
Abstract
Background:
Vitamin D is an immunomodulator and may affect autoimmune thyroid diseases. Vitamin D has also been shown to influence thyrocytes directly by attenuating thyrotropin (TSH)-stimulated iodide uptake and cell growth. However, it is unclear how vitamin D status is related to TSH at the population level. The goal of the present study was to investigate the relationship between vitamin D status and TSH levels according to thyroid autoantibodies in a population-based health survey in Thailand.
Methods:
A total of 2582 adults, aged 15–98 years, were randomly selected according to the geographical region from the Thailand 4th National Health Examination Survey sample. By study design, the sexes were equally represented. Serum levels of 25-hydroxyvitamin D [25(OH)D], TSH, the thyroid peroxidase antibody (TPOAb), and the thyroglobulin antibody (TgAb) were measured in all subjects.
Results:
The mean age was 55.0±0.4 (SE) years. In subjects positive for serum TgAb, serum TSH levels were higher, whereas total serum 25(OH)D levels were lower. In addition, the prevalence of vitamin D insufficiency in TgAb-positive subjects was significantly higher than that observed in TPOAb- and TgAb-negative subjects, whether based on cutoff values of 20 or 30 ng/mL: 8.3% vs. 5.6%, p<0.05; or 47.6% vs. 42.0%, p<0.05, respectively. However, vitamin D status was not associated with positive TPOAb and/or TgAb after controlling for sex and age. To explore the probable interaction between vitamin D status and age on serum TSH, analyses were performed according to age tertiles; it was found that higher 25(OH)D levels were independently associated with lower TSH, but only in subjects in the lowest age tertile.
Conclusions:
This population-based study showed that high vitamin D status in younger individuals is associated with low circulating TSH.
Introduction
Vitamin D is well recognized as an immunomodulator (12), and vitamin D insufficiency has been associated with autoimmune thyroid disease (13). Besides potentially affecting the thyroid gland through immune-mediated processes, vitamin D has also been shown to influence thyrocytes directly by attenuating the thyrotropin (TSH)-stimulated iodide uptake and cell growth of rat thyroid cells (14). On the other hand, it has been shown that vitamin D modulates TSH secretion of pituitary thyrotrophs by binding to specific binding sites (15). Moreover, an increased TSH level has been observed after acute administration of 1,25-dihydroxyvitamin D [1,25(OH)2D] (16). It is unclear, however, how vitamin D status is related to TSH levels at the population level. Therefore, the purpose of the present study is to investigate whether vitamin D status is associated with circulating TSH according to thyroid autoantibodies in a population-based health survey in Thailand.
Materials and Methods
Population
This study used data and blood samples from the Thai 4th National Health Examination Survey (NHES-IV) conducted in 2008–2009 by the National Health Examination Survey Office, Health Systems Research Institute. Subjects aged 15–98 years were randomly selected from 21 provinces in four geographical regions of Thailand as well as the capital city, Bangkok, using stratified, multistage probability sampling of the population aged ≥15 years, with a sample size of 21,960 individuals. Demographic data, such as age, sex, and religion, were included. Body mass index (BMI) was measured using standard procedure. Fasting blood samples were obtained and transferred to a freezer at a central laboratory in Ramathibodi Hospital, a university hospital in Bangkok, where they were kept at −80°C.
The present study used a subsample of the NHES-IV serum samples to measure serum levels of 25(OH)D. The subjects were randomly selected in 1:1 sex ratio according to the age group (15–29, 30–44, 45–59, 60–69, 70–79, and ≥80 years), region, and urban/rural place of residence from a sample size of 21,960. In each stratum, 25 individuals were randomly selected using statistical software. A total of 2700 were sampled, of which 2587 serum samples were available. Five subjects with marked hypothyroidism (serum TSH >50 mIU/L) were excluded from the study. The study was approved by the ethics committee of Ramathibodi Hospital. Informed consent was obtained from all subjects.
Serum 25(OH)D measurement
Serum 25(OH)D2 and 25(OH)D3 were analyzed by liquid chromatography–tandem mass spectrometry (LC-MS/MS) using an Agilent 1200 Infinity liquid chromatograph (Agilent Technologies, Waldbronn, Germany), coupled to a QTRAP® 5500 tandem mass spectrometer (AB SCIEX, Foster City, CA) using a MassChrom® 25-OH-Vitamin D3/D2 diagnostics kit (ChromSystems, Munich, Germany). The 25(OH)D assay was performed according to the manufacturer's instructions. This method used a deuterated 25(OH)D3 as an internal standard to correct for sample and instrument variability. Samples were analyzed using an atmospheric pressure chemical ionization source for maximum sensitivity. The 25(OH)D separation was performed using a Chromsystems precipitation reagent and trap column in conjunction with an Agilent 1200 high-performance liquid chromatography system configured for online sample preparation according to the configuration included in the documentation with this method. Briefly, 25(OH)D3 and 25(OH)D2 were extracted by mixing 100 μL of serum sample with 25 μL precipitation reagent and 200 μL of the internal standard solution. The mixture was vortexed for 20 seconds and incubated for 10 minutes at 4°C. After centrifugation of the mixture for 5 minutes at 9000 g, the upper layer was transferred to an autosampler vial and 5 μL was injected to the LC-MS/MS. The summation of serum 25(OH)D2 and 25(OH)D3 was used to reflect vitamin D status. The interassay and intra-assay coefficients of variation of total serum 25(OH)D level were 6.3% and 5.0%, respectively.
Serum TSH, Thyroid peroxidase antibody, and antithyroglobulin antibody (TgAb) measurements
Serum TSH, the thyroid peroxidase antibody (TPOAb) and the thyroglobulin antibody (TgAb) were measured by electrochemiluminescence immunoassay on a Cobas e 411 analyzer (Roche Diagnostics GmbH, Mannheim, Germany). The assays have an intra-assay precision of 3.6%, 9.2%, and 6.1%, respectively. Positive TPOAb and TgAb were defined as a value greater than 34 IU/mL and 115 IU/mL, respectively.
Statistical analysis
Data are expressed as mean±SE. Differences between two groups were assessed by the Student's t-test. Logistic regression analysis was performed to identify the predictive variables. Linear regression analysis was used to examine the relationship between vitamin D status and serum TSH. A p-value less than 0.05 was considered statistically significant. All analyses were performed using SPSS statistical software package, version 16.0 (SPSS Inc., Chicago IL).
Results
Table 1 demonstrates the clinical and laboratory characteristics of the remaining 2582 subjects. The mean age was 55.0±0.4 (SE) years. The mean level of total serum 25(OH)D [summation of 25(OH)D2 and 25(OH)D3] was 32.5±0.18 ng/mL. Women had a higher BMI, serum TgAb and TPOAb levels, but lower serum 25(OH)D levels than men. Figure 1 shows the distribution of log-transformed TSH levels. Four percent had serum TSH levels above 5 mIU/L, while 19.8% had serum TSH levels above 2.5 mIU/L. Of the 2582 subjects, 425 (16.5%) and 315 (12.2%) subjects were positive for serum TPOAb and TgAb, respectively. When subjects with positive serum TPOAb and/or TgAb were excluded, the distribution of TSH did not change appreciably.
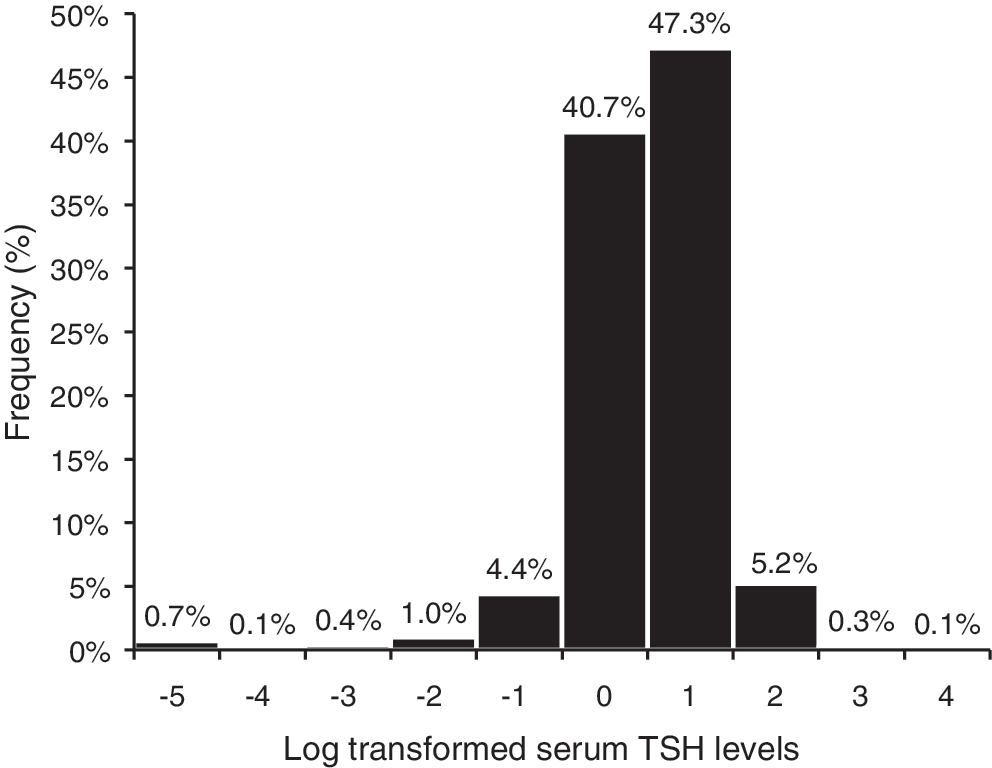
Distribution of log-transformed serum thyrotropin (TSH) levels.
Values are mean±SE.
Significantly different from men (p<0.001).
TSH, thyrotropin; BMI, body mass index; TPOAb, thyroid peroxidase antibody; TgAb, thyroglobulin antibody.
Table 2 compares the clinical and laboratory characteristics based on positive serum TPOAb, TgAb, and TPOAb and/or TgAb. Subjects with positive serum TPOAb and/or TgAb were older, had a higher serum TSH level, and included a lower proportion of males. After excluding subjects with positive TPOAb and TgAb, the mean serum TSH levels decreased from 2.09±0.04 to 1.94±0.03 mIU/L. In addition, the prevalence of vitamin D insufficiency [whether based on cutoff values of 20 or 30 ng/mL (17,18)] in TgAb-positive subjects was significantly higher than that observed in TgAb-negative subjects. Multivariate analysis using logistic regression revealed that independent determinants of positive TPOAb and/or TgAb were age and female sex. Serum 25(OH)D levels, however, were not associated with positive TPOAb and/or TgAb (Table 3), or positive TgAb alone (Supplementary Table S1; Supplementary Data are available online at
Values are mean±SE or number (percent). Cutoff values for serum TPOAb and serum TgAb were 34 IU/mL and 115 IU/mL, respectively.
NS, not significant.
OR, odds ratio; CI, confidence interval.
To account for the probable interaction between vitamin D status and age on serum TSH, further analyses were performed according to age tertiles. The mean age (±SD) of subjects in the first, second, and third tertiles were 29.2±9.2., 57.6±7.3, and 78.66±5.4 years, respectively. Serum TSH levels were log-transformed before regression analysis. With regard to the relationship between vitamin D status and serum TSH, it was found that higher 25(OH)D levels were associated with lower TSH independent of age, sex, BMI, serum TPOAb, and/or TgAb only in subjects in the lowest age tertile (Table 4). Age, BMI, and thyroid autoantibodies, but not 25(OH)D or sex, were associated with serum TSH in the upper age tertile.
Discussion
Similar to studies in other populations (19 –21), the distribution of serum TSH in our study did not follow a true Gaussian distribution, but was skewed toward the higher values. In addition (also not unlike other previous studies), serum TSH levels were higher in subjects with evidence of autoimmune thyroid disease, as indicated by the presence of TPOAb and/or TgAb. After excluding subjects with positive TPOAb and/or TgAb, the mean serum TSH levels decreased, which is likely to more accurately reflect the mean reference value of serum TSH. It is now well established that serum TSH levels are partially defined by ethnicity; hence, the reference value of serum TSH should be determined specifically based on ethnicity. Besides thyroid autoimmunity, factors previously reported to be related to TSH levels or thyroid hormones include age, sex, smoke exposure, and ethnicity (19,20,22). The association of circulating TSH with age and sex was also reflected in the present study.
With regard to the immune system, it has been found that vitamin D regulates the differentiation and activation of CD4+ T lymphocytes and can prevent the development of certain autoimmune disorders (23). Moreover, 1,25(OH)2D reduces the number of antigen-presenting cells in vitro (24). In vivo, 1,25(OH)2D has a direct immunosuppressive effect on dendritic cells and reduces the production of cytokines (25). Regarding autoimmune thyroid disease, previous studies have demonstrated a lower vitamin D status in Graves' disease (GD) (26,27), Hashimoto's thyroiditis (13), or thyroid autoimmunity (28). Moreover, an association between Graves' disease and vitamin D receptor (VDR) polymorphisms has been demonstrated in a number of studies (29). The effect of vitamin D on Graves' disease may not be mediated through the inhibition of antibody production, but by its effect on modulating autoimmune-induced thyroid hormone production (30).
In the present study, we could not demonstrate an independent relationship between vitamin D status and thyroid autoimmunity as assessed by the presence of TPOAb and/or TgAb. However, a number of limitations exist in the present study. First, TSH receptor (TSHR) stimulating antibodies were not measured in our study. Second, the study was cross-sectional in nature and the causative role of vitamin D, if any, on thyroid autoimmunity could not be readily determined. Lastly, in addition to environmental factors, genetics plays an important role in thyroid autoimmunity. Many genes have been proposed to be associated with GD (31), including genes encoding human leukocyte antigen (HLA) class II, cytotoxic T-lymphocyte antigen-4 (CTLA-4), protein tyrosine phosphatase-22 (PTPN22), TSHR, and more recently CD40 (32) and Fc receptor-like 3 (FCRL3) (33). It is possible that there might be an interaction between vitamin D status and genetic determinants of thyroid autoimmunity; this may render the effect of vitamin D less apparent if genetic variation in relation to thyroid autoimmunity is not concurrently determined.
We found in the present study that a higher circulating 25(OH)D was associated with lower TSH levels in younger individuals. Besides affecting the function of the thyroid gland through autoimmunity, it is likely that vitamin D may influence the thyroid gland through its action on the central nervous system and the thyrotrophs. There is evidence that vitamin D affects central nervous system function. Low vitamin D status may adversely affect brain development (34) and neurocognitive function (35). Moreover, vitamin D can enhance the responsiveness in TRH-induced TSH secretion of rat pituitary thyrotrophs (36). On the other hand, VDRs are present in thyrocytes and modulate their differentiation and function (15). It is therefore conceivable that the lower TSH in the presence of a higher vitamin D status observed in the present study could also be the result of increased thyroid hormones caused by the stimulatory effect of vitamin D on thyrocytes. (37). However, the underlying basis of the observed association of high vitamin D status with low serum TSH that is only present in the younger age group is unclear. Further clinical investigation of the effect of vitamin D supplementation on circulating TSH and thyroid hormones, particularly in younger individuals, is needed to elucidate an effect of vitamin D on either the thyrotrophs or the thyroid gland that might provide insight into this relationship.
Footnotes
Acknowledgments
This study was supported by: the Thailand Research Fund; the Health Systems Research Institute; the Bureau of Policy and Strategy, Ministry of Public Health; the Thai Health Promotion Foundation; and the National Health Security Office, Thailand. NHES-IV was conducted by the National Health Examination Survey Office, Health Systems Research Institute, Thailand. The NHES-IV study group included the following offices/regions: National Health Examination Survey Office (Wichai Aekplakorn, Rungkarn Inthawong, Jiraluck Nontaluck, Supornsak Tipsukum, Yawarat Porrapakkham); northern region (Suwat Chariyalertsak, Kanittha Thaikla [Chiang Mai University], Wongsa Laohasiriwong, Wanlop Jaidee, Sutthinan Srathonghon, Ratana Phanphanit, Jiraporn Suwanteerangkul, Kriangkai Srithanaviboonchai); northeastern region (Pattapong Kessomboon, Somdej Pinitsoontorn, Piyathida Kuhirunyaratn, Sauwanan Bumrerraj, Amornrat Rattanasiri, Suchada Paileeklee, Bangornsri Jindawong, Napaporn Krusun, Weerapong Seeuppalat [Khon Kaen University]); southern region (Virasakdi Chongsuvivatwong, Rassamee Sangthong, Mafausis Dueravee [Prince of Songkla University]); central region (Surasak Taneepanichskul, Somrat Lertmaharit, Vilai Chinveschakitvanich, Onuma Zongram, Nuchanad Hounnaklang, Sukarin Wimuktayon [Chulalongkorn University]); Bangkok region (Panwadee Putwatana, Chalermsri Nuntawan, Karn Chaladthanyagid [Mahidol University]). We thank Roche Diagnostics Thailand for kindly providing the TSH and TgAb assays and partial support TPOAb assay used in this study.
Disclosure Statement
The authors declare that no competing financial interests exist.