options for radioiodine-refractory DTC and ATC we have started to evaluate novel polyplexes for non-viral NIS gene delivery, aiming at establishment of radioiodine therapy in these cancer types.
We have used nanoparticle vectors based on linear polyethylenimine (LPEI), shielded by polyethylene glycol (PEG), and coupled with the synthetic peptide GE11 as an epidermal growth factor receptor (EGFR)-specific ligand, that have been demonstrated by our earlier work to own high potential for systemic gene delivery. First, we have analyzed EGFR expression levels in various radioiodine-refractory DTC and ATC cell lines (ATC: SW1736, HTh74; DTC: ML-1, B-CPAP, FTC-133) by FACS-analysis. Thyroid cancer cells were incubated with LPEI-PEG-GE11/NIS and control polyplexes (LPEI-PEG-Cys/NIS) lacking the EGFR-specific ligand, followed by analysis of transfection efficiency by iodide uptake assay.
SW1736 and ML-1 showed the highest levels, B-CPAP and HTh74 intermediate levels, and FTC-133 the lowest levels of EGFR expression. Transduction efficiency correlated well with EGFR expression levels reaching highest levels with a 7–10-fold increase in perchlorate-sensitive iodide uptake activity in SW1736 and ML-1 cells as compared to mock transfected cells. Incubation with untargeted polymers (LPEI/PEG-Cys/NIS) resulted in a very low iodide uptake activity in all cell lines, demonstrating the EGFR-specificity of these polymers. In preliminary in vivo experiments, we established subcutaneous xenografts derived from ATC cell lines SW1736 and HTh74 in nude mice. 24h after systemic (i.v.) LPEI-PEG-GE11/NIS application SW1736 and HTh74 xenografts accumulated approx. 5–6% ID/g 123I as determined by γ-camera imaging.
In conclusion, our data clearly demonstrate the feasibility of establishment of radioiodine therapy for radioiodine-refractory DTC and ATC by tumor-selective systemic NIS gene transfer using EGFR-targeted synthetic nanoparticle vectors.
Thyroid Research Unit, James J Peters VA Medical Center, Mount Sinai School of Medicine, New York, NY
Autoimmunity Thursday Poster Basic
Extra-thyroidal expression of the TSH receptor (TSHR) has been detected in a variety of cell types and appears to have potentially important physiological roles. Of great interest is TSHR expression in fibroblasts, adipocytes, and macrophages, each of which has been implicated in the pathophysiology of Graves' Orbitopathy (GO). In particular, it has been hypothesized that the TSHR autoantigen on fibroblasts and adipocytes may be responsible for selective targeting of the immune system to the retro-orbit. Antibodies (Abs) to the TSHR may have stimulating, blocking, or neutral activity when compared to TSH action and TSHR-Ab titers in patients with Graves' disease correlate with the extent of their GO. Since we have recently observed that neutral TSHR-Abs are far from “neutral” but rather have distinct signaling imprints in thyrocytes resulting in cell apoptosis (Endocrinology 2010, 151:5537), we have extended this evaluation to the study of fibroblast cultures.
Antibody-treated murine preadipocytes (3T3-L1 cells) were selected for their TSHR expression using magnetic beads bound to TSHR-mAb (RSR-1) after which they were >90% TSHR positive.
These cultures responded to TSH and stimulating TSHR-mAbs with enhanced proliferation over a 3 day culture. In contrast, neutral TSHR-mAb (Tab-16) activated stress signaling, as determined by the induction of ROS, and later induced widespread apoptosis in up to 50% of cells after 5 days (compared to ∼10% in controls), as measured by Annexin V and mitochondrial marker (JC-1) assays. This enhanced apoptosis was caspase dependent as evidenced by up to a 40% increase in total caspase activity (by FLICA).
These data show that while stimulating TSHR-Abs may contribute to fibroblast and adipocyte proliferation, neutral TSHR-Abs may aggravate the local inflammatory infiltrate within the thyroid and in the retro-orbit by inducing cellular apoptosis; a phenomenon known to activate innate and by-stander immune-reactivity via DNA release from the apoptotic cells. (Supported by DK 080459, DK052464 and DK069713).
GM-CSF Matured Bone Marrow Dendritic Cells Can Expand Tregs and Suppress Experimental Autoimmune Thyroiditis (EAT)
Autoimmunity Thursday Poster Basic
Autoimmune thyroiditis is a common endocrine disorder, and has no effective treatment. GM-CSF, which primarily acts on bone marrow (BM) precursors, can suppress ongoing EAT. Bone marrow derived dendritic cells (BMDCs) were able to expand natural Tregs (Tregs) significantly more efficiently than splenic DCs (SpDCs). These ex vivo generated Tregs could suppress mTg specific T cell responses in vitro. In this study we wanted to test the suppressive capacity of Tregs to suppress EAT, and determine the underlying mechanism of BMDC induced Treg expansion.
BM precursors were cultured in the presence of GM-CSF to obtain BMDCs, which were co-cultured with CD4+ T cells. Five days later, the T cells were analyzed for Treg expansion, cytokine production and in vitro suppressor function. BMDCs and Tregs were adoptively transferred to assess their ability to suppress EAT. BMDCs were characterized for cell surface expression of relevant molecules and their role in Treg expansion was determined either using cells from knockout mice or blocking antibodies.
Adoptive transfer of BMDCs or Tregs, generated ex vivo, were able to suppress EAT in recipient mice. Using MHC class II-/- BMDCs, we showed that Treg expansion occurred in the absence of TCR engagement, but was contact dependent and required IL-2. Further investigation revealed significantly higher levels of expression of OX40L and Jagged-1 on BMDCs, and OX40 and Notch3 on Foxp3+ T cells. Blocking OX40L or Jagged-1 on BMDCs, or Notch signaling in Tregs abrogated BMDC mediated Treg expansion. Therefore, it is likely that the Notch3 and OX40 on Tregs act as the cognate receptors for Jagged-1 and OX40L respectively, and mediate the required co-signaling for Treg expansion. We ruled out any role for other molecules expressed on BMDCs in Treg expansion in the absence of TCR stimulation.
Our studies show the potential use of BMDCs in vitro or in vivo for Treg expansion to treat EAT. We show OX40 and Notch mediated signaling, which hitherto has not been recognized, as critical for Treg expansion. These findings have significant implications for developing novel therapies for autoimmune diseases in general, and thyroiditis in particular.
First Department of Internal Medicine, Wakayama Medical University, Wakayama, Japan
Autoimmunity Thursday Poster Basic
Development of Autoimmune thyroid disease (AITD) including Graves' disease (GD) and Hashimoto's disease (HD) is related to expression of HLA-DRB1*0301(DR3). The extracellular domain (ECD) of human TSH receptor (hTSH-R) is a crucial antigen in GD.
DR3 transgenic mice immunized to recombinant hTSH-R-ECD protein or hTSH-R-ECD peptides were generated as an AITD model. Serum anti hTSH-R protein antibody, or anti hTSH-R peptide antibodies were titrated by ELISA to recognize B cell epitopes. hTSH-R peptide 37 (AA78–94) is an important immunogenic peptide in DR3 transgenic mice. A mutant hTSH-R peptide 37 (ISRIYVSIDATLSQLES:37m), in which peptide 37 HLA-DR3 binding motif position 5 was mutated V>A, and position 8 Q>S, was synthesized. 37m was predicted to bind to HLA-DR3, but not bind to T-cell receptors. DR3 transgenic mice were immunized with hTSH-R peptide 37 and 37m.
Mice immunized to hTSH-R protein developed strong TRAb, and weak TSI. Antisera from DR3 immunized transgenic mice reacted strongly with hTSH-R-ECD peptides 1 to 5, covering amino acid residues 20–94, sequences recognized as B-cell epitopes that react with human TRAb. In addition, antisera to hTSH-R protein recognized hTSH-R peptides 21 (258–277), 41 (283–297), 36 (376–389), and 31 (399–418). Antisera raised to peptide 37 provided striking results. The antisera bound to peptides 1–7 (20–112), 10 (132–150), 33 (137–150), 41, 23 (286–305), 24 (301–320), 36, and 31, as well as to hTSH-R-ECD protein. Antibody titers to peptide 37, and reaction of splenocytes to peptide 37, were significantly reduced in mice immunized to peptide 37 plus 37m, compare to mice immunized to peptide 37 alone (SI: 0.92±0.13 vs 1.77±0.87, P=0.0081).
Binding of anti hTSH-R-antibodies to the amino-terminal end of the ECD was confirmed in our DR3 transgenic mice. The ability of immunization to a single peptide to induce antibodies that bind whole TSHR protein, as well as multiple un-related peptides, is a unique observation. The mechanism may relate to developing immunity to host TSH-R, and epitope spreading along this antigen. Immunogenic reaction to peptide 37 could be partially suppressed by competing peptide 37m, and in theory this might contribute to immunotherapy of AITD.
Cell-Mediated Immunity Against Calsquestrin (CSQ) and Collagen XIII (COLLXIII), A Possible Link Between Thyroid Autoimmunity and Orbital Inflammation in Thyroid Eye Disease
Autoimmunity Thursday Poster Clinical
The link between thyroid autoimmunity and orbital inflammation seen in thyroid eye disease (TED) is unclear. A proposed link is the presence of a thyroid and orbital tissue shared antigen that triggers the autoimmune reactions in the orbit. There are few candidate extraocular muscle and connective tissue antigens including Calsquestrin (CSQ) and Collagen XIII (CollXIII). The genes encoding CSQ2 are upregulated in the thyroid of TED patients. In addition, CSQ1 is expressed 4.7 times more in the extraocular muscles than any other skeletal muscles explaining the specificity of the autoimmune reactions to the tissue. Furthermore, a recent study has identified serum CSQ1 antibodies as specific markers of ophthalmopathy and sensitive indicators of eye muscle damage. CollXIII also seems to play a role in the development of TED where majority of patients have increased serum antibody levels to the protein. The role of cell-mediated immunity to these antigens has not yet been extensively addressed. The current study objective is to examine the specificity of intrathyroidal T cells to the antigens in patients with TED. This aims to clarify whether cell-mediated immunity against the proteins is a possible link between thyroid autoimmunity and orbital inflammation seen in the disease.
Analysis of intrathyroidal T-cell sensitivity to the proteins was done by culturing thyroid mononuclear cells in the presence of the antigens in a cell proliferation assay. Proliferation of the cells was quantified using Bromodeoxyuridine (BrdU) uptake method and enzyme-linked immunosorbent assay (ELISA).
Results have indicated higher T-cell response to both antigens for patients with TED compared to controls.
Cell-mediated immunity against CSQ1 and CollXIII is a possible link between thyroid and orbital autoimmune reactions in TED. Further research into these proteins and their link to TED would shine new insights into the triggering events in the development of the disease and can be used as a way to develop possible therapies for the disorder.
Absence of Neonatal Hypothyroxinaemia in Infants Born to Goitrous Mothers with Potent Thyrotropin Receptor Blocking Antibodies
Autoimmunity Thursday Poster Clinical
The emergence of thyroid receptor blocking antibodies (TSBAb) has been suggested by some to account for the remission of Graves' disease in pregnancy (1). Theoretically however, the presence of these autoantibodies may potentially pose a separate problem to the neonate, giving rise to transient hypothyroidism by blocking the neonatal TSH receptors.
Two clinical cases are presented.
Patient A had a long-standing history of Graves' disease and was frankly toxic at first presentation. She was later found to be pregnant and became rapidly hypothyroxinaemic requiring LT4 by 16 weeks. Evaluation at 16 and 30 weeks revealed that she had no TSI but had potent TSBAb activity. The neonate had mildly elevated TSH levels for 15 weeks but serum thyroxine levels remained normal without treatment. The patient became pregnant again 3 years later. The second offspring was born with TBII (>40IU/L) with strong TSBAb activity (7%) but maintained normal thyroid function throughout the perinatal period. Patient B was diagnosed with hypothyroidism at the age of 13. Biochemical tests revealed strong TBII (>40IU/L) and TSBAb activities (8%). She became pregnant at age 27 and her TBII levels remained >40IU/L throughout pregnancy. Her offspring was born with an elevated TBII level of 22.6 IU/L (NR 0–1.5) but normal thyroid function. Evaluation of the mother's serum post-delivery showed persistent TBII and TSBAb activities.
These cases illustrate that potent maternal TSBAb need not necessarily result in neonatal hypothyroidism and suggests that the maternal and fetal thyroidal responses to these antibodies may not be identical.
Serum Levels and Medications of Patient A
Reference
Autoimmunity Thursday Poster Clinical
B cells have multiple functions and when activated contribute to the pathogenesis of autoimmune disease. B-lymphocyte activating factor (BAFF), a member of TNF family, promotes the maturation and of transitional B cells and proliferation. Serum BAFF concentrations were found increased in several systemic and organ specific autoimmune disease. In the present study we aimed to measure serum BAFF concentrations in patients with GD with and without GO and in relation to either intravenous steroid (IVGC) or rituximab (RTX) treatment for active GO.
We studied 8 patients with GD without GO, 23 patients with active GO, 12 patients with inactive GO and 9 normal control subjects (C). Nine patients with active GO were treated with RTX and 14 with IVGC. Serum BAFF concentrations were measured in all patients at baseline, at the time of peripheral B cell depletion and repopulation in those treated with RTX and IVGC.
Overall, mean serum basal BAFF concentrations were found to be significantly elevated in GD patients when compared to C (P=0.001). Serum BAFF concentrations were also significantly correlated with serum TgAb (P=0.04), but not with sex, age, smoking habits, therapy and serum TPOAb and TRAb (P=NS). No difference was found in basal serum concentrations of BAFF in patients with active or inactive GO (P=NS). On the other hand, changes of serum BAFF in relation to treatment of active GO were highly remarkable. After RTX, there was a significant, marked increase of serum BAFF concentrations at the time of B cell depletion (P=0.02) and also at B cell repopulation (P=0.04). After IVGC, basal serum BAFF concentrations decreased significantly (P=0.001).
We report, for the first time, that BAFF concentrations are increased in the serum of patients with GD and GO. Serum BAFF is further increased in patients with active GO after B cell depletion with RTX, when maturation of transitional B cell is highly stimulated for repopulation. On the other hand, the significant decrease of serum BAFF after IVGC may imply an immunosuppressive role on the B cell compartment by steroid therapy. These data further underscore the importance of B cells involvement in the pathophysiology of GD and GO.
Association of Nuclear Transcription Factor Peroxisome Proliferator-Activated Receptor-γ (PPARγ) Gene Polymorphism with Susceptibility to Graves' Ophthalmopathy
Autoimmunity Thursday Poster Clinical
Graves' ophthalmopathy (GO) is an autoimmune disorder characterized by the autoimmunity against TSH receptor in the orbit. The nuclear transcription factor peroxisome proliferator-activated receptor-γ (PPARγ) may be involved in adipogenesis and increased expression of TSH receptor on adipocytes. Recently the association of Pro12Ala PPARγ gene polymorphism with severity of GO has been reported in Caucasian population. The aim of this study is to evaluate whether Pro12Ala PPARγ gene polymorphism could be associated with GO in Japanese population.
We studied 419 Japanese patients with Graves' disease (GD) in our outpatient clinic and 300 healthy subjects. Ophthalmopathy was classified using the classification of the American Thyroid Association. Blood samples were taken for DNA extraction. The Pro12Ala PPARγ gene polymorphism was genotyped by polymerase chain reaction amplification and followed by digestion with the restriction enzyme BstUI or direct sequencing.
There were no differences in CC genotype (Pro12Pro) frequency or C allele frequency between GD and control subjects. However, the C allele frequency was significantly greater in patients with ophthalmopathy (ATA class III or more) than those with ATA class 0-II (98% vs. 92%, p=0.044). The CC genotype and C allele frequencies were significantly greater in patients with ophthalmopathy (classified as ATA class III) compared to those in patients without ophthalmopathy (ATA class 0) (CC genotype, 99% vs. 92%, p=0.0197 ; C allele, 99% vs. 96%, p=0.0309).
The results suggest that Pro12Ala PPARγ gene polymorphism may be associated with susceptibility to GO in Japanese population, as previously reported in Caucasian population.
Simultaneous Occurrence of Subacute Thyroiditis and Graves' Disease
Autoimmunity Thursday Poster Clinical
Rare cases of Graves' disease occurring years after subacute thyroiditis (SAT) have been reported. We hereby present the first known case of simultaneous occurrence of Graves' disease and SAT.
A 41 year-old woman who initially presented with neck pain, dysphagia, odynophagia, cough and hyperthyroid symptoms. Physical examination: HR 110/ min, thyroid gland was diffusely enlarged and tender; no evidence of orbitopathy. There were resting tremors of the fingers and brisk DTRs.
Laboratory values: TSH<0.01 mcIU/mL (nl 0.39–5.33), FT4 2.0 ng/dL (nl 0.59–1.60), free T3 6.6 pg/mL (nl 2.3–4.2), thyroglobulin 20.1 ng/mL (nl 2.0–35.0), Tg antibody 843 IU/ml (nl 0–80), TPO antibody 130 IU/mL (nl 0–29), thyroid stimulating hormone receptor antibody 22.90 IU/L (nl<1.22), thyroid stimulating immunoglobulins 299 units (nl<140), ESR 120 mm/h (nl 0–20), CRP 1.117 mg/dL (nl 0–0.5). Thyroid ultrasound showed an enlarged patchy heterogeneous gland with hyperechoic areas bilaterally and mild hypervascularity. Thyroid FNA done to rule out acute hemorrhage revealed granulomatous thyroiditis (Figure). Thyroid uptake and scan (I-123) showed a diffusely enlarged gland with a 5-hr uptake of 6.6 % (nl 4–15) and heterogeneous trapping. The patient was given atenolol and ibuprofen. Symptoms resolved over the next several weeks.
Figure showing granulomatous lesions in thyroid FNA cytology specimen.
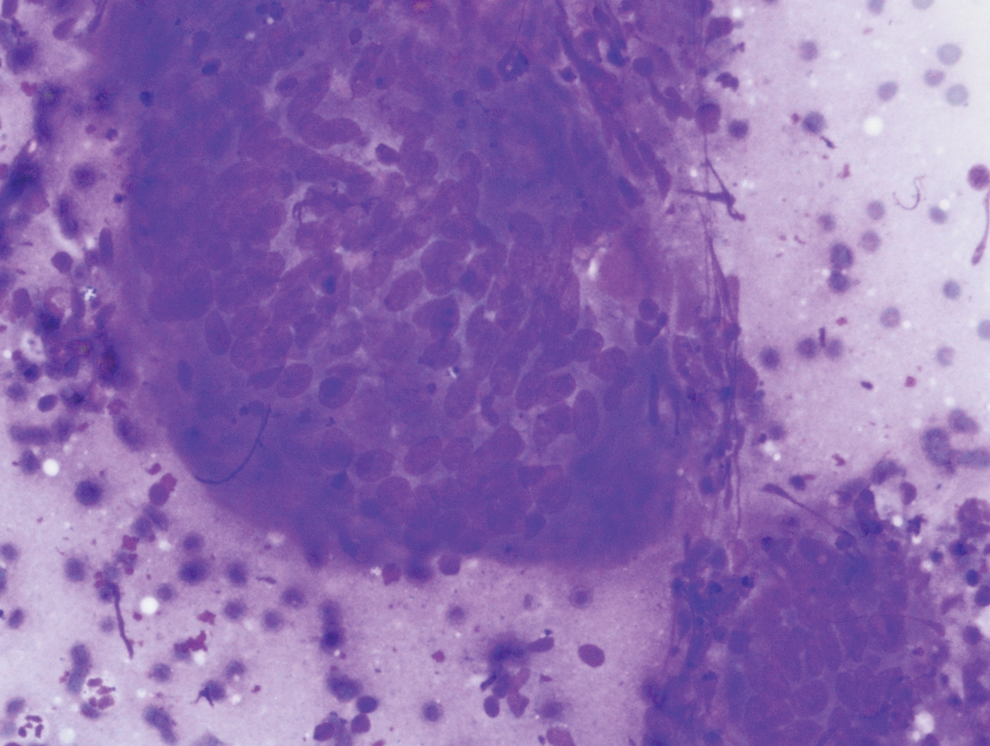
This case illustrates a rare simultaneous occurrence of Graves' disease and SAT. Previous case studies have shown that Graves' disease may develop months to years after an episode of SAT. Although the occurrence of SAT with Graves' disease may be co-incidental, SAT-induced autoimmune alteration may promote the development of Graves' disease in susceptible patients (Bartanlena et al). Genetically mediated mechanisms may also be involved.
Reference
Medicine I, Gutenberg University Medical Center, Mainz, Germany
Autoimmunity Thursday Poster Clinical
We aimed to compare the analytical sensitivity of a FDA-cleared chimeric TSH-R bioassay that measures thyroid stimulating immunoglobulin (TSI) and TSH-R binding inhibitory immunoglobulin (TBII) assays.
Sera from patients with Graves' disease, positive for both TSI and TBII, were serially diluted into normal serum at final dilutions of 1:3, 1:9, 1:27, 1:81, 1:243, 1:729, 1:2187 and 1:6561 in triplicate. TSI levels were expressed as the percent specimen-to-reference-ratio SRR%. Two TBII methods were used (Brahms RIA and Roche ECLIA). Titres were expressed as the dilution of the serum that reduced the TSI or TBII level to below the cut-off of each assay (TSI SRR%<140; Brahms<1.0 IU/L and Roche<1.75 IU/L).
A total of 96 serum samples from 23 hyperthyroid patients with Graves' disease were prospectively evaluated prior to and during antithyroid treatment. A markedly higher analytical sensitivity for the TSI bioassay was observed in all undiluted sera (p=0.006) and at each dilution: 1:3 (p<0.001), 1:9 (p=0.002), 1:27 (p<0.001) and 1:81 (p<0.001; Chi-square test). At dilutions 1:243 and 1:729 four and two samples, respectively, were TSI-positive, whereas all samples were negative in the TBII-assays at 1:243. There was a close correlation between the undiluted values and the TSI titers. The mean (±SD) baseline TSI values of samples with TSI titres of 1:3, 1:9, 1:27, 1:81 and 1:243 were SRR% 223 (±66), 311 (±48), 397 (±76), 474 (±53) and 461 (±51). A “hook effect” was observed in samples with the highest titers. This may explain why the undiluted SRR% of the 1:243 dilution (461) is not higher than that of the 1:81 (474).
This dilution analysis demonstrates the high analytical sensitivity of the chimeric TSH-R bioassay. TSI titers closely correlate with the undiluted TSI values and offer additional information which may have clinical utility.
Oxidation Res, Cor.Con.International Srl, Parma, Italy
Disorders of Thyroid Function Thursday Poster Basic
T3S (3,5,3′-triiodothyronine sulfate) has been shown to be a thyromimetic in surgically hypothyroid rats following daily ip injection in the nanomolar range. The activity of T3S was found to be about 1/5 of T3. However, there are no data about the modification of the oxidative balance and hs-CRP.
Fifty male rats Charles River weighing 200–220 g were used; 10 rats were considered as a control group (sham operated for thyroidectomy), whereas the remaining 40 rats underwent surgical thyroidectomy and were divided into 4 groups of 10 animals each (respectively A,B,C,D). Group A was the control group, group B was treated with T3S (50 mcg/kg/day); Group C was treated with T3S+T4 (respectively 50 mcg and 125 mcg/Kg/day); Group D was treated with T4 (125 mcg/Kg/day). All the treatment continued for 10 days. Body weight (g), serum TSH (ng/mL) and T3 levels (ng/mL), plasma d-ROMs test (for hydroperoxides in terms of U.CARR.-Carratelli Units) and serum hs-CRP (mcg/mL) were measured at baseline, 10 days after thyroidectomy, and finally 10 days after treatments with T3S and T4.
In the control group all the animals survived, whereas in the treatment groups the survived animals were from 8 to 10 (see table 1). After 10 days of treatment (20 days after thyroidectomy) the body weight increase was similar in the control group and in groups C and D, whereas it was significantly lower in the group A. Thyroidectomy causes a significant reduction of OS (oxidative stress) which, at the opposite, increases after the hormones treatment, with the maximum level in the combined treatment with T3S and T4 (Group C). The hs-CRP increase was evident in all the animals, and again the highest values were found in the Group C.
Determination of Body Weight, TSH, T3, d-ROMS Test and h-CPR in Rats 10 Days After Thyroidectomy (Mean Value±SD)
t test Vs Group A p<0.05; bt test Vs Control p<0.05; ct test Vs Group B; dt test Vs Group D.
Both T3S and T4 administered to rats after surgical hypothyroidism causes OS, which becomes extremely high together with a concomitant increase of hs-CRP.
Disorders of Thyroid Function Thursday Poster Clinical
Thyroid storm is a rare complication of thyrotoxicosis associated with a high mortality. The Burch and Wartofsky (BW) scoring system is the most widely used instrument to aid in the diagnosis of thyroid storm. The diagnostic accuracy of the BW scoring system has never been evaluated in a large contemporary cohort. The purpose of this study is determine the ability of the BW score to diagnose thyroid storm compared to expert opinion, and to determine the ability of the BW score to predict adverse clinical outcomes.
The charts of all patients presenting to 4 acute care hospitals in Hamilton, Ontario between January 2000 and December 2010 with a diagnosis of thyrotoxicosis were reviewed (n=1310). Patients with normal thyroid indices, subclinical hyperthyroidism, and stable thyroid disease were excluded, leaving 228 subjects included in final analysis. The BW score was calculated for each patient. Sensitivity and specificity of the BW score was determined using expert opinion as the gold standard. Chi squared and Mann Whitney U tests were used to correlate the BW score with mortality, admission to a monitored care setting (intensive care unit or step down unit), and length of hospital stay. Logistic regression was used to determine elements of the BW score most associated with mortality and admission to a monitored setting.
The mean age of participants was 54.8 years, with 71.9% females. With a cutoff of 45 points, the sensitivity and specificity of the BW score was 85.7% and 71.0%, respectively. A score of 45 or greater was associated with mortality (12.2% vs. 3.2%, p=0.015) and admission to a monitored setting (52.7% vs. 19.5%, p<0.001) but not with length of hospital stay (p=0.055). Congestive heart failure and precipitating event were predictive of mortality (p=0.009, 0.015). Tachycardia, congestive heart failure, and precipitating event were predictive of admission to a monitored setting (p=0.032, 0.002, <0.001).
The BW score has good sensitivity and moderate specificity for diagnosing thyroid storm and has utility in predicting mortality and the need for monitored care. Only a few elements of the BW score were found to be predictive of clinically relevant outcomes independently.
Parathyroidectomy in Illinois: Volume, Setting, and Practice Pattern
Disorders of Thyroid Function Thursday Poster Clinical
Over time, surgery has become progressively specialized. We hypothesize that parathyroid surgery has become more commonly performed in tertiary care centers under the care of specialized surgeons.
All the parathyroidectomies performed in Illinois from 2001 to 2010 were retrieved from the Illinois Hospital Association database. The 10-year time frame was divided into early (2001 to 2005) and late (2006 to 2010) periods. CPT and ICD 9 codes were used to identify the operations and diagnoses. The hospitals were categorized into university, university-affiliated, and community hospitals. The operating surgeons were identified and categorized into general surgeons (GS), endocrine surgeons (ES), surgical oncologists (SO), and otorynolaryngologists (ENT) according to their training. The volume and extent of parathyroidectomy by the different types of surgeons and hospitals were compared for the two time periods.
3464 and 3204 parathyroidectomies were identified in the early and late period, respectively. There were 5 university, 15 university-affiliated, and 117 community hospitals. Community hospitals had the highest percentage of operations in both periods, 44% and 41%, respectively (p<0.003). University hospitals had 34% in both periods, while university-affiliated hospitals had an increase from 22 to 25%. ES performed the highest percentage of parathyroidectomies in both periods: 43% and 42% respectively (p<0.003). GS performed 36% in both periods while ENT performed 15% and 16%, respectively. SO performed 6% of the operations in both periods. Irrespective of diagnosis, GS had the highest percentage of total parathyroidectomy with reimplantation, 15% and 19%, in the early and late period, respectively (p<0.001). In comparison, ES performed 7% and 8%, 10% and 8% for SO, 12% and 10% for ENT, respectively.
In Illinois, the volume of parathyroidectomies has remained stable over the past 10 years. Community hospitals and endocrine surgeons continue to perform the majority of parathyroidectomies (p<0.003). General surgeons perform the highest percentage of total parathyroidectomies with reimplantation. The degree of specialization has remained stable during this time period.
Changes in Serum TSH Receptor Antibody Values in Different Thyroid Volume After Radioactive Iodine Therapy in 61 Women of Child-Bearing Age with Graves' Disease
Disorders of Thyroid Function Thursday Poster Clinical
A high serum TSH receptor antibody (TRAb) value during pregnancy is one of the risk factors for fetal and neonatal hyperthyroidism. Although surgical resection of the thyroid is usually followed by a reduction of serum TRAb levels in variable degrees, the changes in the TRAb values in different post-radioiodine thyroid volume have never been studied.
Sixty-one female patients (mean age 24.1yr; range 13–35yr) with Graves' disease who received radioactive iodine (RAI) therapy before the age of 35 years old were examined. Thyroid function, serum TRAb values and ultrasonographic thyroid volume were obtained for 3 years after RAI. Based on the difference of the thyroid volume at 0.5 year after RAI, patients were divided into 2 groups: Shrinkage group (thyroid volume<10 ml at 0.5 year, n=30) and Non-shrinkage group (>or=10 ml at 0.5 year, n=31). We compared the serum TRAb values between the two groups.
The TRAb values (mean 34.1IU/L vs. 36.8IU/L, P=0.88) and the thyroid volume (mean 40g vs. 50g, P=0.10) before RAI were not significantly different between the two groups. The mean TRAb values measured for 3 years after RAI were significantly lower (P<0.05) in Shrinkage group than in Non-shrinkage group (36.3IU/L vs. 110.1IU/L at 0.5yr, 13.0IU/L vs. 44.0IU/L at 1yr, 5.3IU/L vs. 18.2IU/L at 2yrs, 3.5IU/L vs. 14.0IU/L at 3yrs). In addition, rate of the incidence of hypothyroidism was remarkably higher in Shrinkage group than in Non-shrinkage group (60.0% vs. 9.7% at 0.5 yr, 66.7 vs. 12.9% at 1 yr, 73.3% vs. 16.1% at 2 yrs, 80.0% vs. 22.6% at 3 yrs).
We believe that the goal of iodine-131 therapy for Graves' disease in child-bearing age is to induce hypothyroidism as a result of thyroid ablation from the viewpoint of reducing the TRAb value.
endocrinology, Scientific research institute of cardiology and internal illnesses, Almaty, Kazakhstan
Disorders of Thyroid Function Thursday Poster
The research objective: studying of a condition of cardiovascular system in advanced age patients with hypothyroidism.
86 patients with subclinical (SHT), 132 with manifest hypothyroidism (OHT) and 18 practically healthy inspected. Levels of thyroid hormones were defined by standard methods in blood. For an estimation of a functional status of vegetative nervous system, cardiovascular system to patients spent analysis of variability people have been of intimate rhythms and measurement of levels systolic and diastolic arterial pressure (AP).
As a result of research it is revealed, that at patients with OHT level of TSH was in limits from 23.7±2.8 to 29.5±2.8 mME/ml and FT4 from 5.0±0.6 to 7.9±1.3 pg/ml at patients with overt hypothyroidism and TSH 7.3±0.8 to 9.2±1.6 mME/ml and FT4 from 11.9±2.2 to 14.3±1.9 pg/ml at patients with subclinical hypothyroidism. At 45.7% of elderly patients OHT the AP raised from 160/90 to 180/110 mmHg, at 15.2% of elderly patients with OHT the AP raised from 180/100mmHg to 220/130 mmHg. The same tendency was marked at 61.1% of patients SHT where increase both systolic is noted, and diastolic AP. It is necessary to notice, that increase in age at patients OHT met an arterial hypertension is more often. Only 4% of patients with OHT of advanced age had high blood pressure and 22%—low arterial pressure. By the data at all patients with hypothyroidism advanced age low levels of integrated indicators of a functional condition of vegetative system were defined. At patients with hypothyroidism the elderly age authentic decrease in indicators RMSSD (20.9±1.9ms) was observed, pNN50 (14.7±6.3%) in comparison with the same indicators of healthy faces (76.8±0.23 ms and 93.17±0.12% accordingly, P<0.05), that testifies to easing of parasympathetic influence of vegetative nervous system. At patients with hypothyroidism authentic increase of indicators AMo (52.7±2.4ms), relation LF/HF (2.5±0.4), that testifies to prevalence of sympathetic part of vegetative nervous system at elderly patients OHT.
Thus, patients with hypothyroidism advanced age most often have arterial hypertension, activation of sympathetic department and braking of parasympathetic department of vegetative nervous system.
Medical Endocrinology, Rigshospitalet, Copenhagen, Denmark
Disorders of Thyroid Function Thursday Poster Clinical
Since commencement of growth hormone (GH) treatment for adult hypopituitary pts, the adequacy of other pituitary deficiencies has been more in focus by clinicians. The purpose of this study was to evaluate if enhanced thyroid replacement in hypopituitary patients improves cardiovascular risk markers.
In all 85 hypopituitary patients (45 women) with GH deficiency; 7 had isolated GH deficiency, 15 had panhypopituitarism, while 25, 16 and 22 patients had 1, 2 and 3 additional deficits respectively. Biochemical and body composition assessment was performed at baseline (when patients were GH naïve), and at follow-up (median 4.7 years (3.0–5.5) after initiation of GH). Patients were divided into TSH sufficient (TSHsuff) (not on T4 and free T4>12 (n=23)), and TSH deficient (TSHdef), and further divided into tertiles according to baseline free T4.
Baseline free T4 was negatively associated with BMI (P=0.003) and total fat mass (P=0.01). TSHdef patients with lowest tertile free T4 had higher total (P=0.01) and LDL cholesterol (P=0.05) and triglycerides (P<0.01) compared to TSHsuff patients, also after adjustment for gender, age, BMI and IGF-I. At follow-up 9 patients initially defined as TSHsuff had initiated levothyroxine treatment. 53 and 28% of patients with free T4 from the low and median tertiles respectively, received an increased levothyroxine dose compared to baseline, whereas 40% of patients with free T4 from the median/high tertile groups had had a dose reduction. None recovered from TSHdef. Free T4 at follow-up was not significantly correlated to body-composition or cholesterol variables, nor were there any group differences among patients in the four groups according to TSH and free T4. Delta free T4 (follow-up−baseline) was negatively correlated to delta total cholesterol (r=−0.23; P=0.06) and LDL cholesterol (r=−0.30; P=0.01) and remained so after adjustment for the change in IGF-I (P=0.02).
After approx 5 years of GH replacement of adult hypopituitary patients, those with hypothyroidism were better adjusted also with respect to the thyroid axis. This was accompanied by an mprovement of the lipids of a higher magnitude than seen after GH replacement alone.
Analysis of Variable Dose I−131 Treatment in Management of Hyperthyroidism
Disorders of Thyroid Function Thursday Poster Clinical
Radioiodine therapy is an established mode of treatment for thyrotoxicosis of large range of etiologies. Different therapeutic regimes have been attempted to institute appropriate dose of radio iodine.However dose regime choice remain highly controversial varying greatly from institution to institution. The objective of this study is to assess the efficacy of three different ranges of variable doses of 131 radio Iodine therapy in patients with hyperthyroidism and to evaluate the incidence of hypothyroidism following radio iodine therapy at different doses.
In this retrospective study, 127 patients treated with I-131 for hyperthyroidism between Jan 2006–Jan 2007 was included. The diagnosis of hyperthyroidism was made clinically and confirmed by laboratory study. Tc 99m Tco4 scan was performed. The dose given to the patients was determined by the size of goiter, clinical problems, avidity of TcO4 on uptake scan and history of any prior antithyroid medication. The patients were categorized in three groups. Group I received 3 mCi I131; Group II received 5 mCi I131; Group III received 7 mCi I131. All patients were followed up at 6 weeks, 3 months and then 6 monthly. Statistical analysis was done with fisher's test.
The requirement of second dose therapy was 70% patients from Group I, 22% patients from Group II and 30% patients from Group III. Relative risk of patients of Group I for requiring second dose was 3 and 2.73 as compared to Group II and Group III respectively which was statistically significant. There was no e/o of prolonging occurrence of hypothyroidism in groupI. No e/o any significantly increased relative risk of hypothyroidism noted in any of the treatment group.
Patients treated with groupI treatment regimen,required multiple doses suggesting ineffective radiation dose delivered to hyper functioning gland to suppress its function and that there was no evidence of prolonging hypothyroidism in patients treated with small dose as compared to other two groups. Our study indicates that the optimal dose of 5mCi of radioiodine should be given for the complete cure of hyperthyroidism to minimize the necessity of multiple doses.
Endocrinology, Tokyo Health Service Association, Tokyo, Japan
Disorders of Thyroid Function Thursday Poster Clinical
Fetal hyperthyroidism (FH) can occur in women who have reached remission status after ablative therapy for Graves' disease. FH in this setting has usually been treated by giving thionamides to mothers. We use iodine first, and add thionamides when fetal heart rates do not sufficiently decrease or increase after a transient fall. Reasons for iodine use are 1) Side effects by thionamides that are unnecessary for the mother should be avoided; 2) Iodine has prompt therapeutic effects; 3) Iodine may expose the fetus to a lower risk of hypothyroidism than thionamides (JCEM 75:738,1992).
We treated 14 cases of FH in women who were euthyroid with or without thyroxine after surgery or radioiodine therapy for Graves' disease. Iodine was initiated between 22 and 36 weeks of gestation because the development of FH was highly probable on the bases of TSAb, TBII values, and/or fetal heart rates. Ten of the 14 were treated with iodine alone (G1), and thionamides were added in the other 4 (G2).
At birth, thyroid function was suppressed in none of the 14 neonates. FT4 was normal in 2 and slightly or mildly above normal in the remaining 8 in G1: the highest FT4 level was 3.4 ng/dL. In G2, FT4 was normal in 3 and slightly above normal in the other one. After birth, neonatal hyperthyroidism developed in all 14 but one in G1.
It is concluded from these findings that, in the treatment of FH in women in remission status after ablative therapy, iodine mitigates or exerts sufficient therapeutic effects at a substantial frequency without inducing hypothyroidism. In order to add thionamides timely and in appropriate dose, development of the method that determine fetal thyroid status definitively and safely is essential.
A Vest to Stop Arrest
Disorders of Thyroid Function Thursday Poster Clinical
Ventricular tachycardia (VT) rarely occurs in the setting of thyrotoxicosis. A case of VT in a patient with Grave's disease and a structurally normal heart is presented below.
Case Report: A previously healthy 55-year-old male presented with 4-months of tremulousness, palpitations, fatigue, and weight loss. TSH was 0.01 and free thyroxine was 3.7. Radioactive iodine was administered for 24-hour uptake. Nine hours later he developed dyspnea, nausea, and epigastric pain and called 9–1-1. He was found to be in VT at a rate of 220 that resolved with cardioversion. On admission to Cardiology, he was afebrile and normotensive with a heart rate of 84 and potassium of 5.8. Physical exam was unremarkable. The 24-hour radioiodine uptake was 56%, consistent with Grave's disease. Therapy with 11 mCi of iodine-131 was administered on hospital day 1. An electrophysiology (EP) study was positive for inducible VT with a distinct morphology from the prior episode. Ablation was not performed. Cardiac MRI revealed a structurally normal heart and catheterization revealed no hemodynamically significant lesions. No subsequent episodes of VT occurred during his hospitalization. He was discharged on propranolol with an external defibrillator vest to be worn until an EP study could be repeated in a euthyroid state. He wore the external defibrillator vest for 1.5 months and elected not to have a repeat EP study. Ten months later he developed recurrent hyperthyroidism and underwent a near total thyroidectomy. It has been 36 months since his episode of VT and he has had no further cardiac events.
Wide complex tachycardia in thyrotoxicosis is not always supraventricular tachycardia with aberrancy. A review of the literature revealed 3 additional cases of VT in patients with thyrotoxicosis and no evidence of underlying heart disease. In all 3 cases, as in this case, VT did not recur after treatment of the underlying cause of thyrotoxicosis. VT has also been reported in the setting of thyroid storm, thyrotoxicosis with pre-existing heart disease, and thyrotoxic hypokalemic periodic paralysis.
Retrospective Audit of the Treatment of Thyrotoxic Patients with I131 at the Churchill Hospital, Oxford, UK
Disorders of Thyroid Function Thursday Poster Clinical
Thyrotoxic patients reduce their risk of bone or cardiovascular complications by undergoing definitive treatment, either surgery or radioiodine (I131). A significant proportion of patients receiving standardised doses of I131 suffer treatment failure requiring retreatment. The use of antithyroid drugs (ATD) before or after radioiodine is known to increase the rate of treatment failure, but reduces the rate of acute thyroid storm or I131 induced hypothyroidism. This audit compares the rate of treatment failure at our centre, where patients stop ATD 1 week before and restart 3 days after I131, to failure rates described in the meta-analysis by Walter et al (BMJ. 2007 Mar 10;334(7592):514) which reports that using ATD within 1 week of I131 increases treatment failure rates.
Data were collected on 101 patients attending thyrotoxic clinic during 2006 using a local patient database. This included: age, sex, referral centre, diagnosis, ATD (type and dose at clerking,) dose of I131 given, TSH at clerking and at 1 year, whether the patient was retreated with I131, and where available, information on TSH levels during the year following treatment.
101 cases were treated with I131 (200–800MBq). 7 (6.93%) were retreated at 1 year. This compared well with reported failure rates of 20–30%. However, for those cases where data were available (45% of the total) 14 were biochemically thyrotoxic at 1 year (31.1%). These cases include not only those in whom treatment with I131 failed, but also those who were rendered hypothyroid and were receiving excess thyroxine at the time of sampling. This may reflect a similar problem in data from the Walter et al meta-analysis. There were no cases of acute thyroid storm.
Our practice of stopping ATD 1 week before and restarting 3 days after I131 does not appear to increase the rate of treatment failure above that reported in the Walter meta-analysis, and may have helped prevent any cases of acute thyroid storm. The Royal College of Physicians (UK) published guidelines for treatment of throtoxicosis in 2007, suggesting stopping ATD 2 days before and restarting 1 week after I131. Our data will be useful in revised guidelines.
The Anti-Obesity Effects of Jueming Recipe by Increasing mRNA Expressions of β3-AR and UCP-2 in Adipose Tissues
Iodine Uptake and Metabolism Thursday Poster Basic
Following theories of Traditional Chinese Medicine (TCM) and combining with modern pharmacological researchs, for the first time our study invented a new recipe: Jueming Recipe (JR), a concoction of TCM, which was composed of Semen cassiae and turmeric. The study was designed to investigate anti-obesity effects of JR, and its influence on mRNA expressions of beta 3 adrenergic receptor (3-AR) and uncoupling protein 2 (UCP-2) in adipose tissue of diet-induced obese rats in a creative way.
Fifty male Sprague-Dawley rats were divided into normal control group (n=8) on ad libitum diet, and obese model group (n=42) on a diet of high fat chow for 2 weeks. Then 29 selected nutritional obese rats were divided into three groups: untreated obese model group (n=9); metformin group (n=10), orally given metformin; JR group (n=10), orally administrated JR, for 8 weeks respectively. Body weight, wet weight of visceral fat and percentage of body fat (PBF) of rats were measured. The levels of serum fasting blood glucose, lipid and insulin were assessed and insulin sensitivity index (ISI) was calculated. The changes of adipose tissue with Hematoxylin-Eosin stain were checked by light microscope, and the cellular diameter and quantity of adipocytes were evaluated. Finally, the mRNA expressions of β3-AR and UCP-2 from perirenal fat were detected by RT-PCR.
Compared with obese model group, body weight, wet weight of visceral fat and PBF of rats in JR group decreased significantly (P<0.01), the level of high-density lipoprotein cholesterol (HDL-C) increased markedly (P<0.01), ISI was higher (P<0.01), the diameters of adipocytes diminished significantly (P<0.01), and the mRNA expressions of β3-AR and UCP-2 from perirenal fat were greatly increased (P<0.05).
Our results of the experiment suggest that JR could reduce body weight and adipocyte size through up-regulating mRNA expressions of β3-AR and UCP-2 in adipose tissue, and improving insulin sensitivity in diet-induced obese rats.
Status of Iodine Nutrition in Asturias, a Iodine-Deficient Area in Spain, After 28 Years of Iodized Salt Promotion
Iodine Uptake and Metabolism Thursday Poster Clinical
Our community is considered one of the iodine-deficient areas in Spain, and promotion of iodized salt use was made over the last 28 years. To consider the eradication of iodine deficiency disorders, the WHO proposes these objectives: Households consuming iodized salt usually >90% Urinary iodine <100 μg/l<50% Urinary iodine <50 μg/l<20% OBJECTIVE: To know current status of iodine nutrition in Asturias, and determine whether Asturias met the target proposed by the WHO for eradication of iodine deficiency disorders after 28 years of promotion of iodized salt intake.
We selected a random sample of schoolchildren across the Asturian geography from 5 to 14 years. A survey on the consumption of iodized salt was answered by their families and the use in school canteen was checked. A urine sample was collected to determine urinary iodine, carried out by HPLC. For the statistical processing we used SPSS version 15.0.
The average urinary iodine excretion was 201.7±118.5 μg/L, with a median of 179 μg/L in a sample of 570 valid measurements. Girls showed a slightly lower half urinary iodine (193.5±106.4 μg/L) than boys (210±130 μg/L), without showing statistical significance (p=0.09). The proportion of children with urinary iodine excretion below 100 μg/L is 16.7%. The proportion of children with very low urinary iodine excretion (<20 μg/L) was only 0.2%. Children taking iodized salt at home on a regular basis have a significantly higher urinary iodine (213±123.5 mg/L) that those who do not use it (178.7±110.3 μg/L, p<0.05). All school canteens used iodized salt and 66.1% of households regularly consumed it. The urinary iodine excretion of schoolchildren who used the school canteen was significantly higher (215.8±120.7 μg/L) compared to those not used (195.2±119.6 μg/L, p<0.05).
The results confirm adequate iodine nutrition in our community at the present time and the effectiveness of prophylaxis with iodized salt, but the household consume has not yet been achieved, still considered at-risk population. We need to continue public education campaigns to increase iodine intake in our population.
Section on Molecular Morphogenesis, Laboratory of Gene Regulation and Development, Program in Cellular Regulation and Metabolism (PCRM), NICHD, National Institutes of Health (NIH), Bethesda, MD
Thyroid and Development Thursday Poster Basic
Thyroid hormone (T3) plays an important role in regulating multiple cellular and metabolic processes, including cell proliferation, cell death and energy metabolism in vertebrates. Mis-regulation of T3 signaling is manifested in developmental abnormalities, metabolic defects and even aberrant cell proliferation leading to cancer. T3 also plays a major role in tissue remodeling and organogenesis during postembryonic development throughout vertebrates. We are using T3-dependent intestinal remodeling during metamorphosis of Xenopus as a model to study how T3 governs tissue remodeling. It has been shown that T3 exerts its metamorphic effects through T3 receptors (TR)-mediated transcriptional modulation of downstream genes and that TRs recruit, in a T3-dependent manner, cofactor complexes that can carry out chromatin remodeling/histone modifications to regulate gene expressions. Whether and how histone modifications change during T3-dependent gene regulation during vertebrate development are largely unknown.
Here, we analyzed histone modifications at T3 target genes during intestinal metamorphosis, a process that involves essentially total apoptotic degeneration of the simple larval epithelium and de novo development of the adult epithelial stem cells, followed by their proliferation and differentiation into the more complex adult epithelium.
We demonstrated for the first time in vivo during vertebrate development that T3-induced gene activation is accompanied by the removal of core histones at the promoter region, accompanied by the recruitment of RNA polymerase. Furthermore, we showed that changes in histone modifications during gene activation by liganded TR correlate largely with the hisone activation and repression marks identified through global analyses in mammal cell cultures with at least one major difference.
Our findings suggest that chromatin remodeling plays an important role in developmental gene regulation by T3 in vivo.
Pediatrics, The Hospital for Sick Children, Toronto, ON, Canada
Thyroid and Development Thursday Poster Clinical
Thyroid-deficient rodents and children with early-treated congenital hypothyroidism (CH) demonstrate compromised visual system development. Blasi et al (2008) showed 8–10 year old CH children on functional MRI (fMRI) engaged a distinct neural network from controls reflecting greater reliance on motor areas when solving visuospatial tasks than controls, suggesting more immature visual processing. However, Blasi's study was limited to a single (i.e., dorsal) visual pathway. Thus, we extended this research to compare CH and control adolescents on dorsal and ventral visual pathway fMRI tasks. Since previous research has shown a developmental shift toward a broader more bilateral neural network with greater frontal involvement between childhood and adulthood, we hypothesized controls would show a more adult-like pattern of neural activations and CH, a pattern resembling younger children.
Eight CH and 11 controls (10–16 years) were given in a 1.5 T magnet two fMRI paradigms that engage distinct visual neural pathways. One task involved judging whether differently rotated objects matched in orientation (dorsal) or identity (ventral) and the other, whether they were identical or mirror images (dorsal). Activation patterns were analyzed using the ANCOVA function of SPM-5 software with age and accuracy as covariates of no interest. Critical contrasts were Orientation/Rotation versus Fixation activations and Identity versus Fixation activations.
On orientation/rotation tasks, controls showed a broader more bilateral activation network with greater frontal and parietal involvement than CH, who relied more on subcortical (hippocampus, caudate) regions and more posterior regions than controls. On the identity task, controls engaged both right ventral and bilateral frontal regions more than CH, who showed no evidence of greater motor area involvement.
The difficulty CH show in visuospatial processing may be explained by compromised development of critical brain structures due to circumscribed lack of TH.
Glass brain patterns showing greater frontal activations in controls (left) than CH (right).
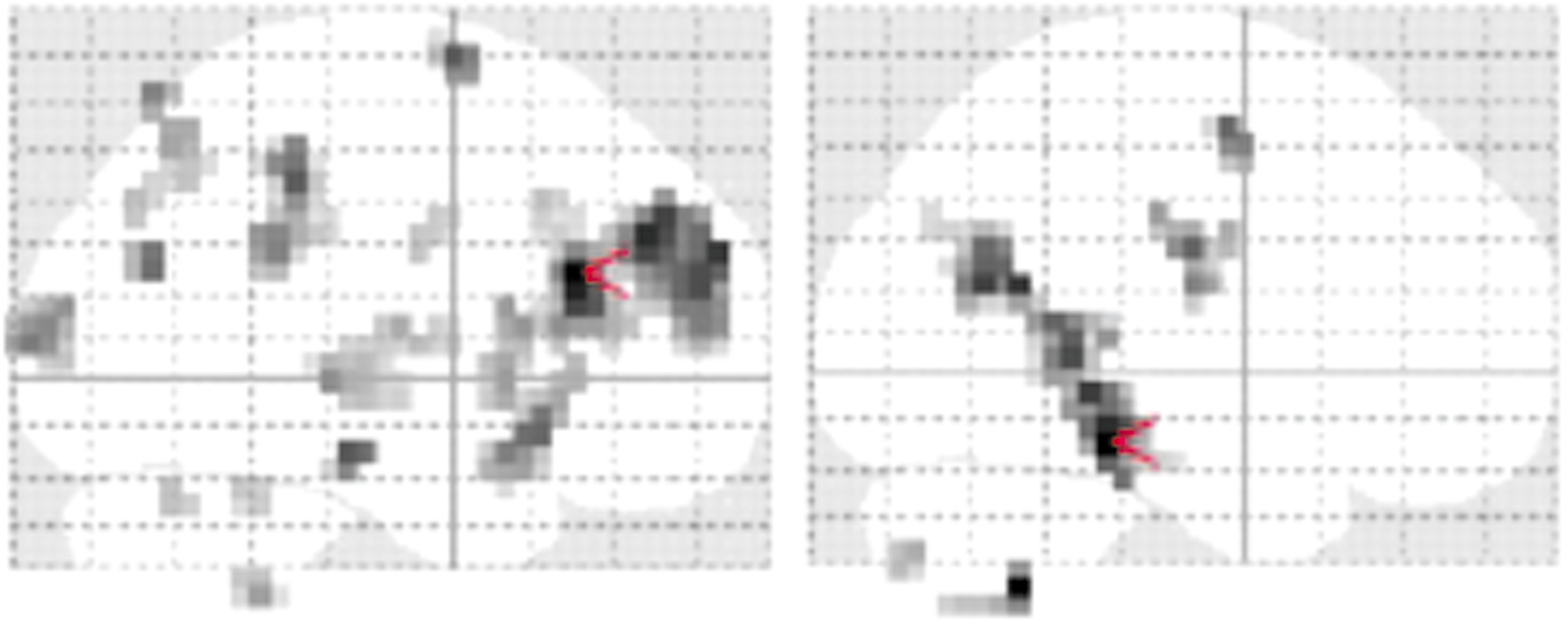
hPTTG Promotes Autocrine Signalling Mechanisms in Thyroid Cells Through Autocrine Pathways of Interaction with Growth Factors
Thyroid Cancer Thursday Poster Basic
The human Pituitary Tumor Transforming Gene (hPTTG) is overexpressed in thyroid cancers; it induces genetic instability and propagates growth through induction of growth factors (GFs). We investigated the pathways of interaction between hPTTG and EGF, TGFα and IGF1 in vitro and in vivo.
Experiments performed in thyroid papillary carcinoma (TPC1) cells, human and mouse primary thyrocytes (HPTCs, MPTCs), transgenic mice with thyroid-targeted hPTTG overexpression (Tg-hPTTG) and PTTG-/- KO mice. TaqMan RealTime-PCR, Western blotting, ELISA.
EGF(5nM), TGFα(5nM) and IGF1(10ng/ml) induced hPTTG protein expression in TPC1 cells (2-fold,4-fold and 2.6-fold, p=<0.01), and in HPTCs (3-fold,2.4-fold and 2-fold, p=<0.01) via MAPK and AKT activation. GF treatment of TPC1 cells following siRNA knockdown of CDC2 or SP1 confirmed that GFs induce hPTTG independently of these reported hPTTG regulators. Transient transfection of HPTCs with hPTTG caused increased EGF (1.7-fold, n=4, p=0.004), IGF1 (1.6-fold, n=5, p=0.002) and TGFα (1.6-fold, n=3, p=0.024) mRNA expression. Treatment of HPTCs with conditioned media from transfected cells resulted in autocrine upregulation of hPTTG protein (4-fold, n=6, p=0.001). This effect was partially abrogated by treatment with the EGFR-inhibitor gefitinib(50μM), the IGFR-inhibitor picropodophyllin(10μM) or TGFα antibody. In vivo evaluation of Tg-hPTTG mice confirmed increased mEGF (2.7-fold, n=3, p=0.012) and mIGF1 (2.0-fold, n=3, p=0.02) thyroid mRNA. Secreted mEGF was elevated in conditioned media from Tg-hPTTG MPTCs (2-fold, n=12, p=0.005). Further, PTTG-/- KO mice showed reduced mEGF thyroid mRNA expression (0.4-fold, n=4, p=0.001). Unexpectedly, 6-week-old Tg-hPTTG mouse thyroids exhibited reduced weight (0.86-fold, p=0.005) and lower cyclinD1 (0.59-fold, p=0.015) and PCNA protein expression (0.61-fold, p=0.021).
hPTTG is involved in autocrine signalling mechanisms with GFs in the thyroid, where aberrant control of these pathways may enhance tumor development. Interestingly, hPTTG overexpression also represses proliferative pathways through inhibition of mitosis. Further elucidation of these complex interactions may provide novel therapeutic targets for the prevention of thyroid tumor growth and progression.
Clinical and Experimental Medicine, University of Birmingham, Birmingham, United Kingdom
Thyroid Cancer Thursday Poster Basic
PBF is a proto-oncogene implicated in the aetiology of thyroid cancer. PBF binds to several proteins, including PTTG and NIS, but its full function is unknown. Understanding the range of interactions PBF has within thyroid cells is therefore vital; these were explored by tandem mass spectrometry (MS/MS), which relies on the predictable fragmentation pattern of an amino acid chain to identify the proteins present in a sample.
K1 and TPC1 papillary thyroid cancer (PTC) cells transfected with HA-tagged PBF were lysed and immunoprecipitated with an anti-HA antibody, before being passed through MS/MS (n=4). 2587 proteins were identified. Those appearing in vector-only controls and those isolated by only 1 peptide in a single run were eliminated.
Ten proteins were stratified as being most likely to interact with PBF. Cortactin, an Src substrate, was identified by 8 peptides, as were FAK2 (2 peptides) and the serine/threonine kinases cMos (1 peptide, 3 runs) and SMG (9 peptides). Thyroglobulin was identified in all runs by 6 peptides. The Src family tyrosine kinase Lyn was identified by 2 peptides in the TPC1 immunoprecipitant but not the K1. This was supported by Western blotting, where K1 cells were shown to have a low expression of Lyn compared to TPC1 cells. Binding to FAP, CIT, ARAP, UACA and was also apparent. Preliminary studies using pull down assays and co-immunoprecipitation have supported the MS/MS findings for Src and on-going studies are seeking to validate the remaining results in an in vivo context.
We have recently identified PBF as a phosphorylated protein and interaction with Lyn, cMos and SMG may be critical to PBF phosphorylation. Given that PBF-transgenic mice demonstrate macro-follicles, the potential interaction between PBF and thyroglobulin may provide a mechanism for this phenotype. We are now validating these interactions, and evaluating their function alongside PBF in thyroid cancer.
Hypoxia-Inducible Factor 1α (HIF-1α) Induces Epithelial-Mesenchymal Transition (EMT) in Thyroid Cancer Cell Lines
Thyroid Cancer Thursday Poster Basic
Hypoxia-inducible factor 1α (HIF-1α) is upregulated by hypoxia and oncogenic signalling in different types of human cancers. HIF-1α activation promotes tumor progression and metastases and have the potential of modulating the activity of major epithelial-mesenchymal transition (EMT)-triggering. But, HIF-1α, its regulation and function in thyroid carcinomas are still unknown.
Three human thyroid cancercell lines, TPC-1, FTC133, and FRO were used in this study. We examined the effects of overexpression or knockout of HIF-1α on cell proliferation, migration, and invasion in thyroid cancer cell lines. Western blots were performed to determine possible mechanisms of EMT.
In vitro studies revealed a functionally active HIF-1a pathway in thyroid cells with transcriptional activation observed after hypoxia or overexpression. Hypoxia or overexpression of HIF-1α promotes epithelial-mesenchymal transition (EMT) and metastastic phenotypes in thyroid cancer cell lines. Also, HIF-1 regulates the expression of GLUT-1, TWIST, Vimetin, Slug, and E-cadherin. However, siRNA-mediated repression of HIF-1α in thyroid cancer cell reversed EMT and metastastic phenotypes.
Our study suggest that hypoxia and/or HIF-1 induces cell proliferation, EMT and metastasis through the regulation of various EMT regulators.
Molecular Virology, Immunology, & Medical Genetics, The Ohio State University, Columbus, OH
Thyroid Cancer Thursday Poster Basic
Carney Complex (CNC, OMIM #160980) is a dominantly inherited tumor syndrome characterized by spotty skin pigmentation and endocrine overactivity. CNC is caused by inactivating mutations in PRKAR1A which encodes the type 1a regulatory subunit of the cyclic-AMP dependent kinase (Protein Kinase A, PKA). A defining feature of CNC is the presence of thyroid nodules and/or cancer, which are observed in approximately 25% and 5% of patients, respectively. Mutations in PRKAR1A have also been identified in patients with sporadic thyroid cancer, indicating a central role for PKA in thyroid tumorgenesis.
In order to elucidate the mechanism by which overactive PKA elicits thyroid tumor formation, we have generated a mouse model harboring a thyroid specific deletion of Prkar1a.
At one year of age, the thyroid glands of these animals are grossly enlarged; pathologically, all animals exhibit follicular thyroid adenomas, with 43% of animals developing follicular thyroid carcinoma (FTC) (Figure 1). Ultrasound imaging revealed that the thyroids of these animals are significantly enlarged beginning as early as 3 months of age. Serum analyses showed that these animals are hyperthyroid, indicating that these tumors are secretory. Interestingly, these tumors do not show activation of the PI3K/AKT or ERK pathways, but do exhibit an increase in phosphorylated Stat3, suggesting that the mechanisms of tumorgenesis in the context of dysregulated PKA are distinct from that in previously described models of FTC. Microarray analyses suggest that altered regulation of transcription by the steroid hormone related receptor family may be involved in tumorgenesis. In vitro experiments with primary cultures of these tumors indicate that suppression of Stat3 inhibits cell growth, highlighting the potential importance of the JAK/STAT pathway in this model.
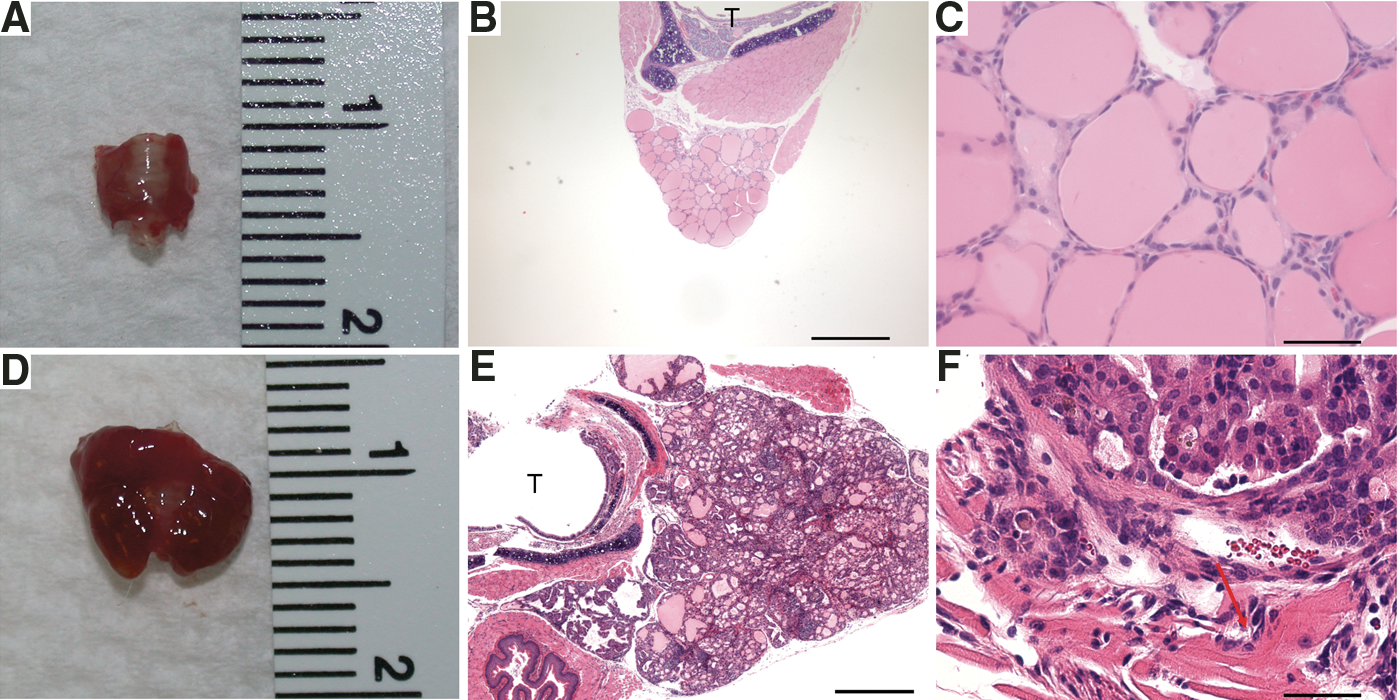
Thyroid specific ablation of the CNC gene, Prkar1a, results in hyperthyroidism and FTC.
This study demonstrates that loss of Prkar1a in the murine thyroid leads to hyperthyroidism and follicular adenoma and carcinoma formation. The model of FTC described here adds to our understanding of the molecular mechanisms involved in FTC development and may help guide the development of new therapies for not only the rare CNC patients, but also for those with sporadic thyroid cancer.
Thyroid Cancer Thursday Poster Basic
Anaplastic thyroid cancer (ATC) is commonly characterized by activation of the mammalian target of rapamycin (mTOR) signaling, which is involved in regulation of cell growth. The AMP-activated protein kinase (AMPK) signaling pathway down-regulates mTOR activity. The anti-diabetic drug metformin reduces mTOR activity and inhibits growth of a variety of cancers in an AMPK dependent manner. We examined the effects of metformin on ATC cell growth and AMPK, mTOR and PI3K/Akt signaling.
Human ATC cells lines (SW1736, C643) were treated with metformin (100 μM−5 mM) and specific AMPK inhibitor compound C (10 μM). Cell growth was examined using Vi-CELL™ Cell Viability Analyzer. The level of protein expression and activation was examined with antibodies against AMPK, pAMPK, Akt, pAkt, mTOR, pmTOR, S6K1, pS6K1, Cyclin D1 and Caspase 3. Expression of 85 molecules involved in regulation of cell growth and proliferation was assessed using rt PCR plates.
Metformin (5 mmol, 72 hrs) inhibited growth of SW1736 and C643 ATC cells. Growth inhibitory effects of metformin were associated with pAMPK induction and down-regulation of pmTOR and its downstream target S6K1 in both ATC cell lines. Inhibition of proliferation was associated with down-regulation of Cyclin D1 in SW1736 and up-regulation of p53 in C643 cell lines. These effects were reversed by AMPK inhibitor (compound C). Expression of apoptotic markers BAX, BCL2 and cleaved caspase-3 was unaffected by metformin. Interestingly, treatment with metformin was associated with activation of anti-apoptotic signaling as documented by activation of pAkt and its downstream target pGSK3β in both ATC cell lines.
Metformin inhibits ATC cells growth through AMPK-dependent down-regulation of mTOR/6SK signaling. At the same time, treatment with metformin is associated with induction of pAkt. These findings suggest that a combination of metformin with an Akt inhibitor might be a potential therapeutic strategy for ATC.
The Role of mTDNA in Oxyphilic and Non-Oxyphilic Thyroid Cancer Cell Lines: A Qualitative and Quantitative Analysis
Thyroid Cancer Thursday Poster Basic
Hürthle cell neoplasms differ from other well-differentiated thyroid tumors by having a large amount of mitochondrial DNA (mtDNA). Because of this structural difference, Hürthle cell malignancies are an excellent model to determine the effect of mtDNA on malignant processes. The role of apoptosis (a tumor suppressing mechanism) in Hürthle cell neoplasms is a paradoxical event in mitochondria. In normal cells, excess reactive oxygen species (ROS) trigger apoptosis by opening the mitochondrial permeability transition pore on the inner mitochondrial membrane. In Hürthle cells the mitochondria are resistant to ROS mediated apoptosis, which favors continued growth of these abnormal cells. The purpose of this study is to demonstrate qualitative or quantitative differences in mtDNA function in thyroid cancer cell lines.
4 thyroid cancer cell lines: metastatic oxyphilic Hürthle cell (XTC.UC1), follicular (FTC-133), non-oxyphilic (WRO), and papillary (TPC-1) and 2 human fibroblast cell lines (HFF, Hs27) were cultured in media. Cobalt chloride was used to simulate hypoxia and ROS production was detected using the H2DCFDA-AM fluorescent probe. Relative quantitation of mtDNA was performed using rt-PCR. Mitochondrial membrane potential (MMP) was assessed using TMRM, a cationic fluorescent probe that accumulates in active mitochondria.
Significantly greater ROS production was found in the XTC.UC1 cell line as compared to the TPC-1 and WRO cell lines (p<0.003). Alternatively, the PCR quantitation of mtDNA demonstrated no difference between the XTC.UC1 and WRO cell lines as measured by the mtDNA versus nuclear DNA ratio (p>0.05; NS). MMP was high in the XTC.UC1 cell line in contrast to minimal activity in the WRO, FTC-133 and Hs27 cell lines as measured by fluorescence.
The oxyphilic XTC.UC1 thyroid cancer cell line demonstrates high levels of ROS activity along with a high MMP with no difference in mtDNA copy number as compared to non-oxyphilic thyroid cancer cell lines. Oxidative stress produced by high ROS activity coupled with high MMP levels, rather than the absolute number of mitochondria may explain the malignant differences between oxyphilic and non-oxyphilic thyroid cancer cell lines.
Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN
Thyroid Cancer Thursday Poster Clinical
Thyroglobulin (Tg) and anti-thyroglobulin autoantibodies (TgAb) show mutual interference in their respective immunoassays. The need of performing a TgAb measurement with every Tg test, to rule out false low Tg results due to TgAb interference, is well recognized. By contrast, the effect of Tg on accurate measurements of TgAb levels is not widely appreciated. The objective of this study was to determined Tg interference in the following TgAb assays: Beckman Coulter, Roche, Siemens-Centaur, and Siemens-Immulite.
Two immunometric (Beckman Coulter and Siemens-Immulite) and two competitive (Roche Elecsys and Siemens-Centaur) immunoassays were compared. TgAb negative samples with a range of different Tg concentrations were tested with these TgAb assays to identify potential Tg interference.
While there was poor numerical correlation between the TgAb assays (r2 ranges 0.09–0.47), they showed reasonable categorical agreement with each other (67–100% concordance) for samples with Tg levels <2000 ng/mL, using clinically validated cut-offs for TgAb positivity (Immulite 20 IU/mL, Centaur 44 IU/mL, Roche 22 IU/mL, and Beckman Coulter 4 IU/mL). The Beckman and Immulite assays remained unaffected by Tg concentrations >2000 ng/mL. However, the Roche assay showed significant differences to the two immunometric assays in these samples, with apparent increases in TgAb levels that correlated with the Tg concentrations (r2=0.99). The Centaur assay showed a similar TgAb increase that was Tg concentration dependent.
TgAb competitive assays are more susceptible to Tg interference than immunometric assays. In patients with a high level of Tg, the TgAb result might be falsely positive/elevated due to this interference. While these false elevations are unlikely to result in misdiagnosis of a recurrent or persistent disease, they might cause confusion and may trigger unnecessary additional tests.
Papillary Thyroid Carcinoma: Genetic Alterations Along RET/RAS/RAF and PI3K/AKT Pathways Correlate with a Specific Gene Expression Profiling and Reveal Dual Mutations Along MAPK Pathway
Thyroid Cancer Thursday Poster Clinical
Papillary Thyroid Carcinoma (PTC) is the most common type of endocrine malignancy. Mutations or rearrangements in genes coding for effectors along the MAPK pathway, are central for its malignant transformation. BRAF V600E mutation is the most common genetic event followed by RET rearrangements, and are mutually exclusive in most series described so far. Moreover, a distinct gene expression is associated with the activation of these oncogenes, which may account for the different biological behavior. It has been suggested that alterations along PTEN/PI3K/AKT may contribute to a more aggressive phenotype. In this study we determined the mutational status of BRAF, RAS and PIK3CA, the prevalence of RET/PTC 1–3 and the expression of PTEN in a series of PTC (n=118) and correlated with expression of genes involved in iodine metabolism (NIS, TSHR, TPO, TG and PDS) and glucose transporters (GLUT1 and GLUT3) and clinical-pathological findings.
Nested RT-PCR was used to identify the RET/PTC isoforms. Quantitative PCR was used to investigate gene expression. Gene mutation was investigated by direct sequencing.
We identified a high prevalence of BRAF V600E (48%) and RET/PTC rearrangements (45%). Unexpectedly, co-occurrence of the mutations was identified in a high number of cases. Although BRAF, RAS and RET/PTC convey signals along same pathway, expression signatures in our analysis showed differences between these effectors. BRAF V600E is associated with lower expression of all genes involved in iodine metabolism and increased expression of glucose transporter genes. RET/PTC shows different pattern of gene expression. Although alterations along PI3K/AKT were rarely found, PTEN expression was lower in BRAF-mutated samples. To investigate the underlying mechanism associated with mutational status in the sporadic PTC, we investigated the expression of enzymes associated with ROS production in thyroid (DUOX1, DUOX2 and NOX4). No association has been found between mutations and DUOX expression.
In summary, the molecular signatures in our analysis may explain the clinical behavior of PTC with BRAF V600E or RET/PTC rearrangement. The acknowledgment of the presence of dual mutation may have important clinical implications.
Otolaryngology & Head-Neck Surgery, Chosun university hospital, Gwangju, Republic of Korea
Thyroid Cancer Thursday Poster Clinical
BRAF V600E is a molecular biomarker of papillary thyroid cancer. We developed an intra-operative molecular diagnostic system of BRAF V600E using direct high resolution melting (HRM).
The 96 patients with thyroid nodule suggesting papillary thyroid cancer by fine needle aspiration biopsy were enrolled in the study. After resection of thyroid lobe with suspicious nodule, surgeon excised each part of suspicious region. Thyroid tissue was placed in microcentrifuge tube containing rapid RBC lysis solution. After tissue homogenization, each lysate was washed and supernatant was discarded. After resuspension, we measured a turbidity of lysate using a spectrophotometer for estimation of template quantity. After adjusting absorbance of lysate, the lysate was repeatedly lysed by bead beating for 2 min. The crude lysate was used directly in the PCR. Direct HRM with the BRAF primers were performed by direct PCR buffer system. We also compare this HRM assay to sequencing and restriction fragment length polymorphism (RFLP) using purified DNA.
Positivities of BRAF V600E in cancerous region were 58/96 (60.4%), 45/96 (46.8%), and 59/96 (61.5%) in direct HRM, sequencing with cutoff of 15%, and RFLP, respectively. Total experiment time was only 50 min.
Direct HRM for intra-operative detection of BRAF V600E is a rapid, reliable, and economic technique.
Translational Research Laboratory, Gustave Roussy Institute, Villejuif, France
Thyroid Cancer Thursday Poster Clinical
Medullary thyroid carcinoma (MTC) could occur either as resectable localized tumors or as refractory metastatic tumors. Like many other cancers, these disparities of agressiveness could be explained by differences of molecular profiles. Until now, the only abnormalities described in MTC were activating mutations in the RET oncogene, leading to an increase in proliferation of C-cells. Recently, Leite et al. have reported mutations in exons 2 and 3 of RAS genes family, in RET wild-type tumors [1].
In order to explore this type of mutations in our cohort of tumors, we analyzed by direct Sanger sequencing BRAF (exons 11 and 15), KRAS (exons 2, 3 and 4), HRAS (exons 2 and 3) and NRAS (exons 2 and 3) genes in a collection of 33 clinically well-defined frozen-tumors, collected at the Gustave Roussy Institute.
The analysis did not show any mutations in BRAF or NRAS genes and none of the 20 tumors carrying a RET mutation has shown any other abnormality. However, amoung 13 RET-negative samples, 7 were mutated in KRAS or HRAS (4/13 and 3/13 samples respectively). Overall, only 6 out of 33 tumors did not harbor any mutation neither for RET nor for RAS genes. Interestingly, 2 of 4 KRAS mutations were located in exon 4, at codon 146 (p.Ala146Val). According to our knowledge, KRAS exon 4 mutation was not previously reported in MTC. Nevertheless, this variant has already been associated with resistance to targeted therapies in colon carcinomas.
Thus, at the sight of the results obtained in our collection of MTC, it seems important to search for mutations in exons 2, 3 as well as exon 4 of RAS genes in non-RET mutated tumors. In addition, since the GTPases encoded by these genes are located in the signaling pathway downstream of tyrosine kinase receptors, these mutations could explain the resistance to RET inhibitors—targeted therapies recently developed for MTC treatment—observed in some patients.
Metastatic Follicular Thyroid Cancer to Iliac Bone 9 Years After Total Thyroidectomy: A Case Report
Thyroid Cancer Thursday Poster Clinical
Bone metastases from differentiated thyroid cancer occur in 2–13% of patients. They are more frequent in follicular thyroid cancer compared with papillary thyroid cancer and are generally diagnosed in those with known thyroid cancer. Here, we report a case of metastatic follicular thyroid cancer 9 years after total thyroidectomy for presumed benign disease.
A 67-year-old Caucasian female with history of thyroidectomy in 2002 for a large cold nodule in the setting of Graves' presented with a 6 month history of left hip pain and swelling. MRI of the pelvis showed large complex mass arising from the superior aspect of left ilium and extended into the left hemisacrum and soft tissues measuring 12.6×11.7×10.0 cm. PET scan revealed a hypermetabolic mass at left bony pelvis with no evidence of any other foci. Presumptive diagnosis was chondrosarcoma. She underwent CT-guided needle biopsy of left iliac mass. Pathology revealed thyroid tissue consistent with metastatic follicular thyroid carcinoma. The tissue was composed mostly of medium-sized follicles filled with colloid. The nuclei were mildly enlarged and hyperchromatic and showed only rare nuclear grooves. Her pathology report from 2002 was obtained and reported: right adenomatous hyperplasia and follicular adenoma with extensive fibrosis and calcification and left adenomatous hyperplasia without evidence of capsular or vascular invasion. She has no history of radiation exposure or family history of thyroid cancer.
The thyroglobulin level was higher than 15,000 ng/mL with the thyroglobulin antibody being negative. She received palliative external beam radiation to the tumor and she was scheduled for bisphosphonate infusion and radioactive iodine treatment.
This is a rare case of metastatic follicular thyroid cancer presented as a large iliac mass 9 years after total thyroidectomy for pathology reported benign disease. Although the initial thyroid pathology may have been overlooked for invasive features (vascular and capsular invasion), there are follicular variant of papillary thyroid cancer reported (FVPTC) that presented similarly. In conclusion, the aggressiveness of thyroid cancer is not always predicted by pathology.
Thyroid Tumors of Uncertain Malignant Potential with Concurrent Papillary Thyroid Cancer: A Report of 2 Patients
Thyroid Cancer Thursday Poster Clinical
The term thyroid tumors of uncertain malignant potential (TT-UMP) has been proposed for a subgroup of follicular-patterned thyroid tumors for which benign or malignant potential cannot be assessed with certainty. The clinical behavior of these tumors is not well understood. We describe the clinical course of two patients with the diagnosis of TT-UMP and co-existing micro-papillary thyroid carcinoma (PTC).
Case report of two patients with TT-UMP and PTC.
Patient 1: A 54 yo female was referred to thyroid clinic for a right-sided nodule measuring 3.8×2.6×2 cm in size with micro-calcifications. She was euthyroid and underwent fine needle aspiration (FNA) of the nodule which showed features of PTC. She underwent total thyroidectomy with one lymph node (LN) excised. Pathology showed incidental micro-PTC, 0.1mm in the left lobe, TT-UMP in larger right-sided nodule 3.4×2.1×1.8 cm and a benign LN. Due to a large index lesion and concurrent PTC, she received low-dose 41 mCi of I-131 therapy after rhTSH stimulation. Post-ablative whole body scan (WBS) showed increased activity in the thyroid bed and in the midline upper chest consistent with mediastinal malignant LN or substernal extension of the thyroid. Patient 2: A 51 yo female was seen in thyroid clinic for a right-sided nodule 3.4×2.6×3.7 cm with mixed echogenicity and multiple calcifications. Sonography showed two right-sided pathological LN's. FNA of the nodule showed follicular cells with focal atypia and FNA of the LN was benign. She had a total thyroidectomy with right level IV LN excision. The 3.2 cm right index lesion was found to be a TT-UMP. An incidental 0.2mm micro-PTC was found on the left along with a benign LN. She was treated with 45.4 mCi of I-131 after rhTSH stimulation. The WBS showed intense uptake in the thyroid bed and in a regional LN.
Micro-PTC and TT-UMP are regarded as low risk neoplasms. However, we report two cases where the co-existence of these two tumors was associated with extra-thyroidal disease on initial post I-131 WBS.
Clinical Ethics Practice Guidelines for Thyroid Disease
Thyroid Cancer Thursday Poster Clinical
Clinical ethics refers to ethical dilemmas that arise in the patient-care setting. Clinical ethics dilemmas are distinct from research ethics issues (which revolve around protocol design and data sharing) as well as professional ethics issues (which revolve around disclosure of conflicts of interest and professional integrity). A variety of medical professional societies have included clinical ethics expertise on clinical practice guidelines committees, or specific clinical ethics content in subspecialty practice guidelines. In the field of endocrinology, reproductive medicine and pediatric endocrine diseases routinely involve clinical ethics expertise.
This presentation will review the areas in thyroid disease where clinical ethics content or guidelines are necessary. It will report on what specific or proposed clinical ethics guidelines in thyroid disease do exist in either the peer-reviewed literature or in thyroid disease practice guidelines published or in press.
In the field of thyroidology, special clinical ethics issues arise in different clinical contexts. Autoimmune thyroid disease raises different clinical ethics issues than thyroid cancer. However, each type of thyroid cancer raises unique and distinct clinical ethics issues and dilemmas. The clinical ethics dilemmas that present in inherited medullary thyroid cancer surrounding genetic screening are not the same as in thyroid cancers that respond well to radioactive iodine. The ethical dilemmas that present in poorly differentiated thyroid cancers are not the same that present in well-differentiated thyroid cancers, where clinical disagreement over what constitutes beneficent care for patients exists. Additionally, new clinical ethics dilemmas are resulting from drug and medical isotope shortages, as well as nuclear disasters.
Despite the prevalence of clinical ethics dilemmas in thyroid disease, clinical ethics guidelines specific to the thyroid disease context are notably absent. Clinical ethics expertise can provide morally sound frameworks for (a) the nuances and complexities of diagnosis and treatment; and (b) allocation of resources in situations where the demand is greater than the supply.
Division of Endocrinology and Metabolism, Mayo Clinic, Jacksonville, FL
Thyroid Cancer Thursday Poster Clinical
Thyroid cancer is increasing in incidence, partly due to early detection from imaging performed for unrelated reasons. Differentiated thyroid cancer (DTC) has an excellent prognosis requiring long term surveillance achieved with serum thyroglobulin (Tg) (indicating residual/recurrent disease or thyroid bed remnant) and neck ultrasonography (US) to detect cervical lymph nodes, the most likely location for recurrences. To increase the sensitivity of detection, recombinant human TSH (rhTSH) stimulated Tg values (Tg-stim) have been used.
Utilizing an automated chemiluminometric assay with functional sensitivity of 0.1 ng/mL, we identified 163 patients status post thyroidectomy and one or more radioactive iodine treatments, who had Tg on L-T4 (Tg-supp)<0.1 ng/mL and rhTSH stimulated thyroglobulin test within 60 days. Neck US was performed in all but two patients, with fine needle aspirates on suspicious lesions.
Post rhTSH stimulation, Tg remained <0.1 ng/mL in 93 (57%), increased to 0.1–0.5 in 57 (35%), >0.5–2.0 in 9 (6%) and >2.0 ng/mL in 4 (2%) patients. Serial Tg-supp levels (n=497) were obtained in 131 patients followed up to 8.8 (mean=3.6) years. Serial neck US were performed on 161 patients. When suspicious sonographic features were observed fine needle aspirates were done for cytology. FNAs were performed in 13 patients, 6 had cytology suspicious for persistent/recurrent disease. All 6 positive FNAs were identified around the time of the initial rhTSH test. No patient with unremarkable US at the time of rhTSH testing developed an abnormality leading to a suspicious FNA subsequently. Recurrent/persistent disease was detected in one patient with Tg-stim >2.0 ng/mL, one with Tg stim >0.5–2.0 and in 4 whose Tg-stim was ≤0.5 ng/mL. All local recurrences were detected by US. Only one high risk patient with Stage 3 Hürthle cell carcinoma, who had an undetectable Tg-stim, had distant disease detected by chest x-ray.
We believe that in patients with DTC whose T4-suppressed serum Tg is <0.1 ng/mL, long-term monitoring with annual Tg-supp and periodic neck ultrasound may be adequate. Therefore rhTSH testing may not be needed as, in our experience, the results do not impact or change management.
Medicine, University of Toronto, Toronto, ON, Canada
Thyroid Cancer Thursday Poster Clinical
Decision-making about adjuvant radioactive iodine treatment (remnant ablation) can be complex. The impact of the process of this decision-making on subsequent regret in thyroid cancer survivors is not known. We explored regret in patients with a history of early stage papillary thyroid carcinoma, relating to the decision to accept or reject adjuvant radioactive iodine treatment.
We recruited patients with a recent diagnosis of early stage papillary thyroid carcinoma, in whom treatment decisions on adjuvant radioactive iodine had been finalized. We asked participants who made the final decision on radioactive iodine treatment, and they completed a Decision Regret Scale questionnaire (scores varying from: 0 to 100, 100=maximal regret). We explored the relationship between decision regret and: a) degree of involvement in decision-making, and b) receipt of radioactive iodine treatment.
We included 44 individuals, more than half of whom received adjuvant radioactive iodine treatment (26/44). Participants reported that the final treatment decision was made by the following: patient and doctor (52.3%, 23/44), completely the patient (27.3%, 12/44), or completely the physician (20.5%, 9/44). Decision regret was generally low (mean=22.1, standard deviation [SD], 13.0). Decision regret significantly differed according to who made the final decision: the patient (mean 19.0, SD11.3), patient and doctor (mean=19.5, SD 7.4), and the doctor (mean 32.9, SD 20.37) (F=4.569, degrees of freedom=2, 41, p=0.016). There was no significant difference in decision regret between patients who received radioactive iodine and those who did not (mean difference=2.5, 95% confidence interval=10.6, 5.6, p=0.540).
Thyroid cancer patients who reported being involved in the final treatment decision on adjuvant radioactive iodine, had less regret than those who did not.
nuclear medicine, AZ Turnhout, Turnhout, Belgium
Thyroid Cancer Thursday Poster Clinical
Definite preoperative definite diagnosis is needed in lower cervical or upper mediastinal mass of suspected (para)thyroid origin. Ultrasound guided (US)FNAC may be impossible. Cytology may be equivocal, e.g. in medullary thyroid carcinoma (MTC), parathyroid tissue.
US-FNAC of masses may be technically impossible e.g deep in the neck or in the upper mediastinum (too deep; presence of bone, vessels, trachea).
3 case reports with applications of both easy EBUS-FNAC and QBA:
Survey of 3 Case Reports with EBUS-FNAC
In neck and upper mediastinal masses of suspected (para)thyroid origin: 1. EBUS adds to US for FNAC. A node/mass may be anatomically out of reach for US-FNAC. EBUS-FNAC samples are of excellent quality. 2. QBA of the rinsing fluid of the FNAC-syringe adds to cytology and ICC, pointing to MTC (CCT and CEA), parathyroid (PTH), or thyroid or thyroidCa (TG). QBA may help to counter: a) sampling error b) equivocal cytology (parathyroid, MTC) c) technically bad smears (cystic component; bloody; drying artefacts).
Thyroid Cancer Thursday Poster Clinical
Hypocalcaemia is a recognized complication of total thyroid surgery. There is however no international agreed consensus on calcium monitoring post thyroid surgery, despite there being several recent studies on PTH and Ca level checks as predictors for development of hypocalcaemia (Pfeider et al. 2009 & Jumaily et al. 2009). Mehanna et al. 2010 suggested that this is due to a lack of an agreed definition amongst clinicians of when treatment for hypocalcaemia should be initiated. The aim of our study was to look at calcium trends and try to devise guidance for calcium monitoring that could be translated to different units in different countries.
A retrospective 7 year review of all patients having total thyroid surgery in a university teaching hospital from 2004 to 2010. Data was collected regarding demographics, the type of operation, histopathology, calcium levels and administration of calcium supplements, and analysed using the latest version of SPSS.
106 patients had total (69%) or completion (31%) thyroid surgery with 66% (71) of surgery done for malignancy. 70% (74) of these patients developed post-operative hypocalcaemia with 30% (32) requiring treatment with supplements. A drop in calcium on the same post-operative day of less than 0.11 from the pre-operative value meant that patient would not develop hypocalcaemia needing treatment (P=0.01). None of the 62 patients with normal calcium levels on post-operative day 1 developed hypocalcaemia needing treatment.
Same post-operative day calcium checks are useful in predicting calcium drop when compared to pre-operative values and can be useful when doing same day total thyroid surgery to determine need for outpatient calcium level monitoring or replacement. Post-operative day 1 (24 and 36 hour check) is when a significant calcium drop is most likely to instigate the need for supplementation. If the calcium levels are in range at these times or not dropping then the patient is safe to be discharged without calcium supplementation. In view of this evidence patients should not remain in hospital post-operatively for prolonged periods for calcium monitoring or be routinely discharged on calcium supplements.
Withdrawn
Institute of Cancer Epidemiology, Danish Cancer Society, Copenhagen, Denmark
Thyroid Cancer Thursday Poster
Thyroid cancer incidence has increased worldwide during the previous decades. In this nationwide study we aimed to identify the overall incidence of thyroid cancer in Denmark from 1943 to 2008 and incidences of the four main histological types of thyroid cancer from 1978 to 2008.
Data were obtained from the Danish Cancer Registry, which was established in 1943. Reporting of new cancer cases has been mandatory since 1978. From this computerized register, we identified all cases of thyroid cancer from 1 Jan 1943 to 31 Dec 2008. The registry includes information on topography, morphology, date of diagnosis and personal identification number on each patient. It is linked to The National Patient Registry and The Causes of Death Registry to ensure completeness, and coverage is close to 100%. In this study special attention was given to the period after implementation of compulsory iodine supplementation in 2000.
Overall, 1925 men (30%) and 4599 women (70%) were diagnosed with invasive thyroid cancer from 1943 to 2008, with a median age of 59 years. Age-standardised incidence rose from 0.22 to 1.73 per 100,000 in men and from 0.57 to 4.30 per 100,000 in women, with an annual percentage change of 1.3 (95% CI, 1.1–1.6) and 1.4 (95% CI, 1.2–1.6), respectively. The rise was almost exclusively caused by papillary carcinoma, and it was particularly high during the last decade coinciding with commencement of iodine supplementation. Mortality from thyroid cancer was not increased during the same period (previous study using the same Registry).
Papillary cancers were responsible for a marked increase in thyroid cancer incidence seen particularly after the introduction of salt iodization, but the rise may both be real and/or artificial, since several factors could be responsible. Thus, both more prevalent use of thyroid imaging, discovering very small tumours, and other factors causing an artificially increased incidence may be responsible, possibly along with known and/or unknown risk factors for thyroid cancer. The lack of increased mortality from thyroid cancer indicates that the increased incidence is most likely accounted for by small non-lethal thyroid cancers.
Surgery, Division of Head and Neck Surgery, UCLA David Geffen School of Medicine, Los Angeles, CA
Thyroid Cancer Thursday Poster Clinical
The optimal management of papillary thyroid microcarcinoma (PTMC) continues to evolve as more studies focus on the disease, treatment, and prognosis. There has been controversy in the thyroid surgical community regarding routine inclusion of prophylactic central neck dissection (PCND) in patients without clinical lymph node metastasis (LNM). Presence of LNM at diagnosis is a well-established significant risk factor for locoregional recurrence and distant metastasis, however the impact on survival is unclear. If predictive factors for LNM could be identified, it would be possible to stratify high-risk from low-risk PTMC patients, which would enable more precise, tailored surgery.
A systematic review of the English language literature published between 2001–2011 identified through the Pubmed database.
Eleven papers were reviewed that analyzed a series of patients with PTMC with specific attention to identifying factors that predict LNM. The incidence of cervical LNM ranged from 3–40% with the most common site being the central compartment. Consistently significant predictors of cervical LNM include: capsular invasion (CI), size >5mm, multifocality, male gender, and nonincidental diagnosis with CI being the most commonly identified predictor (6/11 studies). Other predictors that showed weak association were lymphovascular invasion and extrathyroidal extension, while age was an inconsistent factor. Overall survival was excellent in all series, with no studies reporting disease related death at follow up; however, recurrence rates ranged from 0–4.7%.
Cervical LNM is common in PTMC, occurring in up to 40% of cases based on this review. While LNM does not appear to impact overall survival, it can lead to disease relapse and may be addressed by using a decision-making algorithm based on significant risk factors to decide which patients would best benefit from PCND.
Internal Medicine, Asan Medical Center, Seoul, Republic of Korea
Thyroid Cancer Thursday Poster Clinical
The aims of this study were to describe the natural course of patients who had no clinical evidence of disease (NCED) and elevated stimulated thyroglobulin 1 yr after total thyroidectomy and remnant ablation (sTg1), and to evaluate the role of repeated sTg measurement to predict spontaneous biochemical remission (BR, stimulated thyroglobulin <1 ng/ml) or clinical recurrence.
Total 183 patients who had sTg1 greater than 2 ng/ml and NCED were included in this study. All patients had negative I-131 scan and NCED confirmed by neck US, FDG-PET, or chest CT. The second sTg measurement (sTg2) was performed 1–2 years after sTg1. sTg slope was defined as the ratio of sTg2 divided by sTg1. Patients were classified into 4 groups according to sTg1 value as follow; between 2 and 4 (group A), 4 and 10 (B), 10 and 30 (C), and higher than 30 ng/mL (D). Patients were also classified into 3 groups according to sTg slope value as follow; lower than 0.5, between 0.5 and 1, and higher than 1. sTg were measured every 1–2 years until BR or clinical recurrence. We evaluated BR and clinical recurrence-free survival rate according to sTg1 and sTg slope categories.
In patients remained NCED, their serial sTg level generally decreased. Finally, 47% patients in group A, 19% in group B, 10% in group C and no one in group D achieved spontaneous BR. In group A, median time from sTg1 measurement to BR was within 72 months. It took more time for the other patients with greater sTg1 to achieve BR. During follow-up, 31% patients had recurrent disease. Among groups of sTg1 and sTg slope, the group with higher value of sTg1 and sTg slope had a greater clinical recurrence rate (p=0.013 and p<0.001).
This study demonstrated that spontaneous BR is achieved in 47% of patients with sTg1 between 2–4 ng/ml and their median time from sTg1 measurement to BR is within 72 months. sTg1 and sTg slope seem to be a good predictor for BR and clinical recurrence. The repeated sTg measurement is useful method for predicting prognosis.
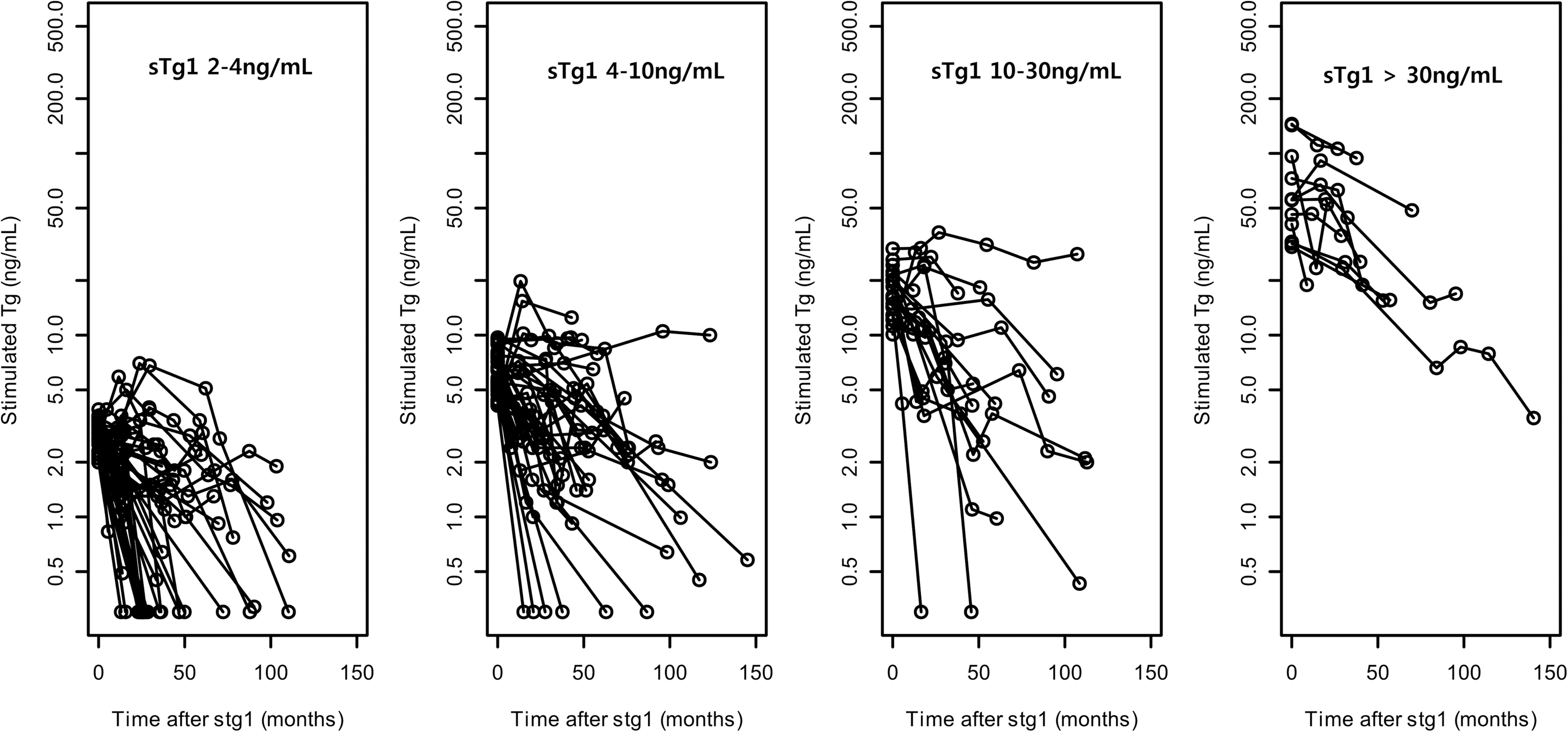
Long-term consequence of elevated sTg in DTC patients who initially underwent total thyroidectomy and remnant ablation.
Thyroid Cancer Thursday Poster Clinical
A 21-year-old Hispanic female with Familial Adenomatous Polyposis (FAP) with a prophylactic colectomy was diagnosed with thyroid cancer at age 16. She underwent total thyroidectomy and radioactive iodine ablation. The original pathology report showed multicentric, macroscopic disease with the larger lesion on the right, classified as tall cell variant of Papillary Thyroid Cancer (TCVPTC).
Five years later she presented to our institution with a new abdominal mass, right paratracheal mass and pathologic neck lymphadenopathy. The abdominal mass was diagnosed to be a desmoid tumor. Fine Needle Aspiration (FNA) of the paratracheal mass was consistent with a metastasis from the primary abdominal desmoid tumor. FNA of the neck lymph nodes was consistent with recurrent PTC. Careful review of the original thyroid surgical pathology slides was consistent with the rare Cribriform Morular Variant of PTC (CMVPTC).
PTC has been identified as one of the rare (1–2%) extracolonic manifestations of FAP for more than 40 years. Young females with FAP have 160 times greater risk of thyroid cancer than the general population. CMVPTC is specifically associated with FAP, and its diagnosis should alert physicians to the diagnosis of FAP, as thyroid cancer can precede other manifestations of FAP. The classic description of CMVPTC is a combination of cribriform, follicular, papillary, trabecular, solid and spindle patterns with interspersed squamoid islands called “morules”. Morule cells have a peculiar nuclear clearing caused by biotin accumulation. Characteristically, both nucleus and cytoplasm stain positive for β-catenin. Colloid is absent. The differential diagnosis includes TCVPTC, columnar cell carcinoma and poorly differentiated carcinoma. CMVPTC can be suspected in FNA samples. APC mutations, as well as either ret/PTC-1 or ret/PTC-3 rearrangements have been reported in CMVPTC. CMVPTC often has a similarly good prognosis as sporadic PTC, although aggressive cases have been reported.
Cribriform Morular Variant of PTC is an excellent example of clinical, morphologic, immunohistochemical and molecular correlation in human cancer.
Surgery, University of Southern California Keck School of Medicine, Los Angeles, CA
Thyroid Cancer Thursday Poster Clinical
Thyroid nodules in pediatric patients may carry a greater risk for malignancy than in adults. Most nodules >1 cm in patients 21 years of age or younger may require thyroidectomy for definitive diagnosis. Although clinic based ultrasound (CBUS) has been shown useful in the evaluation of thyroid nodules in adults, its utility in evaluating nodules in the pediatric population remains unclear.
Prospectively collected data of 50 patients ≤21 years who underwent preoperative CBUS and initial thyroidectomy at a single institution were retrospectively reviewed. All CBUS were performed by thyroid surgeons certified in basic and cervical ultrasonography. Preoperative CBUS characteristics of pediatric thyroid nodules were analyzed with respect to final pathology.
Of 50 patients ≤21 years who underwent surgery for a dominant thyroid nodule, there were 45 females and 5 males with an average age of 17.4 years (range: 10–21 years). On univariate analysis, microcalcifications (p<.001), abnormal lymph nodes (P<.001), and taller>wider shape (p=.033) were individual CBUS characteristics predictive of thyroid malignancy. All 9 patients with abnormal lymph nodes on CBUS had malignant disease on final pathology. Multiple thyroid nodules, a cystic component, and echogenicity did not help predict malignancy; regular borders trended towards predicting benignity (p=.066). When the presence of classically malignant CBUS features were analyzed (hypoechoic, irregular borders, microcalcifications, shape taller>wider), having one malignant feature predicted malignancy with an odds ratio of 2.0, while having ≥2 features held even greater significance (p=.004, OR 4.0). All patients with ≥3 malignant features had thyroid cancer on final pathology.
CBUS may be useful in determining malignancy status of thyroid nodules in patients ≤21 years of age. CBUS should therefore be employed as part of a standard, initial assessment of any pediatric patient presenting with a thyroid nodules to help guide further management.
Role of FGRS in Thyroid Tumor Progression and Their Involvement in the Correlation Between Thyroid Cancer and Melanoma
Thyroid Cancer Thursday Poster Clinical
Thyroid cancer is the most common endocrine malignancy. It is known that cancer progression involve dysregulation of growth factors (FGFs) and their receptors (FGFRs) have been identified. In thyroid tumors. In particular, FGFR1 and FGFR3 are expressed in most well differenziated tumors, FGFR4 is predominantly expressed in aggressive tumor types and cells lines, while FGFR2 is the only receptor consistently detected in normal human thyroid tissue and its expression is downmodulated in thyroid cancers and carcinoma cells lines.
The study is conduced on a series of 7963 patient undergoing t.t. in the Department of Surgical Science, Policlinico Umberto I, Sapienza University of Rome, from 1996 to 2011of these patients 1391 had a diagnosis of thyroid cancer.The aim of the study is the evaluation of a possible correlation between FGFR2 expression and progression/prognosis of thyroid cancer, analyzing FGFR2 downregulation in normal thyrocytes, in term of proliferation, differentiation, apoptosis and expression of tumoral markers.
Recent studies have identified an association between cutaneous malignant and thyroid carcinoma. Molecular studies show that TSHR is expressed by cutaneous melanocytic lesions, with higher expression in malignant and premalignant lesions, and that cultured melanoma cells, but not melanocytes, are induced to proliferate by TSH; this suggests that hypothyroidism may promote the development and progression of melanoma.
We will set up a retrospective analysis of FGFR1–4 expression in patients with thyroid carcinoma that have successively developed a melanoma or vice versa, in order to identify differences in FGFR expression in “double positive” patients versus patients affected by only thyroid cancer or melanoma. Since BRAF-activating mutations have been reported in 70% of melanoma cases and in 30–70% of thyroid carcinoma cases, and 10% of melanoma tumors and cell lines harbour loss of function mutations of FGFR2 gene, in this study we will also analyze the correlation between FGFR2 expression and BRAF mutation in patients with thyroid cancer and/or melanoma.
Risk Factors for Neck Lymph Node Metastasis in Papillary Thyroid Microcarcinoma: A Study in 1066 Patients
Thyroid Cancer Thursday Poster Clinical
The surgical management of papillary thyroid microcarcinoma (PTMC), especially regarding the necessity of central neck dissection (CND) remains controversial because evidence doesn't demonstrate that CLND improves locoregional recurrence or survival in PTMC.
In this retrospective cross-sectional study, data from the medical records of 1066 consecutive patients diagnosed with PTMC over a 5 year period at a university-based tertiary care cancer hospital were analyzed.Ipsilateral lobectomy plus prophylactic CLND was performed as the predominant surgical treatment in a US-selected population. Aseries of clinicopathology features and outcome variables were assessed at the time of surgery for the primary tumor. Risk factors of neck lymph node metastasis were identified using binary logistic regression.
Our multivariate logistic regression analysis found male gender, younger age, multifocal lesions, invasion and larger size of the primary tumor (>6mm) to be associated with CLNM; multifocal lesions were associated with the highest risk (OR 4.422, 95%CI 2.943–6.642). Invasive tumor, multifocal lesions and CLNM were associated with lateral cervical metastasis. In patients with a solitary primary tumor, tumor location in the upper third of the thyroid lobe was associated with a lower risk of CLNM and a higher risk of lateral cervical metastases,which may cause a skip metastasis. All patients had a 12 month follow-up and many were followed for a longer period,in the 990 patients who did not undergo total thyroidectomy, only 7 (0.81%) suffered from a malignant recurrence in the contralateral lobe.
Prophylactic CND should be performed in PTMC patients presenting with risk factors. In PTMC patients with a solitary primary tumor, tumor location can assist the evaluation of lymph node metastasis. We recommend multicenter research and long-term follow-up to better understand risk factors and surgical management of PTMC.
Insular Thyroid Cancer: A Population-Level Analyses of Demographic and Clinical Characteristics Associated with Survival
Thyroid Cancer Thursday Poster Clinical
Insular thyroid cancer (ITC) is an uncommon aggressive, poorly differentiated variant. Data on ITC are culled largely from small series. There are no data on the clinico-pathologic features and survival outcomes of ITC patients at a population level.
We used the Surveillance, Epidemiology, and End Results (SEER) database, 1988–2007. Demographic, clinical, and pathologic characteristics of patients with ITC were compared to those with well-differentiated thyroid cancer (WDTC) and anaplastic thyroid cancer (ATC). Disease-specific survival was evaluated. Data analyses were performed using χ2, ANOVA, log-rank tests, and Cox multivariate regression.
There were 115 ITC, 735 ATC, and 50229 WDTC patients in the study. Mean patient age for ITC was 62.1 yrs, compared to 48.5yrs for WDTC and 70.5yrs for ATC (p<0.001). ITC patients were more often male compared to WDTC and ATC (47.8% vs. 24.7% and 37.1%; p<0.001); mean tumor size was 5.9cm, compared to 2.1cm for WDTC and 6.5cm for ATC (p<0.001). Solitary tumors were more likely in ITC compared to WDTC and ATC (80.5% vs. 66.5% and 76.4%; p<0.001). Distant metastases occurred in 31.0% of ITC, compared to 4.7% of WDTC and 56.2% of ATC (p<0.001). Most ITC patients were treated with thyroidectomy (80.9%) and radioiodine (56.5%); 15.7% received external beam radiotherapy. The 5-year disease-specific survival rate was 67.0% compared to 96.8% for WDTC and 9.3% for ATC (p<0.001). After multivariate adjustment, the factors independently associated with survival for ITC were radioiodine (HR: 0.15, 95% CI: 0.04–0.5) and distant metastases (HR: 15.3, 95% CI 3.7–62.2). For patients with distant metastases, those who underwent thyroidectomy and radioiodine/external beam radiation had improved survival compared to those who did not have aggressive treatment.
ITC patients of all stages should be treated with total thyroidectomy, radioiodine and, if necessary, external beam radiation.
Factors Related with Metastasis of Right Retroesophageal Lymph Nodes in Papillary Thyroid Cancer
Thyroid Cancer Thursday Poster Clinical
Right retroesophageal lymph nodes (LN) should be involved in central lymph node dissection (CLND) in patients with papillary thyroid cancer (PTC). But, there is a possibility of injuring to the nerve during the procedure. The purpose of this study was to assess the incidence and factors related to right retroesophageal LN metastasis.
From January 2008 to March 2010, 129 patients were underwent total thyroidectomy with CLND including right retroesophageal LN for PTC. There were 101 women and 28 men whose mean age was 41.6±12.9 years. We retrospectively reviewed these patients. The following criteria were used to study the predictive value of Right retroesophageal LN metastasis : age, sex, tumor size, multiplicity, preoperative LN enlargement, number of central LN metastasis, number of central LN removed, extrathyroidal extension, lateral LN metastasis, capsular invasion and T stage.
26 of 129 patients exhibited nodal metastasis in right retroesophageal LN (20.1%). Metastasis of right retroesophageal LN was associated with large tumor size more than 1 cm (p<0.01), multiplicity (p=0.03), preoperative LN enlargement(P<0.01), metastasis of non-retroesophageal lateral LN (p<0.01) and large number of central LN metastasis (P<0.01) in univariate analysis. With use of multivariate analysis, tumor size (>1cm) and metastasis of non-retroesophageal lateral LN were independent correlates of right retroesophageal LN metastasis.
Right retroesophageal LN may be removed during operation for PTC particularly in patients with tumor larger than 1.00cm and lateral LN metastasis.
Surgery, Wonju College of Medicine, Yonsei University, Wonju, Republic of Korea
Thyroid Cancer Thursday Poster Clinical
There are many clinical pathologic factors and staging systems are used when classifying the severity of thyroid cancer and analyzing a variety of biological characteristics. Identifying these factors that affect the recurrence of papillary thyroid carcinoma and using the staging system that can appropriately reflect the prognosis can be useful in high risk patients by carrying out a proper treatment plan, and in low risk patients by avoiding any unnecessary studies and treatments. With this, this study creates a new staging system through risk model that use clinicopathologic factors, associated with recurrence, checked by preoperative clinical information and imaging study and was compared with other staging systems
A review was conducted of patients who have previously performed thyroidectomy and were able to undergo follow-up sessions between January 1, 1983 and September 31, 2007 at Yonsei University Wonju Medical Center. There were a total of 599 patients.
The Risk model that are associated with the recurrence included six variables abbreviated by age, sex, tumor size, extrathyroidal extension, lymph node metastasis, and distant metastasis. The final prognostic score was defined as New staging system=0.03×age+0.06×tumor size (in centimeters), +0.8 (if male), +0.6 (if locally invasive), +0.6 (if lymph node metastases present), +2.6 (if distant metastases). In comparing the other staging systems, proportion of variation explain (PVE) was calculated for each, and was ranked in order. Out of the seven, New staging system appeared to be the most accurate prognosis predictor with 21.6%. University of Chicago clinical staging system in second with 18.9%. AJCC/UICC TNM staging system in third with 16.7%.
New staging system can predict recurrence very well and has the advantage can use preoperatively. Those patients diagnosed as high risk patients through new staging system should be treated with aggressive surgical treatment, and with close follow-up.
Otorhinolaryngology-Head and Neck Surgery, Pusan National University Hospital, Busan, Republic of Korea
Thyroid Cancer Thursday Poster Clinical
Nodal metastasis of papillary thyroid cancer (PTC) has been known to occur from the central- to lateral lymph node compartments. However, lateral cervical lymph node metastasis (LNM) without central lymph node (CLN) metastasis is not infrequently. This study was designed to investigate the pattern of skip metastasis and to determine the relationship between skip metastasis and clinicopathologic factors.
We reviewed PTC 131 patients who underwent total thyroidectomy with CLN dissection and selective lymph node dissection (SND) between January 2004 and June 2009. Clinical diagnosis of LNM was confirmed by ultrasonography and CT. Tumor location was classified in three areas based on the results of preoperative ultrasonography. We analyzed the relationship between tumor location and nodal metastasis pattern. The relationships between metastasis pattern and clinicopathologic parameters were analyzed.
All skip metastases occurred in patients whose tumors had been on the upper part of the thyroid (P<0.001). Level III lymph nodes were the most frequent site of metastasis, regardless of tumor location. LNM from tumors in the upper portion of the thyroid were relatively common in level II lymph nodes (not significant). Level III lymph nodes (6/9) were the lymph nodes that were most frequently involved in skip metastasis, followed by level II nodes, level IV nodes, and level V.
Primary tumors in the upper portion of the thyroid are closely linked to skip metastasis. Careful preoperative evaluation of lateral cervical lymph nodes is necessary when a tumor is in the upper portion of the thyroid.
Robotic Thyroidectomy via Transaxillary Single Port Approach for Papillary Thyroid Cancers: Preliminary Reports
Thyroid Cancer Thursday Poster Clinical
Recently, various robotic surgical procedures have been performed, and most reports have proved that the application of robotic technology for surgery is technically feasible and safe. The feasibility and safety of robotic thyroid surgery was examined via transaxillary single port approach without gas insufflation.
The study included 54 consecutive patients with papillary thyroid cancer who underwent robot assisted endoscopic thyroid surgery using a gasless transaxillary single port approach by a single surgeon (Y.W.K.) between May 2010 and March 2011 at the department of otorhinolaryngology, Yonsei University College of Medicine.
The actual operating time (console) for 22 hemithyroidectomy (HT) with ipsilateral central compartment neck dissection (CCND) was 47.43 min, and that of 32 total thyroidectomy (TT) with ipsilateral or bilateral CCND was 91.82 min. The amount of postoperative drainage was 224.5 ml, and the duration of drainage was 3.5 days. The postoperative hospital stay was 6 days. Mean primary tumor size was 6 mm. The average number of lymph nodes resected was 5 (range, 1–10). Temporary hypoparathyroidism encountered with twelve patients in the TT group. There were no perioperative complications (hemorrhage, hematoma, seroma, recurrent laryngeal nerve (RLN) palsy, and injury to the adjacent structures, including the trachea and esophagus. One case of temporary brachial plexus injury occurred due to arm positioning.
The technique of robotic thyroid surgery using a gasless transaxillary single port approach is a feasible, safe, and effective method for selected patients with thyroid cancer. The authors suggest that application of robotic technology for endoscopic thyroid surgeries could overcome the limitations of conventional endoscopic surgeries in the surgical management of thyroid cancer.
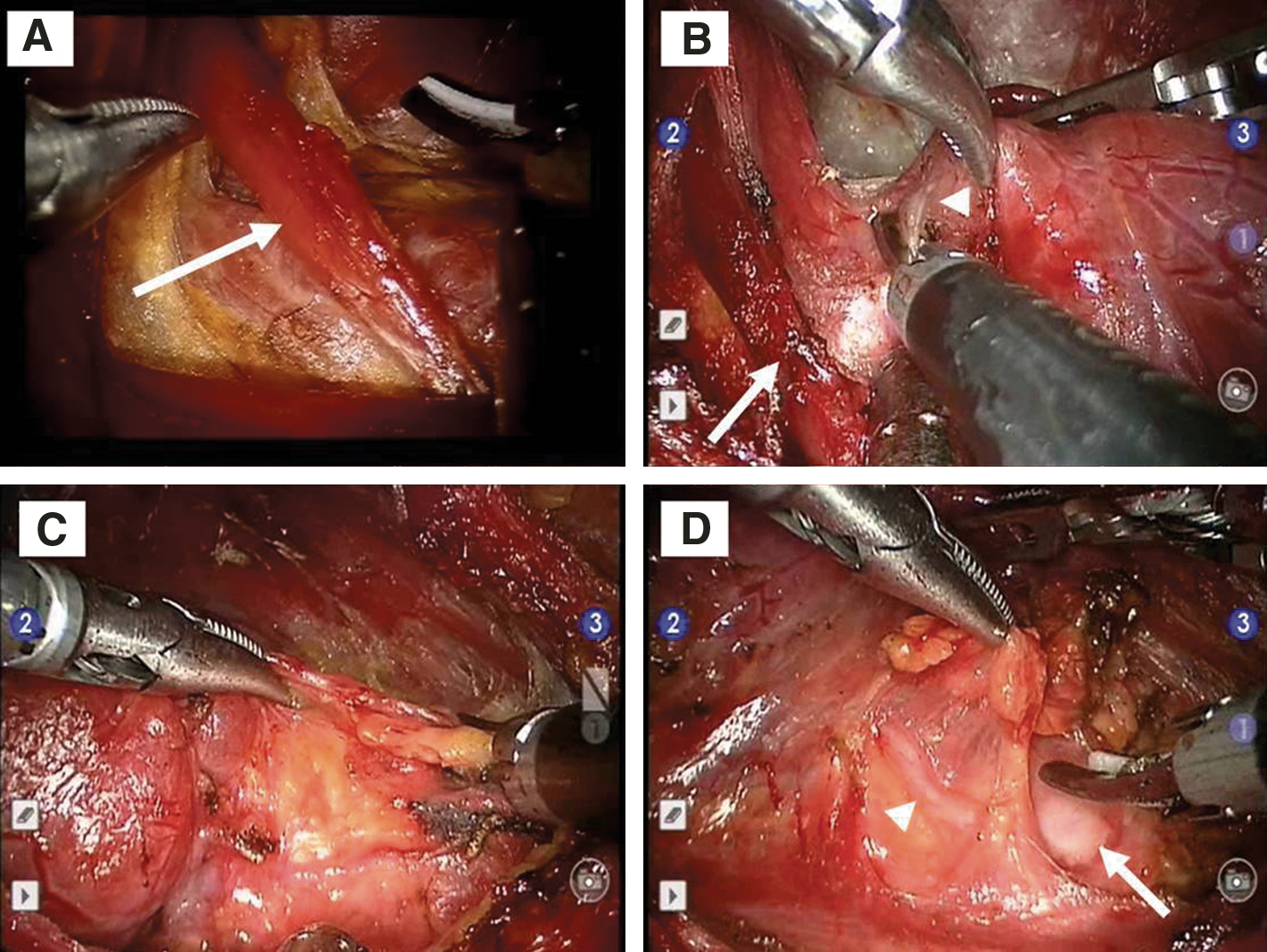
A, Rt. Flap elevation & Omohyoid muscle (Arrow). B, Rt. STA (Arrowhead) & Omohyoid muscle (Arrow). C, Rt. CCND. D, Rt. Trachea (Arrow) & RLN (Arrowhead). STA : Superior thyroid artery, CCND : Central Compartment Neck Dissection, RLN : Recurrent Laryngeal Nerve.
Thyroid Cancer Thursday Poster Clinical
The scope of operations such as a lobectomy or a total thyroidectomy in micropapillary thyroid carcinoma (mPTC) is controversial. In this sense, preoperative assessment of the extrathyroid extension and central compartment lymph node metastasis is very important. However, it is difficult to predict extrathyroid extension and lymph node metastasis in central compartment preoperatively. The purpose of this study is to evaluate the ultrasonographic characteristics of single intraglandular mPTC and to predict extrathyroid extension, central compartment lymph node metastasis and multifocality.
From January 2008 through December 2009, 118 patients with single intraglandular mPTC in preoperative ultrasonography underwent total thyroidectomy with bilateral central neck dissection. The relationship between the preoperative ultrasonographic features and pathologic results of tumor was assessed retrospectively.
In single intraglandular mPTC, extrathyroid extensions, central compartment lymph node metastasis, and multifocality were 24.6%, 43.2%, and 19.5% respectively. Marked hypoechogenicity was significantly correlated with central compartment lymph node metastasis (p=0.033).
It needs a discreet decision making for surgery in single intraglandular mPTC, if ultrasonographic features of primary tumor show marked hypoechogenicity. These results would give an aid to determine the extents of thyroid surgery.
Thyroidology Department, Belarussian Medical Academy of Postgraduate Education, Minsk, Belarus
Thyroid Cancer Thursday Poster Clinical
Thyroid carcinoma is the most common endocrine malignancy. There are still a lot of debates about the reason of increased number of differentiated thyroid carcinoma in young population of Belarus. The aim of the study was to analyze retrospectively clinical data and ultrasound characteristics of thyroid carcinomas in follow up patients of Gomel region of Belarus in dependence of age at the moment of the Chernobyl accident and age at the verification of malignancy and surgery.
A total of 117 patients in dynamic follow up after thyroidectomy because of differentiated thyroid carcinoma, living in Gomel region of Belarus and being under 18 years old at the moment of the Chernobyl NPP accident were enrolled in the study. Age varied from 26 to 31 years. None of the enrolled patients had a family history of thyroid cancer. They were followed up and examined regularly after the thyroidectomy. Subjects were diagnosed and operated during 1991–1996 years (1st group) and during 1997–2006 years (2nd group). Diagnosis of thyroid carcinoma was histologically proved after the surgery. Male to female ratio was 1:2,4 in the 1st and 1:1,3 in the 2nd groups. Serum levels of TSH, thyroglobulin (Tg), fT4, fT3, TPOAb, TgAb were checked regularly. The diagnostic I131 whole body scan was done after the surgery in all patients.
The Me of the age at the moment of the Chernobyl NPP accident differed in this two groups - it reached in 1-st group 3,38 yrs (1,40; 5,39) and 2.03 (1.01;3.19) in the second (p=0,003). The Me of the age at the moment of verification of malignancy was 11.00 (9.00; 13.00) and 9.00 (8.00; 10.00). The latent period was longer in the second group - Me was 13.98 (12.65; 15.95), p=0,001. There were differences in ultrasound pattern and morphological characteristics of thyroid cancer cases in two groups. Thyroid volume was higher but nodular size lower in the second group.
Interestingly, we faced the fact that patients with longer latent period were younger at the moment of the accident and had a coexistence of malignant and multiple nonmalignant thyroid nodules. This fact still requires some additional research in the aspect of variable variants thyroid carcinoma types due to radiation induction.
Surgery, Kuma Hospital, Kobe, Japan
Thyroid Cancer Thursday Poster Clinical
Tumor size, extrathyroidal extension, node and distant metastasis, age and gender are prognostic factors for papillary thyroid carcinoma (PTC). Recently we have reported that serum thyroglobulin-doubling time (Tg-DT) was the most powerful prognostic indicator in patients with PTC who underwent total thyroidectomy and who do not have detectable thyroglobulin antibody (Tg-Ab) (Thyroid, 2011, to be published). Tg-DT was calculated from serum Tg levels measured at TSH suppressed condition. The classical prognostic factors and Tg-DT were significant prognostic factors for survival on univariate analysis, but Tg-DT remained the only independent factor on multivariate analysis. Tg-DT implies speed of tumor growth. Here, we analyze factors that associate with Tg-DT.
Between January 1998 and December 2004, 1515 patients with PTC underwent total thyroidectomy in Kuma Hospital. After excluding patients with other thyroid cancers and anti-Tg antibody, 426 patients with 4 or more serum Tg measurements at TSH<0.1 mIU/L condition were selected for further analysis. There were 349 females and 77 males, aged from 14 to 81 years with a mean of 51.5 years. Tg-DT was computed. Univariate and multivariate analyses were performed to find factors that associate with Tg-DT.
Tg-DT showed a wide range of variation, being <2 year, 2 to 6 years, >6 years, and a negative value due to decrease in Tg values in 33, 20, 17 and 72 patients, respectively. For 88 patients with 3 or fewer detectable Tg levels, Tg-DT was not calculated, and 196 patients demonstrated undetectable Tg levels only. Among the 142 patients with calculable Tg-DT, Tg-DT <2 years, indicating rapid tumor growth, was associated with only age and not with classical prognostic factors (Table). Patients 55 year or older were 5.6 times likely to have Tg-DT<2 years than patients younger than 55 years (p=0.00035). The proportion of patients with Tg-DT<2 years increased with age, being 5.9% in those younger than 40 years, 14.8% in those between 40 and 60 years, and 46.8% in those 60 years or older.
pEx2: pathological massive extrathyroidal extension
Only age at surgery independently associated with Tg-DT, indicating that patients with rapidly growing tumors increase with age.
Carcinoma Showing Thymus-Like Differentiation
Thyroid Cancer Thursday Poster Clinical
Carcinoma showing thymus-like differentiation (CASTLE) is a rare thyroid neoplasm believed to arise from ectopic thymic tissue adjacent to or within the thyroid parenchyma, typically in the lower poles. A 47 year-old male presented with hoarseness. On physical exam, a thyroid mass was palpable but there was no palpable cervical lymphadenopathy. A thyroid ultrasound demonstrated a 4×3 cm thyroid mass over the lower left lobe. Fine needle aspiration of this mass was positive for poorly differentiated carcinoma.
Intraoperatively, the mass arose from the inferior aspect of the left lobe and extended into the strap muscles.
Microscopically, the tumor consisted of infiltrative cords and nests of large, polygonal and pleomorphic epithelial cells with large, round nuclei and prominent nucleoli. There were regions of necrosis as well as occasional mitotic figures. A small thymic remnant was found in the soft tissue adjacent to the thyroid as well as two lymph nodes with metastatic tumor. The histologic and immunohistochemical properties of this tumor were those of a thymic neoplasm, i.e., positive for pancytokeratin (CAM 5.2) as well as a keratinizing marker (p63), typical for thymic neoplasms. The T-cell antigen CD5, inexplicably expressed by the neoplastic epithelial cells of thymic neoplasms, was also reactive in this case.
Metastatic disease to regional lymph nodes is found at presentation in approximately 33% of patients with this tumor (Chan 1991). In one of the largest series of patients with CASTLE, the 5 and 10 year survival rates after curative surgery were 90% and 82% respectively. The presence of positive lymph nodes significantly decreased survival (Ito 2007). After undergoing total thyroidectomy and elective nodal dissection, our patient is currently undergoing concurrent chemoradiotherapy.

3,5-T2 and T3 Interact with and Activate Different Isoforms of the Thyroid Hormone Receptor β1 in Teleosts
Thyroid Hormone Action Thursday Poster Basic
We have previously demonstrated that 3,5-T2 (T2) regulates the transcription of T3-responsive genes, in some teleosts. Furthermore, EMSAs of hepatic nuclear proteins of hypothyroid killifish replaced with T2 or T3 revealed two TRE-TR (T3 responsive element-thyroid receptor) complexes of different weight, suggesting that T2 and T3 bind to transcriptional protein complexes that could involve one or more TR isoforms. Indeed, cloning the TR expressed in killifish liver showed two different TRβ1 mRNAs; both lack 75 amino acids at the N-terminus, as compared to the human TRβ1, and differ in the presence (long: L-TRβ1) or absence (short: S-TRβ1) of 9 amino acids inserted in their ligand binding domain.
To test the influence of this insert in the selectivity and binding proprieties of teleostean TRβ1 isoforms to T3 or T2, we evaluated their transactivation capacity using a reporter gene coupled to luciferase and containing a TRE. We also evaluated the selectivity of both TRβ1 isoforms to form complexes with T3 or T2 by EMSAs.
The transactivating capacity of the TRβ1 isoforms varied depending on the iodothyronine tested and the nature of the transfected cell line. In GH3 cells, a higher transactivating activity was observed in cells transfected with L-TRβ1 and treated with T2, while those transfected with S-TRβ1 showed activity only when treated with T3. In contrast, in the CV1 cell line, the highest activity was observed when cells were transfected with S-TRβ1and treated with T3. These results suggest that the effects of T2 could be mediated by a different TR isoform. The lack of response in CV1 cells transfected with L-TRβ1 and treated with T3 or T2 suggests that this TRβ1 isoform might interact with coregulators that are not expressed in all cell types. The selectivity of TRβ1 isoforms to associate with TREs also varied in the presence of T3 or T2. The formation of L-TRβ1-TRE or S-TRβ1-TRE complexes were favored by T2 or T3, respectively, suggesting that the stability of these complexes could be ligand (iodothyronine)-specific.
Altogether, our results strongly suggest that the nuclear effects of T2 are mediated by L-TRβ1. Supported by: CONACYT 080420 and PAPIIT IN208511.
University of Pisa, Pisa, Italy
Thyroid Hormone Action Thursday Poster Basic
T1AM is an endogenous compound structurally related to thyroid hormone.In mammals, acute treatment with exogenous T1AM has been found to decrease carbohydrate metabolism, heart rate, and temperature. In the present study, we analyze the breath metabolic response to chronic low-dose T1AM administration in mice by using Cavity Ring Down Spectrometry (CRDS).
Mice were treated for a week with 10 mg/Kg/day T1AM, monitoring food intake and body weight up to 35 days. All animals were injected daily from day 0–7 intraperitoneally with either 10mg/kg T1AM or vehicle. Real-time sampling of breath carbon in exhaled CO2 (13CO2/12CO2 delta value) was performed by CRDS (CSN-015 Cavity Ringdown Spectrometer Picarro, Sunnyvale, CA, USA). All animals were sampled for a total of 6 hours per injection. Plasma was also collected on day 0, day 7, and day 35 and analyzed by NMR spectroscopy. Prior to data collection samples were treated with ice-cold methanol (2:1, v/v), placed at −20°C for 20–30 minutes, centrifugated at 15000 rpm for 5 min. The supernatant was then removed from the protein pellet and dried. Supernatant was then reconstituted by adding a 20 mM PBS containing 1 mM DSS, 0.1 mM NaF, pH 7.4. All NMR spectra were collected by a Varian NMR system 600 MHz spectrometer.
Exogenous T1AM administration was associated with a body weight loss trend in mice (−8.2% of initial body weight by day 9; p=0.076). After T1AM withdrawal, mice regained only part of lost weight (±1.8% of initial weight regained) in the following 2 weeks, indicating long-lasting effects of this natural molecule. No difference in food intake was observed during and after treatment. After administration of T1AM the breath delta value dropped significantly (−1.8%) within 80 minutes of injection, indicating a switch from carbohydrate to lipid metabolism, as a leading contribution to weight loss. NMR spectroscopy revealed key metabolites in lipid catabolism that are altered following T1AM treatment.
Metabolic switching leading to lipid mobilization by physiological dose T1AM may provide a new opportunity for development of this endogenous compound as an effective human weight-loss drug.
Activity of Some Physiological Modulators in Reducing the Side Effects of Levothyroxine in Patients Suffering from Primary Hypothyroidism
Thyroid Hormone Action Thursday Poster Clinical
The use of L-T4 (levothyroxine) in the treatment of primary hypothyroidism causes oxidative stress (OS) and daily discomfort. It is believed that the use of physiological modulators (PMs) may make the treatment more tolerable.
Thirty six patients of both sexes (15 M; 21 F) with hypothyroidism were enrolled (age 44–64 years), starting the treatment with LT-4 at the fixed dose of 75μg/day. Subjects were randomly divided into three groups (A, B and C) of 12 subjects each in a double blind design. Group A was treated with a formula based on bioflavonoids; group B with a formula B based on oligomeric proanthocynidins (OPA); group C with placebo. Treatments continued for 30 days. Plasma levels of T3, T4, TSH, plasma hydroperoxides and hs-CRP, were determined before and after 30 days of treatment. During the treatment anxiety/agitation, sweating, palpitations, headache and daily discomfort were recorded through a daily questionnaire.
The same adequate hormone balancing was observed in all three groups (T4, T3, TSH). The hydroperoxide levels in the three groups (A, B and C) were similar at baseline (373±36.1, 384±39.1, 376±24.0 U.CARR. respectively); after 30 days the values were significantly different (of 312±21.0, 273±24.3, and 409±31.7 U.CARR respectively). The levels for hs-CRP at baseline were 3.8±1.41, 3.4±1.34, 3.6±1.03, and 3.8±1.31, 3.2±0.99; and 4.4±0.90 mg/L at 30 days respectively. Both markers were more consistently reduced by Formula B (anova p<0.05). The incidence of side effects and the number of days of daily discomfort were significantly lower in the same group only (anova p<0.05).
The use of a formula containing OPA with other PMs may limit the incidence of the side effects that occur during the initial phase of L-T4 treatment in hypothyroidism.
Medicine, Oregon Health & Science University, Portland, OR
Thyroid Hormone Action Thursday Poster Clinical
Patients with benign and malignant thyroid diseases are often treated with doses of levothyroxine (L-T4) to suppress TSH levels below the normal range. It is not clear whether this mild exogenous thyrotoxicosis affects metabolism or body composition.
To address this, we recruited otherwise healthy women into two age and BMI-matched groups: 1. L-T4-treated hypothyroid women with normal TSH levels (T4Tx-Nl, N=53), and 2. L-T4-treated hypothyroid women with low or suppressed TSH levels and normal free T4/T3 levels (T4Tx-Low, N=16). Women in the second group had treated thyroid cancer with no evidence of disease (N=9) or benign disease (N=7). Subjects underwent measurements of Resting Energy Expenditure (REE), respiratory quotient (RQ), and Thermic Effect of Food (TEF) by indirect calorimetry, and body composition by DEXA.
Groups differed in thyroid function as expected. The T4TX-Low group had higher REE, but not TEF, than the T4TX-Nl group, with lower BMI and a trend toward lower LBM (see table). By correlation analysis, log free T4 was directly related to REE (Pcorr=0.23, p=0.06), but inversely related to TEF (Pcorr=−0.28, p=0.03). Log fT4 was also inversely related to BMI (Pcorr=−0.22, p=0.07) and lean body mass (Pcorr=−0.24, p=0.05). Log fT3 was only directly related to % body fat (Pcorr=0.33, p<0.01).
Results are means±S.E.M, or medians and ranges for thyroid hormone levels. ap<.0001, bp<0.05, cp=0.1 compared to T4Tx-Nl by regression models adjusted for age and BMI as appropriate.
Utilizing sensitive techniques, women receiving suppressive doses of L-T4 had increased resting energy expenditure compared to euthyroid women receiving L-T4. These preliminary data suggest that such increases may affect BMI and body composition.
Endocrinology and Metabolic Service, Walter Reed Army Medical Center, Washington, DC
Thyroid Hormone Metabolism and Regulation Thursday Poster Basic
The use of herbal/natural supplements is rising in the United States and these substances are not closely regulated by the FDA under the Dietary Supplement Health and Education Act (DSHEA) 1997. We examined the thyroid hormone content in over-the-counter (OTC) health supplements marketed as a “thyroid support”. There are no previous reports detailing thyroid hormone content in OTC supplements.
Ten commercially available thyroid supplements were purchased from the local stores and online distributors. The ten most popular thyroid health products identified on an internet search were selected. Thyroid supplements were dissolved in 10 ml of acetonitrile and water with 0.1% trifloroacetic acid and analyzed using HPLC. The selected products were analyzed for the presence of thyroxine (T4) and triiodothyronine (T3) using levothyroxine and liothyronine as a positive control.
The amount of T4 and T3 was measured separately for each supplement sample. Nine out of ten supplements showed a detectable amount of T3 (1.3–25.4 mcg/tablet). Taken at the recommended dose, five supplements delivered T3 quantities of greater 10 mcg/day, and four delivered T4 quantities ranging from 8.57 to 91.6mcg/day. Among the five thyroid supplements labeled as containing bovine thyroid tissue, extract or concentrate, one had no detectable level of T3 or T4, two contained T3 only, and two showed detectable amounts of both T3 and T4.
Most of the OTC thyroid supplements studied contained clinically significant amounts of T4 and T3, some of which exceeded common treatment doses for hypothyroidism. This potentially exposes patients to risk of iatrogenic hyperthyroidism by taking easily accessible OTC supplements not requiring prescription. The current study results emphasize the importance of patient and provider education regarding the use of OTC herbal supplements and highlights the need for greater regulation of OTC supplements potentially dangerous to the public.
Oncology, Georgetown University Medical Center, Washington, DC
Thyroid Hormone Metabolism and Regulation Thursday Poster Clinical
The harmful effects of tobacco smoke exposure on pregnancy outcomes associated with infertility, preterm delivery, stillbirth, low birth weight, and sudden infant death syndrome have been documented. The objective of this study is to examine whether cigarette tobacco smoke exposure is associated with lower thyroid hormone levels and inflammation.
Serum thyroid hormones, thyroid-stimulating hormone (TSH) and C-reactive protein (CRP), a non-specific marker of acute inflammation, were measured in 300 healthy, non-pregnant women of reproductive age (18–45y). Associations between CRP levels, thyroid hormones, TSH and steroid hormones (cortisol, aldosterone, estrone and progesterone) were also explored. Serum concentrations of CRP were determined using an immunoturbidimetric high sensitivity CRP (hsCRP) assay. Serum thyroid hormone, steroids and cotinine levels were measured by isotope dilution tandem mass spectrometry (LC/MS/MS).
In general, all hormone levels were within the normal ranges. A significant, positive correlation between hsCRP and cotinine levels was observed. Cotinine explained approximately 3% in the variance in hsCRP. BMI was a significant predictor of hsCRP after adjusting for age. No significant correlations were observed between hsCRP levels and TSH, aldosterone, estrone and progesterone.
The results observed suggest that smoking intensity (represented by the nicotine metabolite cotinine) plays an important role in inflammation. Additionally, higher BMI was associated with higher hsCRP levels in healthy women of reproductive age. While cigarette tobacco smoke was associated with changes in hormone levels, there lacked a correlation between the levels of the hormones examined and hsCRP. This suggests that a mechanism independent from the one leading to inflammation, may underlie the changes in hormone levels seen in women who are exposed to cigarette tobacco smoke. Further studies examining the inter-relationships between hsCRP and thyroid and sex hormones are essential in determining a possible role for inflammation in women's health.
T4 Malabsorption
Thyroid Hormone Metabolism and Regulation Thursday Poster Clinical
The case who underwent total thyroidectomy for thyroid papillary carcinoma continued to have elevated thyrotropin (TSH) level and received levothyroxine (LT4) at a dose of 400 mcg. During follow-up, the TSH level was found to be high and LT4 was combined with liothyronine (LT3). Given continuing high TSH level, the patient was deemed to be resistant to oral administration and vaginal administration was offered in another clinic.
The patient's TSH level was found to be 93 μIU/mL in the first measurement and the treatment was initiated with LT4 at a dose of 450 mcg/day and LT3 at a dose of 100 mcg/day. First, all the previous drugs that might inhibit LT4 absorption were stopped and the drugs were administered per oral route under the surveillance of a nurse. Considering that vitamin C provides an acidic environment and enhances the absorption of LT4, LT4 in combination with vitamin C were administered per oral route. At follow up examinations, the TSH level was found to be 98 μIU/mL. Endoscopy was planned to evaluate atrophic gastritis but required to be performed under anesthesia due to the patient's intolerance. The case with markedly elevated TSH level wasn't considered as appropriate for anesthesia and endoscopy couldn't be performed. Anti tissue-transglutaminase and anti-endomysium antibodies revealed negative results for celiac disease. The urea-breath test and stool test were negative. The results of the lactose tolerance test revealed normal.
Based on these data, the case was considered to have T4 malabsorption and intravenous (iv) LT4 was purchased overseas. Infusion of LT4 at a dose of 50 mcg was administered for two hours; however, blood pressure increased up to 220/140 mmHg during infusion and subsequently, the patient developed a minimal left hemiparesis, inability to speak but had no chest pain or no electrocardiographic changes. Blood pressure was gradually decreased by infusion of nitroglycerin. The computerized tomography yielded normal. The second and third vials were administered more slowly and no problems were encountered.
At present, maintainenance doses of iv LT4 are expected to arrive from overseas. During this time, the patient is being followed up with per oral 2400 mcg/day LT4.
Thyroid Hormones and Reproductive Aging
Thyroid Hormone Metabolism and Regulation Thursday Poster Clinical
Hormonal imbalances of thyroid combined with imbalances of gonadotrophic hormones can produce a multitude of menopausal and perimenopausal symptoms, due to many changes which affects all physiological activities of thyroid and reproductive gland. An untreated thyroid problem could contribute to worsen the perimenopausal problems and can mainly affect the bone mineral density and risk for osteoporosis.
Study Population: Women in perimenopausal stage (age group—35 to 45 years old) Study Area: Urban Vadodara Sampling Method: Purposive sampling based on MRS scoring Biochemical estimations: ECL (Electrochemiluminescence) assay
Total of 57 perimenopausal women were enrolled for the study based on menopause rating scale. Serological testing for T3,T4, TSH, FSH and LH were carried out. Out of n=57 women, 35.1% had high FSH (55.51±7.65 mIU/ml) and 36.8% had high LH (41.5±3.5 mIU/ml) values. Amongst these, 20% had low TSH values (age>40 years). Hormonal fluctuations observed mainly in the women aged more than 40 years. The gonadotrophic hormones (FSH and LH) are significantly correlated with thyroid hormones (p=0.000).
Co-existence of premature menopause and hypothyroidism was observed during late 40 years of age in women. Early sensitization and intake of healthy food (phytoestrogen rich) is recommended as a means to cope up with low gonadotropin secretion and prevent the thyroid hormone imbalances.
Endocrinology, Harbor-UCLA, Torrance, CA
Thyroid Imaging Thursday Poster Clinical
A 71-year-old Filipino female underwent thyroidectomy after fine needle aspiration of a thyroid nodule was noted to be suspicious for malignancy. Surgical pathology revealed multifocal disease, with a mixed follicular and papillary pattern. The patient's post radioactive iodine ablation scan showed intense uptake in the thyroid bed as well as in the right middle lobe of the lung concerning for pulmonary metastasis.
Repeat I-131 scan one year post initial therapy again disclosed abnormal right middle lobe uptake. Thyroglobulin and anti-thyroglobulin antibodies were consistently undetectable under conditions of both thyroid hormone suppression and stimulation, and the patient was asymptomatic. Work-up was initiated to elucidate the etiology of her abnormal pulmonary iodine uptake. Careful pulmonary history revealed that the patient had previously been diagnosed with bronchiectasis and atypical mycobacterium colonization (Mycobacterium chelonae) when she had presented with a cough and hemoptysis. A CT scan confirmed the presence of extensive cystic bronchiectasis in the right middle lobe of the lung which coincided anatomically with the iodine-avid area noted on scan. No other lesions concerning for malignancy were identified. The same area of abnormality was identified by ventilation/perfusion and gallium scans. A bronchoscopy was negative for malignant cells. Sputum consistently revealed colononization with M chelonae. Therefore, the diagnosis of a false positive I-131 scan secondary to bronchiectasis and coincident mycobacterial colonization was highly suspected.
The most common cause of false positive I-131 uptake in the lungs are primary lung carcinoma followed by infectious and inflammatory causes. Conditions such as upper respiratory tract infections, interstitial lung disease, bronchiectasis, mycobaterial infection and rheumatoid arthritis have been reported to yield a false positive result. Iodine excretion into alveolar/bronchial inflammatory exudates has been postulated to be the mechanism underlying iodine localization in the lungs.
False positive iodine scans can occur and may lead to overtreatment of thyroid cancer if not suspected when standard thyroid cancer follow-up data do not correlate.
A “One Medicine” Example: Humans as the Model for a Feline Disease
Thyroid Nodules and Goiter Thursday Poster Basic
Every day, the news media reports findings of potentially toxic compounds in consumer products ranging from baby seats to soda cans. Human beings and other animals share the same planet and the same environments, and because of their shorter life spans, companion animals may serve as sentinels for public health hazards. The principle of “One Medicine” embraces the concept of physicians and veterinarians working in unison to identify, treat, and prevent common diseases and those diseases that cross species lines. While epidemiologic studies of several cancers in cats and dogs have implicated hazards known or likely to lead to cancers in their human caregivers, numerous chronic diseases occur in humans and companion animals as well. In particular, feline hyperthyroidism shares histopathologic and metabolic features with toxic nodular goiter, a disease of older people with iodine-deficient diets or exposed to substances that interfere with iodine uptake or thyroid hormone metabolism. This feline disease, first described in the late 1970s, has become the most common endocrine disease of older cats.
My presentation will review the epidemiology of this disease for which humans have provided the model, including host, dietary, and environmental risk factors.
Published reports worldwide have identified numerous risk factors that are common to humans and cats, such as age, female sex, the potential for iodine deficiency, and exposure to goitrogens in cats' diets and environments.
These findings may pave the way toward research collaborations for identifying potential public health risks in the environment that we share with our companion animals.
Nuclear Medicine, Medical University of Bialystok, Bialystok, Poland
Thyroid Nodules and Goiter Thursday Poster Clinical
The aim of our study was to evaluate the efficacy of radioiodine therapy in patients with non-toxic nodular goitre.
We treated 160 patients, aged 20–76 years; 87% of the studied groups were female and 13% male; Iinitial 24 h radioiodine uptake (RAIU) was ranged between 22–44%, and thyroid volume ranged between 44–170ml, effective half-life was more than 3 days at the time of treatment. Malignant changes were excluded in all nodules by fine needle aspiration biopsy. The activity dose was calculated by the use of Marinelli's formula and ranged between 200–800 MBq. The absorbed dose ranged between 150 and 260 Gy. Thyroid ultrasonography, and thyroid scan with RAIU at 24 and 48-hours was done before, after 6, 12 month and yearly for four year of radioiodine therapy. Follow up control with evaluation of fT3, fT4, TSH was done every 6 weeks in the first year. Then every 6 months for four years.
After 12 months of radioiodine therapy a mean thyroid volume reduction of 46% was achieved. Euthyroidism persist in 92% of patients, and hypothyroidism develop in 8% of patients. After 3 years of radioiodine therapy 9% of patient develop hypothyroidism. After 5 years of radioiodine therapy a mean thyroid volume reduction of 49% was achieved and 11% of patients develop hypothyroidism. All patients were highly satisfied; the compressive symptoms relieved and exercise tolerance improved.
Radioiodine is non-invasive, safe and cost effective method of therapy for reduction of large non-toxic goitre and should not be restricted to patients with high operative risk, but should be used as first choice in every patient with non toxic nodular goitre with thyroid volume >40 ml. The reduction of thyroid volume with low percent of hypothyroidism, were due to well accurate measurement of administered activity, relatively high effective half-life, and well-organised follow up.
Single Incision Endoscopic Thyroidectomy by Axillary Approach for Patient with Benign Thyroid Tumor
Thyroid Nodules and Goiter Thursday Poster Clinical
Endoscopic thyroidectomy to thyroid tumor is generalized recently. And development of minimally invasive surgery had drived surgeons to less invasive and less incision. The aim of this study was to evaluate the early surgical outcomes of single incision endoscopic thyroidectomy (SIET) by axillary approach for patients with benign thyroid tumor.
Between June 2009 and April 2011, 54 patients with benign thyroid tumor underwent SIET by axillary approach. We analyzed the patient's clinico-pathologic characteristics, surgical outcomes and cosmetic results.
The mean age of the patients was 37.12±10.16 (range 13–59). The mean tumor size was 22.81±12.62 (range 2–60) mm. The each operative time was 134.15±28.26 (range 80–206) min in 49 lobectomy, 237.33±39.0 (range 210–282) min in 2 subtotal thyroidectomy, 180 min in 1 isthmectomy and 210 min in 1 completion subtotal thyroidectomy. The pathology was confirmed 2 follicular adenoma, 1 Hurthle cell adenoma, 1 chronic lymphocytic inflammation, 1 chronic granulomatous inflammation, 1 Grave's disease and 49 nodular hyperplasia. Postoperative pain was estimated by visual analogue scale(VAS) system and the score was 2.94±1.95 (range 1–9). Cosmetic result was estimated by verbal response system(1. extremely satisfied; 2. satisfied; 3. Acceptable; 4. dissatisfided) and the mean scale was 1.19±0.4 (range 1–2). Immediate postoperative bleeding was occurred in 2 cases and recovered by conservative treatment. During the follow up period, there were 8 transient paresthesia, 2 transient voice change, 2 transient swallowing difficulty and all problem was resolved without any treatment.
The SIET by axillary approach is safe and feasible. And we think that reducing of the incision size and the dissection area can enhance the cosmetic results and the postoperative pain.
Robotic Single-Incision Transaxillary Total Thyroidectomy
Thyroid Nodules and Goiter Thursday Poster Clinical
Robotic approaches to thyroidectomy are gaining more popularity over the recent years. There is debate about whether total thyroidectomy should be done through a unilateral or bilateral axillary incision. We have been performing total thyroidectomy through a single axillary incision. The aim of this study is to report our initial results with this approach.
Within 18 months, 19 patients underwent robotic transaxillary thyroid and parathyroid procedures. Among these, 9 patients had total thyroidectomy through a 5–6 cm unilateral axillary incision. The procedures were done under general anesthesia using the robotic camera and 2 working ports. Lessons from conventional surgery for removing substernal goiters were used to resect the contralateral thyroid lobe by following a medial to lateral dissection plane. Data were collected prospectively. Perioperative outcome was analyzed. All data are expressed as mean±SEM.
All patients were female with a mean age of 53±3. Mean body mass index was 23.1±0.4. Mean nodule size was 1.2 cm±0.6. Indications for surgery included follicular neoplasm (n=5) and suspicion for thyroid cancer (n=3) on fine needle aspiration biopsy and multinodular goiter with a history of neck radiation (n=1). The mean operative time, which was 256±16 minutes in the first half of the study, decreased to 166±11 minutes in the second half. Between the first and second half of the study, the flap, docking and console time decreased from an average of 72, 17, and 125 minutes to 30, 13, and 100 minutes, respectively. All patients were discharged home on postoperative day 1 without complications. Pathology showed papillary thyroid carcinoma in 5 patients and benign multinodular goiter in 4. Postoperative mean tyroglobulin values were 0.95 ng/mL. The 24-hour radioactive iodine uptake in one patient who was ablated was 1.15%.
Our initial results show that robotic total thyroidectomy through a unilateral axillary incision is feasible and safe. We believe that in experienced hands, this technique may be preferred over the bilateral axillary incision technique for robotic total thyroidectomy.
Department of Medicine, Maruyama Hospital, Hamamatsu, Japan
Thyroid Nodules and Goiter Thursday Poster Clinical
Thyroid cyst can be classified into simple colloid and complex cysts, including hemorrhagic cysts, cysts with epithelial component or cysts filled with transudate. The common clinical manifestation of hemorrhagic cysts is an anterior neck mass, sometimes accompanied by cervical pain.
This is a clinical case report from Hamamatsu University School of Medicine.
In September 2007, a 61-year-old man was referred to our hospital because of a right thyroid cyst of 5.3cm maximum diameter found on ultrasonography at a medical checkup. Palpation revealed a firm thyroid nodule but no subjective symptoms were noted. Since fine needle aspiration biopsy showed benign cytology, he stopped consulting our hospital. In April 2009, he was admitted to another hospital with acute myocardial infarction. His manifestations improved after emergent pericutaneous coronary intervention, and subsequent antiplatelet therapy with 100mg aspirin plus 75mg clopidogrel was started. He was referred to our hospital again for evaluation of the right thyroid cyst. Ultrasonography exhibited negligible changes. In May 2010, he visited our hospital with complaints of vague anterior neck pain and hoarseness. Computed tomography delineated a low-density mass of 6.8 cm maximum diameter causing tracheal deviation as well as compressing the right common carotid artery and brachial artery (see figure). Subsequent laryngoscopy revealed right vocal cord palsy. Emergency hemithyroidectomy was performed and surgical exploration revealed that a non-invasive firm nodule had deviated the brachial artery below, resulting in compression of the right recurrent laryngeal nerve. Histological findings confirmed the diagnosis of hemorrhagic thyroid cyst. His complaints gradually improved and normal recurrent laryngeal nerve function was observed two months after surgery.
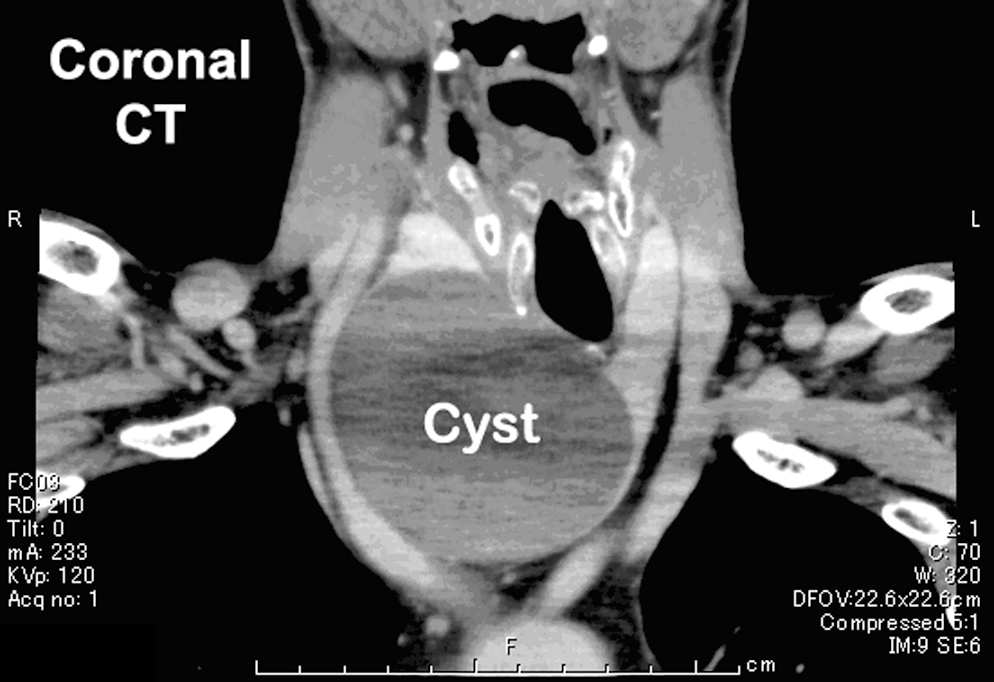
We report here a very interesting patient with hemorrhagic thyroid cyst causing right recurrent laryngeal nerve palsy. Physicians should be aware of the possible risk of hemorrhagic cyst, especially in patients treated with antiplatelet or anticoagulation therapy, since it can lead to potentially life-threatening vocal cord palsy.
Otolaryngology, Head and Neck Surgery, University Hospital Birmingham, Birmingham, United Kingdom
Thyroid Nodules and Goiter Thursday Poster Clinical
In the UK, trainees in Otolaryngology and Endocrine Surgery are required to gain skills in thyroid surgery. As trainee numbers are increasing and the duration of training decreasing, there is concern that trainees are not receiving sufficient experience and supervision in thyroidology. We set out to determine whether operations performed by trainees differed in complication rate, length of stay and duration compared with consultants.
A prospectively collected database of all thyroid operations performed at our tertiary referral centre was analysed. Operations performed by trainees were compared with those performed by consultants, specifically examining the operation length, complication rate and length of stay.
1470 patients from 1994–2009 were included in the analysis. 1139 cases were performed by a consultant and 331 by a trainee. The percentage of trainee cases per year increased slightly over the study period (R2=0.03). The overall complication rate was 21% for consultant cases and 14.5% for trainees. Temporary hypocalcaemia rate was 28% and 32% for consultants and trainees respectively, while temporary RLN palsy rate was 2.4% for consultants (1523 nerves at risk) and 2.1% for trainees (387 nerves at risk). There was no significant difference in length of stay for hemi-thyroid surgery between the two groups, although the duration of surgery was significantly shorter for consultant procedures (69 mins vs 75 mins, P<0.001). For total thyroid surgery, duration of surgery did not differ significantly; length of stay was longer for the consultant group (3.2 days vs 2.7 days, p=0.03), likely reflecting the fact that the consultant cases tended to be more complicated.
We have demonstrated that there is no increased risk of complication when thyroid surgery is performed by a trainee, provided that there is an appropriate level of supervision and that cases are selected to match the trainee's level of experience. Trainees learning thyroid surgery should be under the supervision of an experienced thyroid surgeon to ensure complications are minimal.
Subdireccion de Investigacion, Facultad de Medicina U.A.N.L., Monterrey, Nuevo Leon, Mexico
Thyroid Nodules and Goiter Thursday Poster Clinical
Systemic Lupus Erythematosus (SLE) is an autoimmune disease whose prognosis has improved in recent decades due to advances in diagnosis and treatment, which has been associated with improvement in quality of life, survival and as consequence the development of co-morbidities such as cancer. Thyroid nodules (TN) are a common clinical problem, whose prevalence is reported up to 7%. Its clinical importance is the need to exclude thyroid cancer which occurs in 5–15% of TN depending on diverse risk factors. In patients with SLE a reported prevalence of 25% of TN has been found. The purpose of this study is to report the prevalence of TN in a group of patients with SLE in a single hospital.
We developed an observational, transverse, analytic study at the University Hospital in Monterrey N.L. during August 2010-May 2011. We included 19 patients over 18 years of age, with diagnostic criteria for SLE. We documented clinic, demographic and anthropometric characteristics. All patients underwent a thyroid ultrasound to document the presence of TN. We calculated the prevalence of TN in SLE patients and compared it with the one found in a previous study in our population. We considered significant a p≤0.05.
We included 19 female patients; average age was 37±9 years old, with a BMI of 27±7 kg/m2, 21% with overweight and 21% with obesity. The time since the diagnosis of SLE was 9±6 years. 21% patients had family history of thyroid disease, 5% smoke, and 16% the diagnosis of primary hypothyroidism. The prevalence of TN in our study population was 32% (95% CI, 15.4–54.3) with a nodular size ranged in 2–8 mm. We did not find any association between the presence of TN and the studied variables.
There is a high prevalence of TN in SLE Mexican patients compared to the one found in the general population.
TN, Thyroid Nodules; BMI, Body Mass Index; SLE, Systemic Lupus Erythematosus.
Pathology, MDACC, Houston, TX
Thyroid Nodules and Goiter Thursday Poster Clinical
Chronic lymphocytic leukemia (CLL) is characterized by clonal proliferation of small mature B-lymphocytes that infiltrate bone marrow, blood, lymph nodes and spleen. In advanced stages, CLL can involve other organs such as the skin and lungs. Thyroid involvement has not been described. We describe a rare case of CLL infiltration of the thyroid gland associated with primary hypothyroidism and Hashimoto's thyroiditis.
A 71-year-old woman with a two-year history of CLL and no history of thyroid disease presented with a markedly enlarged thyroid gland. Thyroid function tests revealed subclinical hypothyroidism with a TSH of 10 MCU/ML. A thyroid iodine-scan revealed nodular foci of increased uptake in the lower pole of the right thyroid lobe and mid aspect of the left lobe with diminished tracer uptake throughout the remainder of the thyroid parenchyma. Ultrasound revealed an enlarged non-homogenous thyroid with increased vascularity.
Fine needle aspiration showed leukemic infiltration of the thyroid gland with histologic staining positive for CD19, CD20, CD5, CD23 and CD38. The patient had elevated titers of thyroid peroxidase antibodies 27358 IU/ML and thyroglobulin antibodies 6612 IU/ML. Patient was treated with lenalidomide. After 6 months of therapy, the patient exhibited a partial remission of the CLL. Thyroid ultrasound revealed a substantial decrease of the thyroid size with normalization of thyroid function tests and decreased titers of thyroid peroxidase antibodies (1346 IU/ML) and thyroglobulin antibodies (2294 IU/ML).
CLL may infiltrate the thyroid gland predisposing to a reversible Hashimoto's thyroiditis and primary hypothyroidism if responsive to systemic therapy. This case illustrates the role of B-cells in Hashimoto's thyroiditis pathogenesis and an unexpected benefit derived from lenalidomide on this disease.
Interleukin-2 Therapy and the Extremes of Autoimmune Thyroid Disease
Autoimmunity Thursday Poster Clinical
Interleukin-2 (IL-2) is a cytokine that regulates differentiation and growth of lymphocytes and is used as a salvage chemotherapeutic regimen for different malignancies. IL-2 causes hypothyroidism in 21% of patients. Hyperthyroidism due to thyroiditis or Graves' disease has been described in some cases.
A 56 year-old woman with primary hypothyroidism and a metastatic renal cell carcinoma developed atrial fibrillation with rapid ventricular response and hyperthyroidism after receiving 2 doses of IL-2. She had high titers of thyroid stimulating immunoglobulins 3.0 (normal<1.3) and thyroid peroxidase antibodies 4368 IU/mL.
She was initiated on a beta-blocker and levothyroxine was discontinued. She continued to receive IL-2 monthly. Four months later, she was found again with primary hypothyroidism with TSH 75.6 uIU/mL. She initiated levothyroxine. After completing two more months of IL-2, the patient developed heat intolerance and weight loss. Thyroid function tests showed TSH<0.01 uIU/mL and Free T4 2.7 ng/dL. Levothyroxine was again stopped. Thyroid scans were not obtained due to a frequent computerized tomography contrast exposure required to evaluate the cancer response to IL-2.
IL-2 therapy causes an enhanced humoral immunity that may affect the thyroid gland in an unpredictable manner. Patients receiving IL-2 need careful monitoring of thyroid function.
Friday, October 28, 2011
Department of General Surgery, Wuhan Union Hospital, Wuhan, China
Thyroid Cancer Friday Oral Clinical 2:30 PM
Prophylactic central neck dissection (CND) is gaining acceptance in treating papillary thyroid carcinoma (PTC) as studies have shown nodal disease increases the rate of local recurrence. But surgical indication of PTMCs is still controversial. Most PTMCs follow an indolent clinical course, but a few present with lymphadenopathy. It's important to indentify the subgroup of PTMCs with high risk to experience lymph node metastasis (LNM) especially subclinically.
From 2003 to 2011, 1456 PTC patients received surgeries in our institution. 212 PTMCs who were received primary treatment here and underwent total thyroidectomy (TT) associated with CND were included in this study. The frequency of LNM was analyzed according to age, gender, tumor size, multifocality and extrathyroidal extension. All pathological results were reviewed by a pathologist. For multifocal lesions, the analysis was first performed according to the largest dominant tumor as previous study, then we calculate the total diameter of each foci as overall diameter of the specimen for further analysis (Table 1). At last we performed a meta-analysis comparing the LNM between mutifocal and unifocal PTMCs in patients that all underwent thyroidectomy associated with cervical lymph node dissection.
Univariate Analyses of LNM with Respect to the Overall Diameter of Multifocal PTMCs.
unifocal PTMCs; bmultifocal PTMCs with overall diameter less than 1cm; cunifocal PTMCs; dmultifocal PTMCs with overall diameter greater than 1cm; eunifocal PTC with diameter less than 2cm greater than 1cm; fmultifocal PTMCs with overall diameter less than 2cm greater than 1cm; gLNM; habsent of LNM.
With use of univariate and multivariate analysis, age, gender, local infiltration and multifocality were independent correlates of LNM in PTMCs. In further analysis, the proportion of LNM was similar in multifocal PTMCs with overall diameter less than 1cm and unifocal PTMCs (37.5% vs. 30%, P>0.05), also similar in multifocal PTMCs with overall diameter less than 2 greater than 1cm and solitary tumors with diameter equivalent to the former (1–2cm) (56.82% vs. 64.96%, P>0.05), however significantly higher in mulifocal PTMCs with overall diameter greater than 1 cm than unifocal PTMCs (60.42% vs. 30%, P<0.01). Using random effects model, a meta-analysis of nine publications with a total 1586 PTMCs demonstrated that multifocality was significantly associated with LNM risk with an OR of 1.842 (95% CI, 1.318–2.574).
Patients who have multifocal PTMC with overall diameter greater than 1cm can not be considered low risk. TT associated with routine CND may be the best surgical approach.
Thyroid Cancer Friday Oral Clinical 2:45 PM
A better understanding of the molecular mechanisms involved in papillary thyroid cancer (PTC) progression and adverse outcome is needed to effectively manage patients. Our objectives were to identify molecular markers associated with unfavorable features and outcome in patients with PTC.
We performed genome-wide expression (GWE) analysis in 64 primary human PTC samples. Clinical, pathologic, tumor somatic mutation status (BRAF, RET/PTC, RAS) and microarray data were analyzed to identify differentially expressed genes associated with unfavorable features and outcome. Quantitative RT-PCR was used to validate the GWE data. Differentially expressed genes associated with adverse outcome in the training 64 PTC samples were then validated in additional 26 primary PTC test samples.
GWE analysis identified 43, 115 and 40 genes that were significantly differentially expressed by gender, tumor differentiation status and mortality, respectively, with a false discovery rate (FDR) of <5%. We found no significantly differentially expressed genes by age, tumor size, extrathyroidal extension, and lymph node or distant metastasis, AMES risk classification, and recurrent disease. For mortality, 5 of the most significantly differentially expressed genes (CPSF2, LARS, AURKC, TRNT1, and BCL11A) were validated. The CPSF2 gene was validated in additional 26 independent samples to predict disease-free survival. Also, lower expression of CPSF2 was associated with larger primary tumors (p<0.01), extrathyroidal extension (p=0.03), high-risk AMES (p=0.03), disease free survival (p<0.01) and mortality (p<0.01), independent of BRAF V600E mutation status.
To our knowledge, this is the first GWE analysis of PTC and unfavorable features and adverse outcome. A lower expression of CPSF2 in PTC is associated with larger primary tumors, extrathyroidal extension, shorter disease-free survival and mortality. Our finding has important clinical management ramification in patients with PTC.
Incidental Findings on Imaging May be Responsible for the Apparent Increasing Incidence of Advanced Thyroid Cancer
Thyroid Cancer Friday Oral Clinical 3:00 PM
The incidence of well-differentiated thyroid cancer (WDTC) in the US is increasing more rapidly than any other cancer. Much of this increase is due to incidental detection on imaging studies of small, nonpalpable tumors, which may be clinically insignificant. There is growing evidence that the incidence of advanced WDTC is increasing as well. We hypothesized that widespread use of imaging studies accounts for increased detection of advanced as well as early WDTC.
A retrospective chart review of 449 patients who underwent initial surgery for WDTC in one institution from 1/1/07–8/31/10 was performed. 45 patients were excluded because the method of initial detection of WDTC could not be determined. The remaining 404 patients were divided into 2 groups: Group 1, in which the tumor was initially detected on an imaging study, and Group 2, in which the tumor was detected because the patient or physician felt a mass in the neck. Tumor size was reported as measured by the pathologist.
188 patients (47%) were in Group 1 and 216 (53%) in Group 2. Patients in Group 1 were more likely to be male (32% vs. 21%, p=0.013) and older (median age 52 vs. 46, p=0.0004) than those in Group 2. Of the patients in Group 1, the tumor was detected on ultrasound in 104 (55%), CT in 37 (20%), MRI in 19 (10%), carotid duplex scan in 13 (7%), and PET or other imaging studies in 15 (8%). 58% of tumors <1cm, 53% of those 1–2 cm, 31% of those 2–4 cm and 39% of those >4cm were in Group 1. Of the 307 (76%) patients with Stage 1 or 2 WDTC, 142 (46%) were in Group 1. Of the 97 (24%) with Stage 3 or 4 WDTC, 46 (47%) were in Group 1.
This study demonstrates that nearly half of all WDTC were incidentally discovered on imaging studies. Incidental findings on imaging were responsible for the detection of close to 50% of early (Stage 1,2) as well as advanced (Stage 3,4) WDTC. WDTC identified by imaging were more common in older male patients, who generally have a worse prognosis. These findings suggest that the frequent use of imaging studies is responsible not only for the increasing incidence of early WDTC, but for more advanced thyroid cancers as well.
Head and Neck, Memorial Sloan-Kettering, New York, NY
Thyroid Cancer Friday Oral Clinical 3:15 PM
Purpose: To describe the outcome of patients with poorly differentiated thyroid cancer (PDTC) presenting with gross extrathyroidal extension (ETE).
Materials and Methods: Retrospective data were collected in a consecutive series of 27 patients with PDTC and gross ETE (T4a) treated by primary surgical resection with or without adjuvant therapy from 1986–2009. Of 27 patients, 52% were female. The median age was 70 (range 27–87). 41 % of patients presented with N0, 6 (22%) N1a and 10 (37%) N1b neck disease. Ten patients (37%) presented with distant metastases; seven to the bone with three also with lung metastases and three only with lung metastases. All patients were managed by extended total thyroidectomy except for two managed by subtotal thyroidectomy. 20 patients (74%) had central compartment neck dissection and more than half of them (11) also had lateral neck dissection. 21 patients (77%) had adjuvant therapy: 15 (55%) RAI only, 3 (11%) postoperative radiation (PORT) only and 3 (11%) both RAI and PORT. Overall survival (OS), disease specific survival (DSS), local recurrence free survival (LRFS) and regional recurrence free survival (RRFS) were calculated by the Kaplan Meier method.
Median follow-up time was 57 months (range 1–197 months ). The 5 year OS and DSS were 47% and 49% respectively. This poor outcome was due to distant metastatic disease; 10 patients had distant metastases at presentation and a further 6 patients developed distant metastases during follow up. Locoregional control was good with a 5 year LRFS and RRFS of 70% and 62% respectively. Overall, 8 patients (30%) had recurrences: 2 had distant alone, 2 regional, 2 regional and distant, 1 local and distant, and 1 had local, regional and distant recurrence.
Aggressive primary surgery in patients with PDTC showing gross ETE resulted in satisfactory locoregional control. Due to the small proportion of patients who received PORT (22%), it is not possible to analyze its benefit on locoregional control. Of significance is the observation that the majority of patients (60%) present with or subsequently develop distant metastases and eventually die of the distant disease. Further improvements in outcome therefore require new systemic therapies to target distant metastatic disease.
Surgery, University of Pittsburgh, Pittsbuth, PA
Thyroid Cancer Friday Oral Clinical 3:30 PM
To exclude or confirm thyroid cancer, accurate evaluation of thyroid nodules is important. Molecular testing of fine needle aspiration (FNA) specimens can help diagnose thyroid cancer although the added cost has not been studied. Our objective was to ascertain if routine molecular testing of FNA specimens in two indeterminate categories (follicular lesion of undetermined significance and follicular neoplasm) can be cost-saving.
A decision tree model was constructed to compare the estimated costs of thyroid nodule evaluation according to the current ATA guidelines either with routine molecular testing (MT) or without (standard of care, StC). Estimates of the probability values were based on a comprehensive review of recent literature and were limited to studies that used the Bethesda 2007 classification system. Cost of surgeries (thyroid lobectomy, total thyroidectomy, and completion thyroidectomy) were calculated from inpatient hospital costs obtained from the Healthcare Costs and Utilization Project, included surgical complication rates, and accounted for an estimated proportion of outpatient surgeries. Estimates for physician fees, outpatient laboratory and medication costs were based on median 2010 Medicare Reimbursement rates for the corresponding CPT code.
Compared to StC, MT use was associated with a decrease in the number of necessary diagnostic lobectomies (StC 11.6% v. 8.2%). In this distributed risk model, initial total thyroidectomy was more frequent with MT use (19.6% v. StC 16.1%). Although MT use added a diagnostic cost of $2,936 to the cost of total thyroidectomy ($11,383), the additive cost was less than the comparable cost in the StC cohort of performing a lobectomy ($7,684) and completion thyroidectomy ($11,954) when indicated by final histologic results. When the cost of MT was varied in sensitivity analysis, cost-savings were demonstrated if molecular testing cost remained less than $1303.
Routine molecular testing of cytologically indeterminate FNA results can be cost-saving because of reduction in two-stage thyroid surgery. Appropriate use of emerging molecular testing techniques may help avoid unnecessary surgery to optimize patient care and improve resource utilization.
Radiology/Nuclear Medicine, Univ Michigan, Ann Arbor, MI
Thyroid Cancer Friday Oral Clinical 3:45 PM
We assessed the contribution of post-operative diagnostic 131-I SPECT-CT to staging in patients (pts) with differentiated thyroid cancer (DTC).
We studied 320 pts (219F; 101M, mean age 47.3±16.4, range 10–90) with DTC (289 papillary, 22 follicular and 9 Hurthle cell) with diagnostic 131-I planar and SPECT-CT. Initial staging using AJCC TNM 7th ed. was based on clinical and pathology data (pTNM). Restaging then incorporated the findings from 131-I imaging. Results were analyzed separately according to age: young pts, age<45, n=138 (43%) and older pts, age≥45, n=182 (57%).
Initial pTNM staging classified all young pts (100%) as stage 1. However, imaging detected distant metastases (mets) in 5/138 (4%) thereby restaging to stage 2, while 133 (96%) remained stage 1. In 95 young pts with central neck dissection, histology revealed 20 (14%) without node mets (pN0), and 75 (54%) with nodal mets (pN1). In 43 (31%) without neck dissection (pNx), SPECT-CT characterized 33 as N0, and 10 as N1. Nodal disease was seen on imaging in 43 (31%) pts: 18 with pN0 or pNx changed to N1 due to detection of unsuspected nodal mets, and 25 with pN1 had additional nodal mets after surgery. The older pts were initially pTNM staged as: 48 (26%) stage 1; 23 (13%) stage 2; 65 (36%) stage 3; 45 (25%) stage 4A/B; 1 (<1%) stage 4C. After imaging pts were restaged as: 33 (18%) stage 1; 19 (10%) stage 2; 52 (29%) stage 3; 58 (32%) stage 4A/B; 20 (11%) stage 4C. Imaging upstaged 46 older pts owing to detection of distant mets in 19 (10%) and of regional mets in 27 (15%). In 119 older pts with central neck dissection, histology revealed 45 (25%) without node mets (pN0), and 74 (41%) with nodal mets (pN1). In 63 (35%) without neck dissection (pNx), SPECT-CT characterized 51 as N0, and 12 as N1. Distant disease was seen on imaging in 20 (11%) pts, and nodal disease in 37 (20%) pts: 19 with pN0 or pNx changed to N1 due to detection of unsuspected nodal mets, and 18 pN1 had additional nodal mets after surgery.
Diagnostic 131-I SPECT-CT detected regional disease in 22% and distant mets in 8% of pts. This led to upstaging in 4% of young and 25% of older pts. Compared with pTNM staging alone, 131-I hybrid imaging leads to more accurate staging.
Diagnostic 131-I hybrid imaging in a 56 year old woman with 1.2 cm papillary thyroid cancer without capsular invasion, no extra-thyroidal extension and negative surgical margins; no pathologic evidence for nodal disease (0/3 central nodes submitted); pT1b,N0,M0 stage I. Planar scan (A) depicts focal neck activity (arrowhead) corresponding on SPECT-CT (B) to thyroid remnant; and focal activity in the liver (arrow) corresponding on SPECT-CT (C) to 0.8 cm hypodense lesion also confirmed on liver US and MRI, consistent with hepatic metastasis, restaging: pT1b,N0,M1 stage IVC disease. Subsequent 131-I scan (D) obtained at 6 months after 200 mCi (5.4 GBq) 131-I therapy documents interval resolution of liver metastasis and of thyroid remnant tissue; there is physiologic tracer distribution throughout the body.
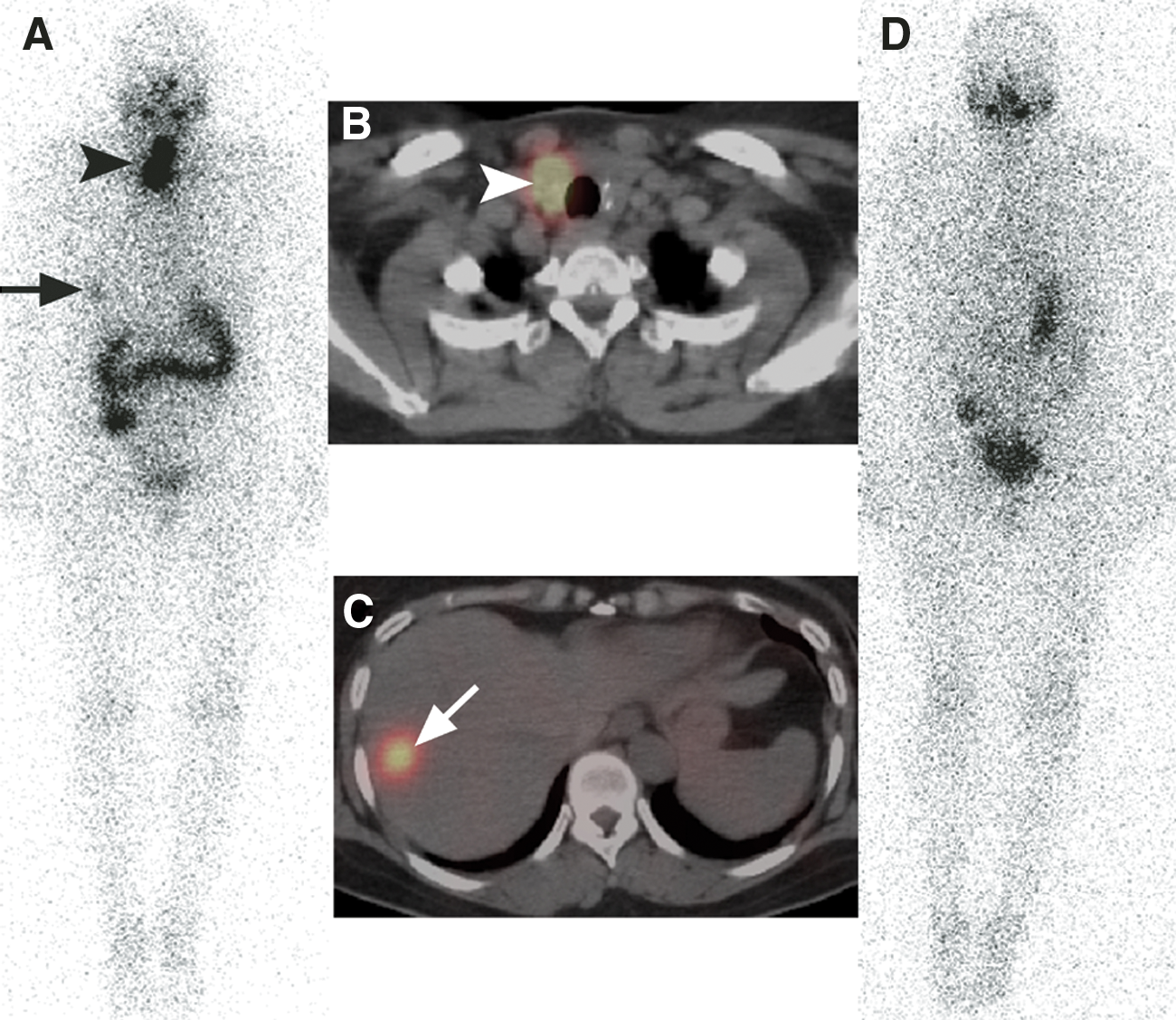
Essential Role Of GATA2 in the Negative Regulation of the Type 2 Deiodinase Gene by Thyroid Hormone
Thyroid Hormone Action Friday Oral Basic 2:30 PM
The negative regulation of the TSHβ gene by T3 is the central mechanism of the hypothalamus-pituitary-thyroid axis. In thyrotroph, T3 concentration is controlled by the type 2 deiodinase (D2), of which enzymatic activity is mainly regulated at the transcription level. The transcription factors, GATA2 and Pit1, determine the thyrotroph differentiation in pituitary and are necessary for the TSHβ expression. We previously reported that true transcriptional activator for the TSHβ gene is GATA2 while Pit1 stabilizes the function of GATA2, and that T3-bound T3 receptor (T3/TR) interferes with the transactivation by GATA2, resulting in the inhibition of the TSHβ gene. As in the case of the TSHβ gene, D2 mRNA is suppressed by T3; however its mechanism is unknown.
The humans D2 promoter was fused to the CAT- or Renilla luciferase gene, generating D2-CAT and D2-hRluc, respectively. They were cotransfected with expression plasmids for Pit1 or GATA2 into kidney-derived CV-1 cells, thyrotroph-derived TαT1 cells or somatotroph-derived GH3 cells. Gel shift assay and chromatin-immuno-precipitation (ChIP) assay with TαT1 cells were performed to detect GATA2 binding with the D2 promoter.
GATA2 but not Pit1 activated the D2 promoter. GATA2-dependent activity was enhanced by the proteins kinase A activator, forskolin. Deletion analysis revealed the existence of two GATA responsive elements (GATA-REs) close to cAMP responsive element. In TαT1 cells, the transactivation by GATA2 was abolished by mutations of the GATA-REs. Gel shift assay and ChIP assay indicated the GATA2 binding with these GATA-REs. When CV1 cells were cotransfected with expression plasmids for GATA2 and the pituitary specific TR, TRβ2, T3 suppressed the activity of D2-CAT. T3 also inhibited the activity of D2-hRluc in GH3 cells over-expressed with GATA2. The inhibition by T3/TRβ2 was dominant over the effect of forskolin on the D2 promoter activity driven by GATA2.
As in the case of the TSHbβ gene, the activation of the D2 promoter is maintained by GATA2 and its activity is repressed by T3/TR.
Signal Transduction Laboratory, Ordway Research Institute, Albany, NY
Thyroid Hormone Action Friday Oral Basic 2:45 PM
A cell surface receptor for thyroid hormone that activates extracellular-regulated kinase (ERK 1/2) has been identified on integrin αvβ3. We examined the actions of thyroid hormone, initiated at the integrin, on proliferation of human NCI-H522 non-small cell and NCI-H510A small cell lung cancer cells.
The methods have been described in our prior publications.
At a physiologic total hormone concentration (10–7 M), T4 significantly increased proliferating cell nuclear antigen (PCNA) abundance in these cell lines; 3,5,3′-triiodo-L-thyronine (T3) at a supraphysiologic concentration also enhanced proliferation. Neutral-izing antibody to integrin αvβ3 and an integrin-binding Arg-Gly-Asp (RGD) peptide each blocked thyroid hormone-induced PCNA expression. Tetraiodothyroacetic acid (tetrac) lacks agonist thyroid hormone function, but inhibits binding of T4 and T3 to the integrin receptor; tetrac eliminated thyroid hormone-induced lung cancer cell proliferation and ERK1/2 activation in both cell lines. In these estrogen receptor-α (ERα)-positive lung cancer cells, thyroid hormone (T4>T3) caused phosphorylation of ERα. The specific ERα antagonist ICI 182,780 (fulvestrant) blocked T4-induced, but not T3-induced, ERK1/2 activation. ICI 182,780 also inhibited thyroid hormone stimulation of ERα phosphorylation, proliferating-cell nuclear antigen (PCNA) expression and hormone-dependent thymidine uptake by tumor cells. In summary,in ERα-positive human lung cancer cells, the proliferative action of thyroid hormone initiated at the plasma membrane is mediated by ERα.
Thyroid hormone may be one of several endogenous factors capable of supporting proliferation of lung cancer cells. In ERα-positive human lung cancer cells, enhancement of cell proliferation by T4 requires crosstalk with the estrogen receptor. Activity as an inhibitor of lung cancer cell proliferation induced at the integrin receptor makes tetrac a novel anti-proliferative agent.
The Hepatic Inflammatory Response Involves Deiodinase Type 2 Induction Which is Independent from Serum T3—A Role for Macrophages
Thyroid Hormone Metabolism and Regulation Friday Oral Basic 3:00 PM
The occurrence of organ- and timing specific changes in deiodinase expression during illness suggests an important pathophysiological role for these enzymes in tissue function. During illness increased expression of type 2 deiodinase (D2) has been observed in tissues expressing very low D2 levels under normal conditions. In the present study we evaluated D2 expression in liver of mice with acute inflammation, chronic inflammation or hypothyroidism and in a variety of cell lines after stimulation with bacterial endotoxin (LPS).
In vivo models: •Acute inflammation in mice induced by administration of LPS (<24h).
•Chronic inflammation in mice induced by a turpentine injection in the hindlimb (<5 days).
•Hypothyroidism in mice induced by low-iodine/PTU or control diet (6 weeks).
In vitro models: HepG2 (hepatoma), THP1 (monocytes) and RAW264.7 (macrophages) cells stimulated with LPS and cultured for 8h. IL-1β, D2, TRα and TRβ mRNA were measured using qPCR. Serum T3 was measured using RIA
Liver D2 mRNA was 500-fold upregulated 4–24h after LPS administration and 10-fold after the induction of chronic inflammation. D2 mRNA expression was positively associated with liver IL-1β mRNA expression in both conditions (acute: r=0.712, P<0.01 chronic: r=0.523, P<0.01). During acute illness, D2 mRNA was negatively associated with low serum T3 levels (r=−0.400, P<0.01). Hypothyroidism did not influence liver D2 mRNA expression in any significant way. LPS stimulation of HepG2 cells did not induce D2 mRNA, while stimulation of both THP-1 and RAW cells resulted in significant D2 mRNA expression both after 4 and 8h, accompanied by an increase in TRα1 mRNA.
Both acute and chronic inflammation induce hepatic D2 mRNA. Low serum T3 levels per se in the setting of hypothyroidism do not induce liver D2. Furthermore, LPS induces D2 mRNA in a monocyte and macrophage cell line, but not in a hepatocyte cell line, which suggests liver macrophages being the source of liver D2 during illness. Finally, the presence and regulation of TRα1 mRNA in a macrophage cell-line support the macrophage as a potential target cell for T3-action during inflammation.
Physiology and Neurobiology, Dartmouth Medical School, Lebanon, NH
Thyroid Hormone Metabolism and Regulation Friday Oral Basic 3:15 PM
Fasting induces rapid changes in thyroid hormone (TH) economy characterized in rodents by decreases in serum thyroxine (T4) and 3,5,3′-triiodothyronine (T3) levels, whereas the serum TSH level remains normal. The types 1, 2 and 3 deiodinases (D1, D2, D3) have been postulated to play important roles in these changes. The goal of these studies was to examine the mechanisms underlying these phenomena.
Experiments were performed in transgenic mice deficient in one, two or all three deiodinases, Mice were fasted for 30h. Serum TH and TSH levels, and tissue TH contents were measured by radioimmunoassay. 5-Deiodinase activity was determined by our published method.
Mice deficient in either the D1, D2 or both enzymes (D1/D2KO) showed fasting-induced decreases in serum T4 and T3 levels equal to or greater than that observed in wild type (WT) animals (43% decrease in T4, 23% decrease in T3). The serum TSH level in all groups was unchanged, as was the tissue contents of T4 and T3 in liver, kidney and muscle. Following an injection of [125I]T4 or [125I]T3 into WT mice, the content of radioactivity in the majority of tissues in the fasting state was increased approximately 2-fold or 4-fold, respectively, due presumably to the accumulation of iodothyronines other than T4 and T3. D1/D2KO mice showed the same distribution of radioactivity. D3 activity was increased in kidney, muscle and liver up to 4-fold during fasting and the production of rT3, a reaction product of the D3, was significantly increased. Notably, fasted mice deficient in only the D3, or in all three deiodinases (D1/D2/D3KO), still showed significant decreases in serum T4 and T3 levels compared to fed animals.
In conclusion, alterations in D1 and D2 activities observed during fasting appear to play little, if any role in the characteristic pattern of serum TH and TSH levels observed in this condition. Rather, the decreases in circulating T4 and T3 appear secondary, in large part, to an increased retention and metabolism of TH in tissues, which may be due in part to enhanced D3 activity.
NIDDK, NIH, Bethesda, MD
Thyroid Hormone Metabolism and Regulation Friday Oral Clinical 3:30 PM
Obesity is a source of considerable morbidity and early mortality in the U.S., and it is the result of a sustained imbalance between energy intake and energy expenditure (EE). In sedentary individuals, resting energy expenditure (REE) may account for up to 85% of total energy expenditure. Thyroid hormone (TH) and particularly triiodothyronine (T3) play a critical role in the modulation of REE and substrate metabolism. Limited information is available on the effects of prolonged weight loss on TH homeostasis. The aim of the study was the evaluation of changes in TH homeostasis in response to a controlled weight loss dietary intervention.
32 Control (19M, 13F, BMI 21.9±1.9 kg/m2) and 47 overweight Subjects (15M, 32F, BMI 34.12±4.6 kg/m2), aged 25–45 years were enrolled in the study. All volunteers were healthy, as determined by medical history and laboratory tests, with no history of thyroid disease. Baseline procedures included: blood and urine sampling, anthropometry, body composition by DEXA, and REE evaluation by indirect calorimetry. Overweight subjects underwent a one-year individualized calorie-restricted diet (≈600 Kcal/day deficit) and were encouraged to increase physical activity, achieving an average rate of weight loss of 0.8±2.3 kg/month. Measurements were performed at 0, 1.5, 3, 6, 9, and 12 months. To date 27 subjects completed the study, 5 subjects completed 5, 8 subjects completed 4, and 7 subjects completed 3 follow-up visits.
Baseline T3 levels in overweight and control subjects correlated with fat mass (r2=0.073, p<0.02). Over the study period the dietary intervention resulted in a decrease in T3 levels (11.14±19.7 ng/dL), which correlated significantly with the weight loss (r2=0.114, p<0.0001). In contrast, no significant correlations were observed between fat mass and free thyroxine (T4) or thyroid-stimulating hormone (TSH) levels.
Our results indicate that T3 is a sensitive index of body weight changes, and that weight loss produces sustained changes in this parameter without affecting TSH or free T4. Taken together, the data suggest that weight loss affects the peripheral conversion of T4 into T3 with limited effects on the central TH homeostasis.
Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN
Disorders of Thyroid Function Friday Oral Clinical 3:45 PM
Heterophile antibodies, or human anti-animal antibodies, are known to affect a variety of immunoassays, including commonly used assays for thyroid stimulating hormone (TSH). Because TSH is widely used as the primary tool to detect thyroid disease, erroneous TSH results caused by heterophile antibody interference could pose a risk to accurate diagnosis and treatment of patients. In the latter half of 2010, Mayo Clinic Laboratories noted a sustained increase in potentially erroneous TSH results using the BCI Access® Assay. We therefore sought to evaluate the prevalence of heterophile antibody interference in patient samples using this assay and to determine its clinical impact.
All physician-ordered TSH samples received with results ≥10.0 mIU/L (Oct–Dec 2010; n=388 from 14,600 total tests) were re-assayed using the alternative Roche Elecsys® TSH immunoassay. Potential heterophile antibody interferences were identified when BCI and Roche TSH results differed by ±20% and confirmed by treating samples with Scantibodies HBT heterophile antibody blocking reagent and retesting. In addition, 970 consecutive physician-ordered TSH samples with BCI TSH results <9.9 mIU/L were tested in the same way.
For the samples where the BCI TSH results were ≥10.0 mIU/L, heterophile antibody interference using the BCI assay was confirmed in 17/388 (4.4% prevalence). Results were concordant between the BCI and Roche methods in 970 TSH samples with results <9.9 mIU/L. Of the 17 samples with confirmed heterophile antibody interference, accurate TSH concentrations were actually <10.0 mIU/L in all cases (3 patients <0.10 mIU/L, 9 patients 0.3–5.0 mIU/L, 5 patients 5.0–10.0 mIU/L).
The prevalence of heterophile antibody interference with the BCI Access® TSH assay in samples with TSH results ≥10.0 mIU/L was 4.4%. In all cases of confirmed heterophile antibody interference, the accurate TSH concentration was <10.0 mIU/L. These patients were therefore at risk of having erroneous diagnoses of hypothyroidism or having preexisting treatment with thyroid hormone adjusted inappropriately. Laboratories using the BCI Access® TSH assay need to be aware of the prevalence of heterophile antibody interference and potential risk to patients.
Dept. of Molecular Medicine, Nagasaki University, Nagasaki, Japan
Autoimmunity Friday Poster Basic
We have recently shown that wild type (wt) mice are highly tolerant, while thyrotropin receptor (TSHR) knockout (KO) mice are susceptible, to immunization with the mouse (m) TSHR, the autoantigen in human Graves' disease. However, because TSHR KO mice lack the endogenous TSHR in their thyroids, Graves'-like hyperthyroidism cannot be expected in these mice. Therefore, we performed adoptive transfer of splenocytes from TSHR KO mice immunized with adenovirus expressing mTSHR A-subunit (Ad-mTSHR A-subunit) into immune-deficient athymic nude mice expressing the endogenous TSHR in their thyroids as well as in orbital tissues.
TSHR KO BALB/c mice were immunized with Ad-mTSHR A-subunit twice at 3-week-intervals. A group of mice was also treated by anti-CD25 antibody. Splenocytes were prepared 2 weeks later, and adoptively transferred to nude BLAB/c mice. Bloods were taken regularly for T4 and TSHR antibody measurements. Thyroid and retro-orbital histology were also examined.
Circulating anti-TSHR autoantibodies were detected in ∼50 % recipient nude mice 4 weeks after adoptive transfer of splenocytes (5x10e7/mouse) from TSHR KO mice immunized with Ad-mTSHR A-subunit and persisted for 24 weeks. Depletion of regulatory T cells by anti-CD25 monoclonal antibody in donor mice increased successful transfer rates without increasing TSHR antibody levels. Some recipient nude mice showed a transient increase in T4 levels 4–8 weeks after transfer, but many became hypothyroid (subnormal T4 and high TSH) 24 weeks later. Moreover, in addition to sparse lymphocyte infiltration in the thyroid glands, macrophage infiltration was observed in the retro-orbital fat tissues and extraocular muscles in a small fraction of the recipients.
Our findings demonstrate successful adoptive transfer of anti-TSHR autoimmune response from TSHR KO mice to nude mice. Although development of hyperthyroidism was transient and infrequent, induction of orbital lesions suggests that anti-TSHR immune response appears to at least partly play a role for the development of Graves' orbitopathy.
Induction of Immune Tolerance in Mice with a Novel Mucosal Nanoemulsion Adjuvant and Autoantigen
Autoimmunity Friday Poster Basic
Experimental autoimmune thyroiditis (EAT) is inducible in mice by immunization with murine thyroglobulin (mTg) and adjuvants. Several approaches have tried to prevent the development of EAT, often by raising the mTg concentration in the blood of immunized animals to induce tolerance. Our previous study has shown that a low-dose administration of mTg in nanoemulsion (NE) can suppress the autoimmune response and prevent EAT development. In the current study, we investigated the mechanism of the blocking effect of administered mTg in NE on subsequent EAT development.
CBA/J female mice received NE or NE+mTg by nasal twice. Then, all mice were immunized with mTg and LPS to induce EAT. Compared with mice that received NE alone, mTg-NE-treated mice developed a milder form of thyroiditis with significantly decreased mononuclear cell infiltration in the thyroid. To investigate whether regulatory T cells (Tregs) play a role in the reduction of anti-mTg immune responses, the proportion of Tregs in the spleen and lymph node cells (LNC) of mice were measured. To further study of mTg-NE trafficking in vivo, a mixture of highly fluorescent silica-based quantum dots (QDOTs), NE and mTg was nasal delivery to mice. The QDOT fluorescence was detected and imaged using a Xenogen Bioluminometer.
The percentage of splenic CD4+ CD25+ FoxP3 cells was similar between mTg-NE- and NE-treated mice. However, the percentage of CD4+ CD25+ Foxp3 cells from the cervical LNC of mTg-NE treated mice was higher than that from the NE-treated mice. Furthermore, the expressions of Foxp3 and TGF-β in the thyroid of mTg-NE-treated mice were significantly enhanced compared to NE-treated mice. In addition, a significant increase in the QDOT fluorescence was detected at 24 hours in mice treated with QDOT+mTg+NE as compare to mice treated with QDOT+mTg.
Collectively, these results suggest that the inhibition of autoimmune responses by the combination of mTg and NE could be related to Tregs expansion and increased antigen uptake by NE.
Iodine-Mediated Induction of TH17 Cell Polarization as well as Inhibition of CD3+ FOXP3+ Regulatory T Cells in the Pathogenesis of Hashimoto's Thyroiditis
Autoimmunity Friday Poster Basic
Hashimoto's thyroiditis (HT) is the most commonly encountered autoimmune thyroiditis that is characterized by the presence of thyroid auto antibodies and varying degrees of destruction of thyroid follicular cells. Although the clinical prognosis of HT is hardly life-threatening, its autoimmune process remains to be clarified. High iodine level is reported to be associated with the pathogenesis of HT and other thyroid disorders, however, the exact pathological mechanism is unclear. Moreover, whether aberrant level of iodine plays a role in the autoimmune process has not been explored.
Recently emerged Th17 cells as well as IL-17 play a vital role in numerous autoimmune processes. Thus, we first investigate whether IL-17 and Th17 cells are present in patients with HT. To further explore the possible link between high iodine level and the autoimmune process of HT, we adopted the bovine thyroglobulin immunized mice feed with various levels of NaI for over three months as the autoimmune thyroiditis model.
Compared with that of healthy individuals, our data demonstrated an elevated serum IL-17 concentration and an increased intra-thyroid infiltrating Th17 cell frequency. Interestingly, the concentration of IL-17 declined progressively with respect to patients' residual thyroid function. In vivo study showed that moderate high level of feeding iodine (1500μg/L) facilitates the polarization of splenic naïve T cells into Th17 cells, while in extreme high level condition (12000μg/L), iodine redirects T cell differentiation into Th1 polarization. Meanwhile, iodine inhibits the frequency of systemic and splenic CD3+Foxp3+ regulatory T cells in a dose dependent manner. Unfortunately, the shift of Th17/Th1 polarization in vitro is not observed, indicating that iodine may function indirectly on immune system.
Our data suggests that HT might be a Th17 cell mediated disease, in which high level of iodine plays a critical role in the pathogenesis of HT through directing T cell differentiation.
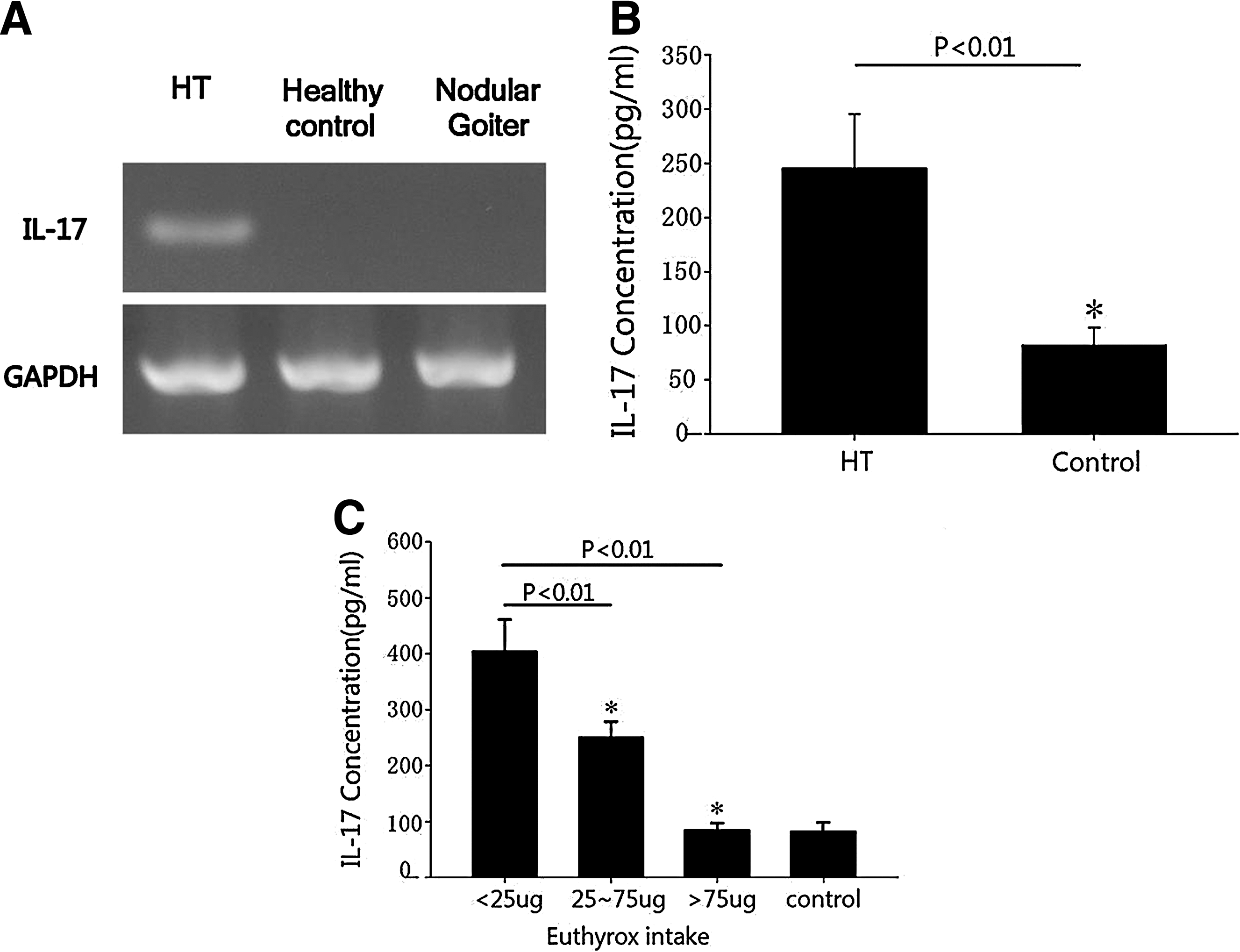
Iodine-mediated induction of Th17 cell polarization as well as inhibition of CD3+ Foxp3+ regulatory T cells in the pathogenesis of HT.
Autoimmunity Friday Poster
Pregnancy and the postpartum (PP) period are characterized by profound and rapid emotional changes, and endocrine changes. Most PP psychometric evaluations target D, and show a link with TAb, not with thyroid function. Only 3 PP studies (2/3 on 77 or 79 women; 2/3 on PP day 1 or 3) evaluated AT, but none its relationship with thyroid indices. AT, which affects ≈10% of women, is the inability to describe emotions with words. AT persons have (or risk to have) D and other psychiatric disorders.
We tested 74 women aged 31.8±4.6, on day 3 PP, by the Edinburgh Postnatal Depression Scale (EPDS), the Montgomery and Asberg Depression Rating Scale (MADRS), and the Toronto Alexithymia Scale (TAS). Concurrently, we measured serum TSH, TH (FT3, FT4), TAb (TPOAb, TgAb). Women were selected based on absence of personal and familial history for any psychiatric disorders, any thyroid disease, and based on other criteria.
Using cut-off scores of ≥12 (EPDS), ≥15 (MADRS) and ≥61 (TAS), rates of abnormal women were similar (31%, 30% and 28.4%). TAS scores were higher and rates of AT were greater in the abnormal EPDS group or in the abnormal MADRS group than in the normal EPDS or MADRS group. EPDS correlated with TAS (r=0.24, P=0.04), matching r=0.21 in 1/3 previous studies. Compared to nonAT women, AT women had lower FT4, higher FT3, lower FT4:FT3 ratio, and insignificantly higher TPOAb or TgAb levels. Only TPOAb and TgAb were significantly higher in D women vs. nonD women, but at EPDS cut-off values of ≥13 or ≥14. TAS correlated directly with TPOAb (r=0.20, P=0.08) and FT3 (r=0.28, P=0.017), and inversely with FT4:FT3 ratio (r=−0.34, P=0.003), while EPDS correlated only with TPOAb (r=0.22, P=0.056). Compared with women normal on all 3 scales, pure D women had lower FT3 and higher FT4:FT3 ratio, while pure AT women had lower FT4 and FT4:FT3 ratio.
The rate of AT in PP women is >in general population women. PPD risk and AT are partly comorbid and associated directly with thyroid autoimmunity. However, AT is also associated with serum TH (FT3 directly, FT4 and and FT4:FT3 ratio inversely). This is of interest, since brain is a target for TH and AT is viewed as a disconnection between the limbic system and neocortex.
Medicine I, Gutenberg University Medical Center, Mainz, Germany
Autoimmunity Friday Poster Clinical
Limited data exist on the role of thyroid stimulating immunoglobulins (TSI) in the management of Graves' disease (GD). In a prospective clinical trial, we aimed to test the hypothesis that TSI levels are useful for predicting response to therapy and/or relapse.
Seventy untreated hyperthyroid subjects with GD were treated with antithyroid drugs (ATD) for 24 weeks. Subsequently, patients were divided into responders (normal thyroid hormone levels) and non-responders. In responders ATD were terminated whereas non-responders remained on treatment for additional 12 weeks. Serum TSI levels were measured at baseline, at 4, 8, 12, 24 and 36 weeks after starting ATD with a FDA-cleared TSHR bioassay (Thyretain) and expressed as the percent specimen-to-reference-ratio (SRR%).
To date 45 hyperthyroid GD patients (35 female, 28 with orbitopathy, GO) have completed the 24 week ATD treatment (interim analysis). 15 of 45 (33%) were responders, 10 female (66%), 9 younger than 50 (60%), 7 (46.7%) with GO. Of 30 non-responders, 21 (70%) had GO, 25 were female (83.3%) and 19 were younger than 50 (63.3%). In the non-responder group, baseline TSI levels were markedly higher in GD+GO vs. GD patients (median SRR% 425 vs. 358, 18.7%), whereas this difference was larger in the responder group (410 vs. 300, 37%). At week 24, TSI levels decreased markedly in all responders (374 vs. 218, Δ minus 41.7%, p<0.05). The decrease was more significant in those with GD only (300 vs. 195, Δ minus 35%) compared to GD+GO (410 vs. 341, Δ minus 16.8%). In contrast, TSI levels increased in all non-responders from 397 to 445, Δ plus 12%).
Response to ATD is higher in patients with thyroidal GD only and is accompanied with significant decrease in TSI levels. In contrast, TSI levels remain unchanged or increase in non-responders, most of whom have systemic GD.
Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Republic of Korea
Autoimmunity Friday Poster Clinical
The role of vitamin D as an immune modulator has been emphasized in recent years, and low levels of the hormone were observed in several autoimmune diseases. Vitamin D levels were found to be lower in patients with AITDs than in healthy volunteers in one study, and in Graves' disease patients when compared to patients with non-AITDs. Significantly low levels of vitamin D were documented in patients with AITDs that were related to the presence of anti-thyroid antibodies and abnormal thyroid function tests, suggesting the involvement of vitamin D in the pathogenesis of AITDs and the advisability of supplementation. To determine the effect of baseline serum vitamin D level on hyperthyroidism in patients with untreated Graves' disease, we performed retrospective study.
44 patiens were divided by 2 groups based on baseline serum 25-hydroxy-vitamin D (25(OH)D) level (vitamin D deficient group (25(OH)D<10 ng/mL), n=21, vitamin D non deficient group (10 ng/mL≤25(OH)D), n=23). All patients receive a daily dose of 15 mg methimazole (MMI). These treatment regimens were continued. Mean follow up duration was 24 weeks. Physicians were allowed to adjust MMI dosage during follow up visits. Blood samples were collected, and serum concentrations of free triiodothyronine (FT3), free thyroxine (FT4), T3, thyrotropin (TSH), TSH-receptor antibody (TRAb), and Thyroid stimulating antibody (TSAb) were determined.
All patients became euthyroid after treatment. The dose of MMI was not significantly different between these two groups. In contrast, decreases in mean serum T3 and FT4 levels were greater in vitamin D non deficient group. Correspondingly, the reciprocal increase in the mean TSH level was more prominent in vitamin D non deficient group. Mean TRAb and TSAb levels did not differ between the two groups at baseline. However, decreases in TRAb and TSAb levels were greater in vitamin D non deficient group.
We suggest that baseline vitamin D level may affect the outcome of Graves' disease.
Internal Medicine, Maryknoll Medical Center, Busan, Republic of Korea
Autoimmunity Friday Poster Clinical
There have been controversial reports linking Helicobacter pylori (H pylori) infection to autoimmune thyroid disorders (ATD). There are some data which demonstrates more frequent H pylori infection in ATD patients. However, data regarding the relationship between H pylori infection and thyroid autoimmunity are limited in Korean population, who has extremely high prevalence of H pylori infection. We performed this study to investigate the prevalence of H pylori infection according to the presence of thyroperoxidase antibody (TPO Ab) in healthy adults without history of thyroid disease.
This study was done in adults aged from 30 to 69 years (median 52 years) who had visited the healthy promotion center at Asan Medical Center, Seoul, Korea, from Jan 2009 to Dec 2010. Subjects with previous thyroid disease were excluded. 5,325 subjects (2,286 females, 3,039 males) were analysed. Thyroid assessment was done by free T4, TSH and TPO Ab. Ig G Antibodies to H pylori (H pylori Ab) were determined as diagnosis of H pylori infection. We compared the prevalence of positive TPO Ab between subjects with positive H pylori Ab and negative H pylori Ab.
TPO Ab was positive in 278 women (12.2%) and 154 men (5.1%). H pylori Ab was positive in 2,787 (52.3%), out of 5,323 subjects. Prevalence of TPO Ab was more higher in subjects with positive H pylori Ab (8.9 % vs 7.2%, P=0.024). After adjusting for age and sex, those with H pylori infection were more higher prevalence of TPO Ab (P=0.026).
In our study, prevalence of TPO Ab was more higher in subjects with H pylori infection. Our findings suggest H pylori infection might be a causative factor to autoimmune thyroiditis.
Division of Endocrinology and Metabolism, UCSF, San Francisco, CA
Autoimmunity Friday Poster Clinical
Thyroid function testing abnormalities are common among the elderly; 13% of individuals over age 80 without known thyroid disease have TSH levels above the reference range. The natural history of thyroid function and its relationship to survival is unknown in this population of the oldest old. We sought to examine changes in thyroid function tests over time and to assess the association between thyroid function, thyroid peroxidase antibodies (TPOAbs), and mortality in a cohort of individuals of advanced age.
TSH, free thyroxine, total T3, and TPOAbs were measured from samples obtained at the 1992–1993 and 2005–2006 study visits in 1049 participants enrolled in the Cardiovascular Health Study All Stars Study (mean age 85.6±3.8 years in 2005–2006, 64% women, and 16% African American). The overall and annual change in TSH, free thyroxine, and total T3 was calculated over the 13 year period between visits in 649 individuals not taking thyroid medication. Age, sex, and race-adjusted Cox proportional hazards models were constructed to determine the relationship between TSH levels and TPOAb status at the 2005–2006 visit and incidence of death.
At the 2005–2006 visit, 88% of participants not taking thyroid medications were euthyroid (n=739) and subclinical hypothyroidism was the most common thyroid function abnormality, affecting 10% of the cohort (n=85). We found a small but statistically significant increase in TSH (0.32mU/L, p<0.01) and FT4 (0.02ng/dL, p=0.01), and decrease in TT3 (−0.23 nmol/L, p<0.01) in the 13 years between assessments. The median annual rate of change of TSH in those who reported no thyroid medication use was 0.017 mU/L/y. We found no association between TSH level at the 2005–2006 visit and death (HR=0.95, 95% CI 0.89–1.02), or TPOAb status and death (HR=1.03, 95% CI 0.65–1.61) over a median follow-up time of 4.8 years.
In this cohort of individuals of advanced age, there was a slight increase in TSH and free thyroxine and decrease in total T3 over a 13 year period. Neither TPOAb status nor TSH levels were associated with mortality. These findings suggest an age-related change in deiodination of T4 that is without clinical significance.
Department of Medicine, The University of Chicago, Chicago, IL
Disorders of Thyroid Function Friday Poster Clinical
Although inactivating thyrotropin receptor (TSHR) gene mutations are not uncommon causes for resistance to TSH they were particularly common in Arab tribes living in Northern Israel. In fact our laboratory has identified 6 distinct TSHR mutations in this population (P68S, L89L, Q90P, P264S, R609X and L653V) and in one tribe the frequency was 4.3%. In a large kindred of 30 individuals (Fam A) 3 nucleotide substitutions were identified in exon 3 producing Q90P and one in exon 9 of the same allele producing P264S. Another family of 9 individuals, reported herein (Fam B), belonging to a different tribe harbors only the 3 nucleotide substitution in exon 3. The aim of this study was to determine if the mutations have common ancestral origin.
Clinical and genetic studies. All coding regions of the TSHR were sequenced and microsatellite markers spanning the TSHR locus (5.19 cM) were used for haplotyping.
Two siblings of Fam B with congenital hypothyroidism were compound heterozygous for TSHR gene mutations. The paternal allele contained 3 nucleotide substitutions in exon 3 producing Q90P. The maternal allele harbored a missense mutation in exon 10 producing L653V. Using genetic markers spanning the TSHR locus, we investigated the possibility of a founder effect with subsequent mutational events for the presence of the same exon 3 mutation in different families. The haplotype of the TSHR allele harboring the mutation in exon 3 in Fam B was identical to the haplotype of the TSHR allele in Fam A, except for the presence of the mutation in exon 9 in Fam A, indicating that this P264S mutation occurred subsequently. Interestingly, wild-type TSHR haplotype was present in Fam B, indicating that the mutation in exon 3 was also a new mutational event in the history of that population.
It is possible that 2 consecutive mutational events occurred on the original wild-type allele generating the allele with both exon 3 and exon 9 mutations, instead of a recombination event that brought exon 3 and exon 9 mutations together on the same allele. We hypothesize that new mutation events contribute to the high prevalence of TSHR mutations in this population in addition to a founder effect and limited gene pool due to inbreeding.
Subacute Thyroiditis de Quervain: Clinical Features and Outcome in 273 Patients
Disorders of Thyroid Function Friday Poster Clinical
As literature on subacute thyroiditis is very scarce, we have retrospectively evaluated data from 273 patients diagnosed with subacute thyroiditis 1990–2010.
To be included in the study, patients had to show 4 of the 7 following symptoms or findings: 1.local pain, 2.fever, 3.increased sedimentation rate, 4.suppressed Tc-uptake in thyroid scan, 5. subclinical or manifest hyperthyroidism, 6. positive cytology, 7. rapid relief with prednisolone.
Clinical findings and technical patient details: (n=number of patients): A. Data at first visit: Sex: female/male n=226 (83%)/47 (17%). Age: <40/41–50/51–60/>60 years n=82 (30%)/97 (36%)/66 (24%)/28 (10%). Clinical findings: local pain/fever n=243 (89%)/73 (27%). Thyroid volume (ultrasound): <20 ml/20–40 ml/>40 ml n=62 (27%)/160 (59%)/49 (14%). Tc uptake (thyroid scan): <0.2/0.3–0.5/0.6–0.9/>0.9%: n=76 (32%)/106 (43%)/40 (17%)/18 (8%) (analyzed pat. n=240). Sedimentation rate: <30/30–49/>50mm/h: n=50 (18%)/101 (37%)/122 (45%). Thyroid status: euthyroid/subclin.hyperth./hyperth./hypoth.: n=76 (28%)/76 (28%)/121 (44%)/0. TPO- and/or Tg-antibodies: positive/negative: n=73 (30%)/171 (70%) (analyzed pat. n=244). B. Time course (Pat. receiving prednisolone were instructed to halve the initial dose, when local pain had ceased (mostly after 3–4 days). After a further 3–4 days the dose was again halved and this was repeated until pain returned, when the dose was doubled once again. After 1–2 weeks without pain, a further attempt was made to reduce the dose.) Initial dose of prednisolone: 0/1–20/21–50/>50 mg/d: n=52 (19%)/150 (55%)/65 (24%)/5 (2%) After cessation of therapy, remission occurred after 1/2–3/4–6/>6 months: n=33 (21%)/54 (34%)/33 (21%)/40 (24%) (analyzed pat. n=160). Reduction of thyroid volume for 0–19/20–39/40–59/ 60–89/>90%: n=45 (22%)/45 (22%)/55 (26%)/55 (26%)/8 (4%) (analyzed pat. n=208). Thyroid function after 1–10 years: euth./subclin.hypoth./hypoth.: n=180 (92%)/9 (5%)/5 (3%) (analyzed pat. n=194).
1. Prednisolone (medium dose (20 mg/d) with rapid dose reduction after clinical improvement) seems to be the optimal regimen.
2. Late hypothyroidism is rare with this regimen.
Second Division, Department of Internal Medicine, Hamamatsu University School of Medicine, Hamamatsu, Japan
Disorders of Thyroid Function Friday Poster Clinical
Axitinib is a selective inhibitor of vascular endothelial growth factor receptors. Although thyroid dysfunction in axitinib-treated individuals was first reported in 2010, the etiology and clinical features remain elusive.
We describe four consecutive patients treated with axitinib for metastatic renal cell carcinoma and referred to our department because of thyroid dysfunction.
Four patients (4 men; mean age 63 years) were started on 5mg axitinib twice daily. Baseline thyroid function tests were within the normal range and thyroid autoantibodies were negative in all patients. Marked elevation of TSH was observed in every patient, reaching more than 100 μIU/mL, within 1 month of axitinib treatment. Two patients showed a transient thyrotoxic phase about two months after therapy. In spite of very high TSH levels, free T4 remained within normal limits in two patients and decreased only slightly in the other two patients.
Administration of 25–125 μg levothyroxine was started in every patient; however, TSH levels remained relatively high. TSH levels returned to normal or to the upper limit of the normal range at treatment interruption in all patients. Since the patients exhibited inappropriate elevation of TSH, which was resistant to levothyroxine treatment, we compared the serum free T4 and TSH in axitinib-treated patients with those in 140 outpatients with thyroid diseases in our institute. Interestingly, most serum in patients treated with axitinib apparently shifted to the right on the free T4 vs. TSH plot (see figure). Inappropriate elevation of TSH induced by axitinib may be due to attenuated biological activity of circulating TSH or an impaired hypothalamus-pituitary-thyroid axis.
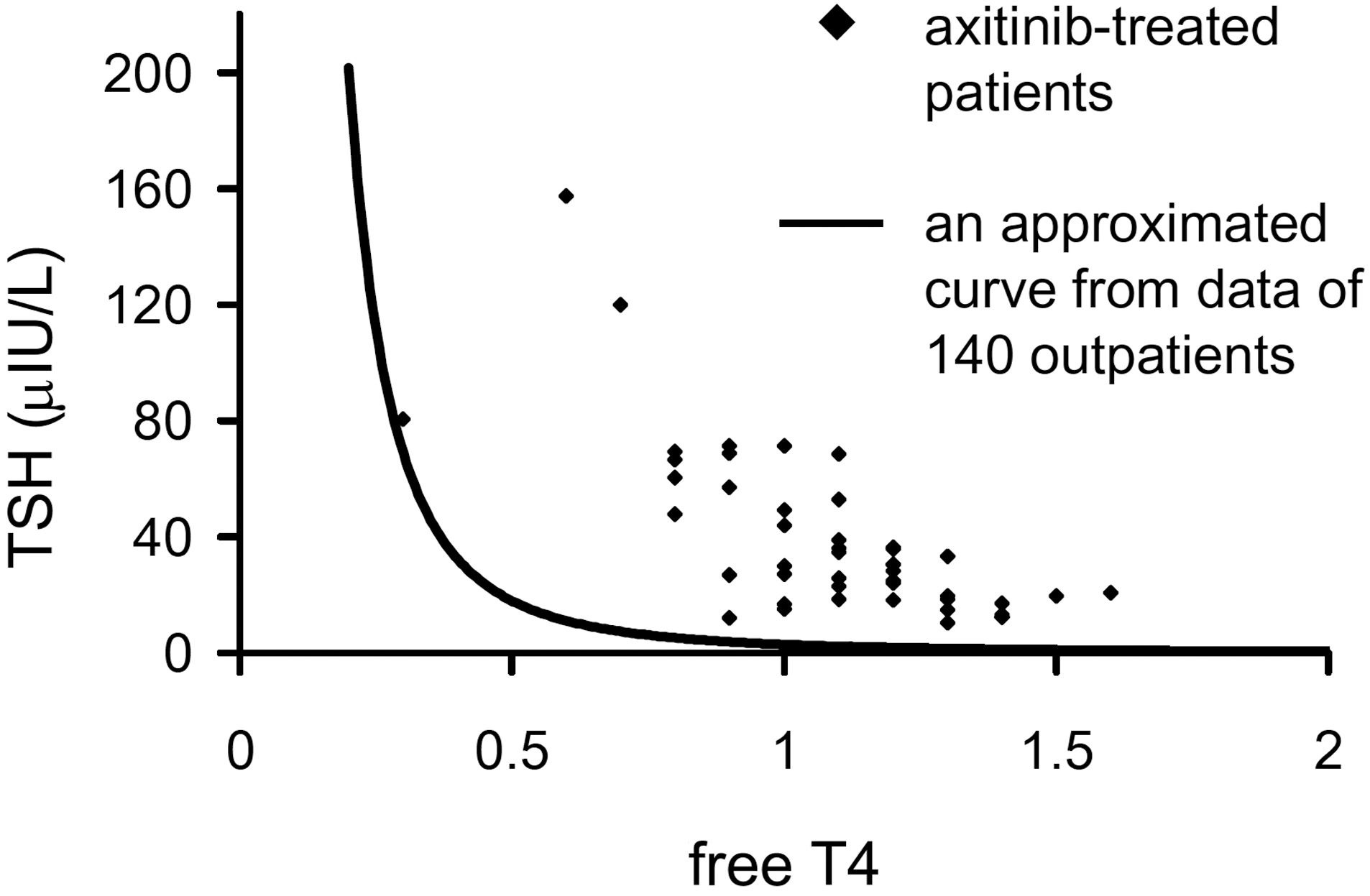
We report here a case series of axitinib-treated patients whose TSH levels were inappropriately elevated.
Black rhombus shows serum TSH and free T4 measurements in axitinib-treated patients. Solid line represents an approximated curve from data of 140 outpatients.
Thyroid Disorders Associated with Over-The-Counter Iodine Supplements: An Increasing Trend
Disorders of Thyroid Function Friday Poster Clinical
There is an increasing trend to self-prescribe over-the-counter iodine (OTC-I) supplements.
Adverse outcomes of using OTC-I are illustrated in the following 3 patients.
Case 1: 63 y/o female presented with 15-hrs of AF with RVR. Her AF had been controlled since initial presentation 5 yrs earlier. She reported taking Cataplex® F and Min-Tran® tablets for the last 3 years and self-discontinued them 1 month prior. HR 140/min, no goiter. Labs: TSH<0.006 μIU/mL; FT4 2.13 ng/dL; T3 164 ng/dL; TSI 96%; TBII<6.0%; ESR 11 mm/hr; plasma iodine 76 mcg/L; 24-hr urine iodine 237 mcg. I131 uptake was 0.9%. She started cholestyramine and a low iodine diet. Normal sinus rhythm was restored within 1 week.
Case 2: 38 y/o female presented with fatigue. Thyroid gland 30 gms. Labs: TSH 3.6 μIU/mL, TPO Ab 1910 IU/mL and TgAb 386 IU/mL. Six months later, she presented with overt hypothyroidism (enlarged thyroid 50gms, TSH 94 μIU/mL, TPO Ab 4670 IU/mL and TgAb 786 IU/mL). She was taking Iodoral™ tablets for 3 months. Plasma iodine was 428 mcg/L and 24-hr urine iodine was 3281 mcg. Iodoral™ was stopped and LT4 125 mcg was started along with low iodine diet. Over the next 4 months, thyroid functions improved.
Case 3: 35 y/o female presented with Graves' disease (Table). She improved with propylthiouracil (PTU) and atenolol. She returned with severe hyperthyroidism and increased TSI levels after taking OTC Tri-iodine™ for 3 months. Iodine levels were elevated. She began a low iodine diet and increased the doses of PTU and atenolol. Tri-iodine™ was discontinued.
Patient started taking Tri-iodine™ (Euro Pharm USA, contains 12.5 mg iodine) in Dec 2010. Tri-iodine™ was discontinued in Feb 2010. ND: not done.
Iodine excess has multiple effects on the thyroid gland, including Jod-Basedow's and Wolff Chaikoff effects. Partly reversible iodine-induced thyroid dysfunction through immune mechanisms has been described. All patients with thyroid disorders should be counseled on OTC-I use.
Surgery, UCLA, Los Angeles, CA
Disorders of Thyroid Function Friday Poster Clinical
Due to the high failure rate with antithyroid drugs, the treatment of pediatric Graves' disease relies on the definitive therapies of radioactive iodine (RAI) ablation and surgery (thyroidectomy). The optimal treatment choice between these two options remains controversial. This study compares the quality of life outcomes in children treated for Graves' disease with either RAI or surgery.
Patients who were treated for pediatric Graves' disease from 1988 to 2008 by either surgery (26) or RAI (43) were identified in the operative and radiation oncology databases of an academic medical center. All patients were mailed two quality of life (QOL) surveys. 1) A novel Graves' disease QOL questionnaire created by the authors focused on the changes in Graves' disease symptoms associated with treatment that were related to physical health, mental health, and social welfare. 2) The CHQ PF-28, a validated generic QOL questionnaire, measuring present-time QOL was also used to evaluate patients under 18 years of age.
Of the 69 patients, 55 (80%) were female. There was a 16% response rate to the surveys (6 patients from the surgery arm and 5 patients from the RAI arm). Follow up times ranged from 4 months to 6 years post-treatment. From the Graves' specific QOL survey, there was a statistically significant benefit from surgery in improving sleep habits and for resolution of eye disease as compared to RAI (Mann-Whitney U test, p<= 0.02). None of the RAI patients with eye disease improved (n=3). Even though the surgical arm patients reported more pre-treatment symptoms than the RAI group (p=0.0067), 95% of symptoms (42/44) resolved completely in the surgery arm as compared to 62% (13/21) in the RAI arm (Z test, p<0.001). There were no significant differences in each of the subscales of the CHQ PF-28 between the surgery and RAI groups (n=4 per group).
This study suggests that eye disease and sleep habits improve more with surgery than with RAI for treatment of pediatric Graves' disease. Of those with pre-treatment symptoms, there is a greater resolution rate with surgery than with RAI. Overall quality of life appears similar between the two treatments; however, a distinction may become apparent in a larger cohort.
Endocrinology, Hospital Curry Cabral, Lisbon, Portugal
Disorders of Thyroid Function Friday Poster Clinical
Familial PHP-Ib is a rare disease with difficulties in differential diagnosis. There is a resistance to PTH action, through its G-Protein-coupled receptor in the renal tubules, resulting from tissue-specific silencing of the G-protein alpha-subunit (Gsalpha), due to imprinting disruption of its encoding locus—GNAS (chromosome 20q13.3). In familial PHP-IB, maternally inherited deletions at the STX 16 gene are associated to a regional GNAS methylation defect. To study a Portuguese family in view to prevent hypocalcaemia—related complications through an early diagnosis and management of PHP-Ib.
We studied 14 elements of a family, including clinical presentation, hormone assays (calcium, phosphorus, Thyroid function tests, parathormone) and genetic study. Genomic DNA of each element was screened for 3 kb STX16 deletion, by amplification of a segment 4.3 kb of the gene for long range PCR.
The cohort was characterized: 4 elements symptomatic for PHP-Ib with the del 3 kb STX16 (2 females and 2 males, one of which with hypothyroidism), 4 elements asymptomatic with the del 3 kb STX16 (4 males) and 6 elements asymptomatic without the del 3 kb STX16 (4 females and 2 males).
The epigenetic study of this family permitted the identification of 8 elements with GNAS methylation defect (DMR 1A), responsible for the tissue-specific silencing of the Gs alpha and resistance to PTH in renal tubules. The deletion 3 kb STX16 was maternally inherited. Females can transmit the mutant allele to next generation, which present the disease independently of their sex. Males can transmit the mutant allele to next generation but the methylation defect and disease will not occur, independently of their sex. Although, if descendents have the genetic defect, they can transmit it to future generations. The genetic identification of hereditary form of PHP-Ib contributes to an early diagnosis and management of families with this disease.
Endocrinology, University of Wisconsin, Madison, WI
Disorders of Thyroid Function Friday Poster Clinical
The management of Graves' disease (GD) in childhood remains controversial as no treatment option is without risk. Thyroidectomy in children is typically associated with higher risk than in adults, and thyroidectomy for Graves' disease can be very challenging. Therefore our goal was to determine if the outcomes of thyroidectomy for Graves' disease were worse in children than they are in adults.
We retrospectively reviewed a prospective database of patients undergoing thyroidectomy for Graves' disease between May 1994 and December 2010. We evaluated the presentation and clinical outcomes in children and adolescents and compared this to adults also undergoing thyroidectomy.
14 children and 40 adults underwent thyroidectomy for GD during this period. The median age in these two groups was 15 years and 38 years respectively. The majority of patients were female in both groups. The presenting symptoms were similar in both groups however the time between diagnosis of disease was longer in the children vs. the adults (14.4 vs 13.7 months, p=0.02). Children were more likely to get a total thyroidectomy than adults (p<0.001). Mean hospital length of stay was 1.4 days in children vs. 1.2 days in adults (p=0.28). Transient hypoparathyroidism was significantly higher in children (31% vs 5%, p=0.04), but there was no difference in the occurrence of permanent hypoparathyroidism (p=0.55). No patients in either group had laryngeal nerve damage, infection or death. One child (7%) and three adults (8%) had recurrence of their disease (p=0.73), all of which had undergone subtotal thyroidectomy.
Signs and symptoms of GD in children were similar to those in adults; however adults had surgery closer to the onset of their disease than children. There was no difference in the length of hospital stay between the two groups. There was a higher incidence in only temporary hypoparathyroidism in children compared to adults. Surgical management of GD in children should therefore still be considered safe and effective when performed by experienced surgeons.
Internal Medicine, Marshfield Clinic, Marshfield, WI
Disorders of Thyroid Function Friday Poster Clinical
Amiodarone is a commonly used anti-arrhythmic drug that can lead to both hypothyroidism and hyperthyroidism. Amiodarone induced thyrotoxicosis (AIT) is a disease which poses a diagnostic and therapeutic challenge.
We report a 79 year old male who had been on Amiodarone 200mg daily for 2 years for atrial fibrillation. He presented with excessive sweating and feeling warm. Evaluation revealed low TSH 0.02 (normal 0.35–4.5 uIU/ml) and high free T4 of 4.8 (normal 0.6–1.2 ng/dL). Amiodarone was switched to Dronedarone, a noniodinated agent.
TPO antibody and Thyroid Stimulating Immunoglobulin were negative. The neck ultrasound showed no nodules and color doppler showed no increase in vascularity. The radioiodine uptake was low at 0.8% at 24 hrs. A diagnosis of AIT, most likely type 2 was established and treatment with methimazole and prednisone was initiated. Patient started feeling better and TSH and free T4 returned to normal in 6 weeks.
Amiodarone has significant adverse effects due to the high amount of iodine content. AIT poses a challenge to the clinician in both diagnosis and treatment. AIT type 1 occurs in pre-existing thyroid disease and is triggered by iodine overload. It is treated with antithyroid drugs. AIT type 2 is a form of destructive thyroiditis that occurs in an apparently normal thyroid and is treated with glucocorticoids. Although investigations such as radioactive iodine uptake scan and ultrasound with doppler are useful tools to distinguish one type from another, there is a mixed variant commonly encountered in clinical practice, in which both forms coexist. The decision to treat with one drug rather than both prednisone and methimazole carries the risk of inadequate treatment with higher mortality and morbidity. A safe approach would be to treat AIT with both antithyroid drugs and glucocorticoids initially, and subsequently alter therapy once patient is better.
The Link Between Respiratory Failure and Congenital Hypothyroidism
Disorders of Thyroid Function Friday Poster Clinical
Congenital hypothyroidism (CH) is common and has an incidence rate of 1 in 3000 to 1 in 4000 newborn infants. Thyroid dysgenesis and dyshormonogenesis are the usual causes of CH. We describe a patient with CH, microcephaly, and respiratory distress at birth, associated with a deletion in chromosome 14.
The subject is a male infant born at 37 weeks gestation via normal spontaneous vaginal delivery after an uncomplicated pregnancy. At birth, the patient had signs of respiratory distress. He was intubated, treated with 3 doses of Surfactant, and ventilated with high frequency oscillatory ventilation and nitric oxide for pulmonary hypertension. The state newborn screen, sent on DOL 2, revealed TSH 427 μIU/mL and total T4 1.2 μg/dL, consistent with CH. Synthroid was initiated. An ultrasound confirmed the presence of a thyroid gland in the neck. See table for subsequent bloodwork results and treatment. The subject was discharged home on DOL 73 with low flow oxygen and Synthroid. Follow up compliance has been poor.
Array comparative genomic hybridization (aCGH) at 7 weeks of age revealed 244.O Kb duplication at 3p26.3 encompassing the CHL1 gene and a 1.1 Mb deletion at 14 q 13.3q21.1. This deletion includes the OMIM gene NKX2–1, also known as thyroid transcription factor 1 (TTF1). Clinical features of a heterozygous deleterious mutation in the NKX2–1 gene include choreoathetosis, hypothyroidism, and neonatal respiratory distress (OMIM #610978). Parental microarray analyses revealed that the phenotypically normal mother is a carrier of the 3p26.3 duplication. This duplication most likely represents a normal population variant. Standard blood chromosome analysis on the subject revealed a normal karyotype.
CH can rarely be caused by a deletion in chromosome 14. This case highlights the importance of utilizing aCGH in the evaluation of patients with hypothyroidism in conjunction with respiratory distress at birth. If aCGH is normal, molecular analysis of the NKX2–1 gene should be considered.
Medical Biochemistry, Acibadem University, Istanbul, Turkey
Iodine Uptake and Metabolism Friday Poster Basic
Perchlorate is an inorganic anion that can disrupt thyroid function by competitively inhibiting iodide uptake at the sodium-iodide symporter (NIS). NIS-mediated iodide uptake can also be inhibited by thiocyanate and nitrate. Prolonged inhibition of iodide uptake can lead to decreased thyroid hormone production and ultimately could result in hypothyroidism.The main objective of this pilot study is to characterize exposure to thiocyanate, nitrate and perchlorate in areas with differing iodine intakes in non-pregnant and non-lactating women.
Health volunteer participants were randomly selected from non-pregnant and non-lactating women 18 years of age or older women. Iodide, thiocyanate, nitrate and perchlorate levels measured in 24 hours collected urine samples from different city in Turkey. NIS inhibitors were analyzed by triple-stage quadrupole ion chromatography-mass spectrometry (IC-MS/MS) using an Applied Biosystems 4000 IC-MS/MS system slightly modified version of the method by Valentin-Blasini et al., 2007 at the Perchlorate Lab of the CDC in Atlanta, USA.
Iodide levels were found to be lower than the required levels suggested by the World Health Organization. All three study populations had median urinary iodide levels lower than 80 μg/L, and thus none of these populations meets the WHO guideline for adequate iodine intake. Iodide levels were lower than urinary iodine levels found in NHANES study. Perchlorate concentrations are higher in the study population compared with NHANES. There are significant differences between Isparta's and Istanbul's perchlorate levels. Nitrate levels in all cities are well exceeding the drinking water standards of World Health Organization. Similarly, thiocyanate levels are not only significantly different from each other but also higher than the suggested drinking water standards published by World Health Organization.
This study provides crucial information about thiocyanate, perchlorate and nitrate exposure in Turkey and gives information about iodide status relationship of non-pregnant and non-lactating adult population with a median urinary thiocyanate, nitrate and perchlorate levels from different locations in Turkey.
Amiodarone-Induced Hyperthyroidism Occurring 1 Year After Amiodarone Discontinuation
Iodine Uptake and Metabolism Friday Poster Clinical
The time course of amiodarone-induced thyrotoxicosis (AIT) typically occurs within months of amiodarone initiation. We describe a case of AIT occurring in a 69 year old male with a 6 year history of atrial fibrillation and coronary artery disease treated on amiodarone for the first 5 years and then discontinued because he was in sinus rhythm. Periodic TFTs during amiodarone treatment were normal. AIT occurred 1 year after discontinuation of amiodarone.
Patient history, exam, lab data were reviewed. The case was discussed with the patient's cardiologist. Review of the literature was conducted via PubMed search.
Current presentation was with acute-onset of palpitations. Physical exam revealed an irregularly irregular heart rate of 84 bpm. Thyroid exam was unremarkable: goiter was absent and he was clinically euthyroid without eye signs. Salient medications included digoxin, dronedarone and diltiazem. Routine thyroid function tests revealed mild biochemical hyperthyroidism with TSH<0.02, FT4 1.6, and FT3 4.7. A thyroid uptake and scan revealed low uniform uptake of 4.9% at 24 hours. A 24 hour urinary iodine was elevated at 1009 mcg/24hr (Normal 75–500mcg/24hr), thyroid-stimulating antibody (TSI) was minimally elevated at 163 (normal<140), and thyroid peroxidase antibody (TPO) was negative. Treatment for hyperthyroidism was initiated with methimazole.
Iodine-induced hyperthyroidism (Jod-Basedow disorder) is an uncommon disorder and typically occurs in association with iodine-containing medications (amiodarone, kelp), high iodine containing foodstuffs (seaweed soup) and CT-contrast usually in the presence of abnormal thyroids such as latent Graves or multi-nodular goiter. AIT tends to be resistant to treatment and very often requires high doses of anti-thyroid agents or thyroidectomy for its control. It typically occurs early on in association with iodine load. Our gentleman is an unusual case because he presented one year after discontinuation of amiodarone in the absence of other recognizable forms of iodine ingestion. It is possible that this gentleman has Type 1 AIT occurring in the presence of mild latent Graves' disease, as he had mildly positive TSI.
Thyroid Hormone Stimulates Mouse Embryonic Stem Cells Differentiation into Cortical Pyramidal Neurons
Thyroid and Development Friday Poster Basic
Thyroid hormone plays an important role in the brain development. Early maternal hypothyroxinemia in rats alters cerebral cortex cytoarchitecture (1). Previously, we demonstrated that triiodothyronine (T3) and retinoic acid (RA) played distinct roles in differentiation of mouse embryonic stem cells (ESC) into neurons. Thyroid hormone induces neural differentiation and reduces RA-induced apoptosis (2). In the present study, we have developed a new T3-directed neural differentiation method that enabled us to study the role of thyroid hormone in the development of cortical pyramidal neurons.
ESC neural differentiation was divided two stages utilizing two different conditioned medium. In the first stage, ESC were differentiated in DMEM/F12/N2/Cyclopamine medium and treated with T3 (1nm) or RA (1μm) for 14 days. In the second stage, differentiation was continued in conditioned medium with supplement of growth factors (B27) for 10 days. We analyzed cell morphology and neural differentiation markers with immunocytochemistry and mRNA expression.
In the first stage of neural differentiation, the number of neural progenitors after T3 treatment was increased compared to the control cells. Neuronal progenitors can further differentiate into different cell lineage: glial cells and neurons. Neuron lineage differentiation occurred two days earlier in the presence of T3 compared to the control. At the end of second stage of neural differentiation, the cortical pyramidal neurons were dominant in T3 treated cells. In RA treated cells, neural lineage appeared early (at day 9) compared to T3 treated cells (at day14). However, continuing RA treatment induced apoptosis, which is consistent with our previous findings (2). T3, but not RA treatment, promotes differentiation of ESC into cortical pyramidal neurons.
The method we utilized to differentiate ESC into pyramidal neurons provided a useful tool to study the role of thyroid hormone in neural development.
Reference
Pediatrics, The Hospital for Sick Children, Toronto, ON, Canada
Thyroid and Development Friday Poster Clinical
Animal evidence indicates hippocampal vulnerability to thyroid hormone (TH) loss reflecting cell reductions and disrupted synaptic functioning in TH-deficient rodents. The hippocampus is not only critical for memory, spatial learning, and novelty detection, it is also highly susceptible to training-induced neuroplasticity. For example, musicians exhibit greater hippocampal activity than non-musicians during novelty detection tasks. However, no study has as yet explored hippocampal neuroplasticity in TH-deficient populations. Children with congenital hypothyroidism (CH) experience TH insufficiency occurred during late gestation and early life and show abnormal hippocampal development. To determine whether they show neuroplasticity in hippocampal development following specialized training, we stratified and compared CH and control groups according to whether children received previous musical training.
Participants were 64 10–15 year old children of whom 28 had musical training (14 CH/14 control) and 36 did not (19 CH/14 control). All underwent a 1-hour MRI session in a 1.5 T scanner; volumetric measurements of their hippocampi were later determined by manual tracing. Past musical training was ascertained by questionnaire or telephone interview.
A significant group by musical training interaction was observed for right hipppocampal volumes (p<.05), after controlling for total intracranial volume, age, and gender. On post-hoc testing, CH without training had significantly smaller right hippocampal volumes than CH with training (p<.01), controls with training (p<.05), and controls without training (p<.05) and hippocampi of CH with training did not differ from controls with training (see Figure 1). Findings were not associated with differences in IQ or family socioeconomic status.
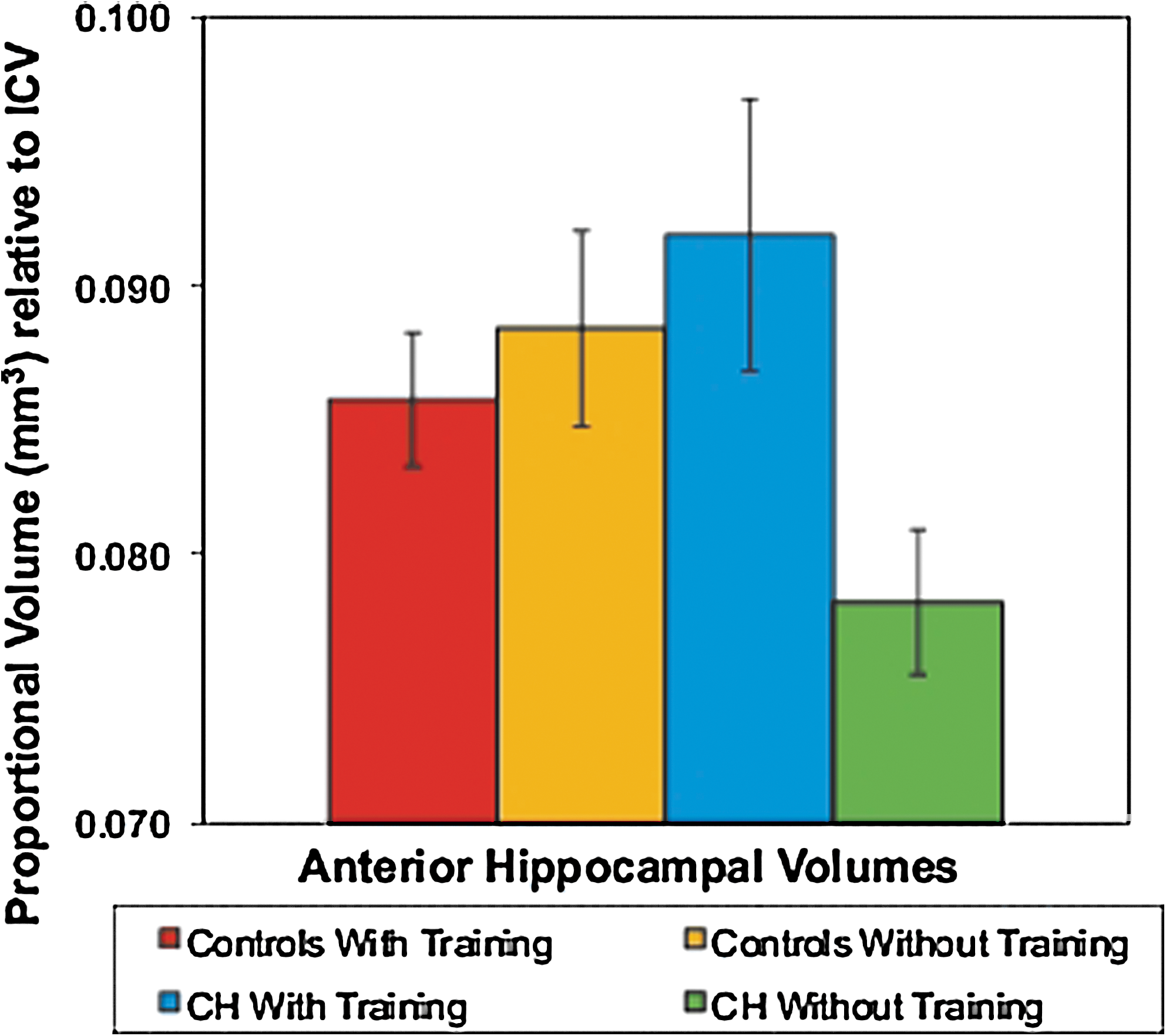
Mean Hippocampal Volumes in CH and Controls With and Without Musical Training.
In CH, musical training may help ameliorate abnormal hippocampal development by later inducing structural neuroplasticity of their hippocampi.
Thyroid Cancer Friday Poster Basic
Introduction: Increasing research has begun to investigate the role of the human pathogenic Parvovirus B19 (B19) in thyroid cancers and other disorders. Wang, et al. 2008 and 2010, found a strong link between PTC and Hashimoto's thyroiditis and B19 detection. Our lab detected B19 in PTC, but also in both “normal” adjacent tissues and ATC, MTC, and FTC tumors. We aimed to expand the number of thyroid tumor cases examined for the presence of B19, and to begin to analyze the relationship of B19 to these disorders, particularly the infectious/replicative properties of B19 in thyroid cancer.
200 thyroid tissue samples consisting of 13 different types of tumors and benign disorders were analyzed for B19 capsid proteins as well as the viral co-receptor α5β1 integrin by IHC and B19 DNA by nested PCR (nPCR). Three samples were analyzed by in situ hybridization to confirm NS1 DNA detection. 5 PTC samples positive for B19 DNA and proteins were analyzed for NS1 by RT-PCR.
We studied the total nPCR and IHC data for 194 cases. Only 6 of the samples showed no B19 staining in 2 interrupted sections. The attached figure shows positive IHC detection of B19 in a PTC tissue (A). 99% of positive tumors showed nuclear staining. Most tumors having cytoplasmic detection showed a shift, with both nuclear and cytoplasmic detection only in the tumor area (B). C summarizes these findings for all 200 tissues based on percentage of tissues expressing B19 in the cytoplasm vs. the nucleus. All samples analyzed by in situ showed positive nuclear NS1 DNA, and the PTC samples analyzed by RT-PCR were also found to be positive. Co-receptor α5β1 was seen primarily in normal adjacent tissue and not in thyroid tumors. We continue to expand sample numbers for RNA and in situ data.
Only 12.5% and 3% of the 194 samples analyzed were negative for viral DNA or proteins,respectively, indicating the thyroid is highly capable of harboring B19. NS1 RNA was detected in all samples analyzed, showing that both the VP and NS1 sequences are expressed in these tissues. Because the co-receptor is primarily detected in the normal adjacent tissue, this suggests B19 infects the thyroid prior to tumor formation.
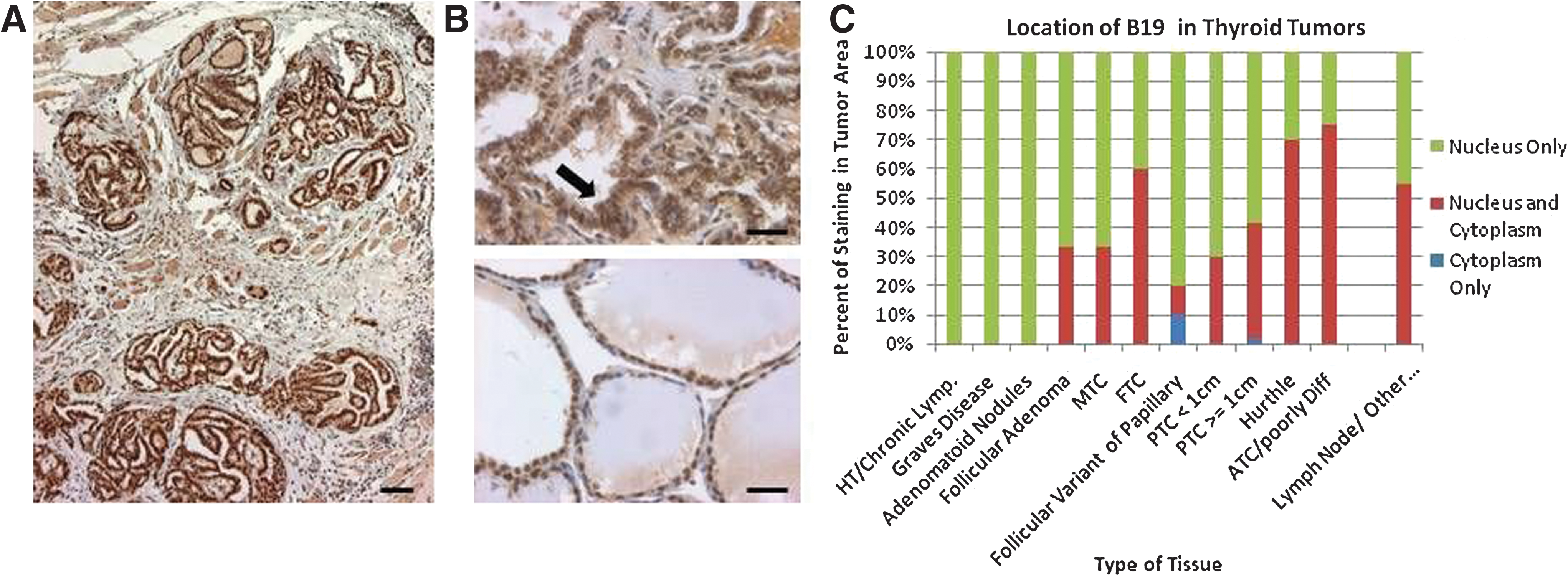
Infection and replication of B19 in thyroid cancers.
Thyroid Cancer Friday Poster Basic
The most difficult thyroid tumors to be diagnosed by cytology are conventional follicular carcinomas (FC) and oncocytic follicular carcinomas (OFC). Several miRNAs were previously reported as reliable markers in papillary thyroid carcinoma, however, limited information is available for FC and OFC. The aim of this study was to find candidate miRNA markers that can be used in diagnostically challenging thyroid specimens.
Thirty two follicular thyroid carcinomas (15 FC, 17 OFC), 6 normal thyroid tissues and two hyperplastic nodules were studied for expression of 380 miRNAs using Human Microarray Assays (Applied Biosystems) on ABI 7900. miRNAs were isolated using Trizol reagents from frozen thyroid tissue and using RecoverAll Total Nucleic Acid kit (Ambion) from FFPE tissue specimens. The data analysis was performed with Data Assist v2.0 (Applied Biosystems) program.
Overall, miRNA expression was different between oncocytic follicular carcinomas and conventional follicular carcinomas demonstrating individual clusters on the unsupervised hierarchical clustering analysis. Strong upregulation (more than 10 fold) of miR-221, miR-222 and miR-885-5p was detected in oncocytic follicular carcinomas, but not found in conventional FCs. Similarly, miR-34-5c was downregulated only in OFCs. Some miRNAs were dysregulated in both types of follicular carcinomas including upregulation of miR-182, miR-183, -and miR-618 and downregulation in miR-199a-3p and -5p and miR-455-3p and -5p.
Oncocytic follicular carcinomas demonstrated distinct miRNA expression profile suggesting an independent origin of these tumors. Several miRNAs were found to be dysregulated in conventional follicular carcinomas and oncocytic follicular carcinomas and may be of diagnostic use in thyroid fine needle aspiration specimens.
Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Republic of Korea
Thyroid Cancer Friday Poster Basic
Systemic chemotherapies for advanced or metastatic thyroid carcinomas have been of only limited effectiveness. For patients with differentiated or anaplastic carcinomas unresponsive to conventional treatments, novel therapies are needed to improve disease outcomes. As the understanding of the molecular biology of thyroid cancer is better understood, new means of targeting these pathways for intervention in thyroid cancer cells is occurring. Honokiol has anti-tumor effect against several human cancer cell lines.However, its antitumor effect in thyroid cancer has not been demonstrated.Clinical trial using kinase inhibitors have demonstrated transient partial responses and prolonged disease control in patients with progressive thyroid cancer. The goal of the present study was to identify the potential value of honokiol as a candicate for the treatment of thyroid cancer and to investigate of anti-tumor effect of honokiol in combination with molecular targeted agents in thyroid cancer cell lines.
Three human thyroid cancer cell lines, TPC-1, FTC133, and FRO, respectively, were exposed to honokiol alone and in combination with sorafenib, sunitinib, RAD001, and AZD6244. Cell proliferation was assessed by MTT assay. Apoptosis was measured by TUNEL assay and FACscan analysis. Western blot analysis was performed to identify that honokiolalone and combination therapy may inhibit the MAPK pathway and PI3K/AKT/mTOR pathway.
Honokiol exhibited significantly anti-proliferative activity in all three thyroid cancer cell lines in vitro. TUNEL assay and FACscan analysis revealed the significant induction of apoptosis after using honokiol in vitro. Western blot analysis showed preferential inhibition of phosphorylation of ERK, AKT or S6K, depending on cell lines. Combination of honokiolwithother molecular targeted agents presented synergistic effects on induction of apoptosis of thyroid cancer cells.
Honokiol, either alone or in combination with other therapeutics, could serve as a new, promising approach for thyroid cancer treatment.
Surgical Oncology, UT MD Anderson Cancer Center, Houston, TX
Thyroid Cancer Friday Poster Basic
Distant metastatic disease occurs in ∼15% of patients with thyroid carcinomas. Although brain metastases are rare, they signify aggressive disease and short survival. The rarity of tissue from distant metastatic sites has limited their evaluation for molecular alterations which may contribute to tumorigenesis and point to therapeutic targets.
Twelve patients with formalin-fixed paraffin embedded tissue available from biopsy or resections of metastatic thyroid carcinomas to the brain from 1995 to 2010 were included in this study. Tumors analyzed included 8 papillary thyroid carcinomas (PTC), 1 follicular carcinoma (FC), 1 Hurthle cell carcinoma (HCC), and 2 medullary thyroid carcinomas (MTC). Extracted DNA was analyzed for 145 mutations/alterations in 30 genes by mass spectrometry based DNA analysis (Sequenom Inc, San Diego, CA).
Brain metastases occurred in 6 men and 6 women, 3 of whom were <45 yrs of age at primary diagnosis. Time to onset of brain metastases from initial diagnosis differed based on age at primary diagnosis <45 or ≥45 yrs, median 15 vs 2.9 yrs (range 1.6 to 24 yrs versus present at initial presentation to 8.8 yrs respectively). At last follow-up 4 patients were alive (12–101 months after brain metastasis diagnosis); 8 were dead (3.7–209 months). Median survival was similar (28.3 vs 30 months) for both age cohorts. 8 of the 12 tumors (75%) showed gene mutations in 5 of the genes tested (Table 1). Six tumors showed one gene mutation. Two PTCs had 2 and 3 different gene mutations respectively (NRAS+PIK3CA and MET+NRAS+PIK3CA). Both MTCs showed sporadic 918 RET mutations. Four tumors were negative for all molecular alterations tested for in this analysis.
Molecular Analysis of Thyroid Carcinomas Metastatic to the Brain.
DX, diagnosis; FC, follicular carcinoma; HCC, Hurthle cell carcinoma; MTC, medullary thyroid carcinoma; PTC, papillary thyroid carcinoma. Mutations are reported as the wild type amino acid abbreviation [left], the amino acid location effected, followed by the altered amino acid resulting from the nucleic acid alteration [right] with the number of tumors showing that mutation in parentheses.
Brain metastases may occur secondary to thyroid carcinomas regardless of age at diagnosis however a more rapid occurrence was noted in patients >45 years of age at diagnosis. Survival remained poor regardless of age. Thyroid cancers with brain metastases are molecularly heterogeneous favoring personalized molecular analysis for targeted therapy. Mutations may be activating allowing targeted inhibitor therapy however, certain loci may signify resistance. Further molecular analyses in larger cohorts and in other metastatic sites are warranted.
Thyroid Cancer Friday Poster Basic
The GWAS studies performed in papillary thyroid cancer shows FOXE1 may be the potential risk gene for papillary thyroid cancer(PTC), which is a transcription factor of thyroid development regulated by TSH. Recently, the endogenous TSH level is described as a predictor of a subsequent thyroid cancer diagnosis. The mechanism of the elevated serum TSH level remains unknown.
A genotyping study for FOXE1 was perfomed in a Chinese series of 647 PTC, 527 benign thyroid disease, and 677 community-based normal controls. The FOXE1 genetic region and its flanking sequences (approximately from 1,100 bp upstream to 500 bp downstream of this gene) were directly sequenced to identify polymorphic sites in 48 samples including 24 unrelated sporadic PTC and 24 controls. ALL of the identified common SNPs (minor allele frequency (MAF>10%) were further genotyped. Genotyping work was performed using the Taqman 5′-nuclease assays for 10 SNPs in FOXE1 gene region. All the PTC and benign thyroid disease cases had a serum TSH measurement by a chemiluminescent microparticle immunoassays with interassay coefficients of variation of less than 10% over the ranges 0.35–4.94 uIU/mliter.
In PTC versus normal, the strongest association results were observed for rs3758248 C>T (OR=2.01; 95%CI=1.20–3.55; P=1.035×10−8), rs907577 A>G (OR=1.98; 95%CI=1.57–2.50; P=1.7388×10−11) and rs1867277 G>A (OR=3.52; 95%CI=2.91–4.24; P=1.9628×10−31); in benign disease versus normal, the strongest association results were observed for rs3758248 C>T (OR=2.19; 95%CI=1.08–4.45; P=6.8563×10−19), rs907577 A>G (OR=1.59; 95%CI=1.20–2.11; P=6.8563×10−19) and rs1867277 G>A (OR=1.72; 95%CI=1.39–2.12; P=6.8563×10−19); in PTC versus benign, the strongest association results were observed for rs3758248 C>T (OR=1.48; 95%CI=1.20–1.82; P=1.0×10−4) and rs1867277 G>A (OR=1.81; 95%CI=1.51–2.17; P=5.2789×10−11). Combing with serum TSH in PTC and benign group, the risk of PTC went higher in patients with allele C of rs3758248 and G of rs1867277 when the serum TSH elevated (Table 1).
The Relationship Between TSH Level and PTC Risk of Patients with rs3758248 C>T and rs1867277 G>A
CA: allele C of rs3758248 and allele A of rs 1867277; CG: allele C of rs3758248 and allele G of rs 1867277; TA: allele T of rs3758248 and allele A of rs 1867277; TG: allele T of rs3758248 and allele G of rs 1867277; Statistical analysis was used Nonzero Correlation(SAS 8.2).
FOXE1 may be a genetic risk gene for PTC in Chinese patients. The special genotype of FOEX1 may be more susceptible by the affect of TSH.
Thyroid Cancer Friday Poster Basic
Many transcription factors are involved in the regulation of NIS expression. Particular attention has been focused on the activation of the NIS Upstream Enhancer (NUE) region, containing an essential PAX8 site and a cAMP response element (CRE)-like site, which bind elements of the CRE binding (CREB) protein family. Among them, a role has been demonstrated for CRE modulator (CREM) protein in normal thyrocytes stimulated by TSH or forskolin. In this work, we examined the expression of CREM in a series of thyroid cancer tissues and its action on NIS promoter in human thyroid cancer cells.
The expression of CREM, PAX8 and NIS mRNA levels were measured by quantitative RT-PCR in 38 thyroid cancer tissues, including 22 papillary thyroid cancer (PTC), 12 follicular (FTC) and 4 anaplastic thyroid cancer (ATC). For NIS promoter studies, the NIS Basal Promoter (BP)+NUE-Luc or 810-BP-Luc promoter and pRc/CMV-CREM-Q2-T2alpha constructs were co-transfected in BCPAP and FRO cells, derived from human papillary and undifferentiated thyroid carcinoma, respectively, or FRTL-5 cells, as control. LUC activity was measured by chemiluminescence.
Reduced NIS transcript levels were found in all the samples, paralleled by similar decrease of PAX8 gene levels. In contrast, CREM mRNA levels increased approximately 5-fold in comparison with normal tissues (p<0.01). Transfection experiments showed an inhibitory effect in both thyroid cancer cell lines examined, at variance with the stimulation obtained in the normal FRTL-5 thyroid cells, also when forskolin was added. The effect was similar using the NIS BP+NUE-Luc or 810-BP-Luc promoter in both cell lines. The inhibition disappeared when testing a construct lacking the CRE binding site.
These data demonstrate that CREM expression is increased in thyroid cancer tissue and may play a role in the downregulation of NIS expression in thyroid cancer, acting at the transcriptional level.
Rhabdomyolysis: An Under-Recognized Complication of Continuing Statin Therapy During Thyroid Hormone Withdrawal for Iodine-131 Ablation in Thyroid Cancer
Thyroid Cancer Friday Poster Clinical
To describe two cases of rhabdomyolysis during withdrawal of levothyroxine for I-131 whole body scan (WBS) while on statin therapy.
A 55-year-old white female was found to have bilateral papillary thyroid tumors. She underwent total thyroidectomy with central node and left modified lateral neck dissection. She was staged at T1N0M0 and treated with 100 mCi of I-131. In the year after treatment she was placed on statin therapy. She presented one year later for endogenous TSH-stimulated Tg and I-131 WBS. During thyroid hormone withdrawal (THW), the patient presented to the emergency room with bilateral leg cramping. Her creatinine kinase (CK) level was 1170. She was taken off of her statin, treated with IV fluids and pain medication, and restarted on levothyroxine. Subsequent CK and TSH three months later had normalized to 108 ng/ml and 0.34 uIU/ml, respectively.
A 40-year-old white male with left 1.6 cm×1.4 cm suspicious thyroid nodule underwent total thyroidectomy and central neck dissection. Pathology confirmed papillary thyroid cancer, follicular variant Stage 1 T1N0MX. On postoperative follow-up, he was instructed to stop his levothyroxine in preparation for endogenous TSH-stimulated I-131 ablation but continued on simvastatin. He presented one month later with sudden left-sided cramping. Laboratory data showed a TSH of 74.74 uIU/ml and a corresponding CK of 3033. He was hospitalized, treated with pain medication and IV fluids, and taken off his statin therapy.
Rhabdomyolysis is a well-described complication of hypothyroidism. Elevated CK has also been well-described with statin therapy. Surprisingly, rhabdomyolysis has never been described as a complication of thyroid hormone withdrawal in preparation for I-131 ablation in thyroid cancer among patients who also take statins. We present two cases of rhabdomyolysis prompting emergency room visits and hospital stays that may have been avoided if statin therapy was discontinued at the same time as cessation of levothyroxine therapy. Currently, there are no formal recommendations on stopping statin therapy in patients undergoing thyroid hormone withdrawal in preparation for I-131 ablation therapy.
Sorafenib at a Low Dose Against Radioiodine-Refractory Metastatic Papillary Thyroid Carcinoma in Lung
Thyroid Cancer Friday Poster Clinical
Sorafenib at a dose of 400 mg twice daily has shown promise in the treatment of patients with advanced or metastatic thyroid carcinoma. However, severe adverse events have been found and the optimal dose has not been established, and data in Chinese population are not available. We conducted a study to assess the responses to sorafenib at a low dose of 200 mg twice daily in patients with progressive radioiodine-refractory pulmonary metastases from papillary thyroid carcinoma (PTC).
Eligible patients received sorafenib 200 mg orally twice daily. Responses were assessed using Response Evaluation Criteria in Solid Tumors and adverse events were assessed periodically. The end points included response rate and progression-free survival (PFS).
Nine patients with radioiodine-refractory PTC were enrolled in the study and treated for a minimum of 13 weeks. The objective partial response rate was 33%. The stable disease rate was 44%. The mean PFS was 42 weeks (95% CI, 29.5 to 53.9). Two patients showed disease progression, and one of them died 4 months after beginning of treatment. There was a marked and rapid change in the serum thyroglobulin level after start of treatment with a mean decrease of 60% within 12 weeks, consistent with radiographic findings. Although the types of toxicities were consistent with other sorafenib trials, their severity was relatively mild. None of the patients discontinued sorafenib or reduced their dose because of treatment-related adverse events.
Sorafenib at a dose of 200 mg twice daily has a potential therapeutic effect in Chinese patients with radioiodine-refractory pulmonary metastases from PTC. Its overall clinical benefit rate is 77% with a mean PFS of 42 weeks and an acceptable safety. Prospective controlled randomized studies with more patients and longer observation times are greatly needed.
Pathology, University of Texas Medical School at Houston, Houston, TX
Thyroid Cancer Friday Poster Clinical
Black Americans with differentiated thyroid cancer (DTC) often present with larger tumors and at advanced age. This difference has been attributed to unequal access to health insurance. The aim of this study was to compare the DTC histology and age at presentation between different racial groups in two metropolitan hospitals; one serves a medically-indigent population and the other a largely insured population.
Retrospective case-control study of patients with DTC who underwent thyroidectomy at a tax-supported versus a private hospital between 1999 and 2009. The effect of insurance status and race on age at presentation, advanced disease, and tumor size was analyzed. Advanced disease was defined as a tumor with extra-thyroidal extension, local, or distant metastasis.
Two-hundred and sixty three patients with DTC who underwent thyroidectomy at a tax-supported hospital (N=185) and a private hospital (N=78) met inclusion criteria. Neither insurance status nor race affected the age at presentation (p=0.38 and p=0.31, respectively). The mean tumor size was larger in the uninsured population versus the insured (2.7 cm vs. 2.1 cm, p=0.04). When compared to Caucasians, Blacks and Hispanics presented with a trend towards larger tumors (OR 1.20, p=0.08 and OR 1.25, p=0.018, respectively). However, this relationship may be accounted for by the observation that Blacks and Hispanics were less likely to be insured when compared to Caucasians (OR 0.27, p=0.004 and OR 0.03, p<0.001 respectively). Patients with larger tumors were more likely to present with advanced disease (OR 2.70, p<0.001), which was independent of race and insurance status.
In this study the uninsured patients were more likely have larger tumors; this population was mainly represented by Black and Hispanic patients. We found no difference in age at presentation, advanced disease, or tumor size based on race.
Radiology, Division of Nuclear Medicine, Memorial Sloan-Kettering Cancer Center, NewYork, NY
Thyroid Cancer Friday Poster Clinical
The aim of this study is to determine if lesional dosimetry determined by 124I PET imaging would correlate with response to RAI therapy in differentiated thyroid cancer patients with metastatic disease.
Sixteen patients (7F, 9 M, 55±16 years) with metastatic thyroid cancer were studied by FDG PET/CT (Mean activity: 15±1 mCi), three time point (24, 48, 72 hours) I124 PET/CT (Mean activity: 6.4±03.7 mCi) and diagnostic CT scan (n=12/16) prior to administration of I131 therapy (guided by whole body and blood RAI clearance studies). Size, FDG avidity and I124 maximal standard uptake value (SUV Max) was determined for each metastatic focus. Objective response was assessed by RECIST 1.1 criteria for CT scan (n=13) and/or by EORTC criteria for FDG/I124 PET (n=9) 1 year after I131 therapy. The median lesion estimated absorbed dose (Gy) was calculated in responder and non responder lesions.
A total of 271 lesions were evaluated (147 pulmonary metastases, 60 bone metastases, 39 loco-regional lymph node metastases, and 25 other metastatic sites). The majority of the lesions were detected only by FDG PET (n=164, 60%), while 55 lesions (21%) were detected only by I124 PET, and 52 (19%) were visualized on both FDG and I124 PET. Mean lesion size was 13.1±10.9 mm. The median I131 activity administrated was 304 mCi (range 122–398). Objective response was detected in 54/227 (24%) evaluable lesions 1 year after I131 therapy. Lesions that demonstrated an objective response to RAI therapy were smaller (9.9±5.2 mm vs 13.9±11.8 mm, P=0.03), more likely to be in the lungs (P=0.003), and had significantly higher I124 SUV max (12.3 vs 1.5, P=0.008) and demonstrated to a first approximation a significantly higher median estimated absorbed dose (2.4 Gy vs 0.37 Gy without partial volume correction; 8.6 Gy vs 0.9 Gy with partial volume correction).
Pre-treatment evaluation by FDG and I124 PET can identify patients with metastatic disease most likely to benefit from additional RAI therapy.
Calcium Checks Post Thyroid Surgery—Are New National Guidelines Being Followed?
Thyroid Cancer Friday Poster Clinical
The second edition of the British Thyroid Association (BTA) guidelines was published in 2007. Regarding calcium monitoring post total thyroid surgery it was modified from the original 2002 version that had advocated same day calcium checks. It stated ‘Serum calcium should be checked on the day after surgery and daily until hypocalcaemia improves.’ These guidelines were implemented due to studies by Szubin et al. (1996) which found that the critical period for monitoring calcium was 24 to 96 hours after surgery, and Bentrem et al. (2001) who stated that the 16 hour calcium level revealed 94.5% of patients requiring calcium supplementation. This audit aims to assess whether the updated version has achieved a standard practise of calcium checks amongst surgeons.
A retrospective 6 year review of all patients having total thyroid surgery in a tertiary referral centre. Data was collected regarding demographics, the type of operation, histopathology, calcium levels and administration of calcium supplements for a 3 year period before (2004–2006) and after (2008–2010) the introduction of new guidelines.
68%(23) of the 34 patients having total thyroid surgery prior to modification of guidelines had calcium checked on the evening of surgery, with no patients requiring calcium supplementation. 82%(49) of the 60 patients having surgery after the introduction of guidelines had evening calcium checks and 4%(2) of these were given prophylactic calcium replacement due to biochemical hypocalcaemia in the absence of symptoms. There were no records of any adverse events as a result of not doing an evening calcium check (23%).
The modification of BTA guidelines regarding the timing of calcium checks post-thyroid surgery has not changed practice, with clinicians still electing to perform a routine evening check. These guidelines are due for review in 2012 and should be updated to include a more detailed regimen of calcium checking post thyroid surgery based on the latest literature, thus encouraging standardisation of practice.
Impact of Distant Metastases at Presentation on Outcome in Patients with Well Differentiated Thyroid Cancer Managed with Thyroidectomy
Thyroid Cancer Friday Poster Clinical
Distant metastases at presentation are rare in well differentiated thyroid cancer (WDTC). The objective of this study is to report outcomes for patients presenting with distant metastases managed by thyroidectomy and radioactive iodine therapy.
52 patients with distant metastases from thyroid cancer diagnosed prior to thyroid surgery (n=32) or on postop RAI scan following thyroid surgery (n=20) were identified from a pre-existing database of 1810 patients with WDTC treated between 1985 to 2005. The median age was 58 years (range 12–83 years), with a male to female ratio of 3:2. 47 patients (90%) had total thyroidectomy, 3 (6%) thyroid lobectomy and 1subtotal thyroidectomy (2%). Distant metastases were classified into pulmonary and extrapulmonary. Overall survival (OS), disease specific survival (DSS) and locoregional recurrence free survival (LRRFS) were calculated by the Kaplan Meier method. Factors predictive of outcome were determined by univariate analyses.
39 patients (75%) were diagnosed with pulmonary metastases alone and 13 (25%) with extrapulmonary metastases. The sites of extrapulmonary metastases were bone in 9, mediastinum in 1, pyriform sinus in 1, skin in 1 and 1 patient had synchronous lung, bone and intracerebral metastases. Following thyroid surgery 47 patients (90%) were treated with RAI alone and 2 patients had external beam radiation in addition to RAI. With a median follow up following surgery of 78.5 months (range 1–281 months), the 5-year OS and DSS were 65% and 68% respectively. 29 patients (56%) died during follow up of whom 24 (46%) died of thyroid cancer. 6 patients (12%) developed recurrent disease in the neck and 3 patients (6%) developed recurrence in the thyroid bed. Age over 45yrs, follicular pathology and extrapulmonary metastases were predictive of lower 5yr DSS (100% vs 56%, p<0.001; 70% vs 50%, p=0.004 and 75% vs 46%, p=0.013 respectively).
One third of patients with WDTC presenting with distant metastases died of disease within 5 years of initial diagnosis despite thyroid surgery and RAI. Age over 45y, extrapulmonary metastases and follicular pathology were significant predictors of poor outcome.
Withdrawn
Oral Surgery, Columbia University, New York, NY
Thyroid Cancer Friday Poster Clinical
131-I is actively secreted by the salivary glands,causing obstructive symptomatology and hyposalivation. Low dose 131I rarely causes dry mouth but commonly causes post-meal obstructive swelling. Dry mouth in a patient treated with 131-I was due to existing secondary Sjogren's syndrome (SS) exacerbated by RAI. Scintographic, serologic, microscopic findings confirmed secondary SS.
Salivary glands concentrate and secrete Technetium-99m pertechnetate (TPT). TPT time/activity scintiscan examines activity of 4 major salivary glands in real-time, distinguishing salivary symptomatology post-131-I from SS. Ductal wall inflammation and blockage following low dose 131-I; scintiscan shows adequate pickup of TPT, but failure to secrete. In contrast, SS causes lymphocytic replacement of entire parenchyma, interfering with acinar cell pickup; scan shows minimal parotid activity.
A thyroid cancer patient treated with 131-I showed no parotid activity, pickup or secretion of TPT, but normal submandibular TPT concentration and secretion. Total parotid parenchymal destruction with hyposalivation is more consistent with SS, rather than 131-I effects. Labial microscopy showed focus score=1 (Chisholm grade 3) lymphocytic clumped foci, consistent with SS. 131-I sialadenitis causes diffuse lymphocytic distribution. Schirmer test: normal bilateral tear production.
Differentiation of dry mouth of autoimmune from radiation sialadenitis is shown by TPT scan. Usually >150 mCi is required for hyposalivation, and drying effect is not total. Total parotid parenchymal destruction with hyposalivation is more consistent with SS diagnosis.
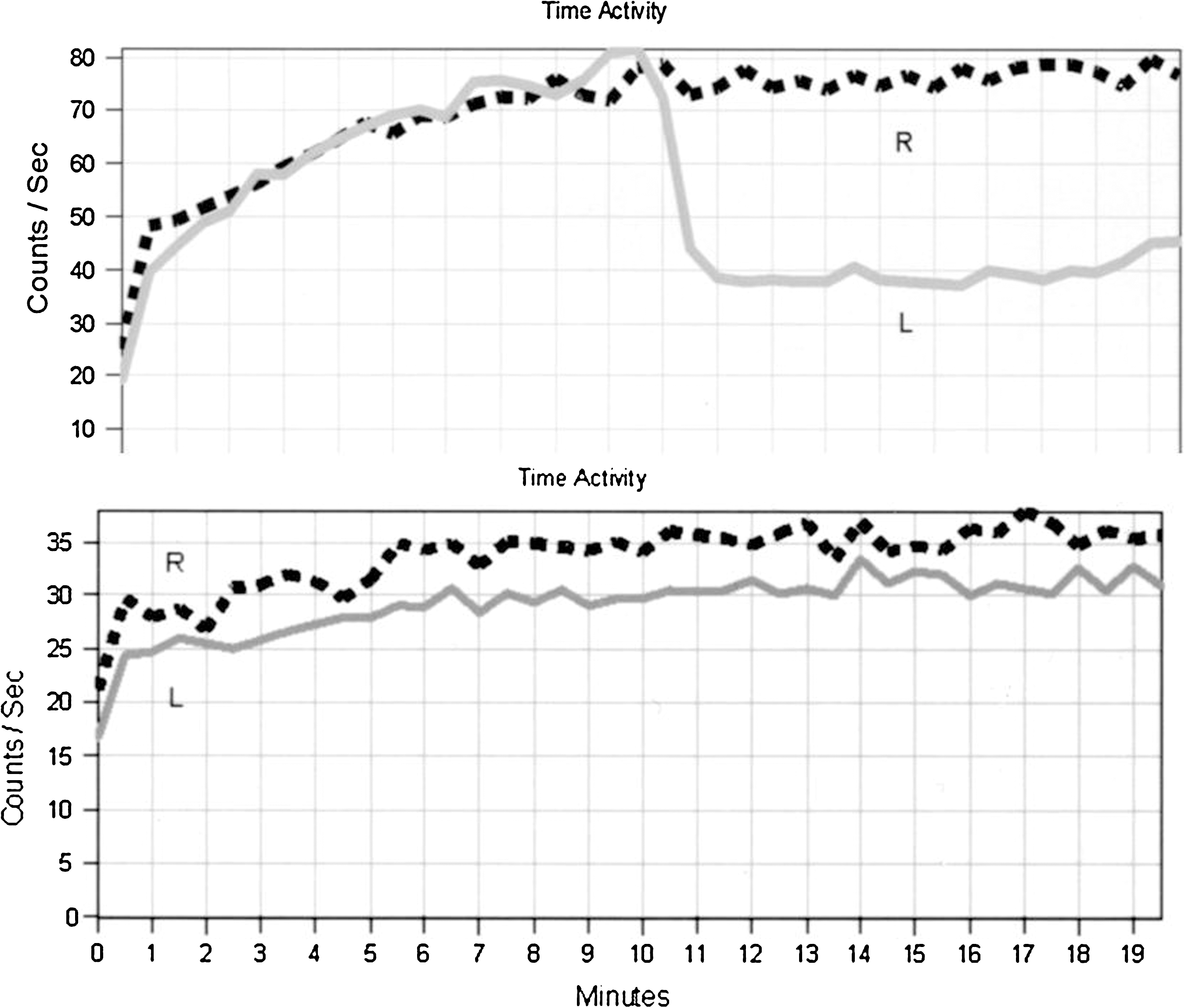
Differentiating 131I sialadenitis from SS sialadenitis.
Thyroid Cancer Friday Poster Clinical
TSHR mRNA is a marker for circulating thyroid cancer cells in peripheral blood. It is often elevated preoperatively in patients with thyroid cancer and is normalized post thyroidectomy in localized disease (JCEM 2007;92:468–75). The effect of hypothyroidism and of increased TSH on TSHR mRNA levels remains to be studied.
TSHR mRNA, TSH and thyroglobulin (Tg) levels were measured twice first one on T4 replacement post thyroidectomy and second one at 4–6 weeks after T4 withdrawal in ten patients diagnosed with thyroid cancer. All patients also had whole body scan (WBS) at the time when the second sample was drawn. TSHR mRNA and Tg levels were compared to WBS results to assess the need for radioactive iodine therapy.
Among ten patients, 8 had pathologic diagnosis of PTC (2 metastatic PTC) and 2 had Hurthle cell cancer. Six of these had preoperative TSHR mRNA levels and 4 (67%) were positive. Post operatively the mean TSH levels (M±S.E.) on T4 suppression and withdrawal were 1.7±7.4 and 43±13.6 μ/mL (P=0.0004) and mean Tg levels were 19.2±9.3 and 45±38 ng/mL (P=0.52). TSHR mRNA was<1.0 ng/μg/mL in all except one (with distant metastasis) on T4 suppression when TSH levels were low. Three patients showed an increase in TSHR mRNA levels post T4 withdrawal when TSH levels were significantly elevated. WBS showed residual iodine avid tissue in thyroid bed in seven, in neck in two (one with regional metastases and other with mediastinal mass on follow-up CT scan) and distant metastasis in one. TSHR mRNA measurement on T4 withdrawal when TSH levels are high detected all three patients with metastatic disease (sensitivity 100%) and correlated well with WBS and/or CT scan.
Our findings suggest that TSHR mRNA levels are increased with increased TSH and are concordant with WBS/CT in detection of metastatic disease. Testing during hypothyroidism (post T4 withdrawal) may enhance diagnostic sensitivity of this test to detect regional metastases. Further studies with larger number of patients are needed to confirm these findings.
Postsurgery Stimulated-Thyroglobuin Measurement Immediately Before Radioactive Iodine Therapy Can Predict Disease Status in Low and Intermediate Risk Patients with Differentiated Thyroid Cancer
Thyroid Cancer Friday Poster Clinical
Postablation stimulated-thyroglobuin (pasTg) measurement, diagnostic whole body scan (DxWBS), and ultrasonography (US) have been used to detect the recurrence/persistence of thyroid cancer for low and intermediate-risk patients. But, there are still no studies to demonstrate the usefulness of postsurgery stimulated-Tg (pssTg) measured immediately before radioactive iodine therapy (RAIT) to predict the recurrence/persistence of thyroid cancer. This study was performed to evaluate the usefulness of pssTg for prediction of disease state after RAIT.
Total 209 patients diagnosed with differentiated thyroid cancer who underwent total thyroidectomy were enrolled prospectively. All patients have been performed the RAIT using the dosage of 100–150 mCi and obtained the blood to measure the pssTg immediately before RAIT. To assess the disease status after RAIT, the pasTg, DxWBS, and US were performed at 12 months after RAIT.
The cut-off level of pssTg for prediction of disease free status was 2.0 ng/ml (sensitivity 84.8%, specificity 79.8%). Among the total 209 patients performed RAIT, 137 patients (65.5%) showed the values less than 2.0 ng/ml of pssTg. When the value of pssTg was less than 2.0 ng/ml, the risk of disease presence was very low, even in patients classified into an intermediate-risk. The negative predictive value (NPV) was 94.9%. When the results of pssTg combined with US, the NPV was increased up to 97.7%.
The pssTg measured immediately before RAIT is very useful to predict the disease status after RAIT in both low and intermediate risk patients.
Internal Medicine, Chang Gung Memorial Hospitals, Chang Gung University, Taoyuan Hsien, Taiwan
Thyroid Cancer Friday Poster Clinical
Most papillary thyroid carcinomas (PTCs) have benign clinical course. However patients with advanced (tumor-node-metastasis [TNM] stage IV) PTCs usually have a poor prognosis even after undergoing aggressive treatment. The aim of this study was to retrospectively review and analyzed the therapeutic outcomes and prognostic factors for patients with advanced PTC at our institute.
A total of 251 advanced PTC patients were categorized into either locally advanced (TNM stage IV-A and -B: 208 patients) or distant metastases (TNM stage IV-C: 43 patients) groups.
Among the 251 patients, with a mean age of 58.8±9.6 years, 86.1% presented with extra-thyroid invasion at the time of thyroid surgery. Age, gender, and tumor size were significantly different between the locally advanced and distant metastases groups. After 6.2±0.3 years of follow-up, 49 (19.5%) patients had died of thyroid cancer. In the locally advanced group, 23 patients (11.1%) died of thyroid cancer, and only 36 patients (17.3%) were disease free status at the time of follow-up. In addition, postoperative thyroglobulin (Tg) and radioactive iodide (131I) diagnostic scanning studies reliably predicted disease recurrence. In the distant metastases group, 26 patients (60.5%) died of thyroid cancer during a mean follow-up period of 3.5±0.1 years. The thyroid cancer-specific survival rates at 5, 10 and 20 years were 92.8%, 88.1%, and 66.0%, respectively, in the locally advanced group and 45.8%, 24.5%, and 16.4%, respectively, in the distant metastases group. Analysis of clinical prognostic factors in advanced PTC revealed age, gender, tumor size, and distant metastases as being statistically significant factors. Postoperative Tg levels and the results of post-operative diagnostic scanning showed significant factors in recurrence in locally advanced group.
Advanced PTC patients with distant metastases at the time of diagnosis have a poor prognosis. Aggressive surgical with post-operative 131I therapy may treat patient to disease-free even the patient presented with bone metastases. Post-operative serum Tg levels and remnant tissue detected by 131I are valuable diagnostic tests for predicting disease recurrence for local advanced group.

Therapeutic outcome of patients with advanced PTC in TNM stage IV.
Thyroid Cancer Friday Poster Clinical
Overexpression of fatty acid synthase (FASN) and activated c-Met in human cancers may have therapeutic implications and they have not been fully investigated in thyroid carcinomas.
We evaluated FASN expression by immunohistochemistry in 32 patients with thyroid carcinomas of follicular origin including 22 papillary thyroid carcinomas (PTC: 6 classical type and 6 follicular, 4 tall cell, 2 columnar cell, 1 diffuse sclerosing, 1 trabecular/insular, 1 solid and 1 cribriform variants), 8 follicular thyroid carcinomas (FTC, 3 conventional type and 5 Hürthle cell type) and 2 anaplastic thyroid carcinomas (ATC, 1 with contiguous PTC and 1 with FTC component). Monoclonal rabbit antibody against phosphorylated(p)-c-Met (Tyr1234/1235) antigen was utilized in 6 of the 32 cases. The adjacent non-neoplastic thyroid tissue was also evaluated for comparison. Immunoreactive intensity and extensiveness were semi-quantified.
FASN was overexpressed in a subset of PTCs including the classical type and tall cell, follicular, trabecular/insular, and diffuse sclerosing variants, a subset of FTCs including all Hürthle cell type FTCs and the concomitant PTC and FTC components in the 2 ATCs. No FASN expression was present in the ATCs per se and the columnar cell, solid, and cribriform variants of PTCs. Complete concordance of immunostaining results of FASN and p-c-Met was observed in all the 6 cases. No FASN overexpression was identified in the non-neoplastic thyroid tissue except the follicular cells with Hürthle cell change, as was p-c-Met expression.
This study demonstrates overexpression of FASN and associated activated c-Met in a subset of thyroid carcinomas of follicular origin, which may be of value for targeted therapy. The mechanism of positive staining for FASN and p-c-Met in Hürthle cells remains to be elucidated.
CRUK & UCL Cancer Trials Centre, University College London, London, United Kingdom
Thyroid Cancer Friday Poster Clinical
Most patients with low risk differentiated thyroid cancer (DTC) have excellent survival and low risk of recurrence. Some clinicians believe RAI ablation after total thyroidectomy does not improve survival or even recurrence rates. Patients may therefore undergo hospital isolation and the risk of short- and long-term side effects (eg second malignancies, dry mouth) unnecessarily. In the absence of randomised studies, the American Thyroid Association are unable to make firm recommendations either for or against RAI ablation in low-risk patients. The IoN trial, to be launched in 2011, will be the first ever randomised study to address this issue.
Eligibility: R0 total thyroidectomy (previous 6 months), and the following features. Papillary thyroid cancer with non-aggressive histological features: pT1b (1–2cm); pT2 (2–4cm); pT3 (intrathyroidal only); multifocal microcarcinoma; pN0; pN1a; pNX. Follicular/Hürthle cell thyroid cancer (minimally invasive with capsular invasion only); primary size 1–4cm intrathyroidal. After surgery all patients have a stimulated thyroglobulin and Technetium 99m scan (for remnant size). Patients will be randomised to receive RAI ablation (1.1GBq) or not. 6–9 months later, all will have an I131 scan, neck ultrasound and stimulated thyroglobulin (Tg). For the following 5 years: Tg every 6 months, and neck ultrasound (with guided cytology as required) every 6 months in year 1 then annually, to detect locoregional and distant recurrence. The main objective is to determine whether 5-year disease-free survival is no worse in the no-RAI ablation group, compared to the RAI ablation group.
None available yet.
570 patients are planned across the UK National Cancer Research Network. It is the natural successor to HiLo, which showed that 1.1GBq is as effective as 3.7GBq. Trans-ION will involve BRAF assay, second generation Tg assay and serum proteomics. Full details about the trial will be available. We invite international co-operation and collaboration.
Cardiothoracic surgery, University of Montreal Hospital Center, Montreal, QC, Canada
Thyroid Cancer Friday Poster Clinical
Thyroid cancer is a malignancy with an excellent prognosis for the majority of cases. Tumor intracardiac extension of thyroid cancer is a rare occurrence with only 15 cases reported in the literature so far.
We report the case of a 58 years-old woman, who had a total thyroidectomy and multiple I-131 treatments. During the course of the disease she developed mediastinal lymph node metastasis and slowly progressive pulmonary metastasis. Thrombus of suspected tumoral origin was noted in the superior vena cava on a CT-scan performed because of increased mediastinal uptake following the last iodine-131 treatement.
Because of rapid progression of the thrombus over a 3 month period despite anticoagulation with low molecular weight heparin and the perceived risk of right atrial blockage and/or the risk of of embolization, surgery was elected. Extended resection was done with cardiopulmonary bypass. Histological examination revealed metastasis of poorly differentiated thyroid carcinoma to the thymus, innominate vein, superior vena cava and right atrium.
We herein report the progression of this case and review the literature of intra-atrial tumor extension of thyroid cancer.
Intracardiac papillary thyroid cancer
A Comparison of I 131 Postoperative Ablation in Stage 1 Differentiated Thyroid Cancers in Norman Regional Hospital in 2008 Versus 2009 to Assess Practice Change After 2009 American Thyroid Association Guidelines Regarding USE of I 131 Ablation in Stage 1 Thyroid Cancer
Thyroid Cancer Friday Poster Clinical
Radioactive iodine has been used to treat thyroid cancer since 1946. Radioactive iodine treatment is given after thyroidectomy to ablate the remnant thyroid tissue and to treat metastatic thyroid cancer. Studies have shown regional differences in opinions on adjuvant radioactive iodine treatment of thyroid carcinoma within Canada and the United States. According to the American thyroid association guidelines 2009, I 131 is not indicated in stage 1 differentiated thyroid carcinoma unless patients have multifocal disease, nodal metastases, vascular invasion or more aggressive histological features. I 131 treatment is associated with both long and short term complications such as nausea, vomiting, ageusia, pain, recurrent sialoadenitis, xerostomia, dental caries, pulmonary fibrosis, nasolacrimal outflow obstruction and second primary malignancies.
We obtained data for Norman Regional Hospital Thyroid cancer cases which were diagnosed and treated in 2008 and 2009, including age, gender, stage and type of Thyroid cancers, mode of treatment, post-op I 131 treatment, cancer histology and behavior and use of chemotherapy. This data was compared to other hospitals in the state and nationwide. Percentages of stage 1 thyroid cancer patients who received adjuvant radioactive iodine in 2008 and 2009 were compared.
There were 26 cases of thyroid cancer cases in 2008 which increased to 32 in 2009. There were 20/26 (76%) stage 1 thyroid cancer cases in 2008 and 24/32 (75%) in 2009. We noted that 11/20 (55%) patients with stage 1 thyroid cancer were treated with adjuvant radioactive iodine in 2008 which reduced to 10/32 (31%) in 2009.
A higher percentage of thyroid cancer patients at NRH received adjuvant treatment with I 131 as compared to all other hospitals nationwide in 2008. Fewer patients with stage 1 thyroid cancer were treated with adjuvant radioactive iodine in 2009 which reflects a change in local practice after the release of 2009 American thyroid association guidelines.
Clinical Strategy for Distant Metastasis Cases of Differentiated Thyroid Carcinoma in Tokyo Metropolitan Cancer and Infectious Diseases Center Komagome Hospital, Japan
Thyroid Cancer Friday Poster Clinical
Because our institution is “metropolis and districts cancer medical examination and treatment cooperation foothold hospital”, the distant metastasis patients with thyroid carcinoma (TC) are referred to various medical department and come to our hospital, and we report our clinical strategy (combined modality therapy) for those patients.
On 28 distant metastasis (first or secondary) cases of differentiated thyroid carcinoma (DTC) performed an operation of primary site in our department (ORL/HN Tumor Surgery) for six years until March 2011, we reviewed histopathology type, metastatic site, introduction course, treatment contents and prognosis.
(Histopathology type) Among DTC 112 cases, papillary thyroid carcinoma (PTC) was 94 cases and follicular thyroid cartinoma (FTC) 18, and the ratio was 5.22:1. It was 28 examples that became this examination subject, and PTC 18, FTC 10, the ratio 1.8:1. In comparison with PTC, FTC has higher tendency of first or secondary distant metastasis, clearly. (Metastatic site) In the whole cases, lung metastasis 17cases, bone 14, brain 3, kidney 1. As for the FTC, 9 of 10 cases were metastases to bone. (Origin of introduction from another hospital) Otolaryngology/head & neck 10, orthopedics 4, surgery 4, internal medicine 3, school examination 1 (Main combined-modality-therapy contents) «Our department» Total thyroidectomy 17 cases, extirpation of not-resected lobe 11. «Radiology» Radioactive iodine treatment 27 cases [various parts] Irradiation simplicity 9 [vertebra, rib, skull, brain] «Orthopedics, radiology (anesthesiology)» Excision→IOR (intraoperative radiation) 8 [a vertebra] Only as for the excision 1 [ilium] «Others» Simple excision 3 [cerebellum, lung, mediastinum] (Prognosis) Survival rate after distant metastasis for four years : PTC 92%, FTC 76%.⇒FTC is tend to do distant metastasis in comparison with PTC, and has high frequency of bone metastasis⇒Most cases become adaptation of iodine treatment (27/28); vertebra metastasis 8 cases of those performed IOR, and simple excision of metastatic tumor was possible for 3 other cases⇒As for the FTC which did distant metastasis, prognosis was poor in comparison with PTC of the same state.
Endocrinology, hc fmusp, Sao Paulo, Brazil
Thyroid Cancer Friday Poster Clinical
Background: Metastatic tumor in the thyroid is uncommon and may be a diagnostic problem confused with primary neoplasia of the thyroid. Its presence often indicates a poor prognosis. Objective—To report one case of metastasis of colon tumor in thyroid
Patient: A 75 year old female patient who was admitted at endocrinology clinic in may 2009 after total thyroidectomy for the papillary thyroid carcinoma. Before thyroid surgery she presented thyroid nodule of 6.0 cm which had been growing for three years concomitant with hoarse voice. The fine needle aspiration biopsy had showed folicular cels in papillary arrangement with nuclear polymorphism and intracelular groves and pseudo nuclear inclusions suggestive of papillary thyroid carcinoma.
The histopathology was inconclusive for diagnosing papillary thyroid carcinoma. The immunohistochemical stainining showed positiveness for colon metastatic carcinoma. The patient was submitted of colon carcinoma resection in 1998 and three years after developed a pulmonary metastasis and received chemotherapy three years after colon surgery. There were no liver metastasis at time. For five years she had no complaint when the hoarseness and neck mass started. The evolution showed a thracheal obstruction as well as progressive dispnea so that it was introduced a definite thracheostomy. The breathing aspect remains stable at present. In addiction the abdome and chest CT detected hepatic and pulmonary metastasis and cervical US showed a mass of 7.0 cm in diameter without any conditions for chemotherapy or surgery.
Comments: This case shows that the citologic exam of epitelial tissues may cause confusion and misdiagnosis. We would like call attention of secondary tumor in thyroid is uncommon, but the number of these cases seems to have increased in recent years by new therapeutics. It should always be considered in patients with a thyroid nodule and a history of cancer.
Key Words: Neoplasm Metastasis; Colon Carcinoma; Thyroid Gland
Endocrinology & Metabolism Institute, Cleveland Clinic, Cleveland, OH
Thyroid Cancer Friday Poster Clinical
Differentiated thyroid carcinoma is known to metastasize to unusual body areas.
We describe the case of a patient with papillary thyroid carcinoma found to have abnormal intense uptake in an abdominal lesion on post-therapy radioactive iodine scan.
The patient was a 60-year old woman who had a fine needle aspiration of a 26-mm right thyroid nodule which showed a hypercellular aspirate suspicious for a follicular neoplasm. She underwent a right thyroid lobectomy and isthmusectomy. The nodule was a papillary carcinoma of the follicular variant that did not invade the peri-thyroidal soft tissues. A completion thyroidectomy followed and there were no other foci of cancer. Final stage was pT2 Nx Mx. The patient elected to have radioiodine ablation off thyroid hormone. Her pre-withdrawal serum thyroglobulin was undetectable and that rose to 3.2 ng/mL (negative antibodies) when her endogenous thyrotropin was 73 mU/L. The whole body post-thyroidectomy scan with 2 mCi I-123 NaI showed 3% neck uptake at 20 hours. There was no abnormal uptake elsewhere. 70 mCi I-131 NaI was administered. A whole body scan obtained 10 days after the treatment showed intense focal tracer accumulation in the right posterior lateral abdomen. SPECT-CT images localized the activity corresponding to a 2×0.9 cm soft tissue nodule in the inner surface of the right posterior abdominal wall adjacent to the posterior edge of the liver. No change in the size or appearance of the lesion was noted on the follow-up CT. The patient elected to have the mass resected. A 1-cm white cystic mass was identified on laparoscopy on the inner surface of the abdominal wall, which was corresponding to the imaging finding. The final pathology diagnosis of the resected mass was a benign epithelial-lined cyst with chronic inflammation. Immunohistochemical stains for TTF-1 and thyroglobulin were negative.
This is the first case of a benign peritoneal cyst accumulating radioiodine, mimicking thyroid cancer metastasis.
Geriatrics Unit, University of Pisa, Pisa, Italy
Thyroid Cancer Friday Poster Clinical
Thyroid cancer can originate from activating mutations or rearrangements in the RET gene and is characterized by a marked angiogenic activity. Sunitinib, a novel tyrosine kinase inhibitor binding to the vascular endothelial growth factor receptors and other mutant kinases associated with thyroid cancer, showed promising results in preliminary clinical experiences. Aim of this report was to evaluate the clinical response and safety profile of sunitinib in off-label treatment of advanced thyroid cancer patients.
11 adult patients with a diagnosis of RAI-refractory advanced thyroid cancer (papillary, follicular and Hurthle cell) were treated with sunitinib and followed by both FDG-PET-CT every six months and thyroglobulin level evaluation, and monitored for adverse events.
Patients (5 women and 3 men) with DTC were treated for at least 6 months (mean 12.5 months). All the patients started sunitinib at 50 mg daily dose (4/2 weeks schedule). We documented partial response in tree patient with substantial regression of lymph node, lung and, in one case, in liver metastases, progression disease (bone metastasis) in two patient and stable disease along with marked improvement of clinical symptoms in the other tree patients. Tree male patients stared sunitinib less than six months ago and have not been yet evaluated for clinical response. Sunitinib therapy was free of significant adverse events up to the first 3–4 months in all the patients when fatigue, mainly at the end of treatment cycle, hypothyroidism (TSH elevation), hypertension (worsening of blood pressure control by current treatment), diarrhea, mucosal aphthae, headache, hematologic toxicity (macrocytosis) and amenorrhea were experienced. No grade IV toxicity was observed during treatment. In two patients we observed low fT3 levels that needed an increase dosage of LT4 or LT4/T3 combined therapy.
In patients with refractory thyroid tumors who have evidence of progressive disease, sunitinib is able to induce responses or disease stabilization in the great majority. Side effects represent the main obstacle to long term therapy.
Medicine, Mayo Clinic, Rochester, MN
Thyroid Cancer Friday Poster Clinical
The PAX8/PPARγ fusion protein (PPFP) present in 36% of follicular thyroid carcinomas (FTC) is considered a putative oncogene due to its in vitro characteristics. However, its precise role in FTC tumorigenesis is unknown. Meta-analysis of extant studies of disease progression in human FTC with and without PPFP indicate that 68% (χ2=0.008) of PPFP-positive FTC are associated with minimally invasive disease (Reddi et al., Genes & Cancer, 2:46–55, 2011). Also, constitutive expression of PPFP in multiple FTC-derived cell lines, inhibited cell growth in vitro and xenograft tumor progression in vivo, indicating that PPFP may function as a tumor suppressor in FTC (Reddi et al., op. cit.). Studies of the mechanism of PPFP tumor suppressor function indicate that it modulates the expression of multiple tumor suppressors, including TIMP-3, PTEN and microRNAs-122 and 375, suggesting its possible use as a prognostic marker in FTC, with implications for theraputic potential.
Stable cells constitutively expressing PPFP were generated in multiple cancer-derived cell lines, including anaplastic thyroid (FRO and KTC-3), colon cancer (ARO), and Melanoma (DRO). Quantitative PCR, western blotting and/or immunohistochemistry were used to confirm expression of PPFP and all molecules known to be modulated including TIMP-3, VEGF, PTEN, miR-122, miR-375 and CD-31.
Expression of PPFP did not affect growth of any cell line in vitro. However, xenograft tumor growth of all PPFP cell lines was inhibited (2–5 fold, p<0.05) in vivo. CD-31 staining was reduced in all the xenograft models expressing PPFP, suggesting the inhibition of neo-vascularization as a potential mechanism. Quantitative PCR studies demonstrate that ARO-PPFP and DRO-PPFP cells are associated with a 2-fold (p<0.005) upregulation of the tumor suppressor TIMP-3, an angiogenesis inhibitor. Studies are currently ongoing to understand the mechanism of PPFP-mediated tumor suppression in the ATC-derived cell lines, including redifferentiation.
Our studies demonstrate for the first time that PPFP, which appears to function as a novel tumor suppressor in FTC, inhibits xenograft tumor growth in non-FTC cancers, highlighting its potential as a novel global cancer therapeutic.
Summary of the Effect of PPFP Expression in Multiple Cancer Derived Cell Line Xenografts In Vivo
Thyroid Cancer Friday Poster Clinical
Some thyroid cancer survivors suffer from recurrent or persistent disease in the neck. Our objective was to explore the experience of thyroid cancer survivors who were treated with neck re-operation for recurrent or persistent disease.
We recruited individuals aged 18 years or older with a history of non-medullary thyroid cancer, who had neck re-operation for disease recurrence or persistence, more than 6 months after completion of primary thyroid surgery. In-depth individual interviews were conducted and a qualitative analysis was performed.
Preliminary data from the first 5 participants in this ongoing study were analyzed, and updated data will be presented. The first 5 participants were 4 women and 1 man, aged 31 to 45 years. All had one re-operation for recurrent or persistent disease in the neck, within the years 2009 to 2011. The major themes that emerged from the qualitative analysis were as follows: 1) Thyroid cancer recurrence or persistence requiring surgery is devastating and triggers thoughts of shock and uncertainty, 2) Patients consult their treating physicians and the internet for information, 3) Treatment decisions are made using a shared-decision making approach with treating physicians and surgeons, 4) Patients with disease recurrence or persistence turn to a variety of sources of social support including family, co-workers, health care professionals and other professionals, and 5) Unmet needs of patients include a paucity of information available about disease recurrence or persistence, as well a lack of in-person support groups dealing with this issue.
Local-regional recurrence or persistence of thyroid cancer requiring surgery is a devastating experience for survivors. Thyroid cancer survivors' needs for specialized information and social support may be incompletely met throughout this experience.
Otolaryngology Head & Neck Surgery, South Infirmary Victoria University Hospital, Cork, Ireland
Thyroid Cancer Friday Poster
Despite preservation of the recurrent laryngeal nerve (RLN), transient vocal cord paralysis (VCP) occurs after 1.2%–10.9% of thyroidectomies. We studied risk factors for transient VCP after thyroidectomy.
Prospective study of 163 (88 bilateral, 75 unilateral) consecutive thyroidectomies performed by a single surgeon. All patients underwent laryngoscopy pre-operatively, and within two weeks postoperatively. Fisher's exact test was used to test for significant association between variables studied and postoperative VCP.
5 patients were excluded (two with pre-existing VCP; and 3 without postoperative laryngoscopy). There was one intentional sacrifice of a RLN, and one unintentional RLN transection. Of the remaining 241 RLNs-at-risk, 13 (5.4%) had postoperative VCP. Revision surgery (p=0.04); operative findings of cancer invading the RLN requiring sharp dissection to separate the nerve (p=0.008); and operative findings of RLN extensively draped along thyroid or intimately associated with thyroid parenchyma at Berry's ligament (p=0.007) were significantly associated with VCP. Malignancy; concomitant central compartment neck dissection; extralaryngeal RLN branching; hyperthyroidism; retrosternal extension; and bilateral surgery, were not significant. Two of the patients with VCP had immediate onset of significant hoarseness and swallowing symptoms. 6 had mild hoarseness, and 5 had very subtle vocal changes. Of cases with follow-up exceeding 6 months, 90% (9/10) showed full resolution of VCP on follow-up laryngoscopic examination.
Revision surgery, invasive cancer, and variants in the anatomic course of the RLN are risk factors for transient VCP after thyroidectomy.
Endocrinology, Cleveland Clinic, Cleveland, OH
Thyroid Cancer Friday Poster Clinical
Practice guidelines of American Thyroid Association (ATA) recommend use of neck ultrasonography (US) in the follow up of the patients with well differentiated thyroid carcinoma (WDTC) in the 6–12 months period after initial treatment and then periodically thereafter. This approach is valuable in patients with less-than well differentiated tumors and in patients with thyroglobulin autoantibodies (Tg-abs). However, the majority of patients have low risk disease WDTC and no Tg-abs. We questioned the value of routine postoperative ultrasound in the management of patients who are considered cured after initial treatment based on post-treatment I-131 scan and undetectable thyroglobulin (Tg) levels.
We examined the medical records of patients with the diagnosis of thyroid carcinoma that had a neck US in the Endocrinology and Metabolism Institute of Cleveland Clinic during the period from January 2008 through December 2009. We excluded patients who had had histologies other than papillary or follicular thyroid carcinoma. There were 206 patients, aged 15–87 years (at last evaluation). There were 19.4% males and 80.6% females. Papillary thyroid carcinoma was present in 94% of patients and follicular carcinoma in 6%. We determined the patterns of findings in patients who were diagnosed with disease persistence or recurrence and in those who were considered cured.
In the group of patients with persistent or recurrent neck disease (N=12), Tg level was positive in 70% of patients, radioiodine scan in 10% of patients and neck US exam in 70% of patients. There were no cases in which neck US exam was positive while Tg level was undetectable. In the group of patients with undetectable Tg levels, 10% had positive findings on neck US but no recurrence was detected on further evaluation.
We conclude that the routine performance of neck US may not be cost-effective in the follow up of patients with WDTC who have no Tg-abs after initial treatment if Tg level remains undetectable. More data are needed to confirm this conclusion.
Oncology, Georgetown University Medical Center, Washington, DC
Thyroid Cancer Friday Poster Clinical
Micro-RNAs (miRNA) represent a class of endogenous noncoding RNAs that regulate gene expression and may have an impact on a number of processes implicated in carcinogenesis. Some studies indicate that there may be deregulation of miRNAs in different types of thyroid tumors. Objective: To identify miRNA expression patterns that may be used to aid in the diagnosis of different types of thyroid cancer and hyperplastic nodules.
We examined the micro-RNA profile of 23 thyroid tissue samples: 4 nodular hyperplasias (NH), 5 follicular carcinomas (FC), 5 follicular adenomas (FA), 5 papillary carcinomas (PC) and 4 normal thyroid tissues. Following amplification by PCR we screened over 75 distinct miRNAs, and quantified the level of expression of each within each tissue group, comparing the groups to determine if there was differential expression of the individual miRNAs among each pair. Those miRNAs with differential expression among two groups of samples were arranged into heat maps to visually represent the degree to which each miRNA was under-expressed or over-expressed.
Ten individual miRNAs showed significantly differential expression between the NH and FC tissue groups, 12 between the NH and the FA groups, 9 between the NH and PC groups, and 21 between the FC and FA groups. Additionally, there were 27 miRNAs that were differentially expressed between the FA group and the PC group and 39 between the FC group and the PC group. A distinct pattern emerges for each comparison of tissue samples, with PC and FA generally showing over-expression in the majority of miRNAs tested, and FC and NH generally showing under-expression. Additionally, there is relatively little overlap in the miRNAs which showed differential expression between groups of tissue samples, indicating that miRNAs may be used as biomarkers of particular types of thyroid cancer.
The MiRNAs examined indicate significantly different expression patterns in normal, NH and different types of thyroid cancers. If replicated in larger studies, this may be a diagnostically useful tool to distinguish between normal or hyperplastic tissue and malignant tissue, and provide early identification of the type of thyroid cancer.
Endocrinology & Metabolism Institute, Cleveland Clinic Foundation, Cleveland, OH
Thyroid Cancer Friday Poster Clinical
When two primary cancers share cytological features, it can be a challenge to differentiate between a metastatic lesion versus a second malignancy.
We describe the case of a 56 year-old man with history of emphysema secondary to cigarette smoking. The patient initially presented with hemoptysis after interventional angioplasty for anginal pain. A chest radiograph showed left hilar fullness confirmed by computed tomography (CT). These findings prompted a bronchoscopy which demonstrated a left upper lobe endobronchial lesion; biopsy revealed invasive squamous cell carcinoma strongly positive for cytokeratin 5/6 and negative for TTF-1. A staging positron emission tomography CT scan showed a confluent area of fludeoxyglucose-avid lymphadenopathy in the right cervical chain and left hilum. Because of these findings, a mediastinoscopy was performed and a benign left hilar lymph node (LN) was found. Based on the aforementioned evaluations, the patient subsequently had a left upper lobectomy. Pathology from this surgery confirmed the diagnosis of invasive, non-keratizinizing, papillary-type squamous cell carcinoma. A CT-guided right cervical node biopsy was done, and cytology showed non-small cell cancer with papillary features.
The cytologist had difficulty ascertaining the origin of the carcinoma but suspected a thyroid primary. Consequently, the patient underwent a needle aspiration of his cervical LN and the thyroglobulin (Tg) level in the needle washing was 142,286 ng/mL. The serum Tg level was 211 ng/mL (normal: 0.8–49 ng/mL) with negative antibodies. The TSH and TSH-receptor mRNA were 5.17 (normal: 0.4–5.5 μU/mL) and <1.0 (normal: <1.0 ng/μg), respectively. A total thyroidectomy with right neck dissection was recommended. Pathology showed tall cell variant of papillary thyroid carcinoma (PTC) with invasion of the strap muscles. Bilateral level VI and right modified radical (levels I-V) nodal dissection showed 18/62 nodes positive for PTC.
A biochemical marker, such as Tg from a suspicious cervical LN, can help elucidate the diagnosis of a new primary cancer. In our patient, the clarification improved the severity of his lung cancer from stage IV to stage I disease, thereby modifying his predicted prognosis.
Revisiting the Use of PPARγ Agents in Patients Undergoing Reablation with RAI for Metastatic Thyroid Cancer: Have We Given Up on These Agents Too Early?
Thyroid Cancer Friday Poster Clinical
Adjuvant radioiodine therapy is the only proven therapy for patients with metastatic differentiated thyroid cancer. However, due to loss of differentiation by cancer cells, repeated therapy is less effective in a sizable proportion of patients. PPARγ agents have been effective in re-differentiating these cells and enhancing I131 uptake in vitro and vivo. The published literature is modest, comprised mostly of case reports and small series. We describe our experience with the use of these agents in subjects with pulmonary metastasis requiring repeat ablation with I131.
Retrospective chart review of metastatic thyroid cancer patients undergoing RAI ablation.
Thirteen subjects (6 females and 7 males) with known distant metastasis were treated with Rosiglitazone 4–8 mg (n=10) and Pioglitazone 30 mg (n=3) for 6 weeks prior to radioiodine therapy. Eleven of these subjects had radiologically proven lung metastases and the remaining 3 were suspected to have distant metastasis. Their age ranged from 29 to 61 years. All of these patients had a statistically significant drop in their thyroglobulin levels after receiving pretreatment with glitazone (mean pretreatment TG 2070.45 vs. post glitazone RAI therapy TG 1395.73, p value 0.0029). Five out of these thirteen pts (38%) who had no or minimal lung uptake in the prior post therapy whole body scans, showed significant increase in uptake within the lungs following glitazone pre treated RAI therapy. A commensurate reduction in their thyroglobulin levels was also noted. No side effects were observed in these subjects.
In our series, 38% of the patients receiving glitazone pretreatment showed enhanced I131 uptake within lung metastases. These subjects had either negative or lower uptake in the pulmonary metastasis in prior rounds of RAI therapy. We also noted a reduction in serum thyroglobulin levels in all subjects. We did not observe predictive factors to enable patient selection for glitazone pre-treatment. A short, 6 weeks therapy with glitazone agents appears not to be associated with the recently described side effects observed with long term use of these agents.
Thyroglobulin Values Before and After Glitazone Treatment
Note: This is a descriptive statistics for 13 patients.
Thyroid Cancer Friday Poster Clinical
The clinical significance of synchronous bilateral papillary thyroid carcinoma (SBiPTC) has not been fully defined, and the prevalence of BRAFV600E mutation in SBiPTC remains unknown. The purpose of this study was to compare the clinical outcomes and BRAFV600E mutation incidence of SBiPTC patients with those of unilateral papillary thyroid carcinoma (UiPTC) patients.
From 1997 to 2008, a total of 903 patients with papillary thyroid cancer were treated at a single institution. Of 891 studied patients, 177 (19.9%) were SBiPTCs and 714 were UiPTCs. SBiPTC was defined as cancer diagnosed in both thyroid lobes at the same time or within a period of three months. The mean follow-up time was 6 yr, ranging from 2.5–13.5 yr. Rates of disease-free survival (DFS) and overall survival (OS) were calculated and compared. BRAFV600E mutation was determined by PCR amplification and DNA sequencing.
When compared with UiPTC patients, patients with SBiPTC were more likely to have larger tumor size, higher frequency of extrathyroidal invasion and lymph node metastasis, and have more advanced stage. The 5-year DFS rate was 86.0% for SBiPTC patients and 94.0% for UiPTC patients (p=0.013). The prevalence of BRAFV600E mutation in SBiPTC group was significantly higher than that in UiPTC group (65.7% vs. 50.4%; p=0.038).
Patients with SBiPTC present with more advanced tumor stage and have shorter disease-free survival than UiPTC patients. Poorer outcomes of these patients may be at least partially explained by the high incidence of BRAFV600E mutation.
Kaplan-Meier survival curves showing disease-free survival for patients with synchronous bilateral papillary thyroid carcinoma (SBiPTC) and controls with unilateral papillary thyroid carcinoma (UiPTC).

While T3 May Stimulate Fibroblast Migration, T3 Does Not Stimulate Keratinocyte Migration Independently
Thyroid Hormone Action Friday Poster Basic
Although the physiologic role of thyroid hormone in skin is not well understood, we have determined that triiodothyronine (T3) is necessary for optimal cutaneous wound healing and that supra-physiologic T3 doses can accelerate wound healing. Important steps in cutaneous wound healing include inflammatory cytokine release, cell migration, cell proliferation and cell differentiation. We have identified a role for thyroid hormone in stimulating epidermal keratinocyte proliferation using both in vitro and in vivo models. The goal of this project was to expand our investigation and determine whether T3 administration could accelerate migration of cutaneous cells.
We used an in vitro assay of cell migration. Briefly, T3 was diluted to the several concentrations. Human epidermal keratinocytes were grown to confluence in 24-well plates. Then, a cross-shaped scratch was created in each well. Images of the scratches were captured using a phase-contrast microscope at baseline and post-scratch to assess the migration rate of the cells. Areas of the scratches were measured. Each dose was evaluated a minimum of 8 times. In order to focus the studies on migration, a standard dose of the proliferation inhibitor, mitomicin, was added for all conditions and the experiment repeated.
In the absence of mitomicin, a trend seemed evident toward a dose-dependent increase in keratinocyte migration in response to T3 administration. Relative to control keratinocyte migration, 100 nM T3 resulted in a 15±9% increase, 1 μM T3 resulted in a 16±11% increase, and 10 μM T3 resulted in a 26±12% increase (p=NS). When the experiment was repeated with mitomicin, the effect of T3 was completely lost, suggesting that apparent keratinocyte migration was an artifact of the T3 stimulated proliferation already noted.
Cutaneous cell proliferation and migration represent key steps in wound healing. We previously proposed that T3 stimulation of dermal fibroblast migration serves as part of the mechanism for acceleration of wound healing by thyroid hormone. We extend our model to suggest that while keratinocyte proliferation may be stimulated by T3, keratinocytes are not stimulated by T3 to migrate independently of associated fibroblasts.
T3 and 3,5-T2 Participate in Tilapia Growth Through a Different Signaling Pathway
Thyroid Hormone Action Friday Poster Basic
Considered the biologically active thyroid hormone (TH); triiodothyronine (T3) actions involve TH-dependent de novo gene transcription and are mediated by TH nuclear receptors (TR). Recent studies from our laboratory have shown that in some teleosts, 3, 5-T2 (T2), a TH formed through the outer-ring deiodination of T3 is also bioactive. The effects of T2 appear to be mediated by a different isoform of TRβ1 that contains a 9 amino acid insert in its ligand binding domain, and which we have denominated long TRβ1 (L-TRβ1). To further understand T2 bioactivity and its action mechanism, we used body growth as an endpoint and analyzed the participation of T2 in this process, as well as the possible differential regulation of the signaling pathway of both iodothyronines.
We treated tilapia fingerlings (∼0.8±0.02 g) by immersion with 1.3 nM of one of the following TH: T3, T2, the prohormone T4 and the inactive isomer rT3. A negative control group was treated with methimazole (MMI: 4.5 mM). All experimental groups were treated for 8 hours, three times per week for a month. We recorded growth (body weight) and measured the expression of GH, IGF-1, L-TRβ1 and S-TRβ1 (short TRβ1: without the 9 amino acid insert). These genes are involved in growth and/or are part of TH signaling pathway.
Growth rate of fish exposed to T4, T3 or T2 was significantly higher (+30%) than that of the control (untreated) group, while growth rate of tilapia exposed to rT3 was similar to control fish. Tilapia treated with MMI showed the lowest growth rate (- 15%). Intrahepatic expression of GH and IGF-1 was up-regulated by both, T3 and T2, while the expression of S-TRβ1 increased only in the T3-treated fish and L-TRβ1 was up-regulated only by T2.
Our results support the notion that as T3, T2 participates in the growth process, and that the signaling pathway that mediates its actions is differently regulated from that of T3.
Acknowledgements: Tilapias were kindly provided by SAGARPA, Querétaro, Qro., and kept in laboratory facilities by Miguel Angel Maqueda. Work supported by: CONACYT 080420 and PAPIIT IN208511.
Medicine, University of Chicago, Chicago, IL
Thyroid Hormone Action Friday Poster Clinical
RTH is inherited in a dominant fashion owing to the dominant negative effect (DNE) of the mutant TRβ. Recessive inheritance due to complete absence of the TRβ was observed only in one of more than 500 families. In addition, very severe RTH phenotype was reported in a child homozygous for TRβ Δ337 with DNE and in a young adult harboring only TRβ I280V, likely caused by a deletion of one parental allele.
Clinical and genetic analysis.
Here we present 3 new patients homozygous for TRβ mutations, products of consanguineous parents with classical, monoallelic RTH: an Australian child with the TRβ G347E and two Turkish siblings with TRβ R316C. All three patients presented with thyroid function tests (TFTs) abnormalities typical for RTH, including elevated T4, T3 and rT3 and non-suppressed TSH. However, compared to their heterozygous relatives, iodothyronine values were 3 to 10-fold higher and TSH concentrations ranged from 50 to 500 mU/L. All homozygous subjects had large goiters (one had partial thyroidectomy) and tachycardia. Now ranging in age from 4 to 10 yrs, they have severely compromised intellectual development with impaired speech, hearing loss only partially corrected with hearing aids and growth retardation. The comparison of these new cases and the 3 listed in the introduction revealed that the patients homozygous for TRβ gene mutations (the current three and the one proven to be homozygous for with TRβ Δ337) have a more severe RTH than the subjects homozygous for absent TRβ in terms of TFTs abnormalities, growth retardation, intellectual deficit and goiter size. Nevertheless, the three siblings with absent TRβ had complete loss of hearing compatible with the absolute requirement of TRβ for development of the inner ear, as demonstrated in TRβ deficient mice. The subject TRβ I280V had a phenotype of intermediate severity but was institutionalized.
These unique cases suggest that in the absence of a wild-type TRβ there is a dose related interference of the mutant receptor with the direct effect on gene expression and/or DNE on the TRα. Studies the using recently acquired fibroblasts from heterozygous and homozygous family members may help in understanding the mechanisms leading the severe RTH.
Pharmacology& Exp Ther, Loyola University School of Medicine, Milan, Italy
Thyroid Hormone Action Friday Poster Clinical
Oxidative stress (OS) in subjects with primary hypothyroidism under therapy with L-T4 might be the cause of the side effects commonly found with this treatment.
Twenty four subjects of both sexes (11 M and 15 F), aged between 41 and 61 years, with primary hypothyroidism were assessed. All the subjects were followed for 30 days during the administration of a fixed dose of 75 μg of L-T4. Levels of T4, T3, TSH, hydroperoxides (as measure of OS), hs-CRP were determined in plasma before and after the treatment. Side effects (anxiety/agitation, sweating, palpitations and headache) and number of days of discomfort were measured for 15 days before and for two subsequent 15-day periods.
Administration of L-T4 satisfactorily balanced the hypothyroidism. A high level of hydroperoxides, 370±27.7 U.CARR. (Carratelli Units: 1 U.CARR.=0.08 mg of H2O2/L), was observed before treatment, and L-T4 administration further increased the level up to 435±39.5 U.CARR. (p<0.05). The treatment produces a significant increase in hs-CRP, from 3.2±2.32 to 4.0±1.27 mg/L (p<0.05). Side effects, almost absent at the baseline 15-day control, occurred with high frequencies during the treatment: between 9.6±1.14 days/15 days for sweating and 14.1±0.93 days/15 days for palpitations. Some side effects were found to be linearly correlated with hydroperoxides (r=0.641, p<0.01 and r=0.658, p<0.01 respectively) or with hs-CRP, as in the case of anxiety/agitation (r=0.629, p<0.01). Following L-T4 administration the days of discomfort turned out to be particularly prominent during the two subsequent 15-day controls (3.8±0.75 and 4.8±0.78 days respectively).
Primary hypothyroidism and therapy with L-T4 at a dose of 75 μg/day cause OS. Side effects following L-T4 therapy depend on OS and cause daily discomfort and loss of working activity in about 1/3 of the days considered.
A Central Role for AMPK in Thyroid Hormone Production
Thyroid Hormone Metabolism and Regulation Friday Poster
The synthesis of TH is dependent on unique features of thyroid epithelial cells, including the accumulation of iodide, which is mediated by the sodium iodide symporter (NIS). Although TH production and NIS regulation have been studied in detail, many questions remain on the integrated regulation of iodide uptake and the other processes leading towards TH production. We anticipated that AMP-activated protein kinase (AMPK) has a functional role in the thyroid because an intimate relationship between TH and AMPK has been described: both the main activator of TH production, TSH and TH itself are likely to be involved in AMPK repression and activation. The downstream targets of the TSH-receptor, cAMP and PKA, inhibit AMPK activation in several cell-lines whereas TH activates AMPK in several cell-lines. However, the functional role of AMPK in the thyroid remains largely unknown.
We tested the role of AMPK in iodine uptake and NIS expression in FRTL-5 cells using AMPK activators (AICAR, metformin) and the AMPK inhibitor CompoundC. Furthermore, we tested whether TH itself would influence AMPK and NIS expression and iodine uptake in FRTL-5 cells. Currently we are using NIS-promoter(-Luc) constructs of various promoter regions to identify which regulatory elements are involved in the observed AMPK effects.
TSH induced iodine uptake in thyroid follicular cells (FRTL-5), was blocked by AMPK stimulation (6x) whereas AMPK inhibition dramatically increased iodine uptake (7x) after 1 week of treatment. The results in iodine uptake can at least partially be explained by in- or decreased NIS protein levels. TH was able to activate AMPK and decrease NIS expression and iodine uptake after 3 days in a dose dependant manner.
We demonstrate that NIS expression and iodine uptake are partially controlled by AMPK in follicular thyroid cells. As iodine uptake is a vital step in TH formation, the strong effects of AMPK modulation on iodine uptake are likely to affect TH production. In reverse, TH was able to stimulate AMPK and inhibit iodine uptake. Therefore we propose that there may be a short negative feedback loop within the thyroid through AMPK where AMPK activation represses TH production and TH activates AMPK.
Foods and Nutrition, The M.S.University of Baroda, Vadodara, India, 2RMC Unit, BARC, Tata Memorial Hospital, Mumbai, India
Thyroid Hormone Metabolism and Regulation Friday Poster Clinical
Pregnancy is a stage when unpredictable physiological changes occur, which leads to increased thyroidal activity in order to accommodate the demands of pregnant mother and developing fetus. Dysfunctional thyroid gland can lead to hypo or hyperthyroidism during gestation. This may increase the risk of low birth weight, preterm delivery and likelihood of the Caesarean deliveries. These situations are preventable, thus screening becomes a must to treat any dysfunctions. Population based reference values can be generated for diversified regions of the world. In the Indian population, there are few studies reported. Our aim was to observe pattern of thyroid hormone levels in Low income group of Gujarat, India and create a database.
Thyroid hormones analysis by RIA
Serology for 256 pregnant women (<15 weeks) attending antenatal clinic with no apparent thyroid dysfunctions were enrolled from a semi govt. Hospital of Vadodara, India. Serum samples were analyzed using RIA method in order to determine levels of thyroid hormones. Mean TSH, FT4 and TT4 observed were 2.2 μIU/ml, 0.88 ng/dl, 10.29 μg/dl respectively, with 23% prevalence of SCH, 11% OH and 12% hypothyroxinemia. 150 subjects were randomly sub grouped to be followed till the end. Second trimester results revealed TSH, FT4 and TT4 as 2.473 μIU/ml, 0.86 ng/dl and 10.79 μg/dl respectively whereas third trimester hormone levels followed by 2.8 μIU/ml, 0.805 ng/dl and 11.6 μg/dl.
It is evinced from the analysis that, a few subjects had suboptimal hormone levels throughout all 3 trimesters, which may hamper the physical and psychomotor development of fetus. The overall pattern is suggestive that, all subjects had normal values according to gestational age for FT4, TSH and TT4. The observed values are coinciding with one of the earlier studies (Marwaha et al,2008) carried out on reference values for the Indian pregnant women.
Pathophysiology Based Review of Food and Drug Interactions with Levothyroxine Therapy
Thyroid Hormone Metabolism and Regulation Friday Poster Clinical
Levothyroxine is the fourth most prescribed drug in the United States in 2010, and is used in primary therapy for hypothyroidism and differentiated thyroid cancer. Pharmacologic interference of levothyroxine action by drugs and food substances is well-established and remains a challenge in clinical practice, particularly in the elderly population where polypharmacy is common. Most reviews of these interactions are not based on underlying pathophysiological mechanisms, and do not review the strength of evidence for the proposed interactions. We reviewed the literature to classify proposed mechanisms for interactions and assessed the accompanying evidence.
We searched the literature for drugs, foods and supplements affecting levothyroxine pharmacokinetics using available scientific databases including MEDLINE, EMBASE, Scopus and Web of Science. A total of 80 citations were identified between 1980 to December 2010. These articles were reviewed for the agent of interference, the proposed mechanism and the level of supporting evidence.
Several agents interfering with levothyroxine pharmacokinetics have been identified. The level of evidence for these interactions varies significantly from individual case reports to prospective studies. Multiple mechanisms have been proposed most of which are theorized and some experimentally demonstrated. The most common mechanism with the strongest level of evidence was interference with levothyroxine absorption in the gastrointestinal tract, including the effect of calcium and iron. Other proposed mechanisms, with variable degree of experimental evidence, include interference with protein-binding, efflux/influx transporters, deiodination, hepatic metabolism, excretion, nuclear protein binding and effects on the hypothalamus and pituitary gland.
We have catalogued several proposed mechanisms for interactions between drug and food products with levothyroxine therapy, with the strongest evidence for interference with absorption in the gut. We established a framework for a pathophysiological approach to assess these interactions, and highlight areas of knowledge deficiency that require further investigation.
Clinical Strategy for Primary Hyperparathyroidism in Japan
Thyroid Imaging Friday Poster Clinical
Preoperative localization investigation is very important for parathyroidectomy to avoid severe surgical complications, for example, recurrent nerve paralysis. We report recent clinical strategy for primary hyperparathyroidism in our institution.
Between 2003 and 2010, parathyroidectomy was performed for 18 patients with primary hyperparathyroidism. We focus on the efficacies of preoperative examinations and examined these cases retrospectively.
We used ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI) and 99mTc-hexakis-2-methoxyisobutylisonitrile scintigraphy (MIBI) for preoperative localization test. In these 18 cases, 15 patients (83%) could be used MIBI. The localizing sensitivities of US, CT, MRI and MIBI were 85.7%, 92.3%, 87.5% and 85.7%. Especially for parathyroid adenoma, MIBI sensitivity was 100%. Although MIBI sensitivity decreased in cases of multiple goiters and secondary hyperparathyroidism, combination with other modalities enabled 100% sensitivity to localize hyperparathyroid preoperatively.
In spite of well-known MIBI efficacy for hyperparathyroidism, its usage in Japan had been restricted until 2010. The sensitivity of MIBI was highly satisfactory for minimum invasive parathyroidectomy in our faculty. We really hope much more prevalence of MIBI usage for parathyroidectomy in Japan.
Department of Molecular and Clinical Endocrinology and Oncology, “Federico II” University of Naples, Naples, Italy
Thyroid Nodules and Goiter Friday Poster Clinical
Thyroid nodules (TNs) are common in the general population, with a prevalence of about 50% in subjects older than 60 years. Percutaneous radiofrequency thermal ablation (RTA) is a new promising approach to manage TNs. The aim of this study was to investigate effectiveness and safety of RTA in the treatment of TNs with pressure symptoms in patients not receiving surgery and radioiodine.
Fourty patients with TNs with pressure symptoms were included in the study. Twenty-two patients had non-toxic TNs and 18 patients had toxic TNs and were treated with metimazole. In all patients a fine-needle aspiration cytology was performed to exclude a thyroid malignancy. Twenty patients were treated with RTA (group A) and 20 other patients were not treated (group B). Age, gender, TN volume, function and ultrasonographic characteristics did not differ significantly between groups. RTA was performed in day-surgery regimen by using a RITA © Starburst needle under ultrasonographic real time guidance. All patients were clinically, biochemically and morphologically evaluated at baseline and at 1, 3 and 6 months follow-up.
At baseline, TN volume was 13.3±8.0 ml in group A and 11.3±6.9 ml in group B. After treatment, TN volume significantly decreased in group A (8.3±5.2 ml at 1 month, 5.9±4.1 ml at 3 month, 3.8±3.3 ml at 6 month; p<0.0001) and remained stable in group B (11.3±6.9 ml at 1 month, 11.2±6.8 ml at 3 month, 11.4±6.9 ml at 6 month; p=NS). At 3 and 6 month evaluation, TN volume was significantly lower in group A than in group B, p<0.0001. At the end of the follow-up, pressure symptoms were improved in all patients of group A while persisted unchanged in group B. In group A, hyperthyroidism completely recovered in 40% of patients with toxic TNs, improved in 40%, while it was unchanged in 20% of these subjects as well as in 100% of patients with toxic TNs of group B. RTA was safe and well tolerated in all patients.
RTA significantly decreases TN volume resulting in parallel improvement of pressure symptoms and hyperthyroidism. RTA may represent a valid therapeutic approach in patients with TNs who refuse or are not candidate to conventional treatments.
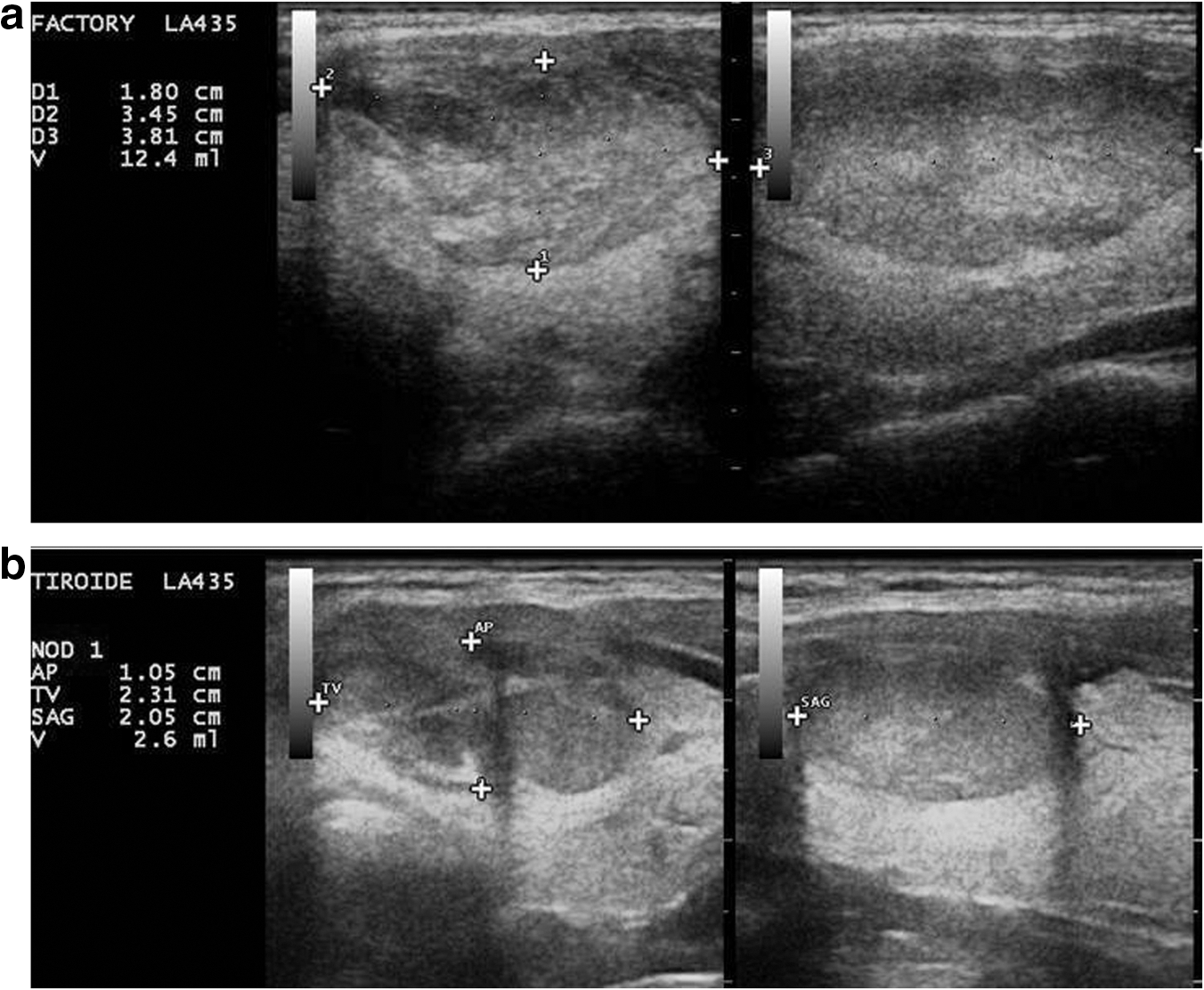
Thyroid nodules treated with radiofrequency thermal ablation.
Thyroid Nodules and Goiter Friday Poster Clinical
To confirm safe implementation of a new technique, we analyzed one institution's evolution from endoscopic (ET) to robotic-assisted (RT) single incision transaxillary thyroidectomy by assessing perioperative outcomes.
Between January 2010 and May 2011, 7 patients underwent ET and 10 patients underwent RT. A gasless, single incision transaxillary approach was used in both groups. Demographic characteristics, perioperative clinical outcomes, complications and pathologic features were compared prospectively
Both patient groups had similar age (ET: 46.1±10.9 years, RT: 37.5±13.6 years, p=0.183) and body mass index (ET: 22.8±4.1 kg/m2, RT: 25.9±5.6 kg/m2, p=0.231). Intraoperative data was similar between the two groups. The mean total anesthesia time for the ET group was 249.7±37.5 min and 252.9±35.0 min for the RT group (p=0.860). The mean total procedure time for ET 148.9±29.8 min and 179.3±36.8 min for RT (p=0.091). There was no difference in estimated blood loss (ET: 39.4±37.4 mL, RT: 25.8±12.4 mL, p=0.474) or length of hospital stay (ET: 0.6±0.5 nights, RT: 0.6±0.5 nights, p=0.913). The mean tumor diameter was 2.18±1.45 cm in the ET group and 1.49±0.72 cm in the RT group (p=0.285). Final pathology indicated benign thyroid tumors for the majority of patients (n=14), except 3 cases of papillary thyroid microcarcinoma. No major perioperative complications occurred in either group. Minor complications included seroma, transient hoarseness, and intraoperative external jugular vein injury in the ET group and transient chest wall numbness, mild chest pain and tightness, shortness of breath, and a rash at incision site in the RT group. One case in the RT group was converted to non-robotic endoscopic thyroidectomy due to mechanical failure of the robot during surgery.
Single incision endoscopic transaxillary thyroidectomy can be performed safely. Our study suggests that although there is relatively no difference in perioperative outcomes between the two procedures, it is important for surgeons to gain sufficient expertise in the non-robotic approach before proceeding to robotic-assisted single incision endoscopic transaxillary thyroidectomy.
Endocrinology and Nutrition, Germans Trias i Pujol, Hospital, Institut Català de la Salut, Badalona, Spain
Thyroid Nodules and Goiter Friday Poster Clinical
There is very few information in the usefulness of postoperative intact parathyroid hormone determination (iPTH) to predict permanent hypoparathyroidism after thyroid surgery. The aim of the present study is to determine the value of iPTH concentration after total thyroidectomy (TT) to predict permanent hypoparathyroidism (PH). Secondary aims are to determine the prevalence of hypocalcemia (hypoCa) and iPTH deficiency after 24 h of this surgery, and its relationship with symptoms of hypoCa.
Forty-six consecutive patients (p) who underwent TT were included in the study. iPTH (normal values 15–65 pg/mL, by an imnunochemiluminometric technique) and albumin-corrected serum calcium concentrations (Ca) were measured at 24 h, 1 and 6 months after surgery. HypoCa was defined as Ca<2.10 mmol/L and iPTH was considered to be low if it was <15 pg/mL. PH was diagnosed in p with serum iPTH <15 pg/mL at 6 months after surgery. Symptoms of hypoCa were recorded.
Twenty-nine (63%) out of 46 p presented hypoCa at 24 h after TT (7/29 were symptomatic); 24 h post TT, iPTH was 26.1±12.65 pg/mL vs 17.2±12.5 pg/mL (p<0.001) in normocalcemic vs hypocalcemic p; 13 out of 46 (28.2%) p showed iPTH concentrations <15 pg/mL. Twelve of them, developed hypoCa and 7, experienced symptoms. P with iPTH deficiency had lower postoperative Ca concentrations (1.97±0.08 vs 2.08±0.09; p=0.025). Among the 29 p showing postsurgical hypoCa, iPTH deficiency was detected in 4 (13.8%) at 1 month and in 3 (10.3 %) at 6 months. Among the 13 p with low iPTH at 24 hours, iPTH deficiency was found in 5 (38.5%) at 1 month and in 4 (30.8%) at 6 months postsurgery. An iPTH concentration at 24 h postsurgery <5.8 pg/mL was 100 % sensitive and 87.8% specific to predict permanent hypoparathyroidism with a PPV of 44.4% and a NPV of 100%. In contrast, a calcium value <2.1 mmol/L predicted permanent hypoparathyroidism with a sensitivity of 75% and specificity of 36.5%.
An iPTH concentration >5.8 pg/mL at 24 h after total thyroidectomy predicts normal parathyroid function at 6 months.
Endocrinology & Metabolism Institute, Cleveland Clinic, Cleveland, OH
Thyroid Nodules and Goiter Friday Poster Clinical
Thyroid implants are rare and occur in the setting of prior thyroid surgery.
We review the case of a patient with a remote history of total thyroidectomy who presented with a supraclavicular mass.
A 51 year old woman consulted her otolaryngologist for a painless right supraclavicular mass. She had a history of total thyroidectomy for a large benign goiter 15 years prior to presentation and she had been maintained on levothyroxine 25 mcg with a serum TSH of 5.4 mU/L at presentation (normal 0.27–4.2). A fine needle aspiration (FNA) showed rare clusters of uniform epithelial cells that were positive for CAM5.2 and TTF-1 suggestive of thyroid follicular origin. Computed tomography showed absence of the thyroid gland and a complex enhancing mass in the right supraclavicular area within the distal sternocleidomastoid (SCM) muscle that measured 28×23×18 mm. Another large enhancing mass measuring 28 mm was seen in the left anterior triangle within the infrahyoid muscle. Neck ultrasonography showed a right level-IV ovoid mass located posterior to the right SCM muscle. The mass measured 30×23×18 mm and contained two hypoechoic areas that were suggestive of confluent lymph nodes; they displayed rich and disorganized vascular flow. No clacifications were noted. In level 3 on the right, there was another ovoid hypoechoic mass resembling a lymph node, measuring 24×12×6 mm that did not have a hilum and contained punctate microcalcifications. Thyroglobulin concentration was 711 ng/mL in needle washing from the supraclavicular mass. FNA cytology from the left neck mass was non-diagnostic. The patient underwent bilateral extended neck dissection and resection of soft tissue tumors from deep intramuscular structures and right subtotal SCM resection. Pathology from the neck masses showed nodules of hyperplastic thyroid gland tissue with associated skeletal muscle and fibroadipose tissue. All lymph nodes were negative for neoplasm. Her post-operative course was unremarkable.
Thyroid implants should be part of the differential diagnosis of patients with a history of thyroid surgery and they can present as suspicious masses outside the operative field.
Post Total Thyroidectomy Hypocalcemia: A Multifactorial Approach to Enable Its Prediction to Facilitate Early Discharge
Thyroid Nodules and Goiter Friday Poster Clinical
After total thyroidectomy (TT) hypocalcemia occurs in some patients. This is a limiting factor in the early discharge. No single factor can predict its occurrence. However presence of a scoring system involving multiple factors can predict this event enabling selective early discharge.
Prospective study at a tertiary care centre. 145 consecutive patients of TT operated for benign goitres are included in the study. Age, presence of hyperthyroidism, pre operative S Calcium & 25 OH VitD, post operative i PTH at 8 hrs & calcium at 12hrs, intraoperative parathyroid preservation status and nodule size were studied. Hypocalcemia score was designed based on these factors (0 to 8). Data analysed with SPSS vs. 13 and appropriate statistical test applied.
30.34% (n=44) developed hypocalcemia. Hypocalcemia commonly developed in patients with low pre operative calcium (p=.008) and S Vit D (p=0.00), lesser number of parathyroids preservation at surgery (p=0.00), Low post operative iPTH at 8hrs (p=0.00) and S calcium at 12hrs (p=0.00). Age of the patient (p=0.2) and nodule size (p-0.17) was not significantly different. Hypocalcemia risk score of >3 had 91% sensitivity, 84% specificity with a PPV of 71% and NPV of 95% whereas a score≥4 had 100% specificity and PPV.
Development of hypocalcemia after TT is multifactorial and a combination of factors can be used to predict it and selectively practice early discharge.
Dept of Developmental Biology, Stanford University School of Medicine,, Standford, CA 94035, CA
Disorders of Thyroid Function Thursday Poster Clinical
An Asian woman had synovial sarcoma (SS) of the right infratemporal fossa diagnosed on Feb 2008, at age 32. Because of the high rate of recurrence and metastasis, she received radiotherapy (Mar-Apr 2008) and chemotherapy (Jun-Oct 2008). Leukopenia and thrombocytopenia ensued. Because of the poor prognosis of SS and fairness in general conditions (ECOG grade 1), she pursued experimental immunotherapy (Feb-Apr 2010).
At the end of Mar 2010, hyperthyroidism (Hypert) developed (TSH=0.13 mU/L, FT3=4.8 pg/ml, TSI=152%, nv<140). Three weeks later, TSH was 0.02, FT3 5.9, with FT4 high (20.4 pg/ml). At the end of Oct 2010, TSH was <0.02, FT3=11.7, FT4=32.6, TSI=248. Not wanting to compromise the effects of immunotherapy and fearful of the hematological side-effects of both ATD and 131I, she refused ATD and 131I, but accepted propranolol(80–20 mg/d). Having become aware of CAR as ancillary therapy for Hypert, based on work by S.B., on Oct 29 2010, she started oral CAR (Sigma-tau, Gaithersburg, Md) at 4 g/d.
Clinical improvement was such that CAR was reduced to 1 g/d. At this point she contacted S.B. Hypert worsened biochemically (FT4 and FT3 consistently >50 and >20, TSI increased to 501) but not clinically. Having accepted the advice from S.B on thyroidectomy as the only other radical cure prior to the appearance of a life-threatening thyroid storm (TS), MIVAT under local anesthesia was performed on Feb 02, 2011. In preparation for MIVAT, lithium was started (300 mg/d) at the end of Dec, then increased at 750 mg/d and stopped 7 days prior to MIVAT. Lugol's solution was started when lithium was stopped, with CAR continued at 1 g/d. MIVAT was uneventful, so CAR was stopped 4 days after MIVAT. As of Mar 2011, under 88 mcg/day L-T4, FT4, FT3 and TSH are 13.7 pg/ml, 2.6 pg/ml and 0.15 mU/L.
This case confirms the great benefits of CAR in severe Hypert, even in clinically compromised patients. Until now, the only report on severe Hypert concerned a young cardiopathic man who survived three subsequent TS that were managed with CAR and low dose ATD (Am J Med, 2003). Considering the high mortality of TS, the role of CAR should be advanced from that of “ancillary” therapy.
Internal Medicine, Division of Endocrinology, University of Wisconsin, Madison, WI
Thyroid Nodules and Goiter Friday Poster Clinical
Obstructive sleep apnea is present in approximately 20% of the general population and when untreated, carries an increased risk of mortality. Patients with goiters often complain of compressive symptoms, which may contribute to symptoms of obstructive sleep apnea. However, the impact of thyroid enlargement on these symptoms is not clear. Therefore we sought to evaluate whether symptoms of sleep apnea resolved after thyroidectomy by using a validated questionnaire.
The Berlin questionnaire, a validated sleep apnea assessment tool, was provided to patients at a single academic institution before and after thyroidectomy. Patients who admitted to symptoms of snoring were asked to complete the questionnaire before and 8 weeks after surgery to assess for improvement in symptoms. The questionnaire uses 3 categories of questions to determine risk of sleep apnea. Two symptom categories must be positive for a patient to be considered “high risk” for sleep apnea.
Forty-five patients completed both pre and post-op questionnaires. The average age of patients completing the questionnaire was 53±2, and 78% of patients were female. Average BMI was 33.3±1.4 kg/m2. Based on their pre-operative questionnaire score 71% of patients were considered to be high risk for obstructive sleep apnea, this decreased to 51% after surgery (p=0.002). Overall scores significantly improved after surgery (mean 2.0 vs. 1.6, p<0.0001). Specifically, patients noted a significant decrease in snoring frequency after surgery (p=0.002), as well as a significant decrease in whether or not their snoring bothered others (p=0.004). The frequency of nodding off during the day also significantly decreased after surgery (p=0.02).
Thyroid surgery appears to significantly improve symptoms of snoring in patients who screened positive for symptoms prior to surgery. Evaluation of patients with obstructive sleep apnea should include evaluation of goiter, as symptoms of sleep apnea may improve with thyroidectomy.
CICS-UBI - Health Sciences Research Centre, Faculty of Health Sciences, University Beira Interior, Portugal, Covilha, Portugal
Thyroid Nodules and Goiter Friday Poster Clinical
The prevalence and pathology patern of iodine deficiency disorders (IDD) are related to dietary iodine intake. Two bilion people worldwide are iodine deficient (ID). Iodine is essential for thyroid hormones production. They regulate metabolic processes in most cells and are important in the development of most organs, particularly the brain. ID leads to sustained increased production of TSH and development of microscopic and macroscopic heterogeneity. ID:increased incidence of thyroid cancer and rise in the ratio of follicular to papillary neoplasia occurs. Mandatory iodization of table salt leads to a decrease in goitres and eradicates IDD. Public education as to adverse effects of ID is needed. Limited data available, shows the whole of Portugal is ID, particularly areas of the interior. Fine needle biopsy (FNB), aspiration or non-aspiration methods is the investigation of choice for thyroid nodules.
Aim of study: relative incidence of different types of thyroid nodular pathology in the most ID area: Beira Interior (BI); population, 232,000 inhabitants (2001 Census). All thyroid cytology and histology reports relating to 6 years from the major referral Hospitals for the study area of BI (MRHBI) were obtained. Aiming at being epidemiologically thorough gathering all clinically manifest patients with thyroid nodular disease in BI, MRHBI data was complemented with equivalent data, Nationally from the 3 existing Portuguese Oncology Institutes. Total of 869 patients evaluated: 607 of them having had FNB (cytology reports) and 278 had histology reports.
From the 869 patients that had thyroid nodular disease 143 had thyroid neoplasms (TNeo). From the 143 patients with TNeo 34 patients had papillary carcinoma and 100 follicular neoplasms. In the 143 TNeo were 4 medullary carcinomas, 4 anaplastic carcinomas and 1 metastatic carcinoma. •Portugal is iodine deficient. •6 year study period: incidence of thyroid nodular disease in the study area of Beira Interior, was 3.75 per 1,000 population. •The incidence of thyroid neoplasms was 0.62 per 1,000. •The follicular neoplasms to papillary carcinoma ratio, in the study period, was 100/34. •Mandatory iodine suplementation should be implemented in Portugal.
Surveillance and Intervention Post Hemi-Thyroidectomy: A Single Surgeon's Experience in a North American Academic Institution
Thyroid Nodules and Goiter Friday Poster Clinical
After a hemi-thyroidectomy, many patients require ongoing care. This study sought to quantify the rates of surveillance and intervention after thyroid lobectomy.
One hundred and seventeen consecutive patients from the time period of January 2008 through June 2011, who underwent a hemi-thyroidectomy by a single surgeon for nodular disease, were evaluated. Clinical and follow-up data were obtained by a review of patient charts.
Seventeen (14.5%) patients required completion thyroidectomy of which fifteen (88.2%) patients had thyroid carcinoma. Of the remaining one hundred patients, seventeen required thyroid hormone replacement. Twenty-three patients had lymphocytic thyroiditis on surgical specimen of which seven (30.4%) patients required thyroid hormone replacement. Thyroiditis, preoperative TSH levels and presence of contralateral nodules didn't predict postoperative need for hormone replacement. Of the 100 patients who did not undergo additional completion thyroidectomy, seven (7%) patients underwent postoperative fine-needle aspiration biopsy of the contralateral lobe, and sixteen (16%) patients were followed with ultrasound surveillance. There was one instances of recurrent laryngeal nerve injury in a cancer patient (0.85%).
After thyroid lobectomy, most patients did not require continued surveillance and intervention. With a <1% complication rate, partial thyroidectomy is an effective and efficient option for the management of nodular thyroid disease.
Radiology, Asan medical center, Seoul, Republic of Korea
Thyroid Nodules and Goiter Friday Poster Clinical
Although ethanol ablation (EA) is effective in treatment of benign thyroid nodules, there have been few studies for analyzing factors related to treatment efficacy. The purpose of this study is to evaluate the efficacy of EA and the factors affecting treatment efficacy.
A total of 217 benign cystic and predominantly cystic thyroid nodules in 209 patients underwent EA between October 2008 and December 2010. After nearly complete aspiration of internal fluid, ethanol was injected about 50% of aspirated volume through 14∼18 gauge needle. Injected ethanol was retained less than 10 minutes and evacuated completely. Follow-up ultrasound was 1, 6, and 12 months or later. The nodule volume, solidity, vascularity, symptomatic and cosmetic score were evaluated before and after EA. The correlation between the volume reduction and several factors (initial volume, solidity, vascularity, fluid nature, ethanol retention time, number of sessions) were evaluated.
The mean nodule volume decreased from 15.7±18.1 ml (mean±SD) to 3.0±7.9 ml and mean volume reduction was 85.2±16.1% at last follow-up (mean follow-up periods, 6±5.6 months). The mean symptom and cosmetic scores were improved from 2.9±2.6 to 0.6±1.0 and from 3.8±0.5 to 1.7±1.0, respectively. Cystic nodule showed greater volume reduction than that of predominantly cystic nodule (89.7±12.4% vs. 78.7±18.5%, P<.001). Linear regression analysis demonstrated that the amount of solid component (P<.001), vascularity (P=.010), the number of session (P=.028) were significantly associated with volume reduction at last follow-up. In cystic nodule, vascularity (P=.006) and the number of session (P=.008) were significantly associated with volume reduction. In predominantly cystic nodule, no factor was significantly associated with volume reduction.
EA is effective in treating both cystic and predominantly cystic thyroid nodules; however EA is more effective in cystic nodules. Amount of solid component, nodule vascularity and number of session are significantly associated with volume reduction of EA.
Saturday, October 29, 2011
Nuclear Medicine, University Hospital, Münster, Germany
Thyroid Cancer Saturday Oral Clinical 1:45 PM
To evaluate the clinical significance of 18F-FDG-PET/CT in the follow up of patients with differentiated thyroid carcinoma and to compare the results with those of 18F-FDG-PET and 131I-whole-body scintigraphy (WBS). In addition, it was the aim to investigate the impact of 18F-FDG-PET/CT on the therapeutic management.
141 18F-FDG-PET/CT studies were analyzed retrospectively: there were 101 papillary and 40 follicular tumours (93 female, 48 male). Mean age was 54±19 years. Distribution of tumour extent was: pT1 16% (n=23), pT2 19% (n=27), pT3 42% (n=59), pT4 17% (n=24) and pTx 6% (n=8); there were 24 low-risk (17%) and 117 high-risk (83%) cases. In addition, an overall clinical evaluation was performed for each case, including cytology, histology, thyroglobulin level, ultrasound, WBS, and subsequent clinical course in order to compare the molecular imaging results. Finally, the change in therapeutic management due to findings of 18F-FDG-PET/CT was investigated.
Sensitivity of 18F-FDG-PET/CT was 88% for the whole group (n=141) and 97% for the group with a negative WBS (n=91). Specificity was 88% in the whole group. Sensitivity and specificity of 18F-FDG-PET alone was 82% and 88%, respectively. The corresponding values of WBS were 63% and 97%, respectively. When 18F-FDG-PET and WBS were considered in combination, tumour tissue was missed in 2%; when 18F-FDG-PET/CT and WBS were combined, tumour tissue was missed in only 1%. 18F-FDG-PET/CT resulted in management change based on these findings in 14% with a change in surgical approach in 7%.
We conclude that 18F-FDG-PET/CT is an accurate method in the follow-up of patients with thyroid cancer and has an added value compared to 18F-FDG-PET alone. 18F-FDG-PET/CT has a direct impact on the therapeutic management of patients with suspected local recurrence or metastases, particularly in those with elevated thyroglobulin values and/or negative WBS.
Literature: 1. Grünwald F et al. Fluorine-18 fluorodeoxyglucose positron emission tomography in thyroid cancer: results of a multicentre study. Eur J Nucl Med 1999;26:1547–1552.
Laboratory of Cancer Molecular Genetics, University of Campinas, Campinas, Brazil
Thyroid Cancer Saturday Oral Clinical 2:00 PM
Regulatory T cells (Tregs), commonly identified as FoxP3+ T lymphocytes (FoxP3), are engaged on the resolution of immune response and may also block antitumor immune responses favoring tumor development and influencing the course of disease. However, likewise Chronic Lymphocytic Thyroiditis (CLT), FOXP3+ role on differentiated thyroid cancer (DTC) patients' outcome is still a matter of debate.
We studied 266 DTC patients managed according to a standard protocol and followed-up for 43.50±33.29 months. According to their serum Tg levels and image exams, patients were classified as no evidence-of-disease (NED=216 cases) or persistence of disease/recurrence (REC=50 cases including 10 deaths). FoxP3+ presence was determined by immunhistochemistry. Chronic lymphocytic thyroiditis was investigated in non-malignant thyroid parenchyma of contralateral lobe and was characterized by extensive lymphocytic infiltration with lymphoid follicles, scarring and follicular regenerative activity in the form of numerous small follicles, frequently lined by Hurthle cells.
Treg lymphocytic infiltration was associated to the presence of CLT (p=0.0002) and was more frequent in smaller tumors (p=0.0078), cases with no extrathyroidal invasion (p=0.0122) and in patients evolving with NED (p=0.0453). CLT was found in 31.57% of the DTC cases and was more frequent in smaller tumors (p=0.0110), cases with no extrathyroidal invasion (p=0.0028), no metastasis at diagnosis (p=0.0026) and in patients with NED (p<0.0001). A multivariate regression analysis confirmed CLT association to NED (p=0.016). In addition, a log-rank test confirmed that the absence of CLT was associated to recurrences (p=0.00149).
In conclusion, our results indicate that Treg lymphocytic infiltration, together with concurrent CLT, may exert a protective role on DTC patient's outcome. Since an appropriated initial management is the most important modifiable prognostic factor, characterizing the immune response profile may help identify DTC patients at higher risk for an unfavorable outcome who would, therefore, benefit from more aggressive therapeutic strategies.
University of Colorado—Anschutz Medical Campus, Aurora, CO
Thyroid Cancer Saturday Oral Clinical 2:15 PM
Novel therapies are needed for poorly differentiated, radioiodine (RAI) resistant thyroid cancer. The retinoid X receptor (RXR) has been identified as a therapeutic target for redifferentiation and direct tumor suppression. The RXR selective agonist bexarotene (Targretin, Eisai, Inc.) is approved for the treatment of cutaneous T-cell lymphoma and has been studied in two thyroid cancer trials with the short-term goal of enhancing radioiodine (RAI) uptake in metastases. We conducted a one-year clinical trial to determine if bexarotene could directly decrease tumor growth or enhance RAI uptake.
Patients with FDG-PET positive and/or progressing RAI resistant, metastatic thyroid cancer with RECIST measurable disease were recruited. Bexarotene was initiated at 300mg/m2. Patients were monitored for tumor response with thyroglobulin, PET-CT fusion scan, neck US, other cross-sectional imaging and rhTSH stimulated 123I WBS at six months or more frequently if clinically indicated. Thyroid function tests, lipid panels and hematology profiles were also evaluated.
Seventeen patients were consented for the study. All patients had a history of a total thyroidectomy ± neck dissection and had received at least one therapeutic dose of 131I. Six had also received XRT and/or sorafenib therapy and two had received chemotherapy prior to enrolling in the trial. Two of 10 patients (20%) completed the full year of therapy and both had stable disease (SD). Four of 10 patients (40%) were removed from the study due to progressive disease (average time to progression was 3.5 months). All patients symptomatically tolerated bexarotene, but 40% of patients stopped drug due to grade 2 or 3 toxicity (3 hyperlipidemia and 1 neutropenia). Of the patients that were treated for at least 6 months, none had increased RAI on WBS or decreased Tg.
Bexarotene therapy resulted in SD in 20% of patients. No appreciable increase in radioiodine uptake was demonstrated up to a year on therapy. Analysis of primary tumor RXR and PPARγ receptors is ongoing to correlate patient response or resistance to bexarotene.
An Accurate Serum Thyroglobulin Assay By Liquid Chromatography Tandem Mass Spectrometry in the Presence of Autoantibodies
Thyroid Cancer Saturday Oral Basic 2:30 PM
Thyroglobulin (Tg) is a 660 kDa homodimer of a secretary glycoprotein produced in the thyroid gland. Tg blood levels are used as a tumor marker for differentiated thyroid carcinoma (DTC). Diverse methods have been developed for quantitation of Tg however, they are subject to interference due to Tg auto antibodies (Ab). This interference is particularly troubling since up to 20% of thyroid cancer patients have Tg autoantibodies.
Serum samples were first reduced, alkylated and digested by trypsin. A specific Tg peptide was purified, enriched and loaded onto an LC-MSMS system. Analysis used MRM transitions coupled with a stable labeled internal standard.
578 patient samples were analyzed. Calibration curves were created by adding Tg standard to sera containing Tg<0.2 ng/mL (Immulite, DPC) and undetectable Tg auto antibody (Tgab<20 IU/mL, Immulite, DPC). Samples were tested on two FDA approved ICMA assays and two LDT RIA assays. Results showed good correlation between our LC-MSMS assay vs. the ICMA assays (n=343, R2=0.95, b=1.03) for Tg Ab negative serum samples but poor (n=235, R2=0.42, b=2) for Tg Ab positive (TgAb>20 IU/mL) sera. Our LC-MSMS method gave higher Tg values compared to the ICMA methods for patient sera in Tg Ab positive patients, as expected. A comparison of the LC-MSMS assay with the two RIA assays showed good correlation in Ab negative patients (n=343, R2=0.91, b=1.1) but poor for Ab positive patients (n=235, R2=0.28, b=0.36). The LC-MS/MS assay gave lower values compared to the RIA values. To validate our assay was recovering Tg accurately from Ab positive sera, recovery studies were undertaken. A high level Tg patient serum sample was spiked into 16 Ab positive patient sera and three control Tg Ab negative patient sera. Tg levels measured by LC-MSMS in Ab positive sera gave an average recovery of 96.2% and the controls gave an average of 98.3%. These results indicate the Tg LC-MSMS method accurately recovers Tg in the presence of auto-antibodies in patients sera.
Results from this study show our LC-MSMS assay to be equivalent to two FDA approved ICMA assays and two LDT RIAs for Ab negative patients while displaying superior accuracy to these tests for Ab positive patients.
Medicine, Mayo Clinic, Rochester, MN
Thyroid Cancer Saturday Oral Clinical 2:45 PM
Anaplastic thyroid carcinoma (ATC) is the most aggressive form of thyroid cancer, accounting for ∼2% of all thyroid cancers, with a mean life expectancy of 2–7 months from time of diagnosis. ATC is unresponsive to routine cancer therapies including radioactive iodide (RAI) therapy due to loss of sodium iodide symporter (NIS) gene expression. To enhance prognosis of this aggressive and fatal cancer, we have conducted preclinical studies in ATC xenografts to validate the efficacy of a novel virotherapy, MV-NIS. The vaccine strain of the oncolytic measles virus (MV-Edm) has been engineered to include the NIS gene leading to over expression of NIS, thereby also rendering these tumors susceptible to RAI therapy.
Western blotting was used to determine expression of NIS protein and CD-46 (measles virus receptor) in all ATC-derived cell lines. Xenotransplant models of two ATC-derived cell lines (BHT-101 and KTC-3) were used to test the preclinical effcacy of intratumorally injected MV-NIS. SPECT CT imaging was used to evaluate NIS expression in the xenografts after Tcm-99 injection.
Western blotting analysis confirmed that eight ATC cell lines tested do not express NIS protein, but do express CD-46. Intratumoral injection of a single dose of MV-NIS in BHT-101 and KTC-3 xenografts demonstrated a 2- and 4-fold reduction (p<0.05) in tumor volume respectively, confirming the oncolytic effect of MV-NIS. Radioactive iodine uptake in both cell lines along with the SPECT CT imaging of xenografts after Tcm-99 administration confirmed NIS expression in vitro and in vivo respectively, indicating that the combinatorial efficacy of radioiodine administration as adjunct therapy post-virus treatment may provide additional benefit.
Since current treatment for ATC is only palliative, our data indicate that targeting ATC with a dual therapeutic such as MV-NIS may prove to be a novel therapeutic strategy for effective treatment of ATC, thereby enhancing the prognosis of this disease. As MV-NIS is currently FDA approved for human clinical trials in myeloma, successful demonstration of pre-clinical efficacy of this virus in the ATC-derived xenograft model has provided the fillip to expedite its testing in clinical trials of this cancer.
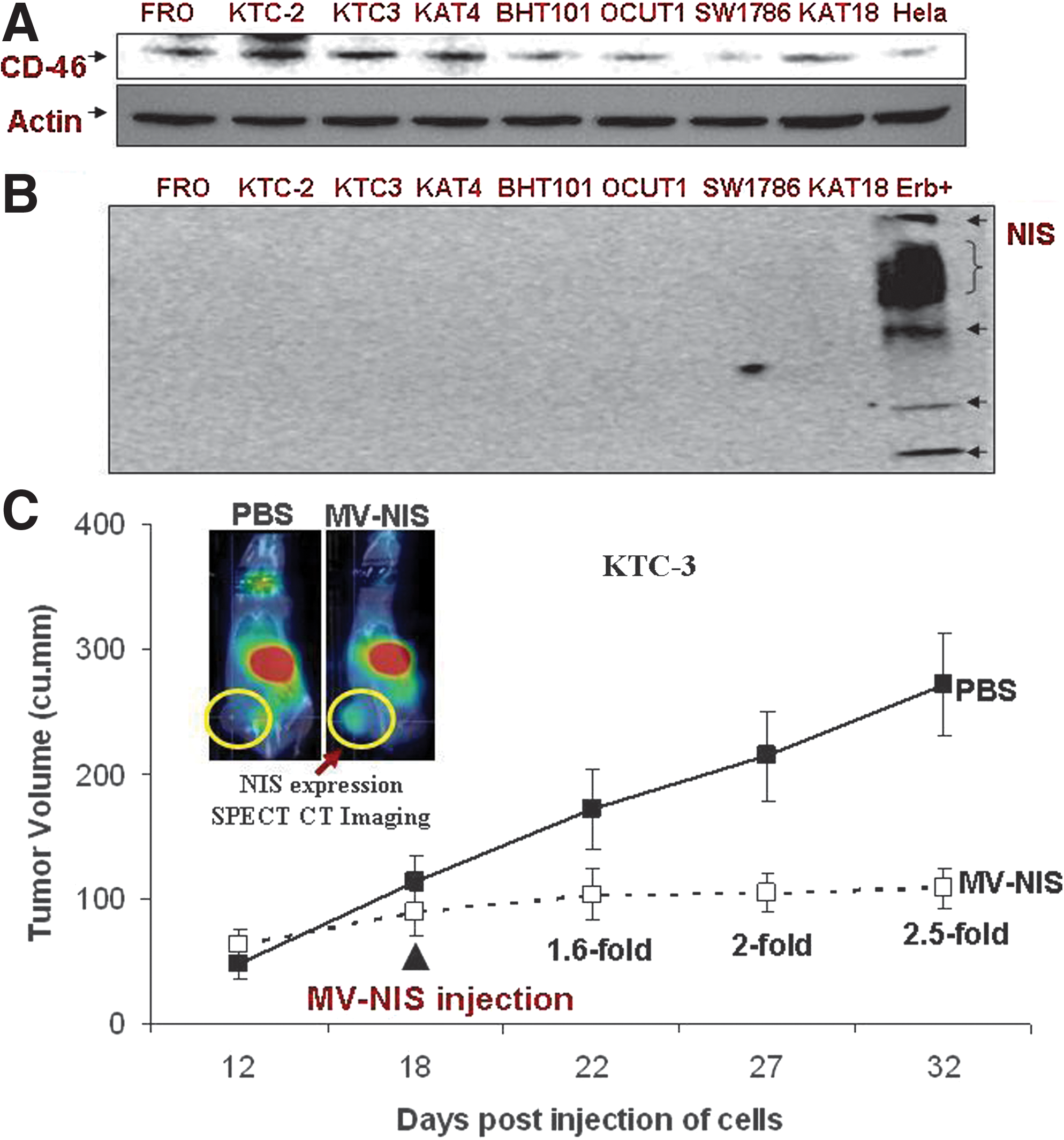
Department of Endocrine Neoplasia and Hormonal Disorders, MD Anderson Cancer Center, Houston, TX
Thyroid Cancer Saturday Oral Clinical 3:00 PM
Cabozantinib is an oral, potent inhibitor of MET, RET, and VEGFR2 that is currently undergoing clinical efficacy evaluation in several oncology indications. Differentiated thyroid cancer (DTC) and renal cell carcinoma (RCC) were chosen for evaluation in this study based on involvement of the MET, RET, and VEGFR signaling pathways. A Phase 1 study was conducted in DTC and RCC pts to determine the effect of cabozantinib on single dose pharmacokinetics (PK) of the CYP2C8 substrate rosiglitazone. The exploratory objectives included assessment of anti-tumor activity of cabozantinib of which data from DTC pts are reported.
DTC or RCC pts with metastatic disease were enrolled to this study. On study Day 1, pts receive a 4 mg tablet of rosiglitazone; PK sampling is completed on Day 2. On Days 2 (post PK sampling) through 21, cabozantinib is administered daily at a starting dose of 175 mg. On study Day 22 pts receive rosiglitazone 4 mg tablet and complete PK assessments. On study Day 57 and every 8 weeks thereafter subjects undergo tumor assessments by RECIST v1.0.
To date, 31 pts (8 DTC; 23 RCC) have been enrolled. All pts had measurable disease. Median number of prior regimens was 2 (6/8 DTC pts had at least 1 prior VEGF pathway inhibitor). Most common related AEs Grade 3 and 4 severity in all pts were: hypophosphatemia (5 pts), proteinuria and lipase increased (2 pts). There were no Grade 5 events reported. Cabozantinib plasma Tmax, Cmax, and AUC0–24h values for 16 pts who completed the PK portion were consistent with that observed in other studies. Preliminary data suggest no drug-drug interactions between cabozantinib and rosiglitazone (CYP2C8 substrate). Overall, of 7 efficacy evaluable DTC pts, 5 (71%) had a partial response (1 confirmed, 4 await confirmation); all pts experienced tumor regression (5–43%) associated with thyroglobulin decrease.
In pts with DTC, cabozantinib treatment resulted in substantial anti-tumor activity and was well-tolerated in this population.
Insight into TSH Receptor Structure and Function from Mutation of Amino Acid Residues at the Junction of the TSH Receptor Leucine-Rich Repeat Domain and the Hinge Region
Autoimmunity Saturday Oral Basic 1:45 PM
The TSH receptor (TSHR) extracellular domain comprises a leucine-rich domain (LRD) linked by a hinge region to the transmembrane domain (TMD). TSH binds primarily to the LRD but also contacts the hinge region. The LRD and TMD structures are known or deduced by crystallization or modeling, respectively. This information is insufficient to understand the mechanism by which ligand activates the TSH-holoreceptor. Such insight requires information on the structure of the hinge region (presently unknown), and the steric relationship between the individual TSH-holoreceptor components (LRD-hinge-TMD). We previously observed that mutation of a residue near the LRD-hinge junction (E251K) partially uncoupled TSH binding and receptor activation.
Because a single residue cannot stabilize the LRD-hinge complex, other residues besides E251 must also be involved. To identify such residues we selected for mutagenesis four additional potential LRD-hinge interface residues based on the TSHR LRD crystal structure. Mutant TSHR were stably expressed in CHO cells.
Individual mutation to alanine (small, neutral side chain unlike K) of residues K244, E247, K250, E251 and R255 did not alter TSH binding or TSHR activation. However, cumulative mutations of pairs, triplets, then four and all five residues progressively reduced TSHR activation without affecting TSH binding. Therefore, some of these LRD-hinge interface residues, in addition to E251, appear to contribute to the LRD-hinge interface and may be involved in signal transmission via the TMD. Unexpectedly, monoclonal antibody CS-17, a TSHR inverse agonist whose epitope straddles the LRD-hinge, was found to interact with residues K244 and E247, indicating their position at the surface of the LRD-hinge complex.
From the crystal structure of the TSHR LRD, accessibility of K244 and E247 to CS-17, together with prior information on the CS-17 epitope, provides insight into the position of the LRD relative to the hinge, as well into the mechanism by which ligands activate the TSHR or suppress its constitutive activity.
R & D, Diagnostic Hybrids, Athens, OH
Autoimmunity Saturday Oral Basic 2:00 PM
We aimed to compare the detection sensitivity of the thyroid-blocking immunoglobulin (TBI) assay with two engineered cell lines, an hTSHR wild-type (wt) and a chimeric TSHR expressing cell line (CHO-MC4) used for detection of thyroid-stimulating immunoglobulin.
Both cell lines were induced with bovine TSH (bTSH) with or without thyroid blocking MAb (K1–70, RSR Cardiff, UK) or serum containing TBI. Luciferase expression levels were measured 3 hours after induction. Blocking activity was defined as percent inhibition of luciferase expression relative to bTSH alone. Chromosomal DNA and total RNA were isolated from both cell lines and quantitative DNA rtPCR and RT-rtPCR were performed. The gene copy numbers and RNA expression levels of the TSHR genes of each cell were measured. Total protein was also isolated from both cell lines and Western blot was performed to measure TSHR levels.
The inhibitory concentration 50% (IC50) of K1–70 was 7-fold lower on CHO-MC4 (IC50 2.24 vs 17.12 ng/ml). This increased sensitivity was also seen when stimulatory MAb M-22 was used in place of bTSH (IC50 0.9 vs. 7.4 ng/ml). A TBI-positive serum from a patient with Hashimoto's displayed 3–4-fold more potent inhibitory activity when tested with the CHO-MC4 cell line compared to the wt cell line (95% vs. 30%). Also, the CHO-MC4 TBI bioassay uniformly displayed sigmoidal dose-response curves with serially diluted blocking sera. The wt TSHR-expressing cell line responded to concentrations of bTSH between 0.8 and 50 mIU/L, whereas the chimeric TSHR-expressing cell line had a wider dynamic range (1.6 to 200 mIU/L) and was induced to 8-fold higher levels. Gene copy number, TSHR RNA expression and TSHR levels were measured and did not fully explain the functional differences between the two cell lines.
The chimeric TSHR expressing cell line performs better than TSHR wt cell for detecting thyroid blocking antibodies.
Thyroid Research Unit, James J. Peters VA Medical Center, New York, NY
Autoimmunity Saturday Oral Basic 2:15 PM
Successful crystallization of TSHR residues 21–260 (including the 10 leucine rich domains—LRDs), has been reported in complex with the Fab fragment of a human monoclonal stimulating antibody to the TSHR (M22) (Sanders et al, Thyroid 2007, 17:395). However, important extracellular regions are missing from this partial crystal structure including the hinge region which is involved in hormone binding, signal transduction and signal amplification. The aim of the present study was to determine if stimulating TSHR-Abs have non-LRD binding pockets and to compare the conformational epitopes of TSHR antibodies reported from the X-ray diffractions of the truncated ectodomain with those obtained from a study of the entire ectodomain (residues 1–412) of the human TSHR using the method of epitope protection.
In this approach, we first protected the highly purified TSHR fragment with TSHR antibody prior to digestion with trypsin and the protected peptides were then delineated by mass spectrometry.
Fourteen out of 23 M22-Fab crystal contact residues were protected by bivalent M22 which may reflect the higher binding energies of certain residues. Comparing the protected epitopes of M22 with that of MS-1, a hamster monoclonal stimulating antibody (Ando et al, J. Clin. Invest. 2002, 110:1667), revealed both similarities and differences. For MS-1 there were 5 major individual linear peptides protected spanning the TSHR-ECD; LRDs 2, 5, 8, 9 & 10 for MS-1, whereas for M22 there were 5 peptides spanning LRDs 1, 2, 3, 4 & 7 protected. However, both antibodies also contacted a region on the amino terminal of the TSHR following the signal peptide encompassing cysteine box 1 of the TSHR which has been shown to be important for TSH binding and activation. In addition, the two stimulating antibodies also revealed a protected epitope in the hinge region (residues 263–293) which encompasses a highly conserved motif (SHCCAF) previously implicated in activation of the receptor.
These data demonstrate that stimulating TSHR-Abs bind to residues not confined to the LRDs but also incorporate additional epitopes likely to contribute to their functional heterogeneity. (Supported by DK080459, DK052464, and DK069713 to TFD).
Medical Clinics, UNICAMP, Campinas, Brazil
Autoimmunity Saturday Oral Clinical 2:30 PM
Genes involved in the cell cycle and apoptosis; in the metabolism of toxicants from the environment or from our own metabolic processes may explain the relationship between Graves' disease (GD) and the environment and may account for patients phenotypic and evolution diversity. Enzymes acting in the detoxification and elimination of estrogens and their metabolites are necessary to prevent excessive exposure. TP53 participates in cell-cycle arrest and apoptosis. Apoptosis normally regulates the maturation and control of both T- and B-cells immune responses, the basic pathogenic components of autoimmune thyroid disease, via removing autoreactive or nonreactive immune elements.
In order to determine the role of polymorphisms in genes involved in steroid biosynthesis and metabolism and in genes of cell cycle in GD, we studied 204 Dutch GD patients and 142 controls from the same population. TP53, COMT, HSD17B-1, GSTP1, SULT1E1, CYP1A1m1, CYP1A2*F, CYP17A1, CYP1B1 genotyping were performed by TaqMan SNP Genotyping.
A multivariate analysis demonstrated that the inheritance of a TP53GC genotype increased the risk for GD (OR=1.89; 95%IC=1.10–3.25; p=0.0181), whereas TP53GG decreased by half the risk to develop GD (OR=0.52; 95%IC=0.32–0.84; p=0.0068). Individuals who inherited a TP53C allele almost doubled their risk to develop GD (OR=1.94; 95%IC=1.19–3.16; p=0.0068).
Concerning SNPs related to estrogen metabolism, the genetic profile was similar in GD and in the controls. However, CYP17GG genotype decreased the risk of GD (OR=0.42; 95%IC=0.23–0.76; p=0.0034). The CYP17A1 protein catalyzes the formation of the precursor dehydroepiandrosterone(DHEA), which is further converted into estrogens or androgen via a series of subsequent tissue-specific pathways. There was no correlation between the investigated SNPs with smoking habits, BMI, presence of ophthalmopathy or any other patients' clinical features.
Our data indicate a protective role for CYP17GG genotype while the inheritance of a TP53C allele increases the risk to develop GD suggesting that an interaction of multiple environmental and endocrine factors might contribute to the pathogenesis of GD and may represent epigenetic modifiers in genetically-susceptible individuals.
Endocrinology, Walter Reed National Military Medical Center, Bethesda, MD
Autoimmunity Saturday Oral Clinical 2:45 PM
Two decades have passed since ATA members were surveyed on management practices for GD. An increased awareness of ocular effects of 131-I, adverse consequences of antithyroid drugs (ATDs), and consequences of thyroid dysfunction in pregnancy has emerged.
Members of the American Thyroid Association (ATA), the Endocrine Society (TES), and the American Association of Clinical Endocrinologists (AACE) were asked to take a web-based survey consisting of 32 questions dealing with testing, treatment preference, and modulating factors.
728 respondents completed the survey, including 641 members of TES, 330 AACE members, and 157 ATA members. US respondents accounted for 59%, European 12.9%, Latin American 11.3%, Asian 9.5%, Canadian 4%, Middle Eastern 3.4%. Regarding the principal mode of therapy in the index case of uncomplicated GD, 54% favored a prolonged course of ATDs, 45.2% 131-I, and <1% surgery. Regional differences persist, but compared to 1991, fewer US (59% vs 69%) and Europeans (14% vs 25%) and a higher %Asian respondents (26% vs 10%) would utilize 131-I as primary therapy. ATD preparation for 131-I was used routinely by 38%, and selectively by 50%. Methimazole (MMI) 83.6% and carbimazole 13.6%, were favored over propylthiouracil (PTU) 2.7%. Monitoring of liver function and CBC was performed by 60% of respondents. Patients with Graves' ophthalmopathy (GO) were treated with ATDs (63%) or surgery (18.4%) and less frequently with 131-I plus corticosteroids (17%) or 131-I alone (1.9%). Women planning pregnancy were treated with ATDs (50%) or 131-I (30%). PTU was favored pre-pregnancy (54.5%) and most (75%) using MMI would switch to PTU when pregnancy occurred; only 46% would switch back to MMI in the 2nd trimester.
1. The updated survey shows striking changes in clinical practice over the past 2 decades, reflecting a lower usage of radioiodine and a higher usage of ATD as primary therapy. 2. Thyroidectomy is rarely selected as primary therapy for uncomplicated GD but is used in 18% of patients with GO, 20% of women desiring pregnancy, and 38% of patients experiencing adverse effects from ATDs. 3. The use of 131-I, even with concurrent corticosteroids, is generally avoided in patients with active GO.
Thyroid Research Unit, James J. Peters VA Medical Center, New York, NY
Autoimmunity Saturday Oral Basic 3:00 PM
Many studies have suggested the complex nature of Graves' disease (GD) with multiple genes and environmental factors interacting to generate the clinical phenotype. Our previous linkage and association studies have identified a multiplicity of genes, each contributing a small proportion of genetic susceptibility to autoimmune thyroid disease. However, to date, no genome-wide association study (GWAS) of patients with GD has been published. Only one 14.5k non-synonymous coding SNPs study on a genome-wide scale has been reported in a clinically diverse population of GD patients and revealed no new confirmed genes (Newby et al, Eur J Hum Genet. 2010, 18:1021). Indeed, controversy has arisen over studies of the genetics of Graves' disease because of the inclusion of phenotypically diverse patients in the studies.
To this end we have performed an initial GWAS employing ∼100K SNPs from Illumina CytoSNP-12 for which we had a sample of 1200 separately genotyped control individuals available. These were compared to 200 clinically homogenous GD patients restricted to those with clinically apparent Graves' Orbitopathy (Werner class IIIa or higher).
As expected SNPs covering the HLA-DR/DQ region showed genome-wide significant association with GD (p=1.34×10−9). In addition, weaker associations were seen for several SNPs near genes that have been previously implicated in GD (including CTLA4, PTPN22 and the TSH receptor). A putatively novel SNP association (P=4.5×10−5) for GD was found on chromosome 5q35; close to a region that has previously been implicated in GD by linkage and association studies. The gene that is closest to the most associated SNPs from this region is predominantly expressed in thyroid and adipose tissue and replication testing is under way.
These early results demonstrate that important additional genes for Graves' disease susceptibility remain to be discovered especially in clinical subsets of the disease. (Supported by DK080459, DK052464 and DK069713 to TFD)
Pediatric Endocrinology and Metabolism, Mayo Clinic, Rochester, MN
Autoimmunity Saturday Poster Basic
Graves' ophthalmopathy (GO) is an autoimmune disorder of the orbital adipose tissue and extraocular muscles. The volume of the orbital fat is expanded and the extraocular muscle fibers are widely separated by hydrophilic glycosaminoglycans, primarily hyaluronic acid (HA). GO is also characterized by high levels of thyrotropin receptor (TSHR) antibodies that target this receptor on orbital preadipocyte fibroblasts. Recent reports have suggested that autoantibodies directed against the insulin-like growth factor-1 receptor (IGF-1R) may also play a role in the development of GO. We have found that both M22, a human monoclonal IgG1 λ-chain stimulatory TSHR antibody and IGF-1 stimulate HA synthesis in orbital fibroblasts from patients with GO. We undertook the current study to determine whether IGF-1R blockade might decrease the effect of M22 (and IGF-1) on HA synthesis in these cells.
Orbital fibroblasts from patients with GO (n=3) were grown to confluence, seeded on 24 well plates and serum starved for 24 hr. Cultures were treated with M22 (10–100 ng/ml), IGF-1 (10 nM) or control for 48 hours in insulin-free medium. The specific mouse monoclonal IGF-1Rα blocking antibody 1H7 (5 μg/mL) was added to some of the wells for 24 hours prior to addition of M22 or IGF-1. HA was measured using an ELISA kit.
Treatment of GO orbital fibroblast cultures with M22 (50–100 ng/mL) resulted in significantly increased secretion of HA (mean 1.4 fold p=0.008 and mean 1.4 fold, p=0.001, respectively). This effect by both doses of M22 was inhibited following pretreatment for 24 hours with 1H7 (24% reduction, p=0.031 and 28% reduction, p=0.012, respectively). IGF-1(10 nM) also increased HA synthesis (mean 1.69 fold, p=0.019), an effect also inhibited by 1H7 (46% reduction, p=0.026).
These results suggest that M22 may in part target IGF-1R on GO orbital fibroblasts or that 1H7 may not be a specific blocker of IGF-1Rα. Whether these findings might reflect physical association between these two receptors on orbital fibroblasts awaits further study.
R & D, Diagnostic Hybrids, Inc., Athens, OH
Autoimmunity Saturday Poster Basic
A bioassay was developed for the detection of thyroid-blocking immunoglobulins (TBI) based on the same cell line (CHO-MC4) expressing a chimeric TSHR that was used for detection of thyroid-stimulating immunoglobulins (TSI).
To detect blocking activity CHO-MC4 cells were induced with bovine TSH (bTSH) mixed with blocking monoclonal antibody (MAb) K1–70 or stimulating MAb M22 (RSR, Cardiff, U.K.) or human sera which contained either blocking or stimulating antibodies. Blocking activity was defined as percent inhibition of luciferase expression relative to induction with bTSH alone. Sera from patients with autoimmune thyroid disease (AITD) were tested with TBI and TSI bioassays and for TSHR binding inhibitory immunoglobulin (TBII).
Luciferase expression of bTSH-stimulated CHO-MC4 cells decreased in response to K1–70 in a dose-dependent manner. Fifty euthyroid controls demonstrated inhibition between 7 to 52% establishing a 95th percentile cut-off of 50% inhibition. Six TBII-positive/TSI-negative sera from patients with AITD reduced luciferase expression to background levels (100% inhibition). Serial dilution demonstrated titers of blocking activity in these samples up to 1:200. We also performed the TBI bioassay with M-22 and TSI-positive sera and observed luciferase expression above that seen with bTSH alone i.e. negative inhibition. The dose-response of M-22 stimulatory activity was identical in both the TSI and TBI bioassays with 50% effective concentrations (EC50) of 0.16 and 0.14 ng/ml, respectively and exhibited an excellent correlation (r=1.0). Serial dilution of TSI-positive sera tested in both assays also showed equivalent dose-response curves. When measuring TSI in 100 sera from patients with Graves' disease in both the TSI and TBI bioassays, there was a 100% positive concordance and a high correlation coefficient (r=0.91) between the two bioassays.
This novel dual TSI/TBI bioassay with CHO-MC4 cells accurately measures both stimulating and blocking TSHR auto-antibodies. It is a promising tool for monitoring anti-TSHR bioactivity during medical therapy.
Nutrition Research Division, Health Canada, Ottawa, ON, Canada
Autoimmunity Saturday Poster Basic
The aim of this study was to identify genes involved in the susceptibility to iodine-induced autoimmune thyroiditis.
Diabetes, thyroiditis-prone (BBdp) and -resistant (BBc) rats were fed either a control or a high iodine diet for 9 weeks. Subsequently, rats were killed and the incidence and severity of insulitis and thyroiditis were determined by histopathology. The expression of several thyroid genes was assessed using DNA microarrays, real-time quantitative PCR and Western blot analyses.
Excess iodine intake increased the incidence of insulitis and thyroiditis in BBdp rats. BBdp rats fed the high iodine diet that did not develop thyroiditis had higher mRNA levels of Fabp4, Cidec, perilipin, Pparγ and Slc36a2 than BBdp rats fed the control diet and BBc rats fed either the control or the high iodine diet. BBdp rats fed the high iodine diet that did develop thyroiditis had higher mRNA levels of Cidec, Icam1, Ifitm1, and Slpi than BBdp rats fed the control diet and BBc rats fed either the control or the high iodine diet. BBdp rats that did develop thyroiditis had lower mRNA levels of Fabp4, perilipin, and Slc36a2 but higher mRNA levels of Icam1, Ifitm1 and Slpi than BBdp that did not develop thyroiditis. Excess dietary iodine also increased protein levels of Fabp4, Cidec and perilipin in BBdp rats.
Differential expression of thyroid genes in BBdp versus BBc rats caused by excess dietary iodine may be implicated in autoimmune thyroiditis and insulitis pathogenesis.
The Correlation Between hsCRP and Immunologic Activity in Graves' Disease
Autoimmunity Saturday Poster Clinical
It is known that Graves' disease initiates the autoimmunologic reaction with the presence of a specific immunoglobulin G for thyrotrophin receptor and coexists with an inflammatory reaction. However, few studies have been reported on the association of high-sensitivity C-reactive protein (hsCRP) to immunologic activity in Graves' disease.
We presently investigated the relationship between hsCRP and thyroid autoantibodies in the patients with Graves' disease (n=260, age 40.5±13.3 years, women 75%). None of these subjects presented a recent history of infection or inflammatory disease and those taking drugs known to influence hsCRP were excluded.
Thyroid function was not correlated with hsCRP, but significant correlation between hsCRP levels and thyroglobulin antibody (Tg-Ab) (r=0.14, P=0.030) was observed. In euthryoid patients (n=143), Tg-Ab was also positively and significantly correlated with those of hsCRP (r=0.20, P=0.019), but thyroperoxidase antibody (TPO-Ab) was not correlated with hsCRP. Tg-Ab was significantly associated with thyroglobulin (r=-0.19, P=0.005) which is might be a result of effect of thyroid function on thyroglobulin. Of total, 79.2% of patients were positive for thyroid stimulating antibodies (TSAb) or thyrotropin-binding inhibitory immunoglobulin (TBII); 1.78–40.00 IU/L for TSAb and 9.92–80.74% for TBII, but only 8.1% had increased hsCRP level; mean 6.21±4.67 mg/L. However, neither TBII nor TSAb activity in these patients was not associated with hsCRP level.
These results indicate that Tg-Ab can demonstrate hsCRP in patients with Graves' disease and thyroid function could affect to hsCRP level indirectly. However, hsCRP levels do not necessarily correlate with immunologic activity in Graves' disease.
Medicine I, Gutenberg University Medical Center, Mainz, Germany
Autoimmunity Saturday Poster Clinical
Immunoglobulins stimulating the TSH-receptor (TSI) likely mediate the extrathyroidal manifestations of Graves' disease (GD). The clinical relevance of TSI was assessed in patients with GD and Graves' orbitopathy (GO) with or without additional acropachy/dermopathy and/or other autoimmune endocrine diseases.
TSI were assessed with a novel bioassay measuring functional immunoglobulins that bind to the TSH-receptor (TSHR) and transmit signals for cAMP-dependent activation of luciferase gene expression. The cAMP/CREB/CRE complex induces luciferase that is quantified after cell lysis. TSI levels were compared with a TSHR binding inhibitory immunoglobulin (TBII) assay.
Of 155 patients with GD and GO, 10 (7%) had acropachy and/or dermopathy and 29 (19%) had other autoimmune endocrine diseases. TSI and TBII were detected in 148 (96%) and in 119 (77%) of 155 GO patients, respectively. Positivity of TSI and TBII was concordant in 117 (80%) and discordant in 38 (20%) patients. Median levels of TSI were SRR% 507 (439–823) in patients with acropachy and/or dermopathy vs. SRR% 440 (44–815) in those without (p=0.008). Ten of 10 patients with acropachy and/or dermopathy were TSI-positive whereas 8/10 (80%) were TBII-positive. All 29 GO patients with other autoimmune endocrine diseases were TSI-positive versus 24/29 (83%) being TBII-positive. No significant differences between the groups regarding the clinical activity (CAS) and severity scores (CSS) was noted: median CAS was 3 (range: 0–7) in patients with GO only and 3.5 (2–6) in patients with acropachy and/or dermopathy. CSS was 5 (1–11) in patients with GO and 5.5 (4–12) in patients having acropachy and/or dermopathy. CAS and CSS were 3 (0–7) and 5 (1–12) in patients with GO only versus 3 (1–5) and 5 (1–9) in patients having other autoimmune diseases, respectively.
TSI-positivity in patients with GD and GO may predict the presence of other extrathyroidal manifestations or of concomitant endocrine autoimmune diseases.
The Relationship Between Serum 25-Hydroxy Vitamin D Levels and Hashimoto's Thyroiditis in Turkish People
Autoimmunity Saturday Poster Clinical
Results of recent studies indicated a significant association between decreased levels of serum vitamin-D and increased incidence of several autoimmune diseases and Hashimoto's thyroiditis (HT) is the most common autoimmune thyroid disease. We investigated the serum 25-hydroxy-vitamin-D (25-OH-D) levels of patients with Hashimoto's thyroiditis and compared to controls.
Thyroid ultrasound, anti-thyroglobulin (Anti-TG) and anti-thyroid peroxidase (Anti-TPO) tests performed to 540 euthyroid subjects. Patients who had recently been diagnosed as HT and on stable dose L-thyroxin therapy for at least 6 months considered as Group-1 (n=180). Sex, age and BMI matched 180 subjects, who had not known thyroid disease, with negative antibodies and normal ultrasound considered as control group and 180 subjects with positive antibodies and parenchymal heterogeneity considered as Group-2. Serum 25-OH-D levels compared for each gender separately.
We compared the serum Vitamin D levels of HT patients; Patients with HT on L-thyroxin replacement (Group1) were lower than the patients with non-medicated euthyroid HT (Group2) [Gr-1: 11.43±5.18, Gr-2: 13±5.92, control: 15.35±6.86 p<0.001]. Female patients with HT and on L-thyroxin replacement (Group-1, n=123) had the lowest serum 25-OH-D levels (10.3±4.5 ng/ml), followed by non-medicated euthyroid HT (Group-2, n=123) and control (n=123) female subjects as 11.4±6.4 and 13.5±4.9 ng/ml respectively (P<0.001). An inverse correlation found between 25-OH-D levels and thyroid antibodies (r=−0.335 p<0.001). There was a significant relationship between Vitamin D levels and thyroid volume (r=0.145, p<0.001).
In animal models active vitamin-D was shown to prevent autoimmune thyroiditis by down regulating the expression of HLA class-II molecules on thyrocytes, inhibiting lymphocyte proliferation and secretion of inflammatory cytokines. Our results show that serum vitamin-D level of patients with Hashimoto's thyroiditis is significantly lower than antibody negative controls, especially in women.According to these findings, vitamin-D replacement may prevent development of Hashimoto's thyroiditis or its progression to hypothyroidism.
Radiation Oncology, Cancer Hospital, Shantou Univeristy Medical College, Shantou, China
Autoimmunity Saturday Poster
Radiotherapy (RT) of nasopharyngeal carcinoma (NPC) requires the irradiation of neck lymphatics. Thyroid gland is often included in the high dose region which induces hypothyroidism after treatment. The aim of this study is to evaluate the influence of post-RT autoimmune antibody changes on radiation induced thyroid abnormalities in NPC patients.
In this longitudinal study, serum TSH, free T3 (fT3), free T4 (fT4), thyroid peroxidase antibody (Anti-TPO) and thyroglobulin antibody (Anti-TG) levels of 50 NPC patients were taken before RT and at 3, 6, 12 and 18 months post-RT. The volume of the thyroid gland was calculated by delineating the structure in the corresponding CT slices using treatment planning system. CT scan was obtained before RT and subsequent CT scans were conducted at 6, 12 and 18 months after RT. Eleven patients demonstrated sub-clinical hypothyrodism at 12 months post-RT and onwards (Hypo group) and their mean hormone and antibody levels were compared with that from the patients with normal thyroid function (Normal group).
There were 11 patients and 39 patients in the Hypo and Normal groups respectively. The mean anti-TPO levels of the Hypo group were higher than that of the Normal group. All their differences were significant except at the pre-RT interval (p=0.215). Significant decreases of the mean thyroid volume at each interval were also detected In the Hypo-group. In the Hypo-group, there was a positive correlation (r=0.51) between TSH level and Anti-TG level, whereas a negative correlation was observed between fT4 and Anti-TPO (r=−0.55). The mean Anti-TPO level for all subjects started to rise after 3 months, and the shrinkage of the gland was the greatest in the first 6 months after RT. Interestingly, more significant changes of the overall mean fT4 and TSH levels were observed between the 6 to 12 months intervals.
Radiation induced damage to thyroid gland in NPC patients, mainly hypothyroidism, was highly associated with the autoimmune response of the gland, which was indicated by the rise of Anti-TPO and Anti-TG levels.
Internal Medicine, Mayo Clinic, Rochester, MN
Autoimmunity Saturday Poster Clinical
It has been reported recently in separate publications that IgG4+ plasma cells are present in both Riedel's thyroiditis (RT) and a subset of patients with Hashimoto's thyroiditis (HT). These findings suggest a possible association of RT and HT with IgG4-related systemic disease. However, whether the degree of infiltration with IgG4+ plasma cells or the clinical association with other IgG4 related disorders is similar in both entities is unknown.
From the medical records available at Mayo Clinic Rochester we identified all cases diagnosed with RT during the period 1958–2008. We then selected all cases having sufficient surgical pathologic material for IgG4 staining. For each case of RT we selected age and gender matched HT controls (1:1 ratio) with the same requirement regarding pathology specimens. IgG4 staining was quantified as average number of positive cells/high power field (HPF) from 20 random fields, adjusted for the degree of inflammation (scale 0–3).
We identified 6 cases of RT that we matched with 6 cases of HT. RT group average age was 44.7 vs. 43.8 in the HT group, with 83% women in both groups. In areas of fibrosis the average IgG4 staining adjusted for the intensity of inflammation was 3.2 cells/HPF in RT vs. 0.97 in HT (p=0.15, CI for difference in means: −1.2 to 5.9). In areas of lymphoid cell aggregation the score was 2.07 cells/HPF in RT compared with 0.94 in HT (p=0.39, CI for difference in means: −2.0 to 4.2).Combining all areas the mean difference was 1.76 cells/HPF in favor of RT (CI: −0.2 to 3.7, p=0.08). 3/6 RT cases had an average IgG4 staining >2.2 cells/HPF compared with 0/6 for HT. There were 2/6 cases in the RT group with additional fibrotic disorders (mediastinal and retroperitoneal) and 1/6 with an IgG4-related systemic disease manifestation (orbital IgG4 disease), compared with 0/6 for both conditions in the HT group.
Both RT and HT demonstrate infiltration with IgG4 positive cells, with the process apparently more pronounced in RT. These findings can be exploited for diagnostic purposes. Our results support the purported association of RT with the IgG4-related systemic disorder and suggest that HT might represent less severe disease on the same immunopathogenic spectrum.
The Prevalence of Thyroid Peroxidase Antibody-Positive Results in a Population of Overt Hypothyroid Pregnant Saudi Women and Its Effects on Obstetrical Complications
Autoimmunity Saturday Poster Clinical
Objective: To estimate the prevalence of thyroid peroxidase antibodies (TPO-Ab) in the overt hypothyroid obstetric population and to compare pregnancy outcomes in (TPO-Ab) positive hypothyroid women with those who are (TPO-Ab) negative.
A case control study conducted in Madinah Maternity and Children Hospital and in Ohud Hospital between June 2009 and July 2010. A total of 87 newly diagnosed overt hypothyroid women who are between 12 and 32 weeks of gestation were studied. Pregnancy outcomes in group 1; hypothyroid women with positive (TPO-Ab), (more than 50 international units/mL by chemiluminescent immunoassay), were compared with group 2; hypothyroid women with negative (TPO-Ab).
Of the 87 pregnant hypothyroid women tested, 31% (27/87) were identified with positive (TPO-Ab). Women tested positive for (TPO-Ab) were older than women with negative test (p=0.005*). The presence of (TPO-Ab) was significantly associated with pregnancy induced hypertension (PIH) 22.2% ; odds ratio, OR=0.68 (95% confidence interval, CI: 0.33–1.38), caesarian section (C/S) 48.1% (13/27), OR=0.46 (95% CI: 0.23–0.94), gestational diabetes (GDM) 44.4% (12/27), OR=0.38 (95% CI: 0.21–0.67). Although the rate of abortion and preterm deliveries were also higher in the (TPO-Ab) positive group, this did not reach a statistical significance.
(TPO-Ab) was present in 31% of the hypothyroid pregnant women and the associated with obstetric complications, warranting routine thyroid peroxidase antibody screening at early pregnancy for this group of women. Further studies are needed to confirm the significance of these antibodies in the subclinical hypothyroid and Euthyroid obstetric population.
PIH: pregnancy induced hypertension, GDM: gestational diabetes, IUFD: intrauterine fetal death CS: cesarean section, NICU: neonatal intensive care unit.
Normalization of Serum TSH in Early Pregnancy Does Not Prevent Prematurity in Hypothyroid Pregnant Women
Disorders of Thyroid Function Saturday Poster
Introduction: Hypothyroid pregnant women are at risk of developing obstetrical and neonatal complications. Their children are at risk of neurological impairments. The study's aim was to assess if early TSH normalization could prevent complications.
Methods: Seventy three previously diagnosed hypothyroid women (other medical conditions excluded), on levothyroxine were followed through 85 deliveries. At the first obstetrical visit they were divided in 2 groups: Group 1: 38 hypothyroid women (43 deliveries) on inadequate replacement; they were further divided into 1a: clinically hypothyroid (15 deliveries) and 1b: subclinically hypothyroid (28 deliveries). Group 2: 35 euthyroid women (42 deliveries) on appropriate replacement. They were seen every 2–4 weeks; TSH, FT4 or FT4I, TPOAb and TRAb were determined at the first visit; TSH, FT4 or FT4I at each follow up visit. Target was TSH<2.5 in the first trimester;<3.0 thereafter. Twenty obstetrical and neonatal complications were evaluated.
Results: Initial visit (weeks) 1a: 8.0 (2–30); 1b:8 (4–29); 2: 8 (2–39). Initial TSH (μIU/L- median [range]): 1a: 18.4 (3.6–513); 1b: 5.2 (2.51–18.4); 2: 1.65 (0.09–2.43). Initial TSH in patients with complications: 1a: 12.2 (3.6–425); 1b: 5.8 (2.72–18.4); 2: 1.6 (0.09–2.43). Total complications: 1a: 60%; 1b: 71.4%; 2: 59.5%. Prematurity was the only complication significantly different between the groups: Group 1a: 3 (20%); Group 1b: 7 (25%); Group 1a+1b: 10 (23.3%); Group 2: 1 (2.4%) P value 0.0044. The serum TSH had normalized before 17 weeks in 6 out of the 10 premature deliveries (Group 1).
Conclusions: 1. (50.5%) of the 85 women on levothyroxine were hypothyroid at conception
2. Prematurity was the only complication significantly lower between euthyroid and hypothyroid groups
3. In 6 out of 10 premature deliveries the serum TSH normalized <17weeks
4. Normalizing TSH before conception might be necessary to prevent premature deliveries.
Prematurity in Hypothyroid Women Treated Early in Pregnancy
Six out of 10 hypothyroid women, serum tsh normalized before 17 weeks gestation.
Disorders of Thyroid Function Saturday Poster Clinical
Coffee (C) drunk with or a few min after L-T4 tablets (“improper habit”, IH) failed to normalize or suppress serum TSH, while C drunk with water (W) ≤30 min after having swallowed the L-T4 tablet (Tab) with W (“proper habit”, PH) normalized or suppressed TSH (Thyroid, 2008).
Because the pharmacokinetics of a new formulation of L-T4 (Tirosint® softgel capsules, Lugano, Switzerland) suggested its lower availability for quick mixing with pharmacological/nonpharmacological compounds that could diminish the intestinal absorption of L-T4, we switched to the same dose of this capsule (Cps), and for 6 months, 8 patients in whom brand L-T4 tablets ingested under an IH failed to normalize (n=1) or suppress (n=7) serum TSH. The Cps was taken with W and having C 1h later from days 1 to 90 (PH), but with C or W followed by C shortly after (IH) from days 91 to 180. Sampling for TSH was monthly.
The historical TSH (hi-TSH) had been 26–34 (IH) and 5.8–22.4 mU/L (PH) in the hypothyroid patient. Upon switch to the Cps, TSH ranged 0.06–0.16 (PH) and 0.025–0.29 (IH). In the other 7 pts, hi-TSH ranged 0.20–6.8 (median 0.84; m±SD 1.23±1.47, IH) and 0.02–1.29 (0.20; 0.28±0.20, PH). Upon switch to the Cps, TSH averaged 0.15 (median) and 0.41±0.46 (P=0.4 vs. hi-TSH 0.39±0.034) under the PH, and 0.34 (median) and 0.34±0.30 (P=0.00004 vs. hi-TSH 1.23±1.47) under the IH. Of the 21 TSH data points during days 1–90, there were 7 (33%)<0.1 mU/L, with at least one such value in 4/7 pts (57%). This contrasts with only 2/19 hi-TSH values<0.1 (10%, P=0.088) in 2/7 pts (29%, P=0.29) under the PH. Of the 21 TSH data points during days 91–180 there were also 7(33%)<0.1 with at least one such value in 3/7 pts (43%) vs. 0/18 hi-TSH values (0%, P=0.01) with at least one such values in 0/7 pts (0%, P=0.19). With the two brand L-T4 Tab TSH levels under the PH and the IH differed (0.39±0.34 vs 1.22±1.52, P=0.0001). In contrast, with the Cps TSH levels under the PH or IH did not differ (0.41±0.46 vs 0.34±0.30, P=0.95).
Tirosint® softgel capsule is C-resistant and can be used to achieve target TSH levels in pts unable/unwilling to change their IH of L-T4 ingestion. In these pts, even under the PH the new formulation ensures better absorption.
Endocrinology, Cesar Milstein Hospital, Buenos Aires, Argentina
Disorders of Thyroid Function Saturday Poster Clinical
Due to frequent alterations of thyroid function in absence of true thyroid disease, thyroid function tests (TFT) are not routinely evaluated in elderly hospitalized patients. Our aim was to describe the thyroid profile best associated with increased morbimortality (MM) in hospitalized elderly patients with indication for TFT.
All patients admitted to our institution between 2009–2010 aged 60 yr or older were included. From 2599 patients, 7% had TFT and those with complete clinical data were analyzed (n=100) and classified into euthyroidism (Eu), nonthyroidal illness (NTI), subclinical (ST) and overt thyrotoxicosis (OT) and subclinical (sh) and overt hypothyroidism (oh). This group was compared to a sub-sample of 100 in-patients without TFT from the same cohort. High MM was defined as mortality, intensive care unit (ICU) requirement and prolonged hospital stay (>15 days, 75 percentile). Long-term MM was defined with the addition of the data concerning mortality at 18 month after being dismissed.
Indications for TFT were hyponatremia (30%), cardiologic evaluation (21.6%) and history of thyroid disease (21.6%). Patients with TFT vs. those without TFT were predominantly female (70 vs. 55%, p<0.05) and were more severely ill with higher need of ICU requirement (27 vs. 7%, p<0,05), longer hospital stay [9 (5–18) vs. 3(2–8) days, p<0.05] and higher mortality rate (11 vs 5%, p>0.05). Patients with TFT were classified as 25%Eu, 61%NTI, 7%ST, 5%oh, 1%sh and 1%OT. Within these patients, those with increased MM exhibited higher TSH (2.50 (0.94–6.40) vs. 1.30(0.78–2.62) mU/l, p<0.05) and lower T4 (6.91±2.36 vs. 8.31±1.99 ug/dl, p<0.005). The decrease of T4 was the only TFT associated with higher short-term MM (OR 2.2, 95%CI 1.2–4.0, p<0.01) adjusted by age, sex, T3 and TSH concentration. However, in the same model, long-term MM was associated only with the increase in TSH concentration (OR 1.6, 95%CI 1.1–2.3, p=0.02).
Increased TSH concentration during hospitalization might be an indicator of worse prognosis among elderly patients with TFT. Future longitudinal studies are needed to confirm this finding.
Endocrinology, Baylor College of Medicine, Houston, TX
Disorders of Thyroid Function Saturday Poster Clinical
Thyroid hormone is largely bound to plasma protein. Removal of plasma reduces the amount of circulating hormone. Plasmapheresis as a treatment for thyrotoxicosis utilizes this concept. Presently there is no clear consensus on this option. We report two cases of thyroid storm successfully managed with plasmapheresis when conventional therapy with anti-thyroidal medications was not feasible.
Case #1: A 27 year old man with known diffuse toxic goiter and CHF presented in thyrotoxic crisis (Burch and Wartofsky score ∼80) months after stopping antithyroidal medications. He was tachycardic at a rate of 280 bpm and had an 80 gm diffuse goiter. Treatment for thyroid storm was initiated (methimazole, hydrocortisone, beta blockade, and potassium iodide), but due to rising transaminases (ALT of 2474 U/L and AST of 5760 U/L), methimazole was discontinued. Plasmapheresis was initiated and continued for a total of 3 treatments. TSI levels dropped from 730 to 384 %. Free thyroxine (FT4) levels declined into the reference range and the patient underwent thyroidectomy as definitive treatment.
Case #2: A 40 year old man with Grave's disease presented with new onset lower extremity edema, atrial fibrillation, and shortness of breath. Initial laboratory testing revealed severe thyrotoxicosis. Several hours after admission the patient progressed to pulseless cardiac arrest. He was successfully resuscitated, and placed on treatment for thyroid storm, but his FT4 levels continued to rise with elevations in transaminases (AST 123 U/L and ALT 177 U/L). Plasmapheresis was initiated, and TSI levels dropped from 551 to 393% within three hours, with a corresponding drop in free T4 from 10.9 to 8.5 ng/dL. He received a total of 3 treatments, and ultimately underwent thyroidectomy.
The mortality rate from thyroid storm is high (20 to 30 %). Plasmapheresis as a treatment option for thyrotoxicosis was first described in 1970, but to date there is no clear consensus on the definite success of this treatment. However, in extreme cases when traditional management is not feasible, plasmapheresis leads to amelioration of symptoms and significant decline in FT4 levels providing a window to definitively treat with thyroidectomy.
Electronic Prescribing of Brand Name Levothyroxine
Disorders of Thyroid Function Saturday Poster Clinical
Levothyroxine is a narrow therapeutic index drug. Consistent dosing is necessary to avoid potential side effects of under or overdosing, which is of particular importance in high-risk populations. To compare brands of levothyroxine, the FDA relies on bioequivalence studies in normal euthyroid individuals given supraphysiologic doses of thyroxine. Importantly, these studies do not rely on TSH measurements or clinical outcomes. In our clinic, prescriptions are almost all sent electronically (eRx). We received many calls from patients stating that their brand name levothyroxine had been substituted.
We conducted an IRB approved, prospective pilot telephone survey at a single site with the aim to study how eRx affects dispensation of brand name levothyroxine. 100 subjects who received an eRx for branded levothyroxine were enrolled. Three telephone calls over 7 months were conducted. Subjects were asked to describe the characteristics of the pill so that brand and dosage could be identified.
128 subjects were identified and 100 were enrolled in the study (79% response rate). At call 1, of the 78 subjects who had picked up a new bottle of levothyroxine since the eRx, 5 had been substituted. We also saw substitutions of new prescriptions over the 2nd and 3rd calls as well as the refill prescriptions. Over the 7-month study, 9 of the 100 subjects were substituted at some time. The average age was higher in those substituted vs. those who were not (61.2±13.2 vs. 48.5±12.4, p=0.009). Men were substituted in 4 out of 24 subjects (16.6%) vs. 5 out of 76 females (6.6%), p=0.21. Of the 156 unique prescriptions eRxd, there were 24 mail order prescriptions, none of which were substituted.
In this 7-month pilot study involving 100 subjects prescribed brand name levothyroxine, 9 were substituted. An educational bias was identified as 2 subjects reported that the pharmacy attempted to substitute their prescription but they insisted on the brand name prior to purchase. Other subjects may have had similar experiences and not have offered that information. Further work with medical boards and pharmacies is required to ensure that patients are able to obtain prescriptions as written so that consistency in dosing can be assured.
Withdrawn
Medicine, Regional Institute of Medical Sciences, Imphal, India
Disorders of Thyroid Function Saturday Poster Clinical
The association of thyroid dysfunction and maternal fetal outcome is well studied and documented around the globe. In the Indian prospective with 20 years of post iodination, thyroid function in pregnancy is not well documented. Though two studies for normative data for thyroid functions in pregnancy had been conducted in India, both the study populations were from northern part of India. Our study aims at finding the reference range of Thyroid Stimulating Hormone (TSH), Thyroxin (T4) and Triiodo-thyronine (T3) levels for normal pregnant women of north-eastern part of the Indian subcontinent where the ethnicity is different from those of the northern part of India.
A reference population is established by excluding patients with grade 1 or 2 goiter,hyperemesis gravidarum, with past or family history of thyroid disorders and connective tissue disorders or any medication altering the thyroid functions. Sample size is calculated with an absolute error of 0.5. The reference population of 246 is established after screening about 500 pregnant women. 49, 108 and 89 pregnant women are from first, second and third trimesters respectively. The reference value for thyroid hormones (TSH, T4, and T3) is established from the 5th and 95th percentile.
The mean age (in years) of the patients are 26.27,27.69 and 27.63 in first, second and third trimester respectively.The mean TSH (μIU/ml), are 2.29, 2.54 and 2.52 in the first, second and third trimesters respectively. The reference range of thyroid hormones for each trimester is shown in the table below.
Trimester Specific Thyroid Hormones Reference Range
Thus the trimester specific reference range has been established for our population.
Iodine Uptake and Metabolism Saturday Poster Basic
Iodine, an essential element for thyroid function is necessary for the normal growth, development and functioning of the brain and body. Iodine is responsible for a wide range of mental and physical disorders collectively termed as “Iodine Deficiency Disorders” (IDD). Iodine deficiency disorder is estimated to have lowered intellectual capacity of several nations by as much as 10 to 15%.
Seven different villages of Vadodara district were purposively selected. Anthropometric data of each subject was availed. Urine and saliva samples were collected. Urinary iodine excretion and Salivary Thyroglobulin estimation were estimated by Sandell Kolthoff method (Wet Digestion Method) and Radio Immuno Assay respectively.
Total of 203 (age group - 16–40 years) were enrolled for the study. The overall prevalence of IDD was 56.1 %, which comprises 45.5 % had mild, 36.3% had moderate and 17% had severe iodine deficiency. The median values for UIE was 47.57 μg/L and mean value for salivary Tg was 9.13 ng/ml. The knowledge assessment revealed low levels of awareness regarding the physiological role of Iodine in human system.
The median UIE value is very low for population and reflects endemicity in this area. There is a strong need for an effective intervention programme to eliminate iodine deficiency amongst all age groups in these areas.
Physiology, University of Benin, Benin, Nigeria
Thyroid and Development Saturday Poster Basic
Polybrominated diphenyl ethers (PBDEs) are a group of halogenated, bioaccumulative flame retardant chemicals, which have been used in a variety of consumer and household products. PBDE currently are ubiquitous environmental contaminants and have been detected in both biotic and abiotic samples. Recent studies have shown that perinatal exposure to PBDE may alter spontaneous motor activity, disrupt learning and memory. Although the molecular mechanisms of PBDE action have not yet been fully understood, studies have shown the possibilities that PBDE may act through the thyroid hormone system. 1. Transient-transfection based reporter gene assay. 2. Liquid chemiluninescent DNA pull down assay 3. mammalian two hybrid assay 4. primary cerebllar culture 5. granule cell reaggregate culture
Several low dose polybrominated diphenyl ethers (PBDSs) suppresses thyroid hormone receptor (TR)-mediated transcription via partial dissociation of TR from TR response elements (TRE), acting via DNA binding domain of TR. Also, PBDE suppresses dendritic arborization of cerebellar Purkinje cells and inpairs granule cell neurite extension.
Taken together, our results indicate that PBDE may disrupt TH homeostasis and consequently impair normal cerebellar neuronal development possibly via TR.
Nuclear Medicine, Smt Kashibai Navale Medical College and General Hospital, Pune, India
Thyroid and Development Saturday Poster Clinical
Ectopic thyroid tissue is an uncommon congenital condition. It is extremely rare to have three ectopic foci at three different sites. The thyroid scan has been used successfully to diagnose ectopic thyroid tissue. We report a case of triple ectopic thyroid in a 16 yr old female who presented with swelling in front of neck. Preoperative thyroid scan helped in establishing diagnosis of ectopic thyroid which was the only functioning thyroid tissue.Thus preventing unnecessary surgery.
A 16 year old girl presented with mid line swelling in front of neck since childhood progressively increasing in size. Clinical examination revealed a firm, non tender swelling of size 2cm × 2cm at level of hyoid in midline of neck, moving with deglutition and protrusion of tongue. USG neck was performed which suggested right paramedian neck mass measuring 26 × 16 × 13 mm probably thyroglossal cyst or solitary nodule of right lobe of throid. Thyroid function tests T3—.28 ng/ml, T4—.65 ug/dl, TSH—3.30 uIU/ml. Antibodies titre showed Microsomal (TPO) antibody levels to be positive (11.4 U/ml) and Anti Nuclear Antibodies (ANA) were negative. Tc99m Pertechnetate thyroid scan was done.
Static images showed avid tracer uptake at the base of tongue and in clinically palpable nodule at the level of hyoid and another small focus of tracer uptake on left side of mid line just above the clinically palpable nodule. Thyroid gland was not seen at its normal location. CT scan showed well defined hyperdense, enhancing soft tissue masses at three levels. First at posterior most part of tongue 10×11mm, second 17 mm×12mm above the hyoid on left side and third 15×24×26mm just below the hyoid in midline.
Preoperative thyroid scan helped in establishing diagnosis of ectopic thyroid which was the only functioning thyroid tissue.Therefore it is suggested that thyroid scan and USG/ CT scan must be done as routine work up in neck swellings pre operatively to avoid unnecessary surgeries.
Tc99m TcO4 thyroid scan.
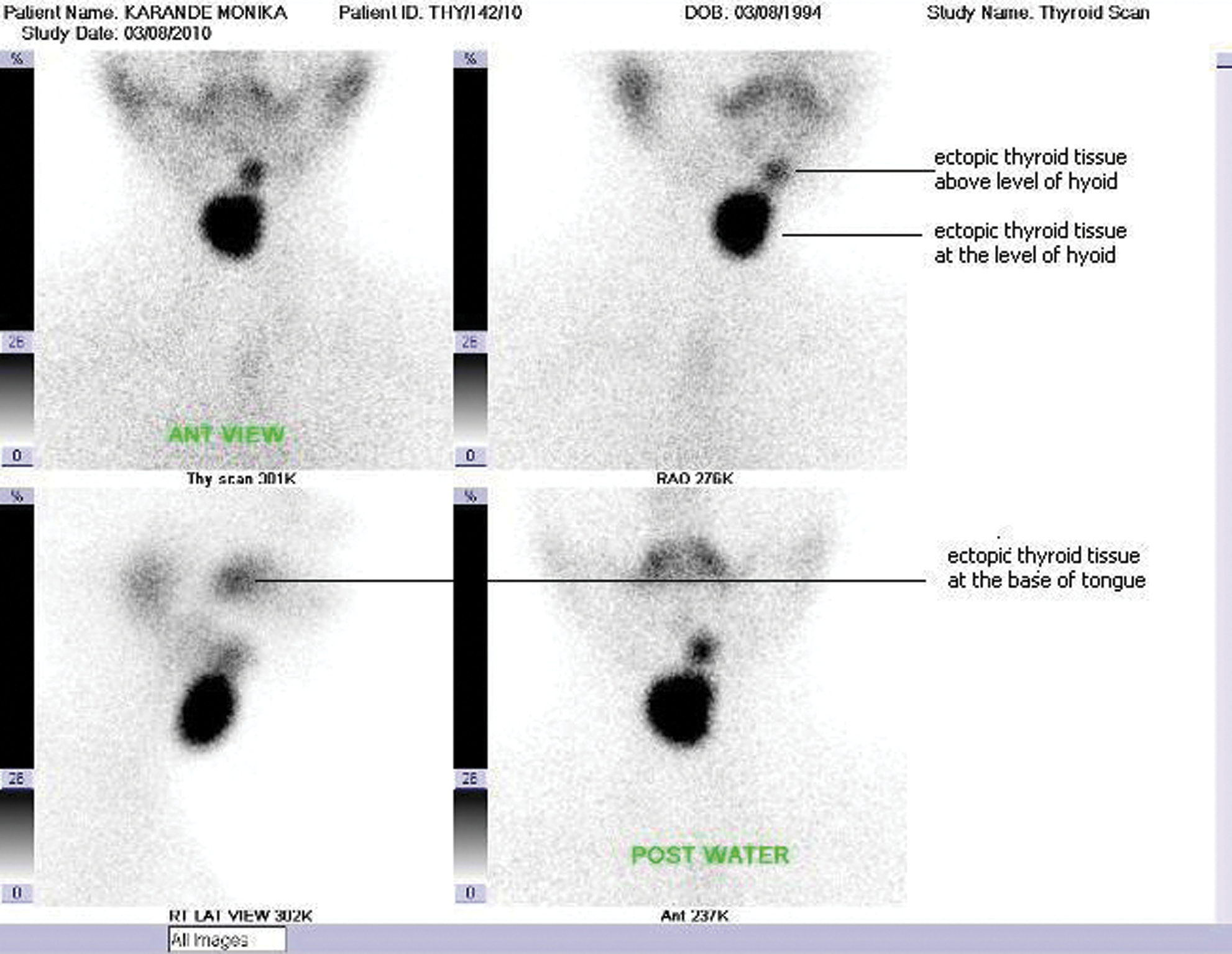
Pathology, University Health Network, Toronto, ON, Canada
Thyroid Cancer Saturday Poster Basic
Medullary thyroid carcinoma (MTC) is a rare but potentially aggressive malignant tumor of thyroid that is derived from calcitonin-secreting parafollicular C cells. The initial treatment of MTC is total thyroidectomy and elective central lymph node dissection; some experts recommend a more extensive neck clearance. Even with current treatment options, MTC is associated with a high incidence of recurrence and metastasis. Targeted therapies such as receptor tyrosine kinase inhibitors and anti-CEA antibodies have been proposed, however, patients with MTC have only moderate responses to these targeted therapies. The success of targeted treatments very much depends on the identification of novel targets proteins. In this study we aimed to identify to identify new prognostic factors and target proteins expressed in medullary thyroid carcinoma.
We constructed a tissue microarray of medullary thyroid carcinomas from 23 patients and stained the slides for 37 proteins involved in carcinogenesis, angiogenesis, inflammation and cell-to-cell contact. Protein expression was determined using computerized image analysis software (Spectrum Plus©, Aperio). Statistical analysis was carried out to correlate patients' clinical data with the protein expression profile.
Expression of COX-1/2, Bcl-2, Bmi-1 proteins and members of the SHH and WNT pathways was observed in medullary thyroid carcinomas however there was no correlation with tumor behavior or patient outcome. Univariate analysis showed that expression of EGFR correlated significantly with decreased disease-free survival (p=0.01), whereas membranous β-catenin expression was associated with improved disease-free survival. (p=0.039).
Our results demonstrate that EGFR and β-catenin may be potential prognostic markers predicting disease-free survival in patients with medullary thyroid carcinoma. We have identified several potentially important protein targets (COX-1/2, Bcl-2a, and Bmi-1) and two pathways (WNT and SHH pathways) that may be therapeutically targeted in medullary thyroid carcinoma.
Surgery, University of California San Francisco East Bay, Oakland, CA
Thyroid Cancer Saturday Poster Basic
Cancer gender disparities have been observed for a variety of human malignancies. Thyroid cancer is one such example where there is a dramatic difference in the incidence, aggressiveness, and death rate by gender. The molecular basis for cancer gender disparity is poorly understood. To address this, we performed genome-wide gene expression profiling in matched papillary thyroid cancer (PTC) samples and identified 10 candidate genes differentially expressed by gender. One of these genes was Reticulon 4 Interacting Protein (RTN4IP1) for which the function and expression is unknown. Thus, we evaluated the expression of RTN4IP1 in human thyroid tissue, and its function in thyroid cancer cell lines.
We used quantitative RT-PCR to measure mRNA expression levels of RTN4IP1 in 6 normal, 6 benign and 47 PTC. We used siRNAs to knockdown RTN4IP1 expression to evaluate its role in cancer cell phenotype (cell proliferation, invasion, migration, soft agar colony formation, tumor spheroid formation) in three authenticated thyroid cancer cell lines (TPC-1, FTC-133, XTC-1).
RTN4IP1 mRNA expression was significantly downregulated in PTC as compared to normal and benign thyroid samples (P<0.05). Lower RTN4IP1 mRNA expression was also associated with larger primary PTC size (P<0.05). RTN4IP1 knockdown significantly; 1) increased cellular proliferation (>3-fold at 7 days), 2) cell invasion (1.5-fold to 3.2-fold within 24 hours), 3) cellular migration (20% to 41% within 24 hours), 4) the number and size of colonies in soft agar (6-fold), and 5) tumor spheroid formation in multiple thyroid cancer cell lines (P<0.05).
Our data taken together suggests RTN4IP1 is downregulated in PTC and has important biologic effects on the hallmarks of cancer cell phenotype. We, therefore, propose that RTN4IP1 may be involved in thyroid cancer initiation and progression, and may explain the different tumor biology observed by gender.
Diagnostic Research and Technology Development, Asuragen, Austin, TX
Thyroid Cancer Saturday Poster Basic
MicroRNAs (miRNAs) are small non-coding RNAs that negatively regulate gene expression at the posttranscriptional level. Compelling evidence indicates that miRNAs play key roles in the development of many diseases and cancers, including thyroid cancer. Histological subtypes of thyroid cancers have distinct miRNA expression profiles. Recent studies have suggested that miRNAs may be used in preoperative FNA samples to distinguish between hyperplastic thyroid nodules and malignant thyroid tumors. The aim of this study was to further investigate miRNAs as candidate diagnostic markers for thyroid cancer. Our goal was to identify a miRNA expression signature that could be used to separate benign thyroid conditions from malignant thyroid tumors, including mutation- and translocation-negative tumors, in preoperative fine needle aspirate (FNA) specimens.
To identify candidate miRNAs, two independent sets of thyroid samples were procured that corresponded to a variety of benign and malignant conditions. The two sample sets consisted of 46 fresh frozen biopsies and 71 formalin-fixed paraffin-embedded (FFPE) samples, respectively. Total RNA was isolated from frozen samples using the mirVana miRNA Isolation Kit (Ambion) and from FFPE samples using the RecoverAll kit (Ambion). miRNA expression profiles were either established on Agilent V3 miRNA arrays, which contain probes against 866 human miRNAs from the Sanger database V12 (fresh frozen samples), or on Affymetrix GeneChip miRNA 2.0 Arrays (Affymetrix) that target 1,105 human miRNAs from the Sanger database V15 (FFPE specimens).
The samples were divided into benign and malignant groups for analysis, according to histology. The 70 most differentially expressed miRNAs identified by array analysis (p≤0.01) were selected for further analysis, using TaqMan miRNA RTqPCR assays (Applied Biosystems). Using these data, miRNA diagnostic classifiers including miR-146b, miR-221, and miR-222 along with novel miRNAs were generated that can discriminate between benign and malignant thyroid tumors in both fresh frozen and FFPE samples.
The relative performance of the top classifiers and their clinical utility are currently being evaluated using thyroid FNAs.
Radiochemotherapy of Medullary Thyroid Carcinoma via Lentivirus-Mediated Transfer of Human Sodium Iodide Symporter Gene and Herpes Simplex Virus Thymidine Kinase Gene
Thyroid Cancer Saturday Poster Basic
Herpes-simplex virus thymidine kinase (HSV-TK) gene/ganciclovir (GCV) system has been wildly used as a traditional gene therapy modality, and the sodium/iodide symporter gene (NIS) has been found to be a novel therapeutic gene. Since the therapeutic effects of radioiodine therapy or prodrug chemotherapy on cancers following NIS or HSV-TK gene transfer need to be enhanced, this study was designed to investigate the feasibility of radiochemotherapy for medullary thyroid carcinoma via co-expression of NIS gene and HSV-TK gene.
TT cells were stably transfected with NIS, TK, and GFP gene via recombinant lentiviral vector and named TT/NTG. Gene expression was examined by RT-PCR, fluorescence imaging, and iodide uptake. The therapeutic effects were assessed by MTT assay and clonogenic assay.
TT/NTG cells concentrated 125I- up to 76-fold higher than the wild-type cells within 20 minutes, and the efflux happened with a T1/2eff of less than 10 min. The iodide uptake in TT/NTG cells was specifically inhibited by sodium perchlorate. Dose-dependent toxicity to TT/NTG cells by either GCV or 131I was revealed by clonogenic assay and MTT assay, respectively. The survival rate of TT/NTG cells decreased to 49.7%±2.5%, 43.4%±2.8%, and 8.6%±1.2% after exposure to 131I, GCV, and combined therapy, respectively.
We demonstrate that radiochemotherapy of medullary thyroid carcinoma via lentiviral mediated co-expression of NIS gene and HSV-TK gene leads to stronger killing effect than single treatment, and in vivo studies are needed to verify these findings.
Internal Medicine, University of Latvia, Riga, Latvia
Thyroid Cancer Saturday Poster Basic
Currently the cytological examination of fine needle aspiration (FNA) biopsies is the standard technique for the pre-operative differential diagnosis of thyroid nodules. However, the results may be non-informative in ∼20% of cases due to an inadequate sampling and the lack of highly specific, measurable cytological criteria, therefore ancillary biomarkers that could aid in these cases are clearly needed. The aim of our study was to evaluate the mRNA expression levels of 8 candidate marker genes as the diagnostic biomarkers for the discrimination of benign and malignant thyroid nodules and to find a combination of biomarkers with the highest diagnostic value.
mRNA expression levels of eight candidate marker genes - BIRC5, CCND1, CDH1, CITED1, DPP4, LGALS3, MET and TFF3 was measured by real-time RT-PCR in paired nodular and surrounding normal thyroid tissue specimens of 105 consecutive patients undergoing thyroid surgery and compared between different types of thyroid lesions.
Significant differences in the mRNA expression levels between the normal and malignant thyroid tissues and between benign and malignant nodules were found for BIRC5, CCND1, CITED1, DPP4, LGALS3, MET and TFF3, but not CDH1. On a single gene basis, relative quantity (RQ) of LGALS3 had the highest diagnostic value for the discrimination of malignant and benign thyroid nodules (AUC=0.832, P<0.0001 and 90.9% sensitivity and 65.6% specificity at the optimal cut-off on ROC curve). The only two-marker set that outperformed LGALS3 was RQ sum of LGALS3 and BIRC5 (AUC=0.841, P<0.0001). An application of multivariate logistic regression analysis resulted in the generation of a multiplex biomarker model based on LGALS3, BIRC5, TFF3, CCND1, MET and CITED1 that had considerably higher specificity than a single marker or two marker gene-based models (AUC=0.895, P<0.0001, 70.5% sensitivity and 93.4% specificity).
This study confirmed that mRNA expression levels of 7 out of 8 candidate genes analysed have a diagnostic value for the distinction of benign and malignant thyroid nodules. The multiplex biomarker model based on 6 genes outperformed a single marker or two marker-based models.
Withdrawn
Robotic Transaxillary Total Thyroidectomy and Central Neck Dissection Using a Single Axillary Incision
Thyroid Cancer Saturday Poster Clinical
Robotic thyroidectomy is gaining more attention in the United States over the recent years. Various techniques for thyroid lobectomy and total thyroidectomy have been described. To our knowledge, total thyroidectomy with central neck dissection through a single axillary incision has not been described in the North American literature.
We herein describe the case of a patient who underwent robotic total thyroidectomy with central neck dissection through a single axillary incision. The procedure was performed under general anesthesia through a 6 cm right axillary incision. The robotic camera and 2 working robotic arms were used for the procedure.
A 43-year-old lady who has been followed for a right thyroid nodule since 2006, Although, her initial biopsy was benign, her repeat FNA recently showed findings suspicious for a follicular neoplasm in a 2.1 cm right thyroid nodule. The left thyroid lobe was of normal size and echogenicity without any nodules. She was consented for a robotic transaxillary right thyroid lobectomy and isthmusectomy. At the time of her procedure, lymph nodes were encountered in the right central neck and biopsied. Frozen section revealed metastasis from papillary thyroid cancer and total thyroidectomy with right central neck dissection was performed. During the procedure, both recurrent laryngeal nerves, right superior laryngeal nerve and the parathyroid glands were seen and preserved. Flap time was 30 minutes, docking 10, console 110 and total skin-to-skin operative time was 180 minutes. She was discharged home on postoperative day (POD) #1 uneventfully. On POD#1, her serum Ca was 8.0 and PTH 21 pg/mL. Pathology showed a 1.1 cm papillary thyroid cancer in the right thyroid lobe, with metastasis involving 11 out of 16 lymph nodes. She is currently being evaluated for radioactive iodine ablation.
This initial report demonstrates that total thyroidectomy and central neck dissection can be performed robotically through a single axillary incision in experienced hands.
Thyroid Metastasis Post Resection of Atypical Bronchial Carcinoid- A Case Report
Thyroid Cancer Saturday Poster Clinical
Carcinoid tumours are derived from neuroendocrine cells mostly from the GI tract or bronchopulmonary system. They are rare, accounting for less than 1% of cancers. Carcinoids are graded based on mitotic count and/or a Ki67 proliferation index. Pulmonary carcinoids are categorised into 4 groups namely typical, atypical, small cell lung carcinoma and large cell neuroendocrine carcinoma. Typical and atypical carcinoids are indolent with a low risk of metastasis. Thyroid metastasis from a primary carcinoid is extremely rare with only few isolated reported cases (1). In addition less than 25% of cases are associated with deranged thyroid function tests or a clinical enlarged gland (2). This makes thyroid metastasis due to a primary carcinoid a diagnostic challenge.
A 76-year-old lady was referred to our endocrinology clinic with a radiological suspicion of possible thyroid metastasis of previously resected lung carcinoid. She had past history of a sporadic bronchial carcinoid. Diagnosis of a bronchial tumour was incidental following imaging for an unrelated condition. She underwent a left lower lobectomy (T1N2M0). Histology was consistent with an atypical carcinoid with clear bronchial margins & a Ki67 score of 10–15%. Ten months later an isotope bone scan was suggestive of bony metastasis. A follow up PET scan showed an incidental increased uptake on the left lobe of the thyroid.
She was clinically and biochemically euthyroid without any palpable glandular enlargement on examination. A multinodular goitre with a 10 mm hypo echoic nodule in left lobe with associated lymphadenopathy was confirmed on ultrasound. Histology from an image guided diagnostic aspirate was consistent with metastatic atypical carcinoid(image). Given the evidence of disseminated disease with OctreoScan negativity, she was referred to oncology for palliative treatment.
Our case has 2-fold significance. Firstly it contributes to the current data of isolated reports of carcinoid secondaries to the thyroid. It also highlights the importance of follow up imaging even after complete resection of a primary bronchial carcinoid in the absence of symptoms.
Endocrine Unit-Dept. of Medical Sciences, University of Milan, Milan, Italy
Thyroid Cancer Saturday Poster Clinical
The evaluation of basal and stimulated serum human calcitonin (hCT) levels are mandatory for the diagnosis and follow-up of medullary thyroid cancer (MTC). Due to the unavailability of pentagastrin (Pg) in the United States and in several European Countries, the reliability of Calcium (Ca) test was tested in patients and controls.
Patients treated for MTC in remission (n=24) or in persistence (n=18), RET gene mutations carriers (n=14), patients with nodular goiter (n=32) and healthy volunteers (n=16) were included. hCT was measured using a two-site immunometric assay before and after stimulation using Pg, 0.5 mcg/kg body weight, or Ca gluconate, 25 mg/kg.
In all groups, no significant differences were noted in the levels of hCT stimulated either by Pg or by Ca (Pearson's rho: 0.8849). In women, basal hCT≤20 pg/ml associated with MTC in 13%, and basal hCT>21 pg/ml in 100% of cases, whereas Ca stimulated hCT between 101–500 pg/ml associated with MTC in 75% and Ca stimulated hCT>500 in all cases. In men, basal hCT 51–100 indicated MTC in 67% and basal hCT>100 pg/ml in 100% of patients, while Ca stimulated hCT levels>500 pg/ml associated with MTC only in 50% and levels>1000 pg/ml in 67% of cases. The most discriminatory peak threshold between normal and CCH (focal, diffuse or nodular) or MTC was 60 pg/ml for women and 100 pg/ml for men. With these thresholds, PPV and NPV were 100% for females and of 91 and 100% for males. Finally, the intensity and duration of side effects were significantly lower during Ca test.
High-dose Ca test is a potent and well tolerated procedure. The prevalence of MTC was high even for low hCT basal levels, confirming the importance of the measurement of hCT during stimulation test. Present results show that the best Ca stimulated hCT threshold able to discriminate between normal and CCH/MTC was 60 pg/ml for women and 100 pg/ml. These data, associated with the significantly lower cost of this test and the worldwide availability of Ca, indicate the high-dose Ca as the test of choice for the diagnosis and the follow up of MTC.
Surgical Oncology, Institute of Oncology, Ljubljana, Slovenia
Thyroid Cancer Saturday Poster Clinical
It is believed that chemotherapy (ChT) is ineffective in follicular thyroid carcinoma (FTC) and Hürthle cell thyroid carcinoma (HCTC). The aim of our retrospective study was to find out if neodjuvant ChT before thyroid surgery had any effect on the size of primary tumor in patients with FTC or HCTC.
Altogether 312 patients (207 females, 105 males; mean age 56 y.) with FTC or HCTC were seen at our institute from 1972–2010. T3 or T4 tumor stage was present in 215 patients. The study included 29 patients (20 women, 9 men; mean age 60.8 y.) with FTC or HCTC, who had T3 or T4 tumor and were treated with neoadjuvant ChT from 1979–2004. A mean tumor diameter was 9.3 cm. Extrathyroid growth of tumor was present in 15 patients. Regional and distant metastases were detected in 6 and 12 patients, respectively. With respect to the site of metastatic spread, the lung was involved in 8 patients and the skeleton in 5. ChT consisted of Vinblastine in 19 cases, Vinblastine with Adriamyin in 5 cases or other ChT regimens in 5 cases.
Altogether, 67 cycles of ChT were given and tumor size decreased for more than 50% in 13 patients (=45%). ChT was effective in patients with FTC and HCTC in 47% and 43%, respectively. In the patients with and in those without distant metastases, a primary tumor size decreased by more than 50% in 17% and 65% (p=0.02), respectively. R0, R1 and R2 resection was performed in 15, 10 and 4 cases, respectively. Histopathology revealed that ChT (i.e. wide areas of tumor necrosis) was effective in 7 patients (24%). The 5-year and 10-year cause-specific survivals of the patients were 77% and 47%, while the 5-year and 10-year disease-free intervals were 57% and 46%, respectively. Six patients are still alive (median survival 162 months) and four of them have no evidence of disease, six patients (five of them without evidence of disease) died of other causes (median survival 101 months), while 17 patients died of FTC or HCTC (median survival 72 months). Among them, 16 died of distant metastases, while only one succumbed to locoregional recurrence and distant metastases.
ChT before surgical procedure may be effective in order to decrease the tumor size in FTC or HCTC in 45% of patients.
Geriatrics, University of Arkansas for Medical Sciences, Little Rock, AR
Thyroid Cancer Saturday Poster Clinical
Serum thyroglobulin (Tg) measurement has become a standard method of surveillance for tumor progression and elevated Tg is often interpreted as evidence of cancer recurrence. Our clinical observations have shown that in some patients, Tg values often stabilize/normalize over time without aggressive therapy. We used a conservative approach to outpatient management of differentiated thyroid cancer (DTC) patients with persistent, non-localizable disease as documented by positive Tg serum values but negative whole body scanning (WBS, positron emission tomography (PET), and/or other imaging modalities.
Outpatient therapy records for DTC patients at the UAMS Thyroid Clinic from January, 1999 to December, 2009 were reviewed. Subjects having total thyroidectomy, radioactive iodine ablation, measurable serum Tg, ages 18–89, and no evidence of disease on WBS or PET scans were included. All available Tg values, MRI, CT, WBS and PET scan results for each patient were recorded and analyzed for evidence of disease progression.
Seventeen patients 20–73 years were studied. Average follow up: 5 years and 6 months (5.5 months to 12 years). All patients were treated with total thyroidectomy and postoperative RAI (doses 99mCi to 210mCi, average of 119mCi). Mean Tg values ranged from 0.41 to 4.34 during the follow up period. Tg levels remained stable or gradually decreased in all patients during the time period studied.
Patients undergoing total thyroidectomy for DTC postoperatively are followed for recurrence by serial serum Tg measurements and imaging modalities including WBS and PET when indicated. Some patients present with mildly elevated Tg values but without localizable disease on imaging. These patients may have additional RAI treatments based on the Tg elevation. However, our clinical experience has shown that many of these patients will have Tg levels that either achieve stability or decrease over time without further treatment.
Pattern and Risk Factors of Central Compartment Lymph Nodal Metastasis in Papillary Thyroid Carcinoma - A Prospective Study from an Endocrine Surgery Center of India
Thyroid Cancer Saturday Poster Clinical
Papillary thyroid carcinoma (PTC) is most common thyroid malignancy with predilection for lymphatic spread mainly central compartment of neck. Routine central compartment lymph nodes (CCLN) dissection is always controversial, with increased risk of morbidity. The aim of our study is to determine pattern and risk of central compartment lymph node metastasis (LNM) in PTC.
Prospective study, PTC who underwent TT and lymph nodal dissection (LND) in primary setting from 2008 till 2010, at our Institute. The right and left central and lateral lymph nodes were submitted separately for pathological examination and determined the number and laterality of positive CCLN. We analyzed the risk of CCLN metastasis and compared the post-operative complications with a control group of 130 patients of benign thyroid disorders (BTD), who underwent TT alone.
N=47; mean age=35.4±12.89 yrs; M:F≈1:2; mean duration of goiter=3.37±5.5 yrs, mean tumor size=3.57±2.42 cm, however (n=8) have <1cm size. N=19 node-negative and n=28 node-positive; multifocal tumor=16 and bilateral=09. N=38, Underwent TT+B/L CCLND, TT+U/L CCLND in-2 and TT+CCLND+LND in-16. Overall Positive LNM in 31(65%), with CLNM in-28(60%). LNM in ipsilateral-paratracheal in-26 and contralateral-paratracheal in-19. Stage wise LN Positivity T1=50%, T2=42%, T3=72%, T4=77%, Subtypewise LN Positivity - Classical variants=63%, Follicular variant=38%, Warthine like variant=100%, Tall Cell variant=67%; Bilaterality=67% & Multicentricity=72% positivity of LN. On comparing with age-sex matched controls with TT-alone, the rate of PTAT (p=0.002), inadvertently removed parathyroid (p=0.000), temporary & permanent hypocalcaemia (p=0.009), temporary-hoarseness (p=0.039) and surgery-duration (p=0.000), were significantly higher in LND group than in TT-alone group. However the rate of permanent RLN palsy, drain-duration and hospital stay was not significantly different.
Tumor size is an important risk factor for the CCLNM, Tumor stage and variants are also important risk factor. Occult contra lateral CCLNM is not uncommon and very well correlated with tumor size so prophylactic B/L CCLND may be useful with the significant morbidity.
Belorussian, International Fund “Help for Patients with Radiation-Induced Thyroid Cancer “Arnica”, Minsk, Belarus
Thyroid Cancer Saturday Poster Clinical
The analysis of health care for childhood long-term radiation-induced thyroid cancer survivors in Belarus has demonstrated numerous issues for the patients that are being monitored according to the contemporary guidelines. In 2010, in the framework of the EC/UNDP project “Establishment of International Scientific and Practical Centre of Thyroid Disease in Belarus” thyroid carcinoma patients with no regular follow-up were identified and evaluated.
The study included 189 patients (127 females, 62 males). All patients were younger than 18 years of age at the time of the Chernobyl accident (mean age 3.7±3.6 yrs). The mean age at thyroid cancer diagnosis was 13.5±4.6 yrs., at the time of investigation was 28.1±3.6 yrs. About 80% of patients had total thyroidectomy (TTE) followed by 131-radioiodine (131-I) treatment and levothyroxine (L-T4) suppressive therapy. Neck ultrasound, thyroid and parathyroid function tests such as serum FT4, TSH, thyroglobulin (TG), thyroglobulin-antibodies (TG-AB), calcium and phosphorus measurements were performed.
All but 11 (5.3%) thyroid cancer patients were treated with L-T4. The average L-T4 dose was 2.5±0.8 mcg/kg. The overall mean TSH level was 4.4±24.3 mIU/l. About 66% of patients had suppressed TSH level (<0.3 mIU/l) and 10% had TSH>4 mIU/l. After TTE, 17.2% of patients had an elevated basal TG levels, i.e.>2 ng/ml, and detectable TG-AB levels (>50 IU/ml) were found in 36.4% of survivors. More than 20% of patients had hypoparathyroidism. Three cases (1.5%) of secondary malignancies (acute leukemia, salivary gland, breast cancer) have been registered.
The study of Chernobyl-related thyroid cancer survivors revealed persistence of TG levels in the setting of inadequate TSH suppression. The latter one may be due to lack of the quality of the test laboratories in local hospitals, insufficient access to specialized medical centers and inadequate patients' compliance.
Pôle Information Médicale Evaluation Recherche, Lyon University Hospital, Lyon, France
Thyroid Cancer Saturday Poster Clinical
Young surgeons need time to accumulate experience necessary to achieve high performance levels. Such a learning process has to be considered when assessing their outcomes. We propose a new approach in monitoring the performance of inexperienced surgeons that incorporates the learning curve inherent to thyroid surgery.
A one-year study was conducted prospectively at five university hospitals. A total of 1,688 bilateral thyroidectomies were performed by 19 endocrine surgeons during their first eight years of practice. Main outcome measures included the occurrence of postoperative recurrent laryngeal nerve palsy and operative time. The database was randomly split into training and testing datasets. Training data served to determine the expected performance curve of surgeons during their career as well as factors influencing outcome variation using mixed models. Testing data were plotted on CUmulative SUM (CUSUM) charts using estimates from previous modeling step. Classical chart displayed case-mix adjusted surgical outcome. Performance chart presented outcome adjusted both for patient's case-mix and surgeon's experience.
For every surgical outcome, a significant relationship between surgeon's performance and experience was observed (P<.01). Generation of performance curve demonstrated improvements in both safety and efficiency of thyroid surgery from the first to the eighth year of surgeon's practice, as evidenced by the gradual reduction from 14% to 4% for the recurrent nerve palsy rate and from 147 to 82 minutes for the operative time. Integrating this learning effect to the assessment of individual surgeons' outcome revealed marked differences in perception of their performance relative to the classical approach. The CUSUM performance chart changed the magnitude of indicator variations and the sign of detected signals in monitoring a surgeon with good (A) or poor outcomes (B).
Not considering the initial learning curve of surgeons performing thyroidectomy leads to imperfect measurement and to misinterpretation when assessing their individual performance. The performance chart represents a valuable tool to monitor the outcome of surgeons at early stage of their career.
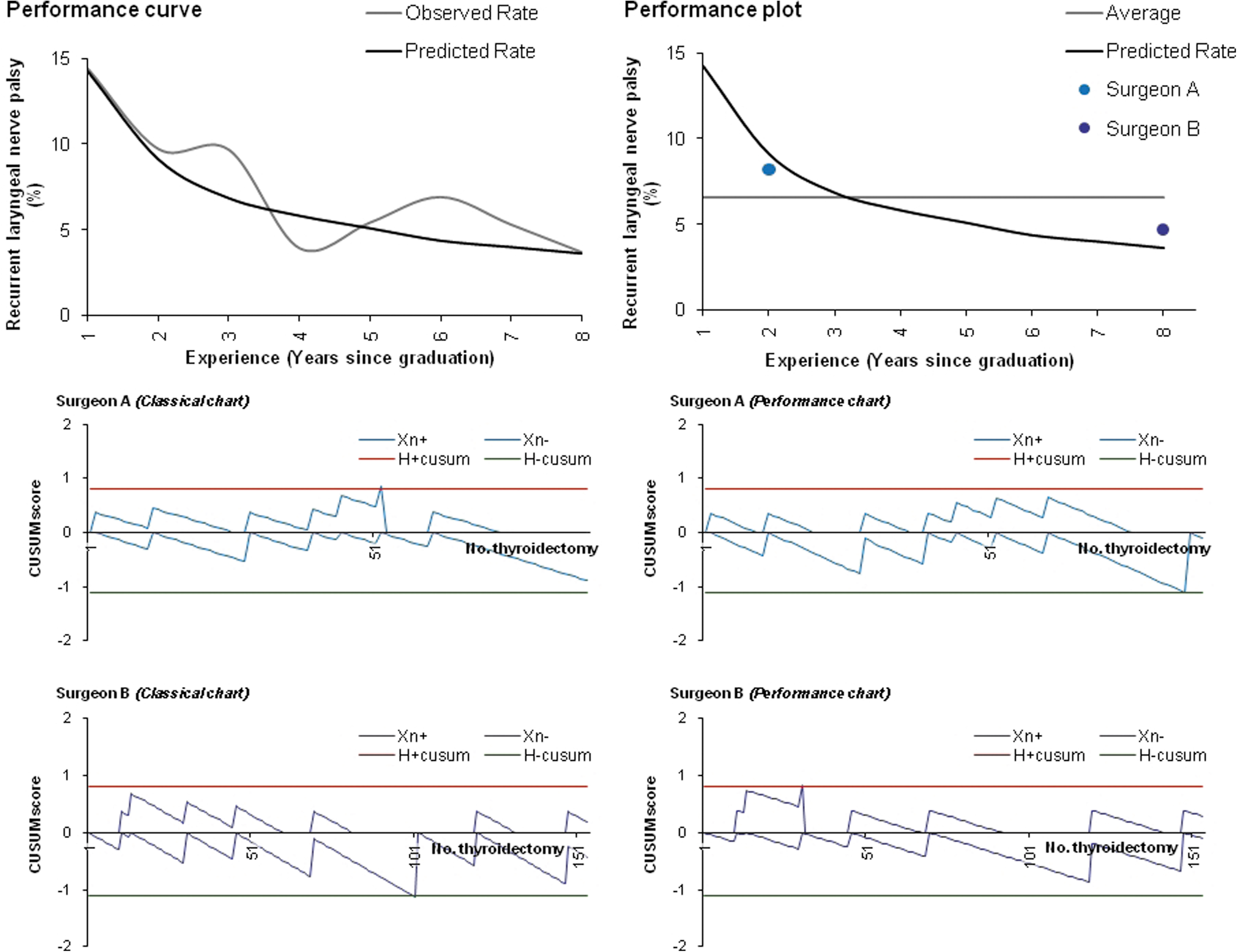
Performance monitoring related to the recurrent laryngeal nerve palsy.
Thyroid Cancer Saturday Poster Clinical
Serum thyroglobulin (Tg) assays are still considered the cornerstone of postoperative surveillance programs for patients with papillary thyroid cancer (PTC). For individuals who have not undergone postoperative radioiodine remnant ablation (RRA), the clinical significance of detectable Tg levels is unclear since the Tg production may well originate from the remnant of normal thyroid tissue. Aim of the study was to explore the evolution of Tg levels over time in PTC patients who have undergone total or near total thyroidectomy without RRA.
We retrospectively analyzed data from 784 consecutively diagnosed PTC patients with low risk of persistent/recurrent disease based on the 2009 American Thyroid Association risk stratification. Additional inclusion criteria were negative Tg antibodies. All 784 had undergone (near) total thyroidectomy (with radioiodine remnant ablation in 495, 63%) and were followed yearly with neck ultrasonography and Tg measurement. To investigate the evolution of serum Tg levels over time we used a multiple-level approach. First, we compared the Tg values (functional sensitivity of 1 ng/mL) measured at the time of last follow-up in patients who received or did not receive RRA. Furthermore, we analyzed the trend of serial Tg determination (functional sensitivity of 0.2 ng/mL) in a subset of not-ablated individuals (n=78).
The median follow-up period was 6 year (2.5–25 years). Final serum thyroglobulin levels were undetectable (<1 ng/mL) in almost all RAI patients (492/495; 99%) and in the majority (274/289; 93%) of non-RAI patients. As for the subset of cases who underwent serial Tg determination (non-RAI patients), 60% had undetectable values (<0.2 ng/mL) already at the first post-surgical evaluation (i.e., 3 to 12 months after thyroidectomy). The remaining individuals showed spontaneously decreased Tg levels over time, with 75% of patients having undetectable levels within 5 years of follow-up.
Post-operative serum Tg values spontaneously drop to undetectable levels in not-ablated PTC patients. Serial Tg determination could turn to be useful in the long term surveillance of such individuals, we will increasingly facing in the clinical practice.
Department of Pathology I, Tokyo Women's Medical University, Tokyo, Japan
Thyroid Cancer Saturday Poster Clinical
Establishment of new methods that can distinguish thyroid follicular carcinoma (FC) from adenoma (FA) is the one of the urgent issues in management of thyroid nodules. In order to address this issue, we utilized 2nd generation sequencing equipments for massive quantitative analysis of RNA from circulating blood cells as well as tumor tissue, because it can elucidate the whole gene expression profiling for statistical analysis. We here present some of our analysis and the potential candidate genes.
Sample collection and analysis were approved by ethical committee of the university. RNA was extracted from whole blood from 3 patients with metastatic FC. RNA was also extracted from frozen tissues of FC and FA. We also extracted from FTC-133 cells in basal and EGF-stimulated conditions. Poly A+RNA was selected as for FTC-133 cells but non-poly A RNA was also utilized by micro RNA extraction kit which exclude ribosomal RNA in blood and tissue samples. SAGE analysis was prepared using SOLiD-SAGE kits and sequencing was carried out SOLiD system. The sequenced tags were referred to reference sequence (NCBI) and the number of tags was counted. We excluded ribosomal RNA from final analysis.
More than 8 million sequences for 117 thousand tags for the tissues and more than 2 million sequences for more than 30 thousand tags for blood samples were obtained. At first we selected 31 tags by the ratio of carcinoma to adenoma and the number of tags in carcinoma. Of interest as for these selected tags, the frequency in these tags in three blood samples well correlated each other (ρ=0.7911–0.9413) The ratio of carcinoma to adenoma had no correlation with EGF-stimulation ratio but negatively correlated with those of blood samples (ρ=−0.4069). Only 4 tags; IYD(deiodinase), TPO, IGSF1, GPX3 were undetectable in blood samples. The most abundant was MT-RNA2-like 8 and others were related with leukemia, cancer invasion and apoptosis. We are going to evaluate the clinical roles of these genes.
The massive quantification and selection of RNA in blood as well as tumor tissues can be a useful method for identification of specific markers for the diagnosis and evaluation of metastasis of FC.
Analysis of Prognostic Factors in Patients with Multiple Recurrences of Papillary Thyroid Carcinoma
Thyroid Cancer Saturday Poster Clinical
Numerous studies in the past have mentioned various factors that influence the recurrence of papillary thyroid carcinoma, including age, tumor size, advanced stage, extrathyroidal extension, and distant metastasis, and attempts have been made to classify the disease into low-risk and high-risk group based on these clinicopathological factors. However, there has been relatively scarce study on patients with multiple recurrent papillary thyroid carcinoma. This study analyzed the risk factors associated with such cases.
This study investigated various clinicopathological factors of 416 patients who were diagnosed with papillary thyroid carcinoma and received primary surgery at Yonsei University Wonju College of Medicine, Department of Surgery, from January 1983 to December 2006 and were followed up until October 2010.
The univariate analysis on risk factors revealed tumor size greater than 2 cm, multifocality, metastasis to central neck lymph modes, AJCC TNM stage III and IV, and MACIS score greater than 6 to be risk factors associated with multiple recurrences of papillary thyroid carcinoma. A multivariate analysis performed on variables selected from univariate analysis demonstrated no significant risk factor. The 10-year disease-specific survival for 3 different patient groups (group 1, 2, and 3) was 100%, 100%, and 83.1%, respectively, and patients in more clinically advanced group demonstrated poorer prognosis (p<0.001). The 10-year overall survival rate for the 3 patient groups was 93.9%, 100%, and 92%, respectively, and clinically advanced groups tended to show poorer overall survival rate as well (p=0.046).
A more aggressive and extensive surgery, as well as closer follow up, is to be required when operating on patients with tumor size greater than 2 cm, multifocality, metastasis to central neck lymph modes, AJCC TNM stage III and IV, and MACIS score greater than 6. The use of imaging modalities, such as ultrasonography and PET-CT scan, may be desirable when monitoring such patients.
Association Between Serum TSH Level and Papillary Thyroid Microcarcinoma in Korean Euthyroid Patients
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer is a common disease, and its prevalence is increasing. Recently, some reports have shown that an elevated thyrotropin (thyroid stimulating hormone, TSH) level is associated with thyroid cancer risk. However, the association between TSH level and thyroid cancer risk is not yet known for euthyroid patients diagnosed with papillary thyroid microcarcinoma (PTMC).
Our study included 425 patients who underwent thyroid surgery and were diagnosed with PTMC between 2008 and 2009. Control group patients were diagnosed with benign nodules ≤1 cm in size by US-guided fine needle aspiration. Nodules with one or more suspected malignant-ultrasonographic feature(s) were excluded from this study. Patients who were not euthyroid or who took thyroid medication were also excluded.
The mean age of all patients was 48.5±11.0 years, and 88.8% were women. The mean age of those with PTMC was significantly lower than that of the control group. The mean TSH level was 1.78±0.93 mIU/L, and the mean free T4 level was 15.96±2.32 pmol/L. There was no difference in TSH level between the PTMC and control groups (1.77±0.93 mIU/L vs. 1.79±0.91 mIU/L, P=0.829). After adjusting for age, TSH level was not correlated with tumor size (r=0.02, P=0.678) in the PTMC group. Moreover, the TSH level did not differ between patients with stage I and stage III-IV carcinoma (stage I: 1.77±0.95 mIU/L, stage III-IV: 1.79±0.87 mIU/L, P=0.856).
TSH levels are not elevated in euthyroid PTMC patients. Thus, further evaluation is needed before serum TSH can be used as a tumor marker for small nodules≤1 cm in size among euthyroid patients.
Hospital Pathology, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
Thyroid Cancer Saturday Poster Clinical
BRAF mutation is the most common genetic event in papillary thyroid carcinoma (PTC); however, the prevalence and patterns of the mutation vary worldwide. We investigated the frequency and type of BRAF mutations based on the histologic subtypes in a large cohort of Korean patients with PTC.
A total of 1041 consecutive PTCs were classified according to histologic subtypes. BRAF mutations were examined by denaturing high performance liquid chromatography and direct sequencing. Rare complex mutations were confirmed by molecular cloning of PCR amplicons and sequencing of the products.
BRAF mutations were found in 839 (80.6%) of 1041 patients with PTC. The histologic subtype specific prevalence of BRAF mutation was as follows: 85.3% (249/292) in classic, 45.8% (11/24) in follicular, 79.9% (576/721) in microcarcinoma, and 75.0% (3/4) in other variants. In addition to the usual c.1799T>A mutation, we identified other four mutation types: c.1799_1800TG>AA, c.[1795_1796insA; 1770_1795 dup 26], c.[1742–10T>C]+[1799T>A] and c.[1796C>G;1799T>A], respectively. The latter three were novel mutations in thyroid tumors. Within the series of microcarcinoma variants, BRAF mutation rate was lower in tumors with follicular morphology than those with non-follicular types (66.7% vs 80.9%, p=0.0145).
Out of 1041 Korean patients with PTC, 0.4% had rare types of BRAF mutation and three new somatic mutations were identified. The BRAF mutation rate was quite low in PTC with follicular morphology regardless of tumor size. However, the prevalence of BRAF mutation in microcarcinoma and follicular variants of PTC is relatively high in Korea and its analysis may be clinically useful for managing the patients.
Department of General Surgery, Istanbul University, Cerrahpasa Medical School, Istanbul, Turkey
Thyroid Cancer Saturday Poster Clinical
The established primary treatment of papillary thyroid cancer (PTC) is either total thyroidectomy or thyroid lobectomy depending on the tumor characteristics. In addition to this, the ATA consensus statement also recommends therapeutic central neck dissection (CND) in PTC patients with clinically involved nodes and prophylactic CND in advanced tumors without evidence of nodal involvement. Despite these recommendations, there is still controversy regarding the ideal surgical management of the central lymph nodes. We therefore analyzed the utility of pre- or intraoperative ultrasonography in performing CND in PTC patients treated with thyroidectomy.
In this prospective study performed between January 2009 and January 2011, 40 patients with PTC diagnosed by fine needle aspiration biopsy and frozen section findings were examined with pre- or intraoperative neck ultrasonography to confirm or to rule out the presence of central lymph node metastases. All patients underwent total thyroidectomy and CND. The ultrasonography findings were compared to the final histopatholgic results. The sensitivity and specificity rates of ultrasonography were evaluated.
There were 33 female and 7 male patients with a mean age of 42 years (range, 23–57 years). The mean diameter of the tumor was 1.1 cm (range, 0.3–3 cm). Ultrasonography revealed suspicious findings for central node metastasis in 16 patients and no nodal involvement in 24 patients. On postoperative histopathologic examination, out of the 16 patients with suspicious ultrasonography findings, 14 patients were confirmed as having central nodal metastases. Out of the 24 patients with negative ultrasonography results, 2 patients were also confirmed as having central nodal metastases. The sensitivity and specificity rates of pre- or intraoperative US for detecting central node metastasis were 87% and 91%, respectively.
Based on the findings of this study, pre- or intraoperative ultrasonography is an effective guide in determining the necessity of CND in patients with PTC.
Division of Endocrinology and Metabolism, Departments of Internal Medicine, The Catholic University of Korea, College of Medicine, Seoul, Republic of Korea
Thyroid Cancer Saturday Poster Clinical
In the management of DTC patients, especially low-risk patients, measurement of stimulated thyroglobulin (Tg) has become a mainstay of follow-up methods. The aim of our study is to verify the role ablation-Tg, 1st-stimulated-Tg and estimation of Tg response in both low- and moderate-to-high-risk patients with differentiated thyroid carcinoma (DTC).
We reviewed the charts of 430 patients with DTC who were treated by total thyroidectomy followed by high dose (100–150mCi) radioactive iodine ablation (RAI) therapy. All were followed up by diagnostic whole body scan (DxWBS) with T4 withdrawal after the first RAI treatment. Tg was measured at the time of RAI ablation (ablation-Tg), and DxWBS after 1st RAI ablation (1st-stimulated-Tg). Factors, which might predict the recurrence, were evaluated by Kaplan-Meier and Cox regression analysis. In cases with decreasing Tg after RAI ablation, Tg response was estimated by absolute value differences between ablation-Tg and 1st-stimulated-Tg, and was classified in to good (decrease in Tg level>2ng/ml), moderate (1–2ng/ml), or no definite response (<1ng/ml).
363 subjects including patients (n=135) with moderate-to-high risk of recurrence were analyzed. Mean follow-up was 62.4 months (range 8–96). Persistent/recurrent cases were found in 32 patients (8.8%). Detectable ablation-Tg (p=0.003), 1st-stimulated-Tg (p=0.0001) and the presence of thyroid capsule invasion (p=0.047) were significant factors predicting the recurrence in univariate analysis. In multivariate analysis, ablation-Tg (p=0.002) and 1st-stimulated-Tg (p=0.008) were independently related to recurrence. In subgroup analysis, ablation-Tg (p=0.016) was the only independent prognostic factor in low-risk patients, and 1st-stimulated-Tg (p=0.0001) in moderate-to-high-risk patients. Especially, among moderate-to-high-risk patients with undetectable 1st-stimulated Tg, Tg response was a predicting factor for recurrence (Figure 1), and the only independent factor related to recurrence (p=0.009).
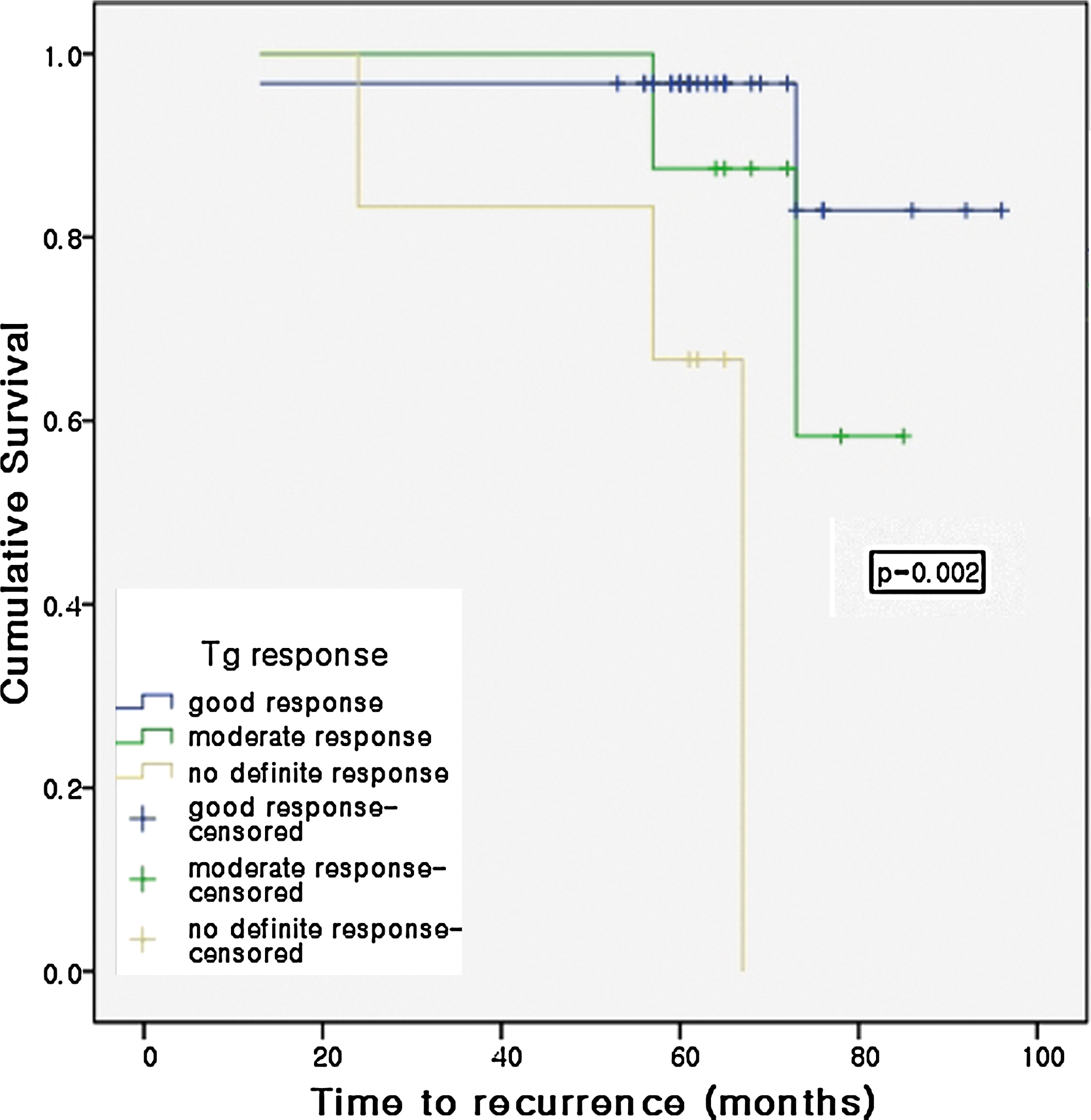
Ablation-Tg or 1st-stimulated-Tg is a reliable predictor of recurrence in DTC patients according to risk stratification. In addition, estimation of Tg response can contribute to management of moderate-to-high-risk DTC patients.
Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea
Thyroid Cancer Saturday Poster Clinical
Current management for patients with differentiated thyroid cancer includes near total thyroidectomy and radioactive iodine therapy followed by administration of supraphysiological doses of levothyroxine (L-T4). The aim of our study is to evaluate the impact of long term suppressive therapy with L-T4 on bone mineral density (BMD) and bone turn over markers in female patients with L-T4 suppressive therapy.
We enrolled 94 female subjects (mean age=50.84±11.43 years) receiving L-T4 for at least 10 years after thyroid cancer management. The subjects were divided into three groups (group 1 with TSH levels≤0.001 μIU/mL; group 2 with TSH levels between 0.001 and 0.07 μIU/mL; group 3 with TSH levels>0.07 μIU/mL) by TSH levels and four groups by quartile of free T4 levels. The subjects were evaluated BMD by dual-energy X-ray absorptiometry.
No significant decrease was detected in BMD and bone turnover markers classified by TSH levels and free T4 levels. Also, the prevalence of osteoporosis and osteopenia was not different among groups.
Long term L-T4 suppressive therapy after thyroid cancer management did not effect on bone density and increase the prevalence of osteoporosis although TSH levels were supraphysiologically suppressed.
Data are presented by mean±standard deviation. Group 1, TSH≤0.001 μIU/mL; group 2, TSH>0.001 and≤0.17 μIU/mL; group 3, TSH>0.17 μIU/mL. L-T4, levothyroxine TSH, thyroid stimulating hormone; CTX, C-telopeptide; BMD, bone mineral density.
Nuclear Medicine, Peking Union Medical College Hospital, Beijing, China
Thyroid Cancer Saturday Poster Clinical
Recent studies have shown that thyroglobulin (Tg) concentration is a useful tumor marker in follow-up of differentiated thyroid cancer (DTC) patients after thyroidectomy and subsequent radioiodine (131I) therapy. However, its role is controversial after total or near-total thyroidectomy before the first 131I ablative treatment. So we used thyroid stimulating hormone (TSH) levels to normalize predictive values of Tg for DTC.
The study was a retrospective analysis. 244 patients with DTC who had undergone a total thyroidectomy and subsequent 131I therapy were included. Exclusion criteria were patients with high serum Tg antibody (TgAb) concentration and in whom it was not measured. Patients were divided into two groups as M1 and M0 according to whether the patient present with or without distant metastases (DM).
Pre-ablative stimulated Tg in Group M0 ranged between 0.1 and 348.9 ng/ml and Group M1 between 0.2 and 1000 ng/ml. Tg/TSH ratios ranged 0.000667–12.143ng/IU and 0.002948–12500ng/IU. (Both of Tg and Tg/TSH values were significantly different between the two Groups (the Wilcoxon rank-sum test: Tg p<0.0001(z=8.785), Tg/TSH p<0.0001(z=8.850)). The areas under receiver operating characteristic curves (ROC) for Tg concentrations and Tg/TSH ratios were 0.913 and 0.916 respectively.
Both Tg and Tg/TSH ratios might be considered predictive markers for metastases of DTC just after total thyroidectomy before the first 131I ablative therapy.
Comparison of Serum Thyroglobulin and Tg/TSH Ratio in Patients with DTC
Thyroid Cancer Saturday Poster Clinical
Cancer gender disparity in incidence, disease aggressiveness and prognosis has been observed in a variety of cancers. The incidence of thyroid cancer is higher in women. Although some investigators have reported male gender is associated with worse prognosis in thyroid cancer of follicular cell origin, this finding is controversial. Thus, we sought to better characterize the role of gender in disease aggressiveness and outcome using a large population-based database.
Data of patients with thyroid cancer (excluding medullary thyroid cancer) from the Surveillance, Epidemiology and End Results 17 Registries Database (1988–2007) was used to compare extent of disease and disease-specific survival (DSS) by univariate and multivariate analyses.
We identified 61,523 patients with thyroid cancer (13,642 men/47,881 women). The median follow up time was 54 months. At diagnosis, 61.2% of men were ≥45 years, compared to 49.7% of women (p<0.01). Men had significantly more aggressive histologic subtypes of differentiated thyroid cancer (DTC) and undifferentiated thyroid cancer (UTC), regardless of age group (p<0.01). Moreover, men had significantly more advanced disease at presentation: larger primary tumor size (p<0.01), and higher rates of extrathyroidal extension (p<0.01), regional lymph node metastasis (p<0.01) and distant metastasis (p<0.01). DSS stratified by pathology was significantly worse in men (227.5 and 234.3 months in men and women, respectively, p<0.01) despite more total thyroidectomies being performed in men (p<0.01). On multivariate analysis, gender was not an independent prognostic factor.
Men with thyroid cancer are more likely to present with more advanced disease, aggressive histologic subtypes, and older age. However, gender is not an independent prognostic factor for DSS.
Significance of Diffuse Liver Radioiodine Uptake in Differentiated Thyroid Cancer
Thyroid Cancer Saturday Poster Clinical
Diffuse hepatic radioactive iodine uptake's significance in differentiated thyroid cancer is contradictory in published literature. Hence, to determine significance of liver to thigh ratio (LTR) in patients with variable disease status of differentiated thyroid cancer.
280 patients of differentiated thyroid cancer were divided into six groups based on their disease status prospectively. Ratio of average counts in the liver ROI and mid thigh ROI was calculated for generating liver to thigh ratio (LTR) from anterior and posterior whole body radioiodine images. Comparison of LTR value among different study groups were done. Correlation of LTR with dose of radioiodine, serum thyroglobulin and TSH of the patients was also obtained.
Patients with negative WBRI scan and raised serum thyroglobulin (group 4) have no significant difference (P=0.233) in LTR in comparison to disease free (group 1) (defined as negative WBRI scan along with serum thyroglobulin <4). Mean LTR is highest in patients with bone or lung metastasis. On the contrary, patients who have only lymph node metastasis or negative radioiodine scan have lowest mean LTR. Patients with remnant thyroid tissue have significantly higher mean LTR than those with lymph node metastasis only or negative radioiodine scan but significantly lower value compared with patients with bone or lung metastasis. There was only a weak positive correlation (r=0.395) between serum thyroglobulin and LTR. There was significant association between LTR and serum TSH (Pearson Chi-square value=0.000).
LTR correlates very well with functional status of tumor cells, while it is independent of amount of radioiodine administered, serum thyroglobulin and hence total disease burden. This study suggests that liver uptake is almost identical in patients who have a negative WBRI scan irrespective of their serum thyroglobulin level, thus not of much help in management of patients who have negative radioiodine scan and raised serum thyroglobulin.
Durable Effect of Radioactive Iodine in a Patient with Metastatic Follicular Thyroid Cancer
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer is usually treated with a combination of surgery and radioactive iodine (RAI). RAI is generally reported to reach its maximal effect in 6–12 months but relatively little is known regarding the long-term duration of benefit from RAI administration. We present a case of metastatic follicular thyroid cancer where RAI has continued to show clinical benefit after 43 months.
Medical record review of a patient with metastatic follicular thyroid cancer.
A 52 year old woman had a left thyroid lobectomy in 1990 for an apparently benign colloid nodule. In 2007 she presented with progressive left hip pain. MRI revealed sacral and iliac tumors. A biopsy of the sacral lesion revealed follicular thyroid cancer, staining for TTF-1. Serum thyroglobulin (Tg) was 2193ng/ml with no interfering antibodies and suppressed TSH. Completion thyroidectomy revealed only a 2mm focus of carcinoma in the right thyroid lobe. She received 200mCi of RAI after recombinant TSH preparation. Post-treatment scan revealed foci of uptake in bilateral lungs and multiple bone lesions. She also received external beam radiation to the sacral disease with effective pain control. Six months later, her Tg was 205ng/ml on TSH suppression and rose to 885ng/ml after Thyrogen; she received another 200mCi of RAI. Post-treatment scan again revealed uptake in the lungs, and multiple bony lesions. Subsequently, her Tg has continued to decline. During her last visit, 43 months after her initial RAI treatment, she is asymptomatic. Her diagnostic imaging does not reveal any evidence of disease progression or reactivation and her serum Tg is 74.5 ng/ml.
This case demonstrates that the benefits of RAI therapy may be very durable, even in cases of widely metastatic thyroid cancer. This suggests that in clinically stable patients who have declining Tg after RAI, further treatment can be deferred since RAI may continued to provide benefit.
Simultaneous Medullary (MTC) and Papillary (PTC) Thyroid Cancer. Cancer Stem Cell Prototype or Coexistence?
Thyroid Cancer Saturday Poster Clinical
We describe a case of simultaneous MTC and PTC in the same thyroid lobe in a man without RET proto-oncogene mutation or history of familial thyroid cancer.
66 year-old man had a chest CT that incidentally revealed a right thyroid nodule. Neck US confirmed a 3.9 cm solid nodule. FNA was suspicious for malignancy. Patient underwent right hemithyroidectomy. Frozen section was benign, however final pathology showed a focus of papillary microcarcinoma. Completion thyroidectomy was performed and revealed a 9 mm MTC and 2 very close foci of PTC, 2.5 and 0.5 mm. He underwent RAI ablation for his PTC. Metastatic survey showed 3 foci of increased uptake consistent with bilateral cervical and upper mediastinal lymph nodes. 6 months later, neck US showed abnormal appearing lymph nodes in same areas. FNA of these lymph nodes was consistent with MTC. Calcitonin was 104 pg/ml while thyroglobulin was undetectable. Patient underwent central and left modified radical neck dissection. Pathology revealed MTC in left neck lymph nodes with extranodal extension. No PTC was identified. Calcitonin level decreased to 11 pg/ml. Patient had no family history of endocrine disorders. He had negative biochemical tests for pheochromocytoma and normal calcium level. Genetic testing was negative for mutations in RET proto-oncogene associated with MEN-2 and FMTC.
MTC derives from parafollicular C cells, originated from ectoderm. PTC derives from follicular cells of endoderm. Coexistent MTC and PTC are described in the literature in 3 scenarios: i) foci of MTC and PTC, separated by normal thyroid tissue, ii) collision tumor (MTC and PTC merge with each other) and iii) true mixed medullary-follicular derived carcinomas (intermixed). In our case, the presence RAI uptake in areas of MTC may be consistent with scenario iii). To date, there are no clear pathways of common pathogenesis for MTC and PTC. Various hypotheses have been proposed. Some suggest these mixed carcinomas may originate from a common cancer stem cell (CSC).
Coexistence of PTC/MTC is rare but interesting phenomenon that needs further investigation. We are pursuing marker-expression profiling to determine the existence of CSC-like cells in MTC RET proto-oncogene independent.
The Clinical Feature of Papillary Thyroid Cancer Patients with Hashimoto's Thyroiditis in an Area with High Prevalence of Hashimoto's Disease
Thyroid Cancer Saturday Poster Clinical
HT is the most common inflammatory thyroid disease with a high prevalence in Chinese population. The relationship between HT and PTC had been studied over decades. Some clinical risk factors had been identified in HT patients who have a PTC simultaneously, but results were inconsistence.
6019 patientstreated in a university-based tertiary care cancer hospital over a 3 year period were included in this study. All patients were grouped based on the final diagnosis. Several clinical features, such as age, gender, nodular size, invasion, central compartment lymph node metastasis (CLNM) and serum TSH level, were compared between different groups. Univariate and multivariate logistic regression analysis were employed to identify whether HT or other features can be defined as risk factors of PTC.
Overall, there were 2821 patients had a final diagnose as PTC. In other 3288 patients who were diagnosed as benign nodule (BN), 653 HT patients had been found. Generally, more PTC patients were found in patients with HT (381/653, 58.3%) than those without HT (2416/5456, 44.3%, p<0.05). In HT group, patients with co-exist PTC had younger age, female gender, smaller nodular and higher TSH level compared to HT patients without PTC. Univariate and multivariate logistic regression analysis showed that presence of HT and higher TSH level were risk factors of diagnosing PTC, on the other hand older age (>45 years old) and larger nodular size (>1cm) played a protect role. Authors also found that, in PTC patients, presence of HT or other BN was a protective factor of CLNM, while TSH level failed to present any positive or negative effects.
According results of our study, a rigorous surveillance should be taken preoperatively in HT patients, especially when higher TSH level, younger age, female gender and smaller nodular were identified at the same time. A prospective and multi-center research with long-term follow up may provide crucial evidence to clarify risk factors of PTC in patients with HT and true relationship between HT and PTC.
Clinic Neo- Style, Tirana, Albania
Thyroid Cancer Saturday Poster Clinical
Objectives: To detect thyroid nodules in patients with Graves' disease and to evaluate the risk of carcinoma.
Methods: The study group included four patient with Graves' hyperthyroidism and cold nodule in scintigraphic image.
Results: From January 2011 to June 2011 we studied four cases with Cold nodules and Graves' disease, from which three cases was underwent thyroidectomiy in euthyroid stade. All the cases were present in hyperthyroid stade, the TSH was suppressed (mean serum values 0.01 mUI/l radioimmunoassay and elevated serum values of FT3 and FT4. The diagnosis of Graves' disease was based on history, signs of hyperthyroidism, and the commonly accepted laboratory criteria. High serum concentrations of TRAb antibodies were found at the time of diagnosis (mean values 13.5±15.31 mUI/l (normal values<1). The scintigraphic image showed a cold area in all four cases from which three with one cold area and one with two cold areas. All the nodules were palpable >1 cm (average volume 18.5 cm±17.2 cm). Thyroid ultrasonography was done for all patients at the time of admission. One of three cases have Graves' exophtalmus. From four cases only two have performed FNA Cytologic evalution, in both cases the result was negative for carcinoma. Three cases was underwent thyroidectomy, from which in two cases the histological diagnosis of cold nodules were papillary thyroid carcinoma.
Conclusion: Due to high risk of thyroid carcinoma in cold nodules in Graves' disease the near total thyroidectomy is the best treatment, but we need to evaluate more cases with these diagnoses.
General Surgery, The Catholic University of Korea, Daejeon St.Mary's Hospital, Daejeon, Republic of Korea
Thyroid Cancer Saturday Poster Clinical
Because of the increased use of ultrasonography (US) and fine-needle aspiration (FNA), the incidence of papillary thyroid microcarcinoma (PTMC) has been rising. We examined the clinicopathologic features of PTMCs according to the tumor size. We thought that if there was any clinicopathologic difference on the basis of the tumor size of PTMC, we could administer less aggressive treatment to the group of patients who have less aggressive PTMC.
Between January 2007 and June 2009, a total of 275 patients with PTMCs underwent surgery. Clinicopathologic features of patients with PTMCs ≤5 mm and those with PTMCs >5 mm but ≤7 mm: capsule invasion was more frequent in the patients with PTMCs >5 mm but ≤7 mm (p=0.045). However, the other clinicopathologic features (including age, sex,extrathyroidal extension, bilaterality, multifocality, surgery type) showed no statistically significant differences for the two groups. They were divided into two groups. Group I included patients with tumors ≤7mm, and group II included those with tumors >7mm but ≤10mm. We compared the two groups' clinicopathologic features.
Total thyroidectomy was more often performed in group II (p=0.003). Central lymph node metastases were identified in 30.6% of the patients in group I and in 47.8% of the patients in group II (p=0.005). A statistically significant difference between the two groups was also found for capsule invasion (p<0.0001), extrathyroidal extension (p=0.005), and lymphovascular invasion (p=0.025). On the multivariate analysis, only central lymph node metastasis showed statistical significance in regard to tumor size (p<0.05).
A PTMC ≤7mm is less likely to have aggressive features, including central lymph node metastasis, capsule invasion, extrathyroidal extension, and lymphovascular invasion, than a PTMC >7mm. Because the agressiveness of PTMC was found mainly in the patients with tumors >7mm, we think that a cutoff value of 7mm may be considered the threshold of aggressiveness of PTMCs.
Relationship Between Multiple Intrathyroidal Primary Lesions and Neck Lymph Node Involvement in Patients with Papillary Thyroid Cancer
Thyroid Cancer Saturday Poster Clinical
There are few studies investigating the relationship between multiple intrathyroidal primary lesions and neck lymph node involvement in patients with papillary thyroid cancer. The objective of this study is to determine the relationship between multiple intrathyroidal primary lesions and neck lymph node involvement in patients with papillary thyroid cancer.
A systematic retrospective study of 2034 patients presenting with papillary thyroid carcinoma from 2007 to 2009 at a university-based tertiary cancer hospital was conducted. The effects of the independent variables of sex, age at diagnosis, tumor size, subtype of papillary thyroid cancer, and presence of multiple intrathyroidal primary lesions on the risk of the neck lymph node involvement in papillary thyroid cancer were determined.
Of the total study population, 1540 (75.72%) patients had only one cancer lesion in the thyroid, while 494 (24.28%) patients had the multiple intrathyroidal primary lesions. The presence of multiple intrathyroidal primary lesions was a risk factor for level VI lymph node involvement (OR 8.656; 95% CI 6.441–11.633) and for lateral neck lymph node involvement (OR 4.364; 95% CI 3.484–5.476) in patients with papillary thyroid cancer.
The presence of multiple intrathyroidal primary lesions is a risk factor for neck lymph node involvement in patients with papillary thyroid cancer. We suggest that patients with papillary thyroid cancer and multiple intrathyroidal primary lesions should be given routine prophylactic level VI dissection, and when these patients have a clinical suspicion of lateral neck metastases, level V should be included in the neck dissection.
Dermatology, Chaim Sheba Medical Center, Ramat Gan, Israel
Thyroid Hormone Action Saturday Poster Basic
Different elements of the hypothalamic-pituitary-thyroid hormone axis have been found to be implicated in the normal physiology of the human skin. Their effects on wound healing and hair growth in rats have previously been described.
This study utilized a guinea pig model of wound healing to assess the effect of different doses of topical T3 (3,3′,5-Triiodo-L-thyronine) and recombinant human thyroid stimulating hormone (TSH) on wound healing. Because of the close homology between the thyroid hormone receptors in humans and guinea pigs we presumed the results would be more pertinent to the wound healing process in humans. The wounds were dressed every other day for seven days during which clinical measurements of the wounded areas were performed. Histological examination was performed at the end of the study.
Application of high and low concentration of topical T3 but not TSH demonstrated a significant dose-dependent reduction in the wound surface area through a process of contraction. The significant histological finding of treatment with high dose T3 was apparent mainly in the hair follicle count.
Topical T3 enhances wound healing in the guinea pig model, primarily by wound contraction. Since this is a critical stage in chronic ulcer healing, topical T3 may be useful in the process when utilized in clinical settings.
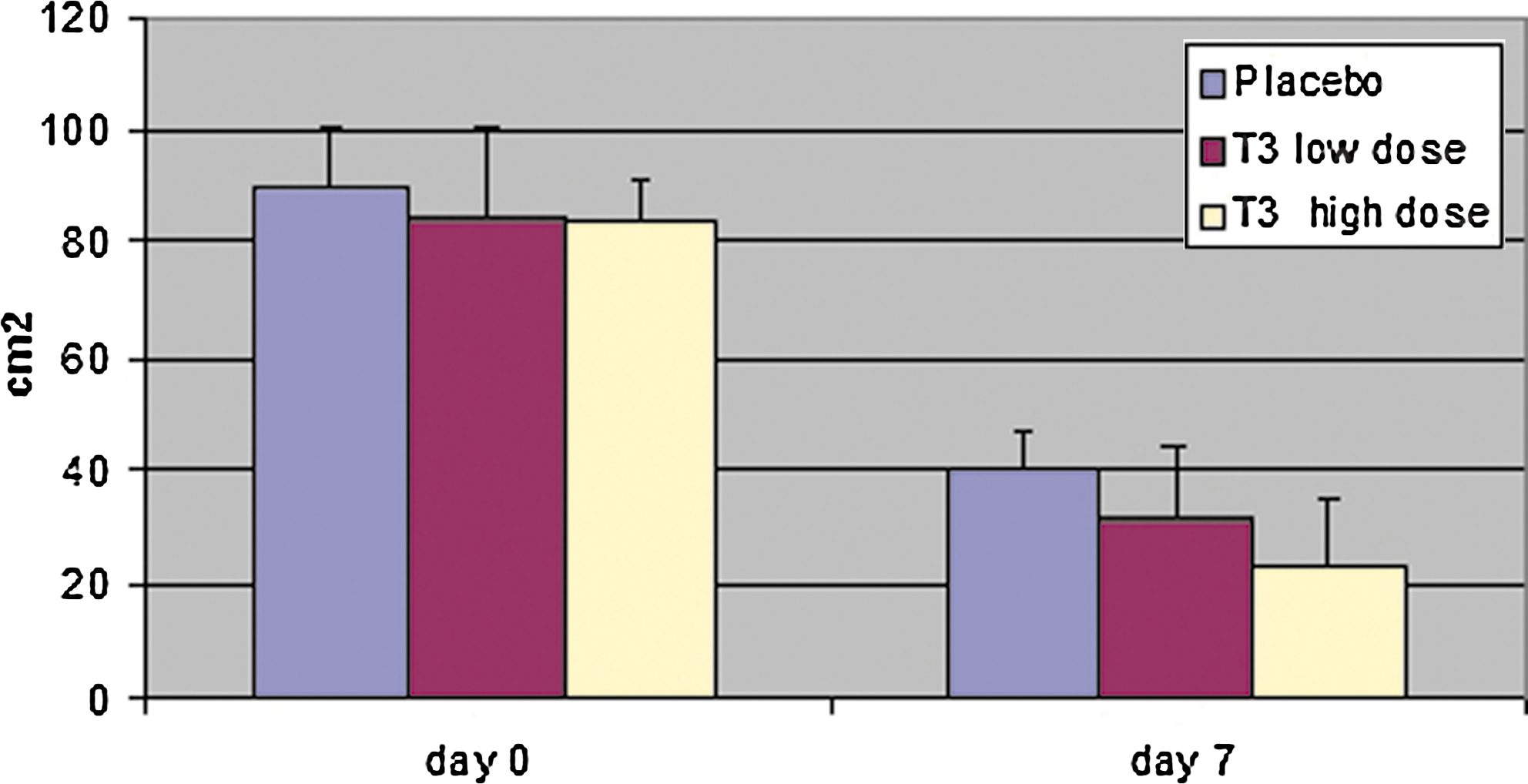
Medicine, Oregon Health & Science University, Portland, OR
Thyroid Hormone Action Saturday Poster Clinical
Patients with overt thyroid disease have alterations in metabolic function, but it is not clear whether variations in thyroid function within the normal range affect metabolism.
To address this, we recruited 67 otherwise healthy age- and BMI-matched women with either no thyroid disease (N=14) or who were receiving levothyroxine (L-T4) for hypothyroidism (N=53). All subjects had normal TSH levels. Subjects underwent measurements of Resting Energy Expenditure (REE), respiratory quotient (RQ), and Thermic Effect of Food (TEF) by indirect calorimetry, and body composition by DEXA. Subjects were divided into two groups: Low-normal TSH (0.42–2.49 mU/L, N=45) and High-normal TSH (2.50–4.87 mU/L, N=22).
Groups differed by TSH as expected. Using a regression model with adjustment for age and BMI as appropriate, there were no differences in any metabolic measures between the two groups (see table). By correlation analysis, log free T3 was directly related to REE (Pcorr=0.36, p<0.005) and % body fat (Pcorr=0.40, p<0.001), while log free T4 was inversely related to TEF (Pcorr=− 0.29, p=0.02) and lean body mass (Pcorr=−0.22, p=0.08). Inclusion of only subjects receiving L-T4 did not substantially alter the results.
Results are means±S.E.M. except for thyroid hormones, which are medians and ranges.
p<0.0001compared to low-normal TSH group.
Utilizing sensitive techniques, there were no differences in measures of energy metabolism, nutrient oxidation, or body composition between subjects with high-normal and low-normal TSH levels. However, associations between free T4/T3 and some of these measures suggest that small variations in thyroid function within the normal range may have a small effect on metabolic function. Further study is required to determine if these effects are of clinical significance.
Thyroid Hormone Metabolism and Regulation Saturday Poster Clinical
Herbal medications are being increasingly used to treat serious medical conditions as well as for health maintenance. Since they do not require approval from the Food and Drug Administration and are essentially unregulated, their interaction with other medications and consequent adverse effects often go unrecognized.
Ten years of clinical and laboratory data from a patient with prostate cancer using a variety of herbal preparations purported to improve his prostate health was analyzed. The medical literature was reviewed for evidence of direct and indirect effects of these herbal preparations.
In a patient who had been treated with I-131 for Graves' disease 30 years earlier who had been stable on 150 micrograms of l-thyroxine, PC-SPES and similar herbal preparations caused a 33% increase in the dose required to normalize his thyrotropin levels. The proximate cause of this disruption in thyroid hormone economy is likely to be the estrogen-like effects on thyroxine binding globulin by components of these preparations. Similar estrogenic effects were seen in other binding proteins and HDL- cholesterol. Koch's postulate is fulfilled in his clinical course.
Physicians should carefully question patients about the use of non-prescription drugs and, in particular, herbal preparations. Herbal preparations through their estrogenic effects can disrupt thyroid hormone economy in patients dependent on l- thyroxine and may confound interpretation of other hormones such as testosterone and cortisol through their effects on binding proteins.
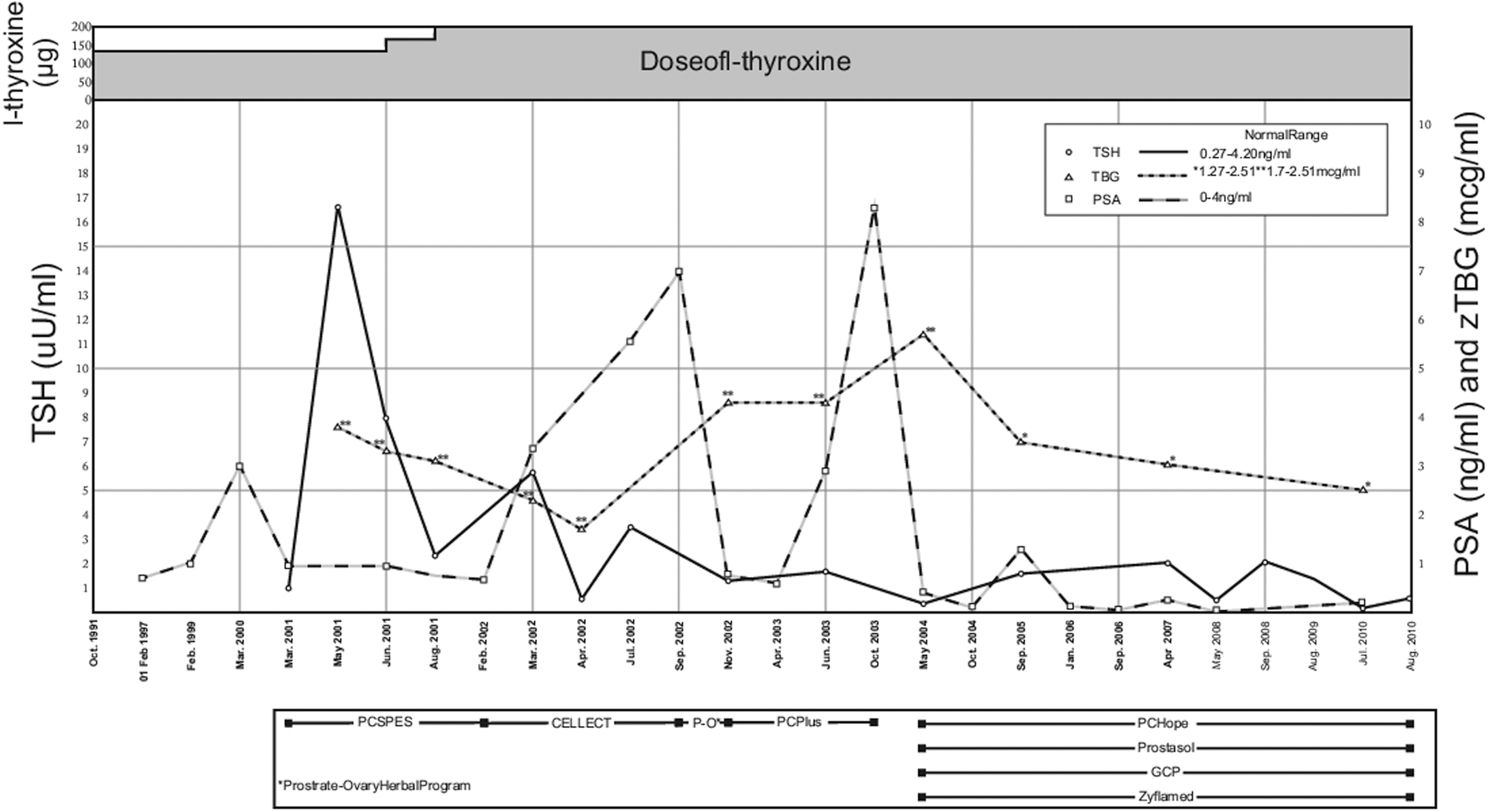
Changes in thyroid economy over time.
Thyroid Imaging Saturday Poster Clinical
Patient is a 74 year-old female who presented to our clinic in September 2010 for hypercalcemia. She had an elevation of her serum calcium level dating back to 2005 in the EMR (10.9 mg/dL). Past medical was negative. She was not taking any medications.
On initial presentation in September 2010, the patient complained of bone pain and leg cramps. Physical exam was normal. She denied being on HCTZ or Lithium. No history of kidney stones. Her serum calcium was 11.5 mg/dL (8.2–10.4 mg/dL) and PTH was 60 pg/mL (10–65 pg/mL). Her 25-OH vitamin D level was 26 ng/mL and a DXA was normal. A decision was made to send the patient for 99mTc sestamibi parathyroid scan. It was normal. The patient then had a thyroid ultrasound in December, which showed a 1.2 cm nodule on the right, inferior to the thyroid gland and a 1.6 cm nodule on the left, inferior to the thyroid gland.
At this time, referral was made to a head and neck surgeon, who recommended CT scan of the neck. The results showed a heterogeneous ovoid soft tissue density, 2.5 cm below the inferior aspect of the right thyroid lobe suspicious for a mediastinal parathyroid adenoma. The decision was then made by the patient and surgeon to undergo surgical exploration. She was found to have a left superior parathyroid adenoma, which was removed. PTH levels dropped intraoperatively from 55 to 29 pg/mL. The heterogeneous ovoid soft tissue seen on CT scan was found to be a benign lymph node. The patient's labs returned to normal range, and her symptoms resolved post-operatively.
99mTc sestamibi parathyroid scans are reported to have a 50–70% sensitivity in pre-operative localization of a parathyroid adenoma. It is interesting to note that some studies found that the false negative rate of sestamibi scan correlated with PTH levels: the lower the level, the more likely a false negative (1). Other recent studies have shown that younger patients, higher levels of PTH, and lack of thyroid nodules correlate with overall sensitivity of the scan (2). The false-negative result of our patient's 99mTc sestamibi parathyroid scan can possibly be explained by her older age and relatively lower PTH levels. Further studies are needed to elucidate other causes of false-negative scans.
Nuclear Medicine, Medical University of Bialystok, Bialystok, Poland
Thyroid Nodules and Goiter Saturday Poster Clinical
The aim of our study was to evaluate the short term effect of radioiodine therapy on the achievement of euthyroidism, and prevention of adverse effects on the cardiovascular and skeletal systems and prevention evolvement to overt hyperthyroidism in patient with subclinical hyperthyroidism.
We treated 740 patients, aged 18–78 years, 86% of the studied groups were female and 14% male; 28% of the patients with multinodular goitre (MNG), and 72% of the patients with autonomous nodule (ATN). Malignant changes were excluded in all nodules by fine needle aspiration biopsy. All the patients had serum TSH levels less than 0.1 mU/l and effective half life measured by the use of T24 and T48 was more than 3 days at the time of treatment. The activity dose was calculated by the use of Marinelli's formula and ranged between 200–600 MBq. The absorbed dose (Gy) for MNG ranged between 160 and 260, and for ATN: 200–300. Follow up control was done every 6 weeks in the first year.
In general the success of treatment after one year was: 99% of patient with ATN and 92% of patient with MNG achieved euthyroidism. 1% of patient with ATN and 7% of patient with MNG develop hypothyroidism. 1% of the patients had persistent hyperthyroidism and received second dose of radioiodine therapy. In all the patients the symptoms and signs of subclinical hyperthyroidism disappeared (palpitation, tachycardia, atrial fibrillation, exercise tolerance improved, the blood pressure normalised and the quality of life improved).
The achievement of euthyroidism and the remission of the symptoms and signs of subclinical hyperthyroidism, were due to good diagnosis, well preparation of the patients; accurate measurement of administered activity, effective half-life, and well-organised follow up.
Insufficient Fine Needle Aspiration of Thyroid Nodules at a Tertiary Center: Risk Factors and Management
Thyroid Nodules and Goiter Saturday Poster Clinical
There is scant data in the literature concerning factors that affect the adequacy of thyroid fine needle aspiration (FNA). The goals of this study were to (1) analyze factors associated with insufficient FNA, and (2) to propose an appropriate management algorithm for insufficient FNA samples.
Data of 1000 ultrasound-guided surgeon-performed FNAs (UGSPF) were reviewed from a prospectively-collected database at a single institution from 2000 to 2010. Of these, 56 were reported as insufficient, while 43 were referred-in with an initial prior FNA reported as insufficient. Age, gender, BMI, nodule size and composition, surgeon experience, FNA technique, final histology, and subsequent management were recorded.
On univariate analysis, nodule composition, surgeon experience, and FNA technique all showed a significant correlation with insufficient versus diagnostic UGSPF. On multivariable analysis, only FNA technique remained a significant factor. Of nodules with insufficient UGSPF, 46% had repeat FNA (yielding a diagnosis in 81%), 23% underwent surgery due to concerning features, 21% with hypocellular features were followed without change, while 9% were lost to follow-up. All nodules with insufficient FNA referred-in underwent repeat UGSPF, which yielded a diagnosis in 93.1%. Due to concerning repeat FNA results, 56% of these nodules were operated on. Half of nodules with benign repeat FNA ultimately had surgery due to other concerning US or clinical features, while the other half with hypocellular features were observed without change. If nodules observed and remaining stable were included, the malignancy rate was 27.9% for those nodules referred-in with insufficient FNA, and 8.9% for those with insufficient UGSPF (p<0.05).
Our results suggest that FNA technique may contribute to insufficient UGSPF and that nodules referred to a tertiary center should be managed with repeat FNA due to a higher risk of malignancy. Surgery should be strongly considered for those with concerning features. A diagnostic result can be achieved for the majority of nodules with initial insufficient FNA, and individual risk assessment achieves safe triage to surgery versus follow-up.
Veracyte, Inc., South San Francisco, CA
Thyroid Nodules and Goiter Saturday Poster Clinical
The Afirma® Gene Expression Classifier analyzes thyroid fine needle aspirates (FNA) with indeterminate cytopathology. In earlier studies, the classifier was able to accurately determine a benign genomic profile with >95% accuracy. However, test performance and its impact on physician decisions in clinical practice have not been reported.
Indeterminate nodules were defined as not benign, malignant or nondiagnostic. After nucleic acid purification and amplification, microarray analysis of mRNA expression of 142 genes in multiple biological pathways were reported using a proprietary algorithm. A web and mail-based survey was sent to physicians with benign Afirma results, to assess whether they recommended surgery or clinical/sonographic follow-up.
FNAs (N=1600) were consecutively tested, 1475 from 85 community and 125 from 10 academic physicians. Of the 1475 FNAs, 70% were benign, 1% malignant, 15% indeterminate and 14% nondiagnostic. RNA was inadequate for 9% of the indeterminate FNAs, all of which had AUS/FLUS cytology. For the remaining 299 indeterminate samples, 53% were classified as benign and 47% suspicious. The survey was completed by 17 of 47 physicians (36%). 41.5% recommended watchful waiting in 100% of their patients, 41.5% in 81–99%, and 17% in 21–40% with a mean of 89%.
Based on the test specificity reported previously, and a 34% risk of malignancy in indeterminate FNAs, we predicted the classifier result to be benign in approximately 50% of cases. This prediction has now been accurately reflected in actual experience. Almost half (47%) of the diagnostic thyroidectomies on cytologically indeterminate nodules could potentially be avoided, as 53% of the time the classifier results in a benign gene expression profile, and 89% of the time physicians recommend watchful waiting.
Physician Decision Survey Results.
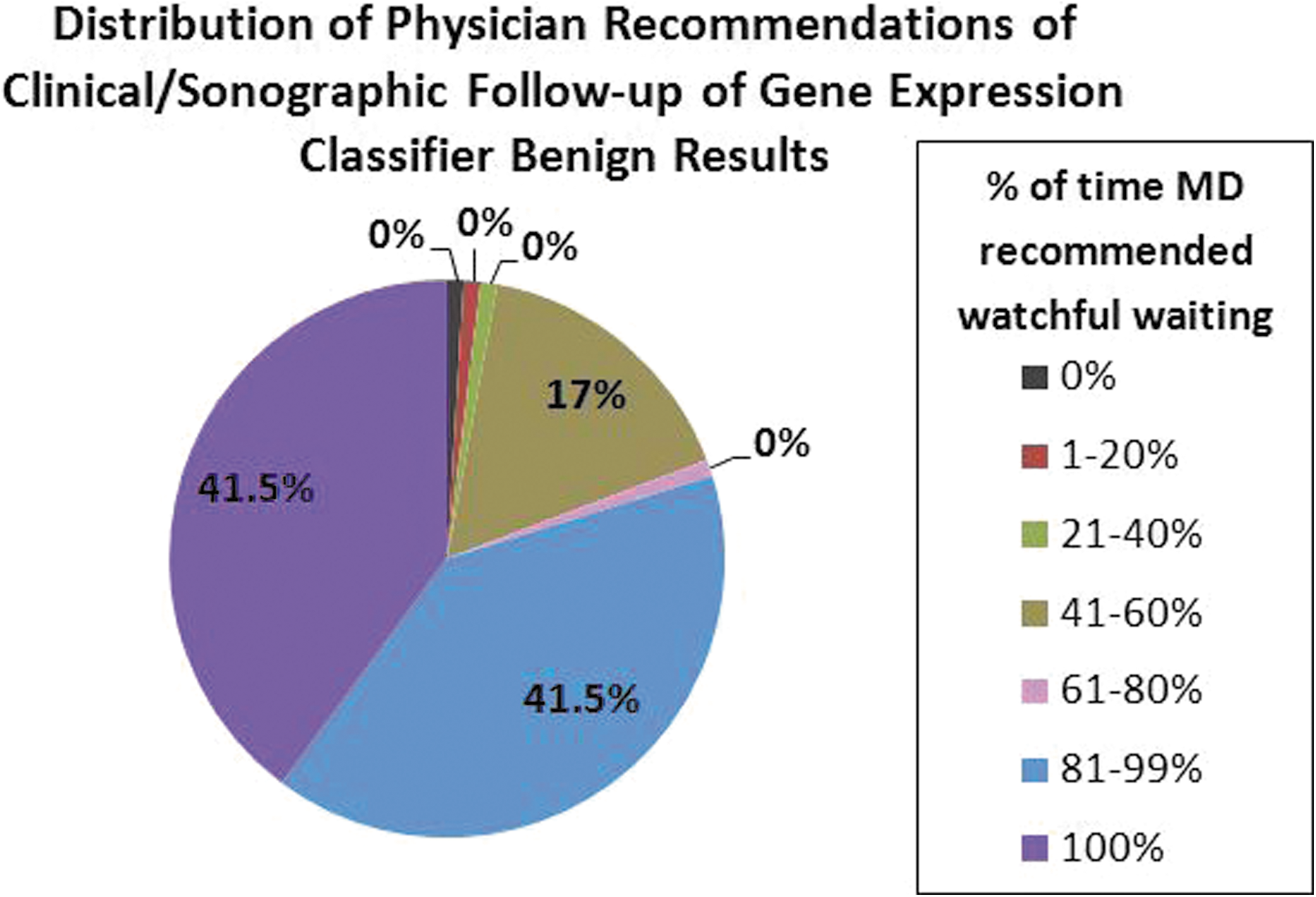
How to Increase Radioiodine Uptake in Multinodular Goiters by Using Metil Mercapto Imidazole
Thyroid Nodules and Goiter Saturday Poster Clinical
MNG usually has a low and heterogeneous radioiodine uptake (RU). Recombinant human (rh) TSH and a new modified release rhTSH formulation have shown to increase the thyroid RU in this setting. Objective: To demonstrate the effect of the administration of metil-mercapto-imidazole (MMI) to increase RAI uptake in patients with MNG and to evaluate the outcome of the goiter size 12 months after 131-I administration.
Eight female patients (mean age 72±4 years old) were prospectively included. Baseline characteristics of included patients can be observed in Table 1. Each included patient had a baseline thyroid profile, and thyroid RU (measured at 24 hours after 30 μCi 131-I administration) and a CT. MMI was prescribed 30 mg b/d. When TSH level was around 5 mUI/L, a new RU was performed and 1.11 Mbq 131-I was then indicated.
Baseline Characteristics of Patients with Multinodular Goiter Included in the Protocol
RU: Radioiodine Uptake; RAI: Radioiodine; Denial (for surgery); DBT: Diabetes; COPD: Chronic Obstructive Pulmonary Disease
Mean baseline RU at 24 hours was 20±8.9%, which increased to 48±16.8% (p<0.001) after the protocol (Mean time for achieving the expected TSH level was 6.6±2.6 months; range 3 to 12 months). Follow-up was 24.8±14.6 months. Untoward effects after RAI were: local pain in two cases (in one of them with a notable increase in goiter size). The pain relieved after 48 hours. Outcome in thyroid function: In 4 patients hypothyroidism was observed 3.5±3.7 months after RAI treatment. One patient developed a Graves' disease and 3 of them still remain euthyroid. Outcome in thyroid size: We observed a decrease of the MNG size, measured by tracheal cross sectional area (TCSA). Baseline TCSA was 191±55.3 mm2. It increased to 296±63.3 mm2 (p=0.02) after 12 months of follow-up in 6 of the 12 included patients. All subjects also referred a subjective amelioration of compressive symptoms.
Although it is impossible to predict the time when TSH will achieve the needed level for administering the radioiodine dose, this protocol seems to be an efficacious alternative to increase RU in patients with MNG in whom surgery is contraindicated or not accepted, while we wait for the approval of rhTSH for this indication.
Thyroid Nodules and Goiter Saturday Poster Clinical
Intrathyroidal ectopic thymomas are rare clinical entities and may be difficult to identify. Most affected patients present an apparent thyroid nodule that is clearly identified through imaging or during the clinical examination. Very often, results of FNAB prove misleading or indeterminate. The correct diagnosis requires a high index of clinical suspicion along with histological assessment and appropriate staining.
Case report: A 27 year old male presented with a 1 cm thyroid nodule on the isthmus; a fine needle aspiration biopsy showed a tumor of poorly differentiated small cells, which was suggestive of insular carcinoma, medullar carcinoma or metastatic cancer. A total thyroidectomy was performed and an intrathyroidal thymoma, a very unusual diagnosis, was confirmed by pathologic examination and immunohistochemistry (immunohistochemical staining of the small cells in the ndolue was performed with chromogranins, synaptophysin, a cytokeratin cocktail, thyroglobulin and a common leukocyte antigen to determine if they were lymphoid or thyroidal in origin. The positive staining for CD45, CD3 and CD20 demonstrated lymphoid cells of T and B lineages; the cocktail of cytokeratins was positive in epithelial cells, while staining for thyroglobulin, chromogranins and synaptophysin was negative) The patient was treated with a supplementary dose of levothyroxine; the follow-up 12 months after did not show evidence of recurrence or metastasis.
We present the case of a patient with intrathyroidal thymoma, an uncommon location for this tumor, especially in males. The patient`s evolution has been benign, with no evidence of metastasis or recurrence during 12 months of follow-up. Unfortunately, there are no clinical signs, laboratory tests or imaging studies that suggest the diagnosis of an intrathyroidal thymoma, and in all cases the final diagnosis is made by histopathology. Thus, intrathyroidal thymoma should be kept in mind in the differential diagnosis of a thyroid nodule, thyroid cancer and thyroid lymphomas.
The positive staining for CD45, CD3 and CD20 demonstrated lymphoid cells of T and B lineages; the cocktail of cytokeratins was positive in epithelial cells, while staining for thyroglobulin, chromogranins and synaptophysin was negative.
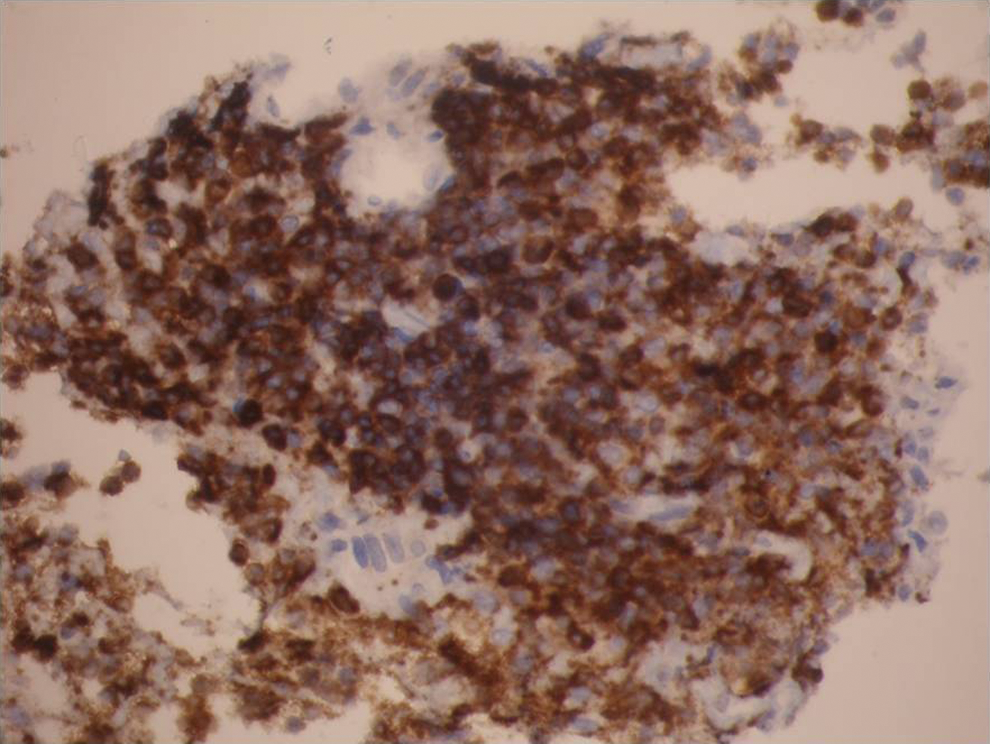
Safety of Thyroid and Parathyroid Surgery on Clopidogrel
Thyroid Nodules and Goiter Saturday Poster
Clopidogrel (Plavix) is widely prescribed to prevent stent thrombosis after percutaneous coronary intervention and current American College of Cardiology guidelines recommend 12 months of uninterrupted therapy. There is no data on the risk of hemorrhagic complication of parathyroid and thyroid surgery in patients taking Clopidrogrel. Our aim was to determine the safety of thyroid and parathyroid surgery on clopidogrel.
Medical records of patients taking clopidogrel and having thyroid or parathyroid surgery between 2005 and 2010 were retrospectively reviewed to determine incidence of hemorrhagic complications.
Twenty-five patients were identified. Indication for clopidogrel included coronary stent (N=21), carotid stent (N=1), and other indications (N=3). Operations included parathyroidectomy (N=13), thyroid lobectomy (N=7), and total thyroidectomy (N=6). Of the 25 patients taking clopidogrel, 11 continued taking clopidogrel through surgery, 11 held clopidogrel for less than 1 week prior to surgery and resumed the day after, and 3 held clopidogrel for more than 1 week. None of the 25 patients had postoperative hemorrhagic complications. One patient who did not discontinue his clopidogrel developed a postoperative seroma requiring multiple aspirations.
Thyroidectomy and parathyroidectomy in patients on clopidogrel does not appear to carry a prohibitively high risk of postoperative hemorrhagic complications. The risk of hemorrhage during these elective operations should be weighed against the risk of stent thrombosis. A larger prospective study is needed to better determine the relative risk of postoperative hemorrhage during thyroid and parathyroid surgery on clopidogrel.
Teaching Recurrent Laryngeal Nerve Dissection [Early Identification and Preservation Using Nerve Monitoring and Loupe Magnification] in Head and Neck Endocrine Surgery
Thyroid Nodules and Goiter Saturday Poster Clinical
Many studies have been published showing no difference in temporary paresis or permanent paralysis of the recurrent laryngeal nerve (RLN) during thyroidectomy with or without laryngeal nerve monitoring [LNM]. Various approaches can be employed in thyroidectomy. Delivery of the gland prior to complete dissection and identification of the RLN is sometimes utilized in the absence of LNM, while identification and dissection of the RLN from the gland is more feasible in the presence of LNM. Objectives: To evaluate teaching RLN dissection technique to residents as primary surgeons [using loupes and nerve monitoring] for postoperative morbidity in head and neck endocrine surgery.
In 101 consecutive thyroidectomies we have modified our technique to teach our residents consistent early identification of the RLN in the paratracheal region by direct visualization [loupe magnification] and nerve stimulation. The thyroid lobe is identified then dissected away from the nerve, as in a parotidectomy, using combined magnification and nerve monitoring [similar to description by Randolph et al, Laryngoscope supplement, Jan. 2011]. All patients had preoperative fiberoptic laryngoscopy and a repeat laryngoscopy one week after surgery. Presence or absence of true vocal fold paralysis/paresis was documented.
119 surgical procedures were available for study; two patients were excluded (one with preoperative vocal fold paralysis and one with ventilator-dependent respiratory failure). There were 20 total thyroidectomies: 15 for malignancy and 5 for benign disease; 6 substernal goiters, 1 revision thyroidectomy and 10 parathyroidectomies. One patient developed a permanent vocal fold paralysis [1/119 or .84%]. There was another patient with a vocal fold paresis which recovered in 4 weeks [1/119 or .84%].
The RLN dissection technique with early identification, dissection and preservation of the nerve using magnification combined with nerve monitoring has emerged as an important resident teaching tool.The morbidity rate is acceptable. Notably in light of the increasing rates of thyroid surgery and LNM utilization, resident physicians may benefit from exposure to this technique as a component of their training.
Abstract Author Index
Abdel-Rahim, M. P-78
Abdelrazek, S. P-84, P-241
Abdulrahman, R. P-162
Abelleira, E. P-245
Abols, A. P-210
Abraham, D. P-156
Adai, A. P-208
Adamson, L.A. P-125
Agah, R. P-30
Agcaoglu, O. P-86, P-212
Agnihothri, R. O-102
Ahluwalia, R. P-213
Ain, K.B. O-15
Akamizu, T. P-19
Akulevich, N. P-218
Al Ghuzlan, A. P-49
Al-Ansari, F. P-20
Alastrue, A. P-168
Algeciras-Schimnich, A. P-46
Allison, R. O-3
Annette, L. O-185
Arai, T. P-146, P-165
Arango-Toro, C. P-246
Arikan, E. P-121
Arnold, A.M. P-111
Arya, A. P-230
Asa, S.L. P-206
Assadi-Porter, F. P-75
Assanti, A.P. P-166
Attard, M. P-220
Auersperg, M. P-215
Auyeung, V. P-120
Avram, A.M. O-97
Aynehchi, B. P-248
Bacher, K. P-113
Bae, J. P-66, P-224, P-226
Baek, J. P-243
Baek, K. P-226
Bahn, R.S. O-185, P-186, P-193
Baker, Jr, J. P-105
Bakirci, N. P-121
Balibrea, J. P-168
Ball, D. O-3
Barank, D. P-82
Bardet, S. O-4
Barendse-Hofmann, M. O-174
Barnes, J. O-10
Barton, L. P-195
Bastie, D. O-4
Bastos, A.U. P-47
Bauer, H. P-186
Baumann, N.A. O-103
Beaudenon-Huibregtse, S.L. P-208
Beauregard-Totaro, C. P-144
Beck-Peccoz, P. P-22, P-214
Belcaro, G. P-161
Bellido Castañeda, V. P-37
Benhamou, E. O-4
Benisvy, D. O-4
Benvenga, S. P-30, P-107, P-196
Berber, E. P-86, P-148, P-153, P-212, P-242
Bernet, V. P-78
Besic, N. P-215
Bhattacharya, P. P-18
Bidart, J. P-49
Biko, J. P-218
Bischoff, L.A. P-122
Blair, E. P-73
Bliddal, S. P-32
Blomberg, M. P-58
Blount, B.C. P-121
Bodenner, D. O-3, P-216
Boelaert, K. O-6, O-13, P-40, P-41
Boelen, A. O-100
Bohacek, L. P-242
Bohinc, B.N. P-131
Boichard, A. P-49
Bommareddi, S. P-207
Bonara, P. P-22
Bonichon, F. O-4
Boonchayaanant, P. P-50
Borget, I. O-4
Boucher, A. P-144
Bourdy, S. P-219
Bournaud, C. O-4
Brandt, M.P. O-8
Braverman, L.E. O-11, O-12
Brent, G.A. P-123
Brenta, G. P-197
Bridji, B. O-4
Brierley, J.D. P-54, P-151
Brose, M.S. O-179
Broutin, S. P-49
Brown, K. P-154
Brown, R.E. P-142
Brunt, K. P-244
Brychta, R. O-102
Buchman, G. P-19
Bufalo, N.E. O-183
Burch, H.B. P-78, O-184
Burman, K. P-44, O-184
Buruju, J. P-170
Busaidy, N. P-128
Butz, D.E. P-75
Buzkova, P. P-111
Cabanillas, M. O-3, O-179
Cakal, E. P-191
Caldwell, D. P-188
Can, O. P-121
Cappola, A.R. P-111
Carhill, A. P-198
Carnaille, B. P-219
Carr, R. O-14
Carty, M. P-219
Carty, S.E. O-96
Cassol, C. P-206
Catargi, B. O-4
Cavaco, B. P-117
Ceccarelli, S. P-63
Celi, F.S. O-102
Centanni, M. O-9
Cerutti, J.M. P-47
Cetinkalp, S. P-80
Cha, B. P-226
Chae, B. P-66
Chand, G.-. P-217
Chandrasekaran, S. P-51
Chang, A.S. P-78
Chao, T. P-141
Chartoff, A. P-120
Chartrand, R. P-144
Chee, R. P-30
Chen, C. O-180
Chen, H. P-171
Chen, K.Y. O-102
Chen, L. P-132, P-209
Chen, Q. P-188
Cherenfant, J. P-28
Chernichenko, N. O-95
Chernyavsky, V. P-247
Cheryk, L.A. P-46
Chiarini, S. P-63
Chiellini, G. P-75
Chindris, A. P-53
Chng, C. P-21
Cho, B. P-140
Choi, E. P-69
Choi, Y. P-224
Choudhary, A. P-208
Chung, C. P-227
Chung, S.H. P-79
Chung, Y. P-140
Clark, O.H. P-45, P-116
Clarke, N. O-177
Clarke, S. P-143
Clyde, P.W. P-24, P-115
Coenen, M. P-186
Cohen, O. P-237
Colak Bozkurt, N. P-191
Colakoglu, B. P-225
Colao, A. P-166
Colato, C. P-149
Colin, C. P-219
Colombo, C. P-214
Contreras, C.M. P-133
Cooper, D.S. O-184
Cordes, A. P-113
Cornelli, U. P-76, P-161
Coskun, A. P-121
Costello, Jr, J. P-44
Courville, A. O-102
Couto, M.F. P-133
Covelli, D. P-22
Crapo, L.M. O-10
Crocetti, U. P-220
Crook, J. P-53
Crystal, J. P-247
Cunha, L.L. O-175
Curran, T. P-247
Currò, N. P-22
D'Agostino, M. P-130
D'Ercole, C. P-63
Damante, G. P-130
Danilova, L.I. P-71
Dardano, A. P-149
Darras, V.M. O-6
Dasari, R. P-119
David, C. P-152
David, D. P-54, P-151
Davidov, T. P-247
Davies, T.F. P-17, O-182, O-185
Davis, F.B. O-99
Davis, P. O-99
Dazzi, D. P-22, P-214
Dean, D.S. P-35
Déandréis, D. O-4, P-134
De Groot, A. P-19
De Groot, L. P-19
Dejax, C. O-4
Del Duca, S. O-9
Delgado Álvarez, E. P-37
Delibasi, T. P-191
Dellavalle, D. O-102
Del Prete, M. P-166
Del Tacca, M. P-149
Demaray, S. P-186
Demidchik, Y.E. P-71
Dettmer, M. P-126
Devi, I. P-202
De Vis, K.K. P-55
de Vries, E. O-100
Diana, T. P-25, P-108
Diehl, N. P-53
Di Rocco, G. P-63
Doherty, G.M. O-97
Dolan, B. P-154
Dolp, P. O-16
Doshi, K. P-139
Dosiou, C. O-10
Dremelj, M. P-215
Driesen, P. P-55
Drozd, V. P-71, P-218
Ducena, K. P-210
Duclos, A. P-219
Duh, Q. P-45, P-116
Dumitrescu, A.M. P-112
Dupuy, C. P-49
Duque, C. P-246
Durante, C. P-130, P-220
Duren, M. P-225
Durso, M. P-126
Duvuru, S. P-119
Dyrmishi, B. P-234
Eberhardt, N. P-150, O-178
Echeverri, C. P-246
Eckstein, A. P-104
Edeiken, B. P-90
Edinboro, C.H. P-83
Eggo, M.C. P-40
Eguchi, H. P-23
Ehrenkranz, J. O-7
El-Shunnar, S. P-56, P-135
Elbardissi, A. P-219
Elisei, R. O-3
Elizondo-Riojas, G. P-89
Ercan, O. P-160
Erdogan, M. P-80
Erovic, B.M. P-206
Evans, C. P-143
Ezzat, S. P-54, P-151
Faggiano, A. P-166
Fagin, J.A. O-5
Fahey, M. P-208
Faingold, C. P-197
Falcao-Alencar, G. O-15
Fan, Y. P-105
Fardo, D.W. O-15
Fareed, J. P-26
Farnell, K. P-143
Farris, C. O-96
Fatourechi, V. P-53
Federici, S. P-63
Federspiel, M. O-178
Feig, D. O-11
Feldmann, B. P-113
Feldt-Rasmussen, U. P-32, P-58
Fenton, M.S. P-130
Ferdeghini, M. P-149
Ferrara, A. P-160
Ferrero, S. P-214
Fig, L.M. O-97
Fileta, B.B. P-78
Filetti, S. P-130, P-220
Finco, A. P-26
Fliers, E. O-100
Fonderico, F. P-166
Fong, J.C. O-6, O-13, P-40
Fossati, P. P-197
Fowler, L.J. P-125
Frank, R. P-216
Franklyn, J.A. O-6, O-13, P-40, P-41
Freeman, J.L. P-151
Freitas, M. P-172
Freudenberg, J. O-185
Friedlander, P. O-2
Fugazzola, L. P-214
Fujimoto, K. P-38
Fukata, S. P-29
Funahashi, Y. O-3
Furukawa, T. P-221
Gafni, A. P-54
Galton, V.A. O-101
Ganly, I. O-95, P-136
Gargano, L. O-9
Gavin, V. P-32
Gazic, B. P-215
Gerhard, R. O-175
German, A. P-112
Gerrard, G. P-143
Gholve, C.S. P-163
Ghossein, R. O-5, O-95
Giannella, A. P-63
Giannelli, S. P-61, P-82
Gianoukakis, A. P-61, P-82
Gild, M. O-5
Giray, S. P-225
Glister, B.C. P-24
Godinho-Matos, M. P-117
Göke, B. O-16
Goldberg, I.J. O-7
Goldfarb, M. P-62
Goldstein, D.P. P-54, P-206
Goldust, M. P-137
Gondek, S.S. P-62
Gong, G. P-60
Gong, Y. P-90
Goodwin, T. P-195
Gopisetty, A. P-18
Gorska, M. P-84, P-241
Gosnell, J. P-45, P-116
Granada, M. P-168
Grant, W. P-199
Grebe, S. P-46, P-150
Greene, L.W. P-138
Gregersen, P. O-185
Grewal, R. P-134
Grilli, P. P-63
Grogan, R.H. P-45
Grove, A. P-240
Grubbs, E.G. P-128
Gruber, H. P-188
Gruenwald, G.K. O-16
Grussendorf, M. P-113
Guastella, C. P-22
Gupta, M. P-139
Gurfinkiel, M. P-197
Gusev, Y. P-154
Gutierrez, A. P-198
Hackshaw, A. P-143
Hale, K.S. P-128
Harari, A. P-116
Harmer, C. P-143
Harper, W. P-27
Harrison, B. P-143
Hartoft-Nielsen, M. P-32
Hartsfield, J.K. O-15
Hasturk, H. P-158
Haugen, B.R. O-176
Haughey, D. P-75
Haviland, J. P-75
Hawkins, R. P-116
He, M. O-93
He, X. O-11, O-12
Heller, K.S. O-94
Hennessey, J.V. P-200
Hercbergs, A. O-99
Hernandez, A. O-101
Hernandez, G. P-195
Hernandez-Coria, M.I. P-89
Hernández-P, A. P-74
Hershman, J.M. P-130
Hesham, S. P-56, P-135
Hiromatsu, Y. P-23
Hirsch, C.H. P-111
Ho, S. P-21
Ho, T. P-141
Hoang, T.D. P-24, P-115
Hobbs, J.A. P-125
Hodak, S.P. O-96
Hofflich, H.L. P-240
Hong, S. P-60
Hoschar, A. P-169
Hosseini, M. P-73
Hovens, G.C. P-162
Hseuh, C. P-141
Huang, B. P-141
Huang, C. P-64, P-236
Huang, L. O-7
Huang, T. O-92, P-106
Huggins, L.A. O-7
Humm, J.L. P-134
Hunt, J.P. P-156
Hurley, R. P-150
Hwang, S. P-109, P-189
Hyer, S. P-143
Ibhazehiebo, K. P-204
Ibrahimpasic, T. O-95
Ichihara, A. P-221
Im, S. P-224
Imam, S. P-232
Inaba, H. P-19
Inabnet, W.B. P-167
Inal, T. P-121
Inman, A. P-27
Irish, J.C. P-206
Ishizuka, K. O-98
Isozaki, O. P-221
Ituarte, P. P-116
Iwaki, H. P-87, O-98, P-114
Iwama, S. P-34
Iwasaki, T. P-204
Iyer, S. P-186
Jahreis, K. O-12
Jain, M. P-207
Jain, S. P-230
Jarjoura, D. P-43
Jarzab, B. O-3
Jaume, J.C. P-232
Jebasingh, F.K. P-202
Jee, Y. P-227
Jensen, K. P-44
Jhiang, S.M. O-8
Ji, Q. P-64, P-129, P-233, P-236
Jimenez, C. P-90, P-91
Jimeno, A. O-176
Johnson, K. P-104
Johnson, S. P-143
Jones, G.N. P-43
Joo Hee, K. P-222
Joshi, K.B. P-163
Joshi, M. P-81, P-203
Julian, M. P-168
Jung, C. P-224
Jung, E. P-223, P-224
Jung, S. P-66, P-226
Kabaker, A.S. O-96
Kadowaki, T. O-3
Kahaly, G.J. P-25, P-108, O-181, P-187, P-190
Kaku, H. P-23
Kandil, E. O-2, P-173
Kane, M. O-176
Kang, C. P-224
Kang, G.Y. P-78
Kang, M. P-226
Kang, Y. P-224
Kanitz, M. P-25, P-108, O-181, P-187, P-190
Kansopon, J. P-45
Kantarci, A. P-158
Kapia, M. P-234
Karatas, A. P-225
Karbek, B. P-191
Karmarkar, M.G. P-203
Kassem, R. P-237
Katz, P.M. O-11
Kazaure, H.S. P-65
Kebebew, E. O-93, P-207, P-229
Kelestimur, F. P-121
Kennedy, G.C. P-244
Kethman, W. O-2, P-173
Khan, S. P-39
Khoo, D. P-21
Kim, D. P-109, P-206
Kim, E. P-60, P-110
Kim, I. P-70
Kim, J. P-66, P-127, O-181, P-187
Kim, K. P-109
Kim, K.H. P-158
Kim, M. P-226
Kim, S. P-66, P-68
Kim, T. P-60, P-110
Kim, W. P-60, P-69, P-110
Kim, Y. P-243
King, B. O-103
Kirschner, L.S. O-8, P-43
Kitano, M. P-207
Kjaer, S.K. P-58
Klasen, R. O-181, P-187
Klee, G.G. O-103
Klefter, O. P-32
Klopper, J. O-176
Klose, M. P-32
Klubo-Gwiezdzinska, J. P-44
Klutz, K. O-16
Knauf, J. O-5
Kniery, K.R. O-2
Knoop, K. O-16
Ko, S. P-226
Kochanowski, J. P-108
Kodalle, T. O-174
Koh, Y. P-42, P-69, P-127
Koibuchi, N. P-204
Kolobova, I. P-77, P-238
Kraimps, J. P-219
Krishnan, B. P-173
Kudo, T. P-72
Kumar, S. P-186
Kushnir, L. P-167
Kwakkel, J. O-100
Kwan, P. O-6
Kwan, P.P. P-40, P-41
Kwang-Min, K. P-67, P-222
La Perle, K.D. P-43
Lacroix, L. P-49
Lakhia, R. P-198
Lamartina, L. P-220
Langfield, L. P-208
Lanman, R. P-244
Larrimer, A. O-181, P-187
Larsen, C.M. P-35
Larson, S. P-134
Lasho, M.A. P-46
Latif, R. P-17, O-182
Lavis, V. P-91
Le Donne, M. P-107
Leboulleux, S. P-49
Ledda, A. P-161
Lee, B. P-68, P-70
Lee, E. P-109, P-189
Lee, H. P-42, P-69, P-127, P-224
Lee, J. P-68, P-70, P-140, P-226, P-243
Lee, K. P-226
Lee, M. P-227
Lee, N. O-95
Lee, R. P-195
Lee, Y. P-68, P-70, O-179
Leenhardt, L. O-4
Lemieux, B. P-144
Lemon, C. P-143
Leonova, T. P-218
Leschik, J. P-25
Leung, A.M. O-12
Lew, J.I. P-62
Lewy, G.D. O-6, O-13, P-40
Li, D. P-64, P-106, P-129, P-233, P-236
Li, H. P-233
Li, L. O-14
Li, T. P-228
Li, Y. P-25, O-181, P-187
Liang, J. P-228
Liao, X. P-112
Licitra, L. O-3
Liezhen, F. P-38
Lifante, J. P-219
Lim, D. P-226
Lim, J. P-189
Lim, Y. P-68, P-70
Lin, H. O-99
Lin, J. P-141
Lin, K. P-141
Lin, Y. P-228
Lin, Z. P-192
Linderman, J.D. O-102
Line, A. P-210
Liu, C. O-92
Liu, J. P-133, P-142
Liu, Y. P-123
Liu, Z. P-106
Lombardi, G. P-166
Lowe, H. P-167
Lu, K. P-36
Lucas, A.M. P-168
Luidens, M.K. O-99
Lunt, C. P-143
Lushchyk, M.L. P-71, P-218
Macchia, P.E. P-166
Madde, P. P-150, O-178
Maffini, A. P-22
Mahruaii, V. P-202
Mai, V.Q. P-24, P-115
Makambi, K.H. P-79
Maker, A.V. O-14
Makidon, P. P-105
Makin, V. P-139
Mallick, U. P-143
Malone, M.K. O-94
Manchanda, P.K. P-43
Mandel, L. P-138
Mansharipova, A. P-31
Mansuri, S. P-56, P-135
Marchese, C. P-63
Marian, C. P-154
Marina, D. P-32
Marques, A. P-172
Marquez, A. P-197
Martin, A. P-41
Martin, W. P-19
Martins, R.G. O-3
Marzano, L.A. P-166
Mason, D. P-155
Massasati, S.A. P-173
Matsunaga, H. P-87, O-98, P-114
Matsushita, A. P-87, O-98, P-114
Matsuura, K. P-38
Mazeh, H. P-171
McAndrews, M. O-1, P-39
McCabe, C.J. O-6, O-13, P-40, P-41
McCaffrey, J.C. O-3
McCarty, S.K. O-8
McCoy, K.L. O-96
McDonald, J. O-103
McDonough, S. O-178
McIver, B. O-103, P-150, O-178, P-193
McLachlan, S. O-180
McPhaul, L. P-61
Meiyappan, S. P-54, P-151
Mendoza-Cisneros, A. P-74
Menegaux, F. P-219
Menéndez Torre, E. P-37
Meng, R. O-99
Meringolo, D. P-220
Meroño, T. P-197
Mestman, J.H. P-195
Mete, O. P-206
Mian, C. P-214
Michalek, K. O-182
Middleton, L. P-216
Milas, K. P-242
Milas, M. P-86, P-139, P-212
Miles, D. O-179
Miller, J.L. P-122
Ming, J. O-92
Mingote, E. P-197
Mircescu, H. P-144
Mirza, L. P-145
Misawa, H. O-98
Misra, S. P-151
Misso, C. P-166
Mitchell, A. P-198
Mitchell, J. P-86, P-212, P-242
Mitmaker, E.J. P-45, P-116
Mitsuhashi, T. P-146, P-165
Mityukova, T. P-218
Miyauchi, A. P-72
Moch, H. P-126
Mohamed, N. P-27
Moise, L. P-19
Mojdami, F.D. P-164
Moldabek, G. P-31
Momotani, K. P-34
Momotani, N. P-34
Monroe, R. P-244
Montesano, T. P-220
Montoro, M. P-195
Monzani, F. P-149, P-220
Moo-Young, T. P-28
Morari, E. O-175
Morel, O. O-4
Moreno, P. P-168
Morford, L.A. O-15
Morris, J. O-178
Morshed, S.A. P-17
Morton, K. P-156
Moss, L. P-143
Mouchati, A.R. P-158
Moura, J.P. P-147
Mousa, S.A. O-99
Mozarowska, A. P-84
Munir, K.M. P-51
Muraishi, K. P-23
Murphy, M. P-152
Nagayama, Y. P-104
Naik, C. P-205
Nair, D. P-203
Nair, S. P-81, P-163
Nakamura, H. P-87, O-98, P-114
Nakatake, N. P-29
Nakhoul, G. P-153
Nalini, R. P-198
Nam, K. P-167
Nam, Y. P-85
Narbuts, Z. P-210
Nasr, C. P-139, P-148, P-153, P-155, P-169
Nasr, G. P-153
Navarrete-Ramírez, P. P-159
Negro, R. O-10
Newbold, K. O-3, P-143
Newman, A.B. P-111
Nguyen, C. P-59
Nicol, A. P-143
Nie, X. O-92
Niel, S. P-108
Niepomniszcze, H. P-245
Nigel, B. P-56, P-135
Nikiforov, Y.E. O-96, P-126
Nikiforova, M.N. O-96, P-126
Nilegaonkar, S.S. P-33, P-205
Nilubol, N. O-93, P-207, P-229
Nishino, N. P-87
Nixon, I. O-95, P-136
Nogogaki, S. O-175
Noureldine, S.I. P-173
Nozima, B.N. P-47
Nozoe, Y. P-221
Nutting, C. P-143
O'Brien, J.P. O-3
O'Connor, A. P-152
Ogilvie, J.B. O-94
Ogris, M. O-16
Ohba, K. P-87, O-98, P-114
Ohishi, T. P-87
Okamoto, T. P-221
Oki, Y. P-87, P-114
Okun, N. O-11
Oler, G. P-47
Olivo, P. P-25, P-108, O-181, P-187, P-190
Olldashi, T. P-234
Omi, Y. P-221
Onigata, K. P-160
Opocher, G. P-214
Ora, M. P-230
O'Reilly, K. P-244
Orlander, P.R. P-133
Orozco, A. P-74, P-159
Ostro, J. P-27
Oundjian, N. P-120
Owen, R. P-167
Ozben, V. P-225
Ozgen, A. P-80
Ozono, S. P-114
Ozpinar, A. P-121
Pacini, F. O-3, O-14
Palmer, F. O-95, P-136
Panasiuk, G.D. P-71
Pande, A. P-133
Panunti, B. P-50
Park, G. P-48
Park, J. P-48
Park, W. P-66
Parks, J. P-78
Pasqualetti, G. P-149
Passon, N. P-130
Patel, A. P-44
Patel, K.N. O-94
Patel, S. O-95, P-136
Pathak, R.D. P-119
Pathak, S.R. P-119
Patterson, E.E. P-207
Pattou, F. P-219
Paulson, J.M. P-200
Pearce, E.N. O-12
Peix, J. P-219
Peker, O. P-225
Pelizzo, M. P-214
Pentlow, K.S. P-134
Perez, J. P-246
Perren, A. P-126
Perrino, M. P-214
Peters, D. P-77, P-238
Picard, M. P-144
Pignataro, L. P-22
Pilli, T. O-14
Pirags, V. P-210
Pitoia, F. P-245
Planer, B.C. P-120
Platonova, T. P-218
Platvoet ter Schiphorst, M.C. O-100
Ponnusamy, M. P-230
Ponto, K. P-25
Ponto, K.A. P-190
Porter, W. P-75
Prabhakar, B.S. O-14, P-18
Pradhan, P.K. P-230
Prasad, L. P-202
Prieto, I. P-144
Pringle, D.R. O-8, P-43
Prinz, R.A. P-28
Provost, Y. P-144
Puig-Domingo, M. P-168
Puppin, C. P-130
Purnell, J. P-77, P-238
Puthan Veetil, P. P-170
Qiao, C. P-188
Qin, J. O-14
Quintanilla-Flores, D.L. P-89
Rahbari, R. P-207
Rajan, M.G.R. P-163, P-203
Ramies, D.A. O-179
Ramundo, V. P-166
Ranabir, S. P-202
Rao, P. P-33
Rapoport, B. O-180
Rasmussen, A. P-32
Rauf, L. O-185
Read, M.L. O-6, O-13, P-40, P-41
Reddi, H.V. P-150, O-178
Redler, A. P-63
Reed, N. P-143
Refetoff, S. P-112, P-160
Reiher, A.E. P-171
Reiland, H. P-75
Reiners, C. P-218
Reitz, R. O-177
Ricci, S. P-149
Riemann, B. O-174
Riestra Fernández, M. P-37
Riggs, A. P-216
Ringel, M.D. O-8
Rivkees, S. P-218
Robbins, R.J. P-134
Robinson, B. O-3
Rodin, G. P-54, P-151
Rogowski, F. P-84, P-241
Roman, S.A. P-65
Roman-Gonzalez, A. P-246
Romanowsky, J. P-244
Ronga, G. P-220
Rosenthal, M. P-52
Rotstein, L. P-54, P-151
Roussilhes, A. O-12
Rovet, J.F. O-1, P-39, P-124
Rubin, B.P. P-148
Rujelman, R. P-197
Russell, S. O-178
Russo, D. P-130
Ryan, G.A. O-6, O-13, P-40
Ryder, M. O-5
Ryu, H. P-222
Ryu, J. P-60
Rödl, W. O-16
Sachdev, P. O-3
Saeki, T. P-38
Safer, J.D. P-158
Sahin, M. P-191
Saji, M. O-8
Salem, A. P-56, P-135
Salvai, M.E. P-245
Salvi, M. P-22
Samuels, M. P-77, P-238
Sánchez Ragnarsson, C. P-37
Sánchez Rivas, V. P-37
Santaguida, M. O-9
Santos, J. P-172
Saraceno, G. P-196
Sasaki, S. P-87, O-98, P-114
Sawka, A.M. P-54, P-151
Saygili, F. P-80
Scanlan, T.S. P-75
Scanlon, T.S. O-7
Schaefer, S. P-171
Scharpf, J. P-169
Schlichtiger, J. O-16
Schlumberger, M. O-3, O-4, P-49
Schnitman, M. P-197
Schober, O. O-174
Schuff, K.G. P-77, P-238
Schuller, K. O-12
Schvartz, C. O-4
Schwartz, A. O-10
Schwenk, N. O-16
Scoggan, K.A. P-188
Sebag, F. P-219
Sebo, T.J. P-193
Secolin, R. O-183
Seed, R.I. O-6, O-13, P-40, P-41
Sellin, R. P-231
Seong, K. P-66
Seong-joon, K. P-67, P-222, P-227
Serteser, M. P-121
Settineri, S. P-107
Severino, R. P-166
Sezgin, O. P-121
Shah, D. P-81
Shah, J. O-95, P-136
Shah, M.H. O-3
Shaha, A. O-95, P-136
Shakir, K. P-24, P-115
Shanker, B. P-247
Sharma, N. O-6, O-13, P-40, P-41, P-88
Sheahan, P. P-152
Shen, Q. P-64
Shen, W.T. P-45
Sherman, S. O-3, O-179
Shi, L. O-92, P-106
Shi, W. P-106
Shi, Y. P-38
Shim, M. P-227
Shimokawa, N. P-204
Shin, D. P-109, P-189
Shin, J. P-86, P-212, P-226, P-227
Shin, S. P-68
Shin, Y. P-227
Shinde, R. P-208
Shon, H. P-223
Shong, Y. P-60, P-110
Silva, A.C. O-183
Simchowitz, L. O-102
Simic, N. P-39
Singh, N.N. P-202
Singh, P. P-202
Siperstein, A. P-86, P-212, P-242
Sippel, R.S. P-118, P-171
Sips, H. P-162
Sirinvaravong, S. P-232
Skocic, J. P-39
Skugor, M. P-153
Smallridge, R. P-53
Smeraglio, A. P-77, P-238
Smit, J.W. P-162
Smith, K.J. O-96
Smith, S. O-102
Smith, V.E. O-6, O-13, P-40, P-41
Soares, F. O-175
Soldin, O. P-79, P-154
Son, S. P-70
Sonar, S. P-205
Soneru, C. P-73
Song, B. P-66
Sosa, J. P-65
Spiezia, S. P-166
Spitzweg, C. O-16
Spratt, S. P-131
Sreemantula, G. P-213
Sretenskaya, Z.L. P-71
Sriphrapradang, C. P-112
Stack, B. P-216
Stagnaro-Green, A. O-10
Stan, M. P-193
Stang, M.T. O-96
Stephenson, T. P-143
Stewart, S. P-40
St. Germain, D.L. O-101
Straus, S. P-54
Sudhakar, P. P-33
Suk, J. P-110
Sun, G. P-155
Sundaram, K. P-248
Sung, J. P-243
Sung, K. P-85
Sungur, Y. P-121
Surovsteva, O.V. O-100
Swist, E. P-188
Synrem, E. P-202
Szelachowska, M. P-84, P-241
Szorc, M. P-241
Szumowski, P. P-84, P-241
Taguchi, R. P-104
Taha, I.M. P-194
Tajiri, J. P-29
Takayama, T. P-114
Tamez Perez, H.E. P-89
Tamez-Peña, A.L. P-89
Tang, H. O-99
Tani, J. P-23
Tars, J. P-210
Taxy, J. P-73
Teixeira, A. O-182
Teng, L. P-157
Teng, X. P-123
Thabane, L. P-54
Thakkar, V.R. P-203
Thosani, S. P-90, P-91
Tin, J.A. P-46
Tirona, R.G. P-164
Tomaz, R. P-117
Tomlinson, G. O-11
Tonelli, M. P-75
Torlontano, M. P-220
Toubert, M. O-4
Touzet, S. P-219
Tran, T. P-61, P-82
Traweek, T. P-244
Trimarchi, F. P-196
Trooskin, S. P-247
Trujillo, M. O-178
Tsang, N. P-141
Tsang, R.W. P-54, P-151
Tuttle, R.M. O-95, P-134, P-136
Ucan, B. P-191
Unal Kocabas, G. P-80
Unsal, I. P-121
Urrutia, A. P-197
Ursino, S. P-149
Valverde-R, C. P-74, P-159
van Beeren, H.C. O-100
Vannucchi, G. P-22
Van Uum, S.H. P-164
van Zeijl, C.J. O-100
Vasko, V. P-44
Vassallo, J. O-175
Velez, A. P-246
Vera, P. O-4
Verbeeck, G. P-55
Verga, U. P-214
Vertes, J. O-11
Vetter, A. O-16
Vicentini, L. P-214
Vigersky, R. P-239
Villalobos, P. P-74, P-159
Vilmanis, J. P-210
Virili, C. O-9
Viswanathan, L. P-239
Vita, R. P-196
Voirin, N. P-219
Vora, J. P-213
Vorasubin, N. P-59
Vos, X.G. O-183
Wadsley, J. P-143
Wadwekar, D. P-156
Wagner, E. O-16
Waguespack, S. P-91
Walfish, P.G. O-11
Wang, J. P-129
Wang, M.B. P-59
Wang, S. P-70, P-105
Wang, W. P-157
Wang, Y. P-64, P-129, P-233, P-236
Wang, Z. P-64, P-233
Ward, L. O-183
Ward, L.S. O-175
Warfield, A. P-40
Waring, A.C. P-111
Wartofsky, L. P-44
Watkinson, J.C. P-41, P-88
Weaver, A. P-199
Weber, K. P-167
Wei, W. P-129, P-233, P-236
Weiss, R.E. P-160
Westfall, J. O-99
Whitcher, M. P-136
Wiersinga, W.M. O-183
Willhauck, M.J. O-16
Williams, M.D. P-128
Willoughby, K.A. O-1, P-124
Winchester, D.J. P-28
Wison, M. P-195
Wong, K. O-97
Wood, B. P-155
Wood, K. P-118
Woodhead, H. P-160
Wu, A. P-59
Wu, G. P-148
Wu, V. P-192
Wu, Y. P-64, P-129, P-233
Xu, K. P-233
Yakupoglu, A. P-225
Yalla, N.M. O-15
Yamada, M. P-104
Yamashita, S. P-71
Yap, B. P-143
Yavuz, S. O-102
Yi, P. P-106
Yildirim Simsir, I. P-80
Yilmaz, C. P-80
Yim, J. P-60, P-110
Yin, R. O-102
Yin, X. O-185
Yin, Z. P-43
Yip, L. O-96
Ylli, A. P-234
Ylli, D. P-234
Ylli, Z. P-234
Yoo, M. P-42, P-69, P-127
Yoon, J. P-60
Yosep, C. P-67
Yu, L. P-43
Yunjung, C. P-235
Zagar, I. P-215
Zalles, C. P-244
Zendel, B. P-124
Zerdoud, S. O-4
Zhang, L. O-93, P-129, P-207, P-233, P-236
Zhang, Y. O-177
Zhao, Q. O-92
Zhao, Y. P-106
Zhu, Y. P-64, P-129, P-233, P-236
Zucchi, R. P-75