
Abstract
Background:
Thyrotoxic disease can be difficult to recognize in patients with resistance to thyroid hormone (RTH) because the clinical symptoms of thyrotoxicosis cannot be observed, and thyrotropin (TSH) may not be suppressed because of hormone resistance. Painless thyroiditis is a relatively common cause of thyrotoxicosis, but its occurrence in RTH has not been reported. We assessed the thyroid profile in a patient with RTH and episodes of thyrotoxicosis who experienced repeated painless thyroiditis.
Patient Findings:
A 44-year-old Japanese woman with RTH, which was confirmed by the presence of a P453A mutation in the thyroid hormone receptor β (TRβ) gene, showed a slight elevation of the basal levels of thyroid hormones, which indicated that her pituitary RTH was mild. She experienced a slight exacerbation of hyperthyroxinemia concomitant with TSH suppression. A diagnosis of painless thyroiditis was made because of the absence of TSH receptor antibodies, low Tc-99m pertechnetate uptake by the thyroid gland, and transient suppression followed by a slight elevation of TSH following the elevation of thyroid hormones. The patient's complaints of general malaise and occasional palpitations did not change throughout the course of painless thyroiditis. Three years later, painless thyroiditis occurred again without any deterioration of the clinical manifestations.
Conclusions:
Mild pituitary RTH can be overcome by slight exacerbation of hyperthyroxinemia during mild thyrotoxicosis. When pituitary resistance is severe and TSH is not suppressed, thyrotoxicosis may be overlooked.
Introduction
Patient
A 44-year-old Japanese woman was evaluated for an exacerbation of hyperthyroxinemia. She initially visited a hospital because of palpitations and general malaise at the age of 29. She lost 3 kg during the month prior to her hospital visit. She was referred to Ito Hospital (thyroid clinic), where SITSH was detected. Her free-T3 (f-T3), free-T4 (f-T4), and TSH levels were 6.9 pg/mL (reference range: 2.5–5.5 pg/mL), 2.44 ng/dL (reference range: 0.8–1.9 ng/dL), and 1.8 μU/mL (reference range: 0.3–3.5 μU/mL), respectively. The presence of antibodies to thyroid hormones and human anti-mouse antibody was excluded. The elevation of serum thyroid hormones then spontaneously normalized (f-T3, 3.2 pg/mL; f-T4, 2.32 ng/dL; TSH, 1.3 μU/mL). Subsequently, her palpitations and general malaise continued, and she was treated by a general practitioner with l-thyroxine and propranolol.
At the age of 36, she was referred to Showa University Hospital for a thyroid function evaluation. Upon physical examination, her heart rate was 80 bpm with 30 mg propranolol, and her thyroid enlargement was mild. Her serum f-T3 was 8.4 pg/mL (reference range: 2.2–4.1 pg/mL), and her serum f-T4 was 7.5 ng/dL (reference range: 0.8–1.6 ng/dL). TSH was undetectable on a dose of 150 μg
After obtaining informed consent, the thyroid hormone receptor β (TRβ) gene was sequenced by standard sequencing using an automated sequencer. The patient had a C to G transition at nucleotide position 1643 in one allele, which results in an amino acid substitution at codon 453 (P453A). This mutation has been reported in several cases of RTH (6).
At the age of 44, hyperthyroxinemia was exacerbated during a routine examination. TSH was suppressed (f-T3, 7.34 pg/mL; f-T4, 4.99 ng/dL; TSH, 0.03 μU/mL). The patient's complaints of occasional palpitations and continuous general malaise were unchanged, and no spontaneous pain or tenderness of the thyroid gland was noted. TSH receptor antibodies (DYNOtest TRAK human assay; Brahms Diagnostica, Berlin, Germany, provided by Yamasa Co., Japan) were negative. In addition, Tc-99m pertechnetate uptake (Tc uptake; 20 min) was low (0.74%; reference range 0.5–3%), which was compatible with destructive thyroiditis (<0.8% in painless thyroiditis without TSH receptor antibodies at Showa University Hospital and Showa University Fujigaoka Hospital). Low-echoic lesions, which generally signify subacute thyroiditis, were not observed by ultrasonography. Thyroglobulin antibodies were measured by radioimmunoassay and determined to be positive (3.9 U/mL; reference <0.3 U/mL), and thyroid peroxidase antibodies were negative. The serum TSH level was low in the following two months, at which point it became mildly elevated before returning to normal (Fig. 1). These findings led to a diagnosis of painless thyroiditis.
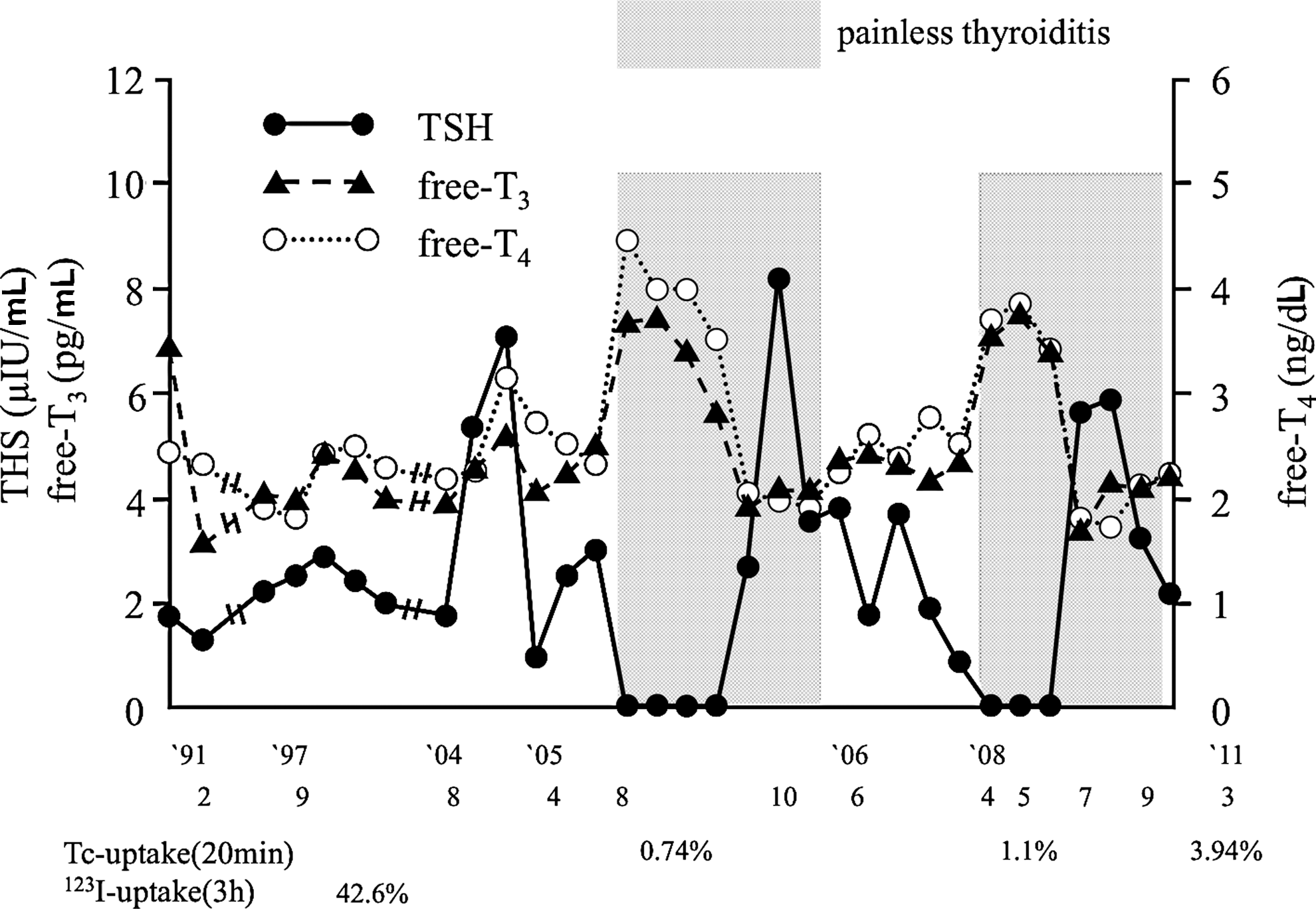
The serum levels of thyroid hormones and thyroid-stimulating hormone during the course of painless thyroiditis.
Three years later, painless thyroiditis recurred with a similar course of serum levels of free thyroid hormones and TSH (Fig. 1). Tc uptake (1.1%) was low compared with the uptake associated with Graves' disease, but relatively high compared with typical (without TSH receptor antibodies) painless thyroiditis. The Tc uptake was 3.94% after the patient completely recovered from painless thyroiditis, and her thyroid function was stable. Thus, the Tc uptake values during the thyrotoxic phases of painless thyroiditis were very low for this patient.
Discussion
Thyrotoxicosis can be difficult to recognize in patients with RTH because the symptoms of hyperthyroxinemia may be masked, or patients with RTH may already have manifestations of thyrotoxicosis, such as palpitations. In addition, a mild exacerbation of the elevated levels of serum thyroid hormones can be missed when TSH is not suppressed. In the present case, mild exacerbation of the serum thyroid hormone level was accompanied by a suppression of TSH, which led us to suspect the existence of concomitant thyroid disease with thyrotoxicosis, and we made a diagnosis of painless thyroiditis. Tc uptake was low compared with the uptake commonly observed in Graves' disease, but relatively high compared with patients with painless thyroiditis without RTH. However, the uptake was markedly low compared with the uptake observed when she was in a stable condition without painless thyroiditis. The patient experienced thyrotoxicosis three times, and we detected painless thyroiditis twice. It is difficult to determine whether the patient's first episode of hyperthyroxinemia with thyrotoxic manifestations and weight loss was a result of painless thyroiditis or transient Graves' disease.
Painless thyroiditis is a destructive thyroid disease with transient thyrotoxicosis that is usually followed by transient hypothyroidism (18). In most cases, thyroid function ultimately returns to its basal level. Painless thyroiditis is believed to be caused by autoimmune thyroid diseases, primarily chronic thyroiditis (also named Hashimoto's thyroiditis) and occasionally Graves' disease. Chronic thyroiditis is a common thyroid disease. It has been estimated that approximately 10% of adult women and 5% of men have antithyroid antibodies, and between 1 in 10 and 1 in 30 women in the general population have autoimmune thyroiditis (19). Moreover, Gavin et al. recently proposed that RTH may facilitate the immune response to thyrocytes (20). In addition, Barkoff et al. reported that individuals with RTH had an increased likelihood of thyroid autoimmunity compared with their first-degree relatives without RTH (21). Thus, a certain proportion of patients with RTH also have chronic thyroiditis. Indeed, cases of RTH and chronic thyroiditis have been reported, and some have been observed in hypothyroid patients. Painless thyroiditis is also a common thyroid disorder. Approximately 5% of patients with chronic thyroiditis experience destructive thyrotoxicosis (22). In addition, painless thyroiditis accounts for 5% of all cases of thyrotoxicosis (23). However, the occurrence of painless thyroiditis in patients with RTH has not been reported. Thyrotoxicosis is usually less severe in painless thyroiditis compared to Graves' disease. It is conceivable that such an occurrence could be overlooked when the excess thyroid hormone induced by painless thyroiditis is not sufficiently high to overcome resistance, and the manifestations of thyrotoxicosis would not be recognized.
The poor tissue responsiveness in RTH can be overcome by excess thyroid hormone. Patients with thyrotoxicosis and RTH manifested the symptoms of thyrotoxicosis, including hypermetabolic features, when the serum levels of thyroid hormones were sufficiently high to cause excess hormone activity (12 –16). Furthermore, TSH was suppressed in all reported cases of thyrotoxic diseases occurring in patients with RTH. The TSH levels were undetectable in half of the patients and very low in the other half (11 –17). When the symptoms of thyrotoxicosis are not apparent, TSH suppression is an important clue for coexisting thyrotoxicosis.
Although the in vitro severity of the dysfunction of mutated thyroid hormone receptor activity is determined by the individual mutation, there is no clear relationship between the type of mutation and the clinical phenotype. Even with the same mutation, clinical features vary among individuals (24). Factors other than the type of mutation are thought to be involved. In contrast, pituitary resistance, which reflects serum levels of thyroid hormones, has been postulated to be correlated with the degree of the defect of mutant receptors (25). Although there is considerable variation in individual f-T4 values among subjects harboring the same mutation, the average f-T4 value correlates with the impairment of T3 binding, except for mutant receptors with very low affinity to thyroid hormone and reduced dominant negative activity (26). Because the impairment of T3-binding activity of the P453A mutant, which our patient had, is high (17% of wild type), the mean pituitary resistance is hypothesized to be high. However, the serum thyroid hormone levels of RTH patients with the P453A mutation vary significantly among individual patients (6), indicating that pituitary resistance varies between affected individuals.
There is little data available concerning the level of thyroid hormones required to suppress TSH when patients with RTH also develop a second thyroid disorder, namely thyrotoxicosis. The TSH response to TRH with graded T3 administration in a small number of RTH patients showed that TSH suppression was correlated with the basal level of thyroid hormone (26), indicating that the degree of basal pituitary resistance determines TSH suppression by increased thyroid hormone. TSH suppression during thyrotoxicosis is not the same as that found during the short-term administration of T3, but it is conceivable that more hormones are necessary to suppress TSH in thyrotoxicosis when pituitary resistance is severe. In the present case, the slight increase in the basal levels of the serum thyroid hormones indicated that the pituitary resistance to thyroid hormone was mild. Therefore, the pituitary gland responded sufficiently to the slight exacerbation of serum thyroid hormone levels, and TSH was suppressed during the course of mild thyrotoxicosis induced by painless thyroiditis. When pituitary resistance is severe and TSH is not suppressed, thyrotoxicosis may be overlooked.
Footnotes
Author Disclosure Statement
No authors have competing financial interests to disclose.