
Abstract

Saturday, October 29, 2011
Selective Endothelial Expression of Thyroid Hormone Receptor Brestores Capillary Density in Heart Failure
Thyroid Hormone Metabolism and Regulation Oral Saturday 10:45 AM
Introduction: Insufficient angiogenesis is one of the causes leading to tissue ischemia and dysfunction. Heart failure is associated with decreased capillary density in the left ventricular (LV) myocardium. Angiogenic effects of thyroid hormone (TH) are recognized but cardiac effects on heart rate limit a potential therapeutic use of TH to induce angiogenesis. In previous studies we demonstrated a role for thyroid hormone receptor β (TRβ) in cardiac angiogenesis. The goal of this study was to investigate if selective expression of TRβ in endothelial cells can return cardiac capillary density towards normal in pressure overload-induced heart failure without detrimental effects.
Methods: We generated binary transgenic mice in which an endothelial cell (EC) directed Tie2 promoter drives conditional expression of TRβ1 in ECs using a tetracycline (Tet) on system termed Tie2-Tet-TRβ1/Dox mice. Pressure overload-induced heart failure was achieved by ascending aortic constriction (AAC) for 10 weeks. TRβ induction was achieved by doxycycline administration. Effects were evaluated after 4 weeks of TRβ expression.
Results: Our results shown that induction of TRβ increased TRβ protein levels by 50% in coronary endothelial cells from Tie2-Tet-TRβ1 mice. Capillary density was increased by 27% in the left ventricle. Coronary blood flow was increased by 76% in transgenic mice. No effects on heart rate, blood pressure or body temperature were observed after endothelial TRβ expression. Tie2-Tet-TRβ1 mice subjected to AAC for 10 weeks showed decreased capillary density by 43%. However, induction of TRβ1 in ECs restored capillary density towards control values in Tie2-Tet-TRβ1 AAC mice. Studies to identify the mechanism of TRβ-induced angiogenesis revealed increased ERK phosphorylation in endothelial cells of Tie2-Tet-TRβ1.
Conclusion: Selective endothelial expression of TRβ is angiogenic in heart failure, avoids undesirable TH effects and the ERK-mediated pathway is involved in the mechanism of action.
Endocrinology, Johns Hopkins Bayview, Baltimore, MD, United States
Thyroid Cancer Oral Saturday 11:00 AM
Introduction: Interferon alfa (IFN) therapy causes several patterns of thyroid dysfunction that previously have been unpredictable. To define risk factors for specific presentations, we analyzed demographic, clinical, and biochemical features in 1,243 initially euthyroid hepatitis C patients from the ACHIEVE 1 study, who received IFN and ribavirin for up to 48 weeks.
Methods: Serum TSH and free T4 were measured pre-treatment and every 4 weeks during IFN therapy, starting at week 8. Subtypes of thyroid dysfunction were defined based on the temporal patterns. Risk factors were analyzed with multivariate logistic regression that included age, sex, race, smoking history, duration of hepatitis C infection, length of therapy, and achieving a virological response.
Results: Overall, thyroid dysfunction of any severity occurring on therapy was seen in 19% of patients. The three most commonly observed patterns were hypothyroidism (n=87 [7.0%]), thyrotoxicosis (79 [6.4%]), and thyrotoxicosis followed by hypothyroidism (67 [5.4%]). Patients' pretreatment TSH levels were strongly associated with their subsequent form of thyroid dysfunction: incident hypothyroidism was 3-fold more common with each +1 mU/L higher pretreatment TSH increment, and thyrotoxicosis was 5-fold more common for each −1 mU/L lower TSH (p<0.001 for each). Duration of IFN therapy was associated with increased risk of hypothyroidism (OR=1.04 per week on therapy, 95% CI 1.01–1.06]; but not risk of thyrotoxicosis. Female sex was a risk factor only for biphasic thyroid dysfunction (OR=9.1, CI 4.6–18), occurring in 11.2% of women vs. 1.5% of men. Biphasic dysfunction was also associated with both duration of IFN (OR=1.06 per week, CI 1.02–1.09, p<0.001) and with increased pretreatment TSH (OR=1.6 per +1 mU/L, CI 1.2–2.1).
Conclusion: In addition to the prognostic utility of these novel observations defining risk factors for specific forms of IFN-related thyroid dysfunction, our results suggest distinctions in the underlying pathophysiology between subtypes, including the role of immunomodulation and the amplification of pre-existing homeostatic imbalances.
Medicine, Memorial Sloan-Kettering Cancer Center, New York, NY, United States
Thyroid Hormone Action Oral Saturday 11:15 AM
Introduction: Resistance to radioactive iodine (RAI) is a significant problem for patients with metastatic, differentiated thyroid carcinoma (DTC). Studies in mouse models show that blocking mitogen-activated protein kinase (MAPK) signaling with a MAP kinase kinase 1/2 (MEK1/2) inhibitor increases sodium iodide symporter expression and iodine incorporation. This pilot study aimed to evaluate if the MEK inhibitor selumetinib (AZD6244, ARRY-142866) could reverse RAI-refractoriness in metastatic DTC patients.
Methods: Patients with RAI-refractory DTC were defined as possessing 1) Non-RAI-avid lesion/son a diagnostic and/or post-therapy RAI scan, 2) RAI-avid lesion/s that remained stable or increased in size after RAI therapy, or 3) Fluorodeoxyglucose (FDG)-avid lesion/s by positron emission tomography (PET) scan. rhTSH-stimulated lesional dosimetry with 1241 PET was performed prior to and after 4 weeks of treatment with selumetinib (75 mg orally b.i.d.). If the second 1241 PET scan predicted that a lesional dose of >2000 cGy could be achieved, therapeutic RAI was administered while on the drug, which was stopped 48h later. RECIST response by CT and suppressed Tg values were assessed after therapeutic RAI administration.
Results: 17 of the planned 20 patients have had pre and post-MEK inhibitor 1241 PET scans. Median age was 61 (range 44–77 yrs), 9 were men. 7 patients had BRAF mutant (MUT) and 10 BRAF wild-type (WT) tumors. All patients completed therapy. Selumetinib increased 1241 uptake in 11/17 patients (4 of 7 BRAF MUT patients and 7 of 10 BRAF WT). Seven received therapeutic RAI (6 BRAF WT patients). Mean percent reduction in thyroglobulin 2 months after therapeutic RAI was 91% (range 76%–100%). Two patients had confirmed partial responses (PRs) and 1 patient had stable disease (SD). Four patients have undergone only 1 post-RAI CT to date: 3 have unconfirmed PRs and 1 SD. Four patients experienced Grade 3 hypertension; no Grade 4 or 5 toxicities were observed.
Conclusion: A 1 month course of selumetinib prior to therapeutic RAI administration is associated with increased RAI uptake in metastatic lesions and objective biochemical and structural response to therapy, particularly BRAF WT tumors.
Endocrinology, Erasmus Medical Center, Rotterdam, Netherlands
Autoimmunity Oral Saturday 11:30 AM
Introduction: Variation in serum thyroid parameters, even within the normal range, is associated with a wide range of health risks. Although 45–65% of the inter-individual variation in serum TSH and FT4 levels is due to genetic factors, the causative genes are not well established. We therefore performed a genome wide association study (GWAS) for TSH and FT4 levels.
Methods: 18,400 subjects, derived from 12 populations with available GWAS, serum TSH and/or FT4 data, were included. To identify genes that influence serum thyroid parameters within the normal range, we included subjects with a TSH level between 0.4–4.0 mU/L, not using thyroid medication. The effects of 2.4 million polymorphisms on TSH and FT4 levels were studied, correcting for age and gender. Promising associations were replicated in 5,200 subjects. A bonferroni-based P-value<5 × 10−8 was regarded significant.
Based on the top polymorphisms, genotype risk scores were calculated in 7,000 subjects, and associated with the risk of an elevated (>4.0 mU/L) or suppressed (<0.4 mU/L) TSH.
Results: For FT4, significant associations were detected at chromosome 1p32 (DIO1; P=6.8 × 10−23), 9q34 (LHX3; P=2.3 × 10−12), 4q33 (AADAT; P=9.2 × 10−9), and 9q22 (FOXE1; P=4.3 × 10−9). For TSH, significant associations were detected at chromosome 5q13 (PDE8B; P=1.2 × 10−40), 6q26 (PDE10A; P=1.3 × 10−18), 1p36.1 (CAPZB; P=3.1 × 10−17), 16q23 (MAF; P=2.3 × 10−15), 6p12 (VEGFA; P=4.3 × 10−14), 4q31.2 (NR3C2; P=3.9 × 10−13), 2q35 (IGFBP5;P=2.6 × 10–12), 9q34 (ABO; P=2.5 × 10-9), and 19p13.2 (INSR; P=1.6 × 10-8). Comparing subjects with a genotype risk score in the highest vs lowest quartile, an increased risk of an elevated TSH (OR=1.43, P=0.02), and a decreased risk of a suppressed TSH (OR=0.42, P=1.2 × 10−10) were found.
Conclusion: In this large GWAS, we replicate previously reported associations of DIO1, FOXE1, PDE8B, and CAPZB with thyroid parameters. We newly report associations of 2 loci with FT4, and 7 loci with TSH levels. In addition, we show that carriers of multiple risk variants have a substantially increased risk of (subclinical) hypothyroidism and decreased risk of (subclinical) hyperthyroidism.
The Braft 1799A Mutation and Poor Outcomes of Papillary Thyroid Cancer—Report from the International Collaborative Braf Study Group
Thyroid Cancer Oral Saturday 11:45 AM
Introduction: The BRAFT 1799A mutation is the most important genetic alteration in papillary thyroid cancer (PTC). Its prognostic potential has drawn considerable interest but has not been established, particularly its role in patient mortality.
Methods: This was a retrospective international study, involving 27 centers in 15 countries, designed to extensively analyze the clinicopathological outcomes of PTC with respect to the BRAFT 1799A mutation status in 5,646 patients.
Results: A strongly significant association of BRAF mutation was found for virtually all the classical high-risk factors, including extrathyroidal invasion, lymph node metastasis, multifocality, larger tumor, distant metastasis, older patient age, and advanced tumor stages. This association was seen on both the overall analysis of all subtypes of PTC and the analysis of the individual subtypes of conventional PTC (CPTC) or follicular variant PTC (FVPTC). Analysis on 2,339 cases from centers that provided complete data on tumor recurrence showed a strong association of the BRAF mutation with tumor recurrence on both the overall analysis of PTC and the analysis of CPTC or FVPTC. The association of BRAF mutation with PTC recurrence was seen even in Stage I disease and tumors of 0.5–1.0 cm. Importantly, mortality analysis on 1,152 cases from centers that provided such data showed a significant association of BRAF mutation with PTC-related patient death. Specifically, PTC-related death rates were 23/520 (4.4%) in BRAF mutation-positive patients vs. 9/632 (1.4%) in BRAF mutation-negative patients (p=0.004) on the overall analysis of all types of PTC and 19/446 (4.3%) in BRAF mutation-positive patients vs. 5/430 (1.2%) in BRAF mutation-negative patients (p=0.009) on the analysis of CPTC. The BRAF mutation was therefore associated with a 3–4 times increase in the risk for PTC-associated mortality. A borderline association (p=0.055) of BRAF mutation with death was seen in patients with tumors of 0.5–1.0 cm.
Conclusion: This large multicenter international study has firmly established the aggressive role of BRAF mutation in PTC and hence its prognostic value in the management of PTC.
Internal Medicine, The Ohio State University, Columbus, OH, United States
Thyroid Cancer Oral Saturday 12:00 PM
Introduction: PAKs are a family of serine/threonine kinases involved in cytoskeletal signaling and epithelial-to- mesenchymal transition (EMT). The six isoforms of PAK are divided into group I (PAKs 1–3) and group II (PAKs 4–6). We previously identified increased PAK signaling in the invasive fronts of aggressive papillary thyroid cancers (PTCs), including those with BRAF V600E mutations. We also demonstrated that BRAF mutation-positive cancer cell motility is dependent on Group 1 PAKs and PAK1. We therefore hypothesized that BRAF regulates thyroid cancer cell motility in part through PAK activation.
Methods: We used three human thyroid cancer cell lines with common thyroid cancer mutations, BCPAP (BRAF V600E), TPC1 (RET/PTC1) and FTC133 (PTEN null).
Results: In all cell lines, we demonstrated that BRAF suppression with siRNA inhibited PAK-mediated phosphorylation of multiple direct targets without reducing PAK levels. In contrast, group I PAK or PAK1 suppression did not affect BRAF function. Transfection of all three cell lines with constitutively active (CA)-PAK1 rescued thyroid cancer cell migration suppressed by BRAF inhibition. Inhibiting MEK1/2 also reduced thyroid cancer cell migration and co-transfection using CA-MEK1 rescued thyroid cancer cell migration suppressed by BRAF inhibition, demonstrating that both pathways are involved in BRAF-regulated thyroid cancer cell motility. To determine whether BRAF regulation of PAK was dependent on MEK, we inhibited MEK1/2 with U0126. U0126 treatment did not decrease PAK phosphorylation or activity in the cell lines, consistent with a MEK-independent pathway. Finally, to determine if BRAF and PAK1 physically interacted, wild type BRAF and PAK1 were co-transfected into HEK293 cells. Co-immunoprecipitation confirmed binding and confocal microscopy demonstrated co-localization, consistent with a direct physical interaction between BRAF and PAK1.
Conclusion: In conclusion, we have identified a new signaling cascade in which BRAF activates PAK1 in a MEK- independent manner. This pathway regulates thyroid cancer cell motility and may be an important novel BRAF pathway involved in thyroid cancer invasion.
Thursday, October 27, 2011
Endocrinology, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States
Thyroid Cancer Clinical Thursday
Introduction: RAS oncogene is frequently mutated in thyroid tumors, can be detected in fine needle aspiration (FNA) samples from thyroid nodules, and reportedly confers a 60–85% risk of cancer. Specific clinical, pathologic and radiologic characteristics of cancers associated with RAS positive FNA have not been reported.
Methods: From 4/07–4/09, we prospectively applied a panel of molecular markers to a consecutive series of thyroid FNAs from 856 patients. Sixty Four nodules were positive for mutations in NRAS (47), HRAS (13) or KRAS (4). For these 62 patients, ultrasounds and cytology findings were re-reviewed and outcomes including histopathology and postoperative thyroglobulin (Tg) levels were evaluated.
Results: Of 64 RAS-positive nodules, only 1 was malignant on cytology and 63(98%) had results in an indeterminate category (32 follicular neoplasm, 22 follicular lesion of undetermined significance and 9 suspicious for malignancy). Among the 57 patients with 59 RAS-positive nodules who had surgery, thyroid cancer was present in 48(81%) nodules. Four were follicular carcinoma (FTC) and 44 were papillary thyroid cancer (PTC). All 44 RAS-positive PTC had follicular variant histology (FVPTC), 40/44 were encapsulated (of which 10 had vascular or capsular invasion) and 4/44 were infiltrative. Ultrasound appearance was considered suspicious in only 38% of cancers. Tumors were T1–T2 in 89% and T3 in 11% of cases. Positive lymph nodes were found in 2% of cases. With mean follow-up of 22 months, 30/33 patients have had no recurrence, while 3(9%) patients have detectable thyroglobulin levels.
Conclusion: RAS-positive FNA results have an 81% malignancy risk and are associated with thyroid cancers that have a predominantly encapsulated and follicular-patterned histology, perhaps explaining the high rate of cytologically indeterminate FNA results and benign/innocuous appearance on ultrasound. Although many RAS-positive thyroid cancers had an early stage at presentation, a significant proportion (38%) were FTC or histologically invasive/infiltrative FVPTC. Risk of persistence/recurrence was low in limited follow-up. Regardless of sonographic and cytologic findings, patients with RAS-positive FNA results should be considered for initial total thyroidectomy.
Anatabine, A Tobacco Alkaloid, Reduces Disease Incidence and Severity in a Mouse Model of Autoimmune Thyroiditis
Autoimmunity Basic Thursday
Introduction: Epidemiological evidence suggests that tobacco smoking favorably influences the course of some autoimmune diseases like ulcerative colitis and Hashimoto thyroiditis. The mechanism of this beneficial effect is unknown and overshadowed by the vast array of detrimental effects that smoking has on human health. We tested anatabine, a minor alkaloid of tobacco, in a mouse model of experimental autoimmune thyroiditis (EAT).
Methods: EAT was induced in female CBA mice by immunization with mouse thyroglobulin mixed in complete Freund's adjuvant on days 0 and 7. Mice were then sacrificed on day 21 for blinded determination of the histological and serological outcomes. Mice (N=37) were divided into two groups: one (N=20) drank regular water, the other (N=17) drank water supplemented with anatabine (0.05 mg per ml of water, for a daily dose of 12.5 mg anatabine per Kg of body weight). Anatabine was synthesized chemically (Rock Creek Pharmaceuticals, Washington, DC).
Results: Anatabine significantly suppressed the incidence and severity of thyroiditis. Only 9 of 17 (53%) anatabine mice developed lymphocytic infiltration of the thyroid, as opposed to 19 of 20 (95%) of the controls. The mean graded histopathological severity was 0.81 in the anatabine group and 1.82 in the water control group (p=0.004 by Wilcoxon ranksum test). Anatabine had no effect on thyroglobulin antibody levels, which increased in both groups of mice upon immunization. To begin investigating the mechanism of action, we tested in vitro the effect of anatabine using a macrophage cell line (RAW 264.7). Treatment with anatabine inhibited in a dose-dependent manner the production of pro-inflammatory mediators like inducible nitric oxide synthase and cyclooxygenase 2 released in response to lipopolysaccharide stimulation.
Conclusion: In summary, we have shown that anatabine attenuates the development of autoimmune thyroiditis in a mouse model of the disease, making the exploration of its mechanisms of action and potential clinical utility worthwhile.
Transaxillary Robotic Thyroidectomy: Northwestern University Early Clinical Experience
Thyroid Diseases Thursday
Introduction: The transaxillary single-incision robotic assisted thyroidectomy (TRAT) is the most recent approach to minimally invasive thyroid surgery. This procedure, although popular in Asian countries, is slowly being adopted in the US, due in part to cultural differences, longer operative times and higher costs. However, TRAT has been shown to be a safe alternative to the conventional open thyroid surgery in appropriately selected patients and when performed in centers with experienced thyroid surgeons. We present a single surgeon's initial experience with six patients in a tertiary referral medical center. The patient selection criteria, the intraoperative time commitments, the technical limitations, as well as the postoperative results are presented.
Methods: The transaxillary robot assisted thyroidectomy was performed on 6 patients over the course of a 4-month period. The criteria for patient selection was unilateral benign disease, and nodules<4 cm in size. Additionally, the patients selected for robotic thyroidectomy had normal body habitus with BMI<30. Exclusion criteria included proven thyroid malignancy, previous contralateral hemithyroidectomy, prior neck surgery, prior axillary surgery, Grave's disease and Hashimoto's thyroiditis.
Results: All 6 patients were females. Average age was 36 (range 28–43). Average BMI was 24 (range 22–29). The dominant nodule size average was 2.45 cm (range 1.2–3.8). All procedures were hemithyroidectomies for benign disease. No major complications, including vascular injury and recurrent laryngeal nerve injury, were reported. All six patients complained of transient postoperative paresthesia in the supraclavicular nerve distribution and there was one incidence of partial dehiscence of the axillary incision; no seromas or hematomas occurred.
Conclusion: Our initial experience showed that TART provides superior 3D visualization, greater video-image stability, and improved maneuverability of the surgical instruments, making it a viable alternative to conventional and endoscopic thyroid surgery. We believe that the continuing development of robotic instruments and technology will render the procedure more affordable and will overcome the steep learning curve and longer operating times.
Friday, October 28, 2011
Department of Surgery, Karolinska Institutet Danderyd Hospital, Stockholm, Sweden
Thyroid Diseases Friday
Introduction: The incidence of hyperthyroidism has been reported in various countries to be 23–93/100,000 inhabitants/year. This extended study has evaluated the incidence for approximately 40% of the Swedish population of 9 million inhabitants. Sweden is considered iodine sufficient.
Methods: All patients including children, who were newly diagnosed with overt hyperthyroidism in the years 2003–2005, were prospectively registered in a multicenter study. Inclusion criteria: clinical symptoms and/or signs of hyperthyroidism with plasma TSH concentration below<0.2 mIE/l, increased plasma levels of free/total T3 and/or free/total T4. Patients with relapse of hyperthyroidism or thyroiditis were not included. The diagnosis Graves' disease (GD), toxic multinodular goiter (TMNG) and solitary toxic adenoma (STA), smoking, initial treatment, occurrence of thyroid associated eye symptoms/signs and demographic data were registered.
Results: 2916 patients were diagnosed with de novo hyperthyroidism giving the total incidence of 27.6/100,000 inhabitants/year. The incidence of GD was 21.0/100,000 and toxic nodular goiter (TNG=STA + TMNG) occurred in 692 patients, corresponding to an annual incidence of 6.5/100,000. The incidence was higher in women compared to men (4.2:1). 75% of the patients were diagnosed as GD, in whom thyroid associated eye symptoms/signs occurred at diagnosis in every fifth patient. Geographical differences were observed.
Conclusion: The incidence of hyperthyroidism in Sweden is in a lower range compared to international reports. Patients with hyperthyroidism had GD in 75% and 20% of them had thyroid associated eye symptoms/signs at diagnosis. The observed geographical differences require further studies.
Shanghai Institute of Immunology, Medical Sciences, Shanghai Jiao Tong University School of Medicine, Shanghai, China
Thyroid Cancer Friday
Introduction: Papillary thyroid carcinoma (PTC) has a tendency to spread into lymphatic channels and metastasizes to regional lymph nodes at a high frequency. The development of metastasis is complex, requiring multiple individual steps to successfully establish a tumor at a secondary site. The link between inflammation and carcinoma has been acknowledged. Regulation and function of Toll-like receptor 4 (TLR4) in PTC still remain to be elucidated.
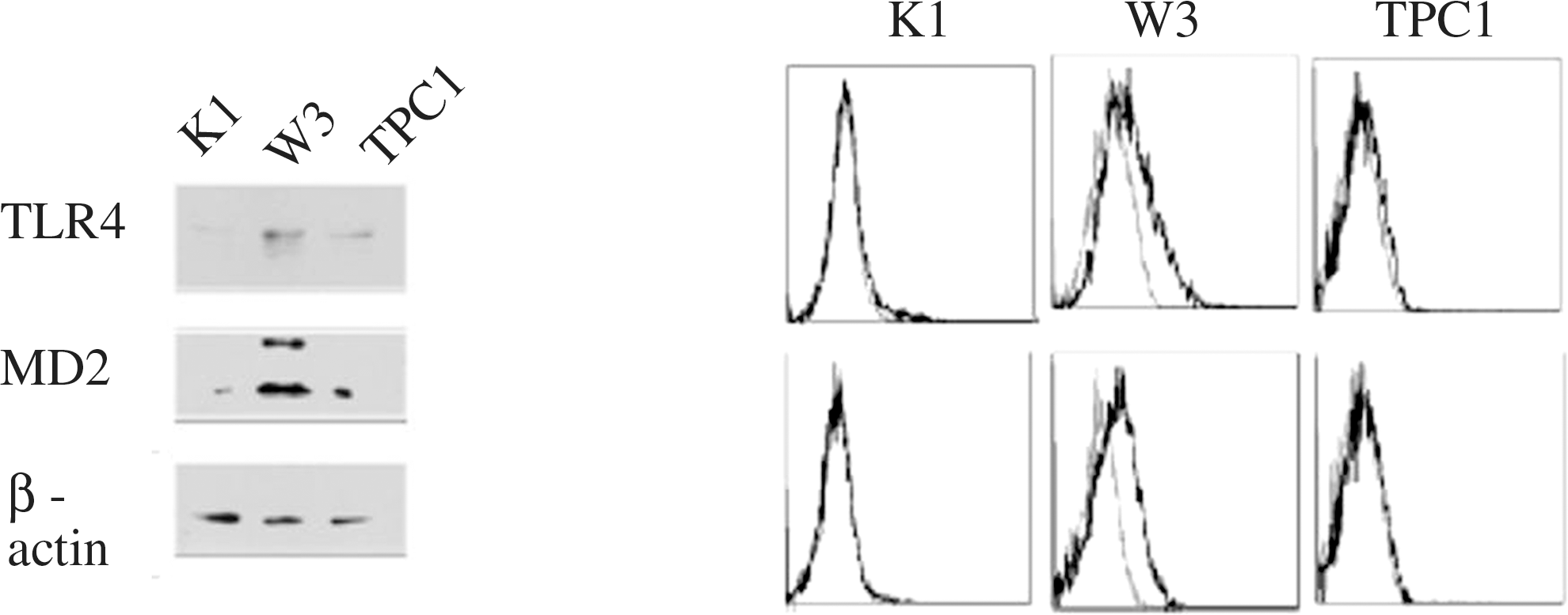
Methods: In the present study, western blot, flow cytometry and real-time PCR assay were used to identify TLR4 and myeloid differential protein (MD-2) in K1, W3 and TPC-1 PTC cells. Incubation with LPS, flow cytometry and real-time PCR assay were used to identify CXC chemokine receptor CXCR7 and CXCR4 expression alterations. We subjected W3 cells expressing TLR4/MD-2 to transient transfection with the siRNA specific for the MD-2 gene. Cell proliferation assay, apoptosis assay and migration experiments were used to comprehend the function of CXCR7. To further support the above results, we investigated the clinicopathologic significance of TLR4, MD-2 and CXCR7 expression using immumohistochemistry in PTC tissues.
Results: We demonstrated that exposure to LPS elevated CXCR7 expression in W3 cells expressing TLR4/MD-2. Knockdown of MD-2 inhibited LPS-mediated time- and dose-dependent CXCR7 expression alterations. CXCR7 is associated with W3 cell proliferation and migration. However, exposure ofW3 cells to LPS had no effect on CXCR4 expression. Higher rates of TLR4 (53%), myeloid differential protein (MD-2) (71%) and CXCR7 (24%) expression were found in PTC tissues than in normal thyroid tissues. The recombination of TLR4, MD-2 and CXCR7 strongly correlated with tumor size and lymph node metastasis in 135 PTC tissue samples (p=0.002, p<0.001, resp.).
Conclusion: Accordingly, simultaneously examination of the expression of TLR4, MD-2 and CXCR7 in PTC tissues may provide valuable prognostic diagnosis of carcinoma growth and metastasis. Interplay of TLR4, MD-2 and CXCR7 may be of interest in the context of novel immunomodulatory therapies for PTC.
Expression of TLRA and MD-2 in PTC cells.
Correlation of TLR4, MD-2, and CXCR7 Expression with Clinicopathologic Features in PTC
Thyroid Cancer Clinical Friday
Introduction: Thyroid cancer is uncommon but perhaps increasing in the pediatric population. Pediatric thyroid cancer is unique from adult thyroid cancer in many ways, with a markedly greater predilection towards metastases but paradoxically also a greater degree of differentiation and correlatively a much better prognosis. The standard threshold for a biopsy of a thyroid nodule in a pediatric patient is 1.0 em, as in the adult population. As such a similar size threshold may be proportionally more significant in a smaller patient, other factors may help to identify the risk of a malignant process. TSH is a well-recognized growth factor which may have a fundamental role in the evolution of thyroid cancer, potentially serving as a marker to identify pediatric patients in whom the risk of a malignant process is greater and for whom the threshold for a biopsy of a thyroid nodule may need to be lower.
Methods: A total of 116 pediatric patients with an indication for thyroidectomy referred to Seattle Children's Hospital, a major pediatric tertiary medical center, between January 1997 and January 2011 were retrospectively assessed in a case-controlled study. Requiring preoperative TSH values and excluding patients with medications that would directly affect thyrotropin secretion, 79 patients between the ages of 3 years and 20 years of age were analyzed.
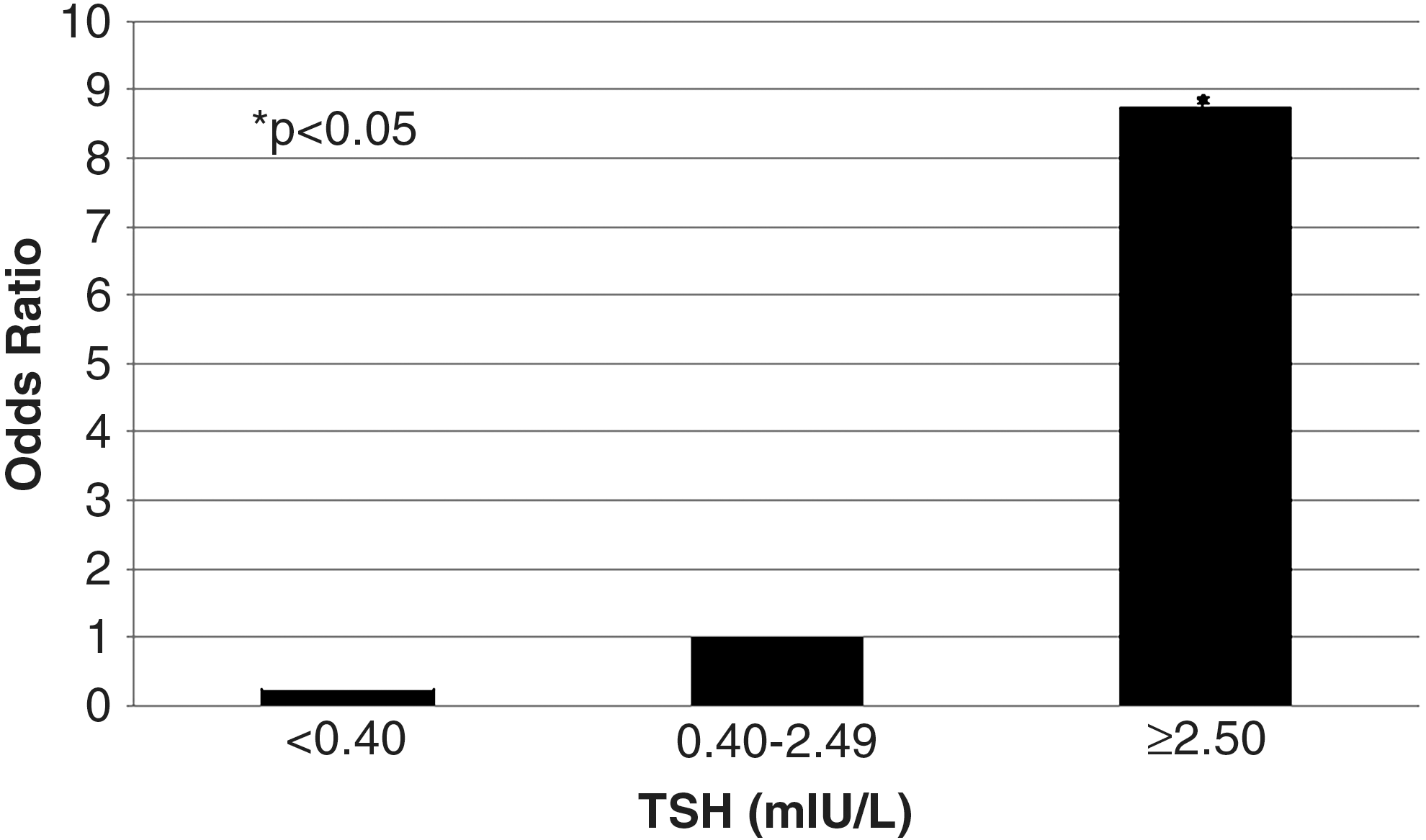
Results: The risk of papillary thyroid carcinoma in pediatric patients correlated with increasing TSH levels. In pediatric patients with papillary thyroid carcinoma, the average TSH 2.71 miU/L ± 3.06 was significantly greater than the TSH 1.07 ± 1.00 miU/L noted in patients without malignancy (p=0.02). A rightward skew of TSH was associated with pediatric patients harboring papillary thyroid carcinoma, with a TSH 2.50 miU/L or greater correlating with a significantly increased odds ratio of 8.75 (p=0.0036) relative to a normal TSH range between 0.40–2.50 miU/L.
Conclusion: Pediatric papillary thyroid carcinoma is associated with higher TSH levels, especially 2.50 miU/L or greater, which may be useful to identify a higher risk of malignancy in a pediatric patient with a thyroid nodule. A higher TSH in a pediatric patient with a thyroid nodule may lower the threshold for a biopsy.
TSH correlates with incidence of papillary thyroid carcinoma.
Withdrawn
Saturday, October 29, 2011
Divison of Endocrinology and Nephrology, University of Leipzig, Leipzig, Germany
Thyroid Cancer Saturday
Introduction: Although fine needle aspiration (FNA) is considered the most sensitive method to select suspicious nodules for surgery this method has some inherent limitations, e.g. “indeterminate” samples. As rearrangements (PAX8/PPARG, RET/PTC) and point mutations (BRAF, NRAS) have been detected in follicular carcinomas (FTC) and papillary carcinomas (PTC), their detection in FNA smears could improve the diagnosis.
Methods: RNA and DNA was extracted from 104 routine air dried FNA smears (59 indeterminate, 29 malignant, 1 non- diagnostic, 15 non-neoplastic) and corresponding formalin-fixed paraffin-embedded tissue (FFPE) samples (54 follicular adenomas, 18 FTCs, 25 PTCs, 7 goiters). PAX8/PPARG and RET/PTC rearrangements were detected by fluorescence resonance energy transfer (FRET)-PCR while BRAF and NRAS point mutations were detected by FRET-PCR and high resolution melting (HRM)-PCR on a Roche LightCycler 480.
Results: The comparison of FRET- and HRM-PCR for the detection of point mutations in a subset of 50 FNA and FFPE samples revealed a significant improvement by HRM-PCR, the number of questionable results and PCRs with no result could be reduced, and the number of mutations detected could be increased. PAX8/PPARG rearrangements were detected in 5 FNA smears and in 3 FFPE samples with overlapping results in 2 FNA and corresponding FFPE samples. RET/PTC rearrangements were detected in 4 FNA smears and in 3 FFPE samples with overlapping results in 2 FNA and corresponding FFPE samples. BRAF mutations were detected in 10 FNA smears and in 19 FFPE samples with overlapping results in 7 FNA and corresponding FFPE samples. NRAS mutations were detected in 12 FNA smears and in 22 FFPE samples with overlapping results in 6 FNA and corresponding FFPE samples.
Conclusion: In summary, these data are the first to show feasibility of extracting RNA from routine air dried FNA smears for detection of PAX8/PPARG and RET/PTC rearrangements with RT-PCR. Moreover, HRM is more reliable and more sensitive than FRET-PCR in the detection of point mutations in FNA smears. These promising methodological advances may lead to the introduction of molecular analysis of routine air dried FNA smears in everyday practice, if confirmed in larger series of FNA and FFPE samples.
Shorter Telomere Length in Fnmtc is not Associated with Alterations in HTERT, TRF1, TRF2, RAP1, TIN2, TPP1 and POT1
Thyroid Cancer Clinical Saturday
Introduction: No susceptibility gene(s) for familial non-medullary thyroid cancer (FNMTC) has been identified. Short telomere length and inherited or acquired genetic defects in telomere length and maintenance have been associated with familial diseases and increased risk of cancers including FNMTC. The aim of this study was to determine whether telomere length, telomerase activity and six-proteins (shelterin) involved in regulating telomere length and/or telomerase activity are altered in a comprehensively screened kindreds with FNMTC.
Methods: Blood samples were collected from 6 families with FNMTC (13 affected, 35 unaffected), and 30 control cases (10 sporadic benign thyroid disease, 10 with sporadic thyroid cancer, 10 non-thyroid disease). All unaffected family members had screening thyroid ultrasound and thyroid fine needle aspiration biopsy, if a thyroid nodule was present, to exclude a thyroid cancer diagnosis. Both DNA and RNA were extracted from peripheral blood lymphocytes. Quantitative PCR (Q-PCR) and RT-PCR was performed to analyze relative telomere length (RTL) and gene copy number, and mRNA expression [(hTERT), TRF1, TRF2, RAP1, TIN2, TPP1, POT1], respectively.
Results: Affected members had shorter RTL as compared with unaffected members in kindreds with FNMTC and control groups (p=0.01). However, there was no significant difference in hTERT gene copy number or hTERT mRNA expression between affected and unaffected members with FNMTC. We also found no significant difference in DNA copy number and mRNA expression for TRF1, TRF2, RAP1, TIN2, TPP1 and POT1 between affected and unaffected members with FNMTC.
Conclusion: Telomere length is shorter in affected members with FNMTC. Altered copy number or expression in hTERT, TRF1, TRF2, RAP1, TIN2, TPP1 and POT1 do not appear to account for the difference in RTL between affected and unaffected members with FNMTC.
Department of Clinical and Molecular Medicine, University of Rome “Sapienza”, Rome, Italy
Thyroid Cancer Saturday
Introduction: Ataxia Telangiectasia (AT) patients develop, with an exceptional high frequency, different types of cancers, particularly breast carcinomas. The molecular defect consists in an alteration in the repair of double-strand DNA breaks. AT is detected in approximately 1 in every 40,000 live births, while the condition of AT carrier can be identified in approximately 1% of the general population. Because of the difficult in the detection of AT carriers, the frequency of tumors in such subjects is not known. Recently, our group develops a new non-invasive test to identify AT heterozygotes (htz) in the general population, by testing p53 centrosomal localization in cell-cycle stimulated peripheral blood lymphocytes. Aim of this study was to evaluate the occurrence of AT-mutated (ATM) gene hzt in a selected group of patients, affected by two different types of tumors, namely breast cancer and thyroid well-differentiated carcinoma.
Methods: Blood peripheral lymphocytes from a total of 13 patients (1 male and 12 females; age ranging from 46 to 71 years, with a mean age of 57.7 years) were analyzed to detect p53 centrosomal delocalization, associated with the presence of ATM gene heterozygous mutation.
Results: We detected the intermediate phenotype of 50% of lymphoid cells having p53 localized at the centrosome and the other 50% with p53 centrosomal delocalization, typically observed in AT htz patients, in one female (A.P.) 58 years of age. This result would give an estimate frequency of 7.7%, much greater compared to the 1% frequency in the general population, reported in literature.
Conclusion: In conclusion, despite the relatively low number of patients, our study suggests a possible role of ATM gene defect in the pathogenesis of thyroid and breast cancer, and indicate the possibility to apply this new test in the analysis of cancer patients in search of ATM gene htz mutation and in the general population to identify those subjects at high risk to develop cancer because of an impaired response to DNA damage.
Short Call Abstract Author Index
Abraham Nordling, M. SCP-10
Alzahrani, A. SCO-5
Armstrongm, M. SCP-7
Beekman, M. SCO-4
Berg, E. SCP-10
Bian, B. SCP-15
Bosenberg, E. SCP-14
Brown, S. SCO-4
Bystrom, K. SCP-10
Calissendorf, J. SCP-10
Cappola, A.R. SCO-4
Carty, S.E. SCP-7
Caturegli, P. SCP-8
Chaung, K. SCP-9
Chiu, H.K. SCP-12
Coyne, C. SCP-7
Dasyam, A.K. SCP-7
Deandreis, D. SCO-3
Den Heijer, M. SCO-4
Dillmann, W.H. SCO-1
Dutra, J. SCP-9
Eszlinger, M. SCP-14
Fagin, J.A. SCO-3
Ferlito, M. SCP-8
Ferraz, C. SCP-14
Filipsson Nyström, H. SCP-10
Fox, C.S. SCO-4
Fury, M. SCO-3
Gesuwan, K. SCP-15
Ghazarian, S. SCO-2
Grewal, R. SCO-3
Group, T. SCO-5
Gulati, N. SCP-15
Gupta, N. SCP-7
Hallengren, B. SCP-10
He, M. SCP-15
Hegedus, L. SCP-14
Ho, A.L. SCO-3
Hodak, S.P. SCP-7
Jansson, S. SCP-10
Jarjoura, D. SCO-6
Jorneskog, G. SCP-10
Karlsson, F. SCP-10
Kebebew, E. SCP-15
Kirschner, L. SCO-6
Krogdahl, A. SCP-14
Ladenson, P.W. SCO-2
Ladenson, P.W. SCP-8
Lahti, J. SCO-4
Landek-Salgado, M.A. SCP-8
Lantz, M. SCP-10
Larson, S. SCO-3
Lavra, L. SCP-16
Lebeau, S.O. SCP-7
Leboeuf, R. SCO-3
Mammen, J. SCO-2
McCarty, S.K. SCO-6
McCoy, K.L. SCP-7
Medici, M. SCO-4
Mendola, A. SCP-16
Meulenbelt, I. SCO-4
Minelli, C. SCO-4
Mingoia, C. SCP-16
Naitza, S. SCO-4
Nikiforov, Y.E. SCP-7
Nikiforova, M.N. SCP-7
Nyström, E. SCP-10
Ohrling, H. SCP-10
Ohrn, T. SCP-10
Paschke, R. SCP-14
Peeters, R.P. SCO-4
Pentlow, K.S. SCO-3
Pfister, D. SCO-3
Pistis, G. SCO-4
Porcelli, T. SCP-16
Porcu, E. SCO-4
Precht Jensen, E. SCP-14
Prodosmo, A. SCP-16
Pulkstenis, E. SCO-2
Rehfeld, C. SCP-14
Ricarte Filho, J.C. SCO-3
Ringel, M.D. SCO-6
Rosen, A. SCO-2
Saji, M. SCO-6
Sanna, S. SCO-4
Savino, G. SCO-1
Sciacchitano, S. SCP-16
Scott, B. T. SCO-1
Sherman, E. SCO-3
Shuldiner, A.R. SCO-4
Simon, P.E. SCP-9
Soddu, S. SCP-16
Stang, M.T. SCP-7
Suarez, J. SCO-1
Suarez-Ramirez, J.A. SCO-1
Subramanian, M. SCO-2
Sulkowski, M. SCO-2
Tanaka, T. SCO-4
Toniolo, D. SCO-4
Torring, O. SCP-10
Trompet, S. SCO-4
Tuttle, R. SCO-3
Volpato, C. SCO-4
Wallin, G. SCP-10
Walsh, J.P. SCO-4
Wang, H. SCO-1
Wolffenbuttel, B. SCO-4
Wu, G.T. SCO-1
Xing, M. SCO-5
Xu, H. SCP-11
Yip, L. SCP-7
Zhang, H. SCP-11
Zhang, X. SCO-6