
Abstract
Background:
The expanding use of 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET) has led to the identification of increasing numbers of patients with an incidentaloma in the thyroid gland. We aimed to review the proportion of incidental thyroid cancers found by 18F-FDG PET or PET/computed tomography imaging.
Methods:
Studies evaluating thyroid carcinomas discovered incidentally in patients or healthy volunteers by 18F-FDG PET were systematically searched in the PubMed database from 2000 to 2011. The main exclusion criteria were known thyroid disease, lack of assigned diagnoses, investigation of diffuse uptake only, or investigation of patients with head and neck cancer, or cancer in the upper part of the thorax.
Results:
Twenty-two studies met our criteria comprising a total of 125,754 subjects. Of these, 1994 (1.6%) had unexpected focal hypermetabolic activity, while 999 of 48,644 individuals (2.1%) had an unexpected diffuse hypermetabolic activity in the thyroid gland. A diagnosis was assigned in 1051 of the 1994 patients with a focal uptake, 366 of whom (34.8%) had thyroid malignancy. Likewise, a diagnosis was assigned in 168 of 999 patients with a diffuse uptake, 7 of whom (4.4%) had thyroid malignancy. In the eight studies reporting individual maximum standardized uptake values (SUVmax), the mean SUVmax was 4.8 (standard deviation [SD] 3.1) and 6.9 (SD 4.7) in benign and malignant lesions, respectively (p<0.001).
Conclusions:
Incidentally found thyroid nodules, using 18F-FDG PET, are at high risk of harboring malignancy if uptake is focal. SUV are significantly higher in malignant than in benign nodules. The pronounced inhomogeneity and other shortcomings of the studies are discussed.
Introduction
18F-FDG PET, with or without CT, is a noninvasive technique, widely used as a diagnostic tool and for the preoperative staging of various malignancies (11,12). 18F-FDG PET exploits the fact that many malignancies metabolize glucose at a much higher rate than normal tissues. However, and importantly, high cellular glucose uptake is nonspecific. Thus, tissues also harboring inflammatory cells have increased glucose metabolism (13), which constitutes a differential diagnostic challenge when 18F-FDG PET is employed in search of malignancy.
The increasing use of 18F-FDG PET or PET/CT has led to the identification of increasing numbers of patients with an incidentaloma in the thyroid gland (14 –16). The prevalence of malignancy in such lesions has varied between 0% (5) and 63.6% (17). The risk seems dependent on whether the 18F-FDG uptake is diffuse [prevalence of malignancy from 0% (5) to 13% (18)] or focal [prevalence from 10% (19) to 63.6% (17)]. As a potential way of discriminating between benign and malignant tissues, several studies have investigated maximum standardized uptake values (SUVmax) as a semiquantitative indicator of 18F-FDG uptake (17,20).
Our aim was to review studies dealing with the risk of malignancy in incidental findings in the thyroid gland found with 18F-FDG PET or PET/CT imaging. The focus being on the relative importance of whether the uptake is focal or diffuse, on the potential role of determining SUV, and on methodological differences and shortcomings.
Methods
Literature search
English language articles published from January 2000 to June 2011, as a source for descriptions of thyroid incidentalomas, were identified via a search in the PubMed database (Fig. 1). The following search strategy was used: #1, carcinoma OR cancer OR malignancy OR gland OR lesion OR disease staging; #2, positron emission tomography OR focal uptake OR fluorodeoxyglucose OR SUV OR diffuse uptake; #3, incidentally OR incidental OR incidentaloma OR incidentalomas OR unexpected; #4 thyroid. The categories were combined as follows: #1 AND #2 AND #4 OR #1 AND #3 AND #4. Our search was restricted to humans and resulted in a total of 602 abstracts extracted for further evaluation.
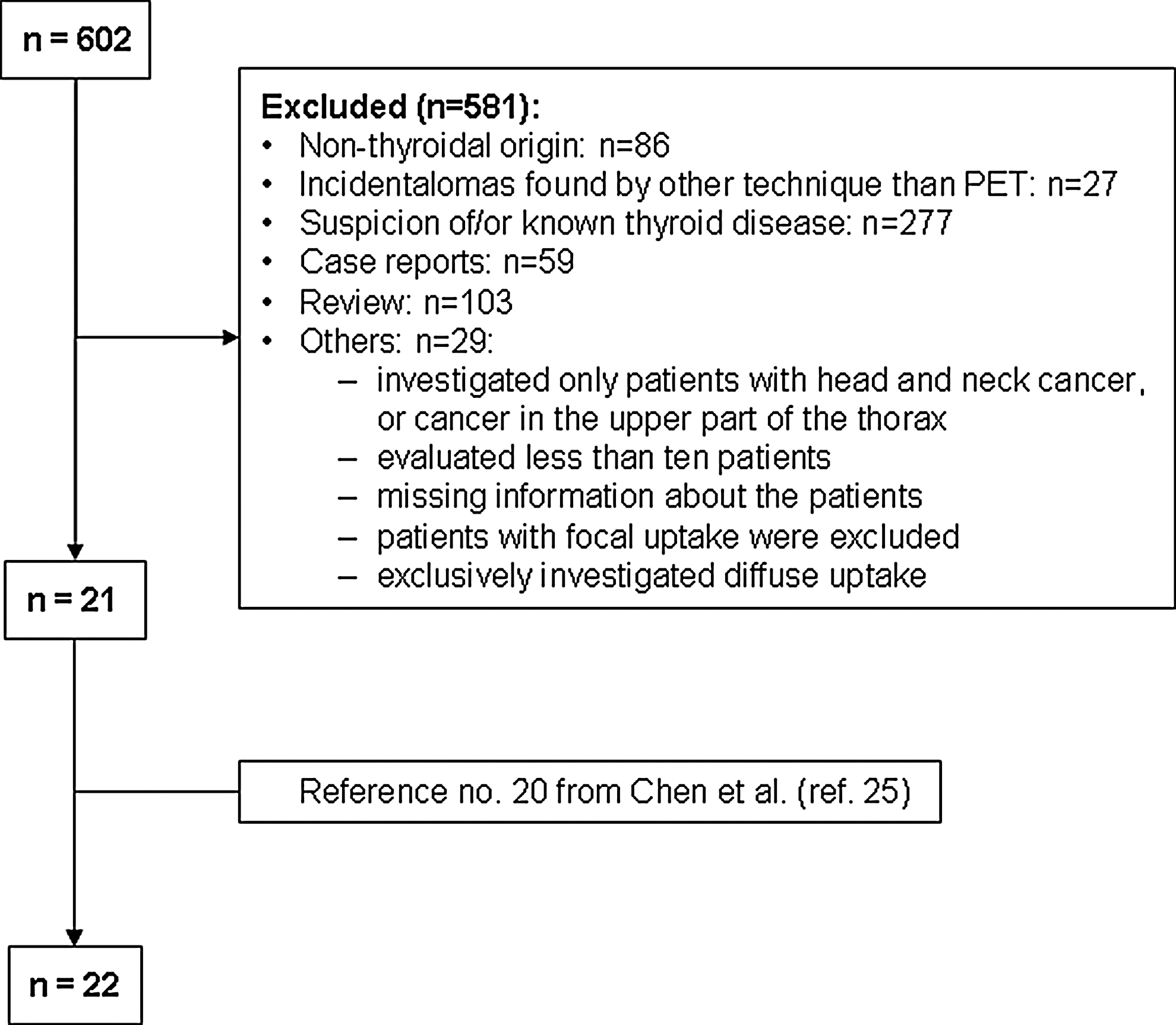
Flowchart showing the data extraction process.
Selection of literature sources
The 602 abstracts were evaluated using predefined inclusion and exclusion criteria. All of the following inclusion criteria needed to be met: incidental finding in the thyroid gland; incidentalomas being defined by the authors of the study as a focal as well as a diffuse thyroid uptake, or solely as a focal uptake, were included; articles were included regardless of their definition of limits for anatomical area of uptake, and the presence of a nodule was not a requirement; the participants in the studies were investigated with 18F-FDG PET or 18F-FDG PET/CT; investigated individuals were either healthy volunteers or individuals undergoing staging, restaging, or assessment of treatment response for nonthyroidal malignancies; there needed to be clinical follow-up or confirmation of thyroid disease by fine-needle-aspiration (FNA) or surgery.
Studies were excluded if they included participants with a prior history of thyroid disease; exclusively investigated diffuse uptake in the thyroid gland; were case reports; evaluated <10 patients; only investigated patients with head and neck cancer, or cancer in the upper part of the thorax.
Data extraction
Any study identified as relevant by reviewing its abstract was retrieved and analyzed as a full text. This yielded a total of 22 studies published as peer-reviewed articles (4 –10,14,15,17 –29). The reference lists of all these studies were scrutinized for additional relevant studies. Data extracted from the studies included first author, country of origin, year of publication, number of patients examined, imaging techniques, study period, number of patients with focal or diffuse thyroid uptake, patients without an assigned (this terminology is used when also patients without cytological or histological confirmation are included) thyroid diagnosis or lost to follow-up, patients with confirmed thyroid pathology, patients without pathology but follow-up, SUVmax for focal uptake, and cytological or histological diagnosis (Table 1).
n 1, subjects with a focal uptake; n 2, subjects with a follow-up; n 3, subjects with cancer; n 4, subjects with a diffuse uptake.
Only patients with focal uptake.
Some patients (from “n 2” in the column “Focal uptake”) were not assigned a final diagnosis due to indeterminate FNA.
Staging, restaging, or assessing treatment responses in various malignancies.
SUVmean analyzed instead of SUVmax.
Eight had no SUV and are therefore not included.
One patient had known thyroid cancer.
All lesions unexpected primary tumors.
Included only thyroid incidentalomas that underwent sonographically guided FNA.
Seven subjects were not included in the calculation.
CT, computed tomography; PET, positron emission tomography; NA, not analyzed; FNA, fine-needle aspiration; SUVmax, maximum standardized uptake value; SD, standard deviation.
Data synthesis
Based on the results of the 22 studies, the prevalence of malignancy in thyroid incidentalomas detected with 18F-FDG PET, with or without CT, was calculated. The total number of patients with an 18F-FDG PET uptake was reached by adding the patients from all the publications. To find the prevalence for unexpected focal as well as diffuse uptake in the thyroid gland, the ratio of patients with positive thyroid findings to the total number of patients was calculated. This was done separately for focal and diffuse uptake.
All findings were categorized into benign, malignant, and indeterminate, as evaluated in the studies by cyto- or histopathology, other imaging such as ultrasound, thyroid 99mTc scan, laboratory evaluation, or with follow-up clinical examinations. The malignant findings were further classified according to type of malignancy: papillary thyroid cancer (PTC) and follicular variant of PTC, follicular thyroid cancer (FTC), medullary cancer, Hürthle cell carcinoma, unspecified thyroid cancer, lymphoma, and metastatic disease from a nonthyroid malignancy. The prevalence of malignancy in patients with a focal uptake or a diffuse uptake was calculated separately by the ratio of assigned cases with malignancy and the total number of patients with follow-up in each group. A subanalysis was performed in eight studies that reported SUVmax for confirmed focal lesions, and thereby allowed calculation of the overall mean SUVmax for benign and malignant focal lesions.
In case of missing information an attempt was made to obtain this by contacting the authors of the articles in question.
Results
Pertinent data from the 22 studies are presented in Table 1. Twenty studies were retrospective studies and 2 were prospective cohort studies (9,28). The number of nodules per patient was not evaluated. Therefore, one patient with several focal nodules in a study was only registered once; for example, Choi et al. (6) reported two foci of thyroid malignancy in one patient. Eleven studies were carried out as a part of disease follow-up, which included staging, restaging, or assessing treatment responses in various malignancies (4,5,7,14,15,18,20 –24). Six studies were based on cancer screening in healthy volunteers and patients with suspected or known cancer (6,8,19,26,27,29). Two studies included only healthy volunteers (9,25). One study was carried out in patients with suspected or known cancer and patients with fever of unknown origin (10). Two studies provided no information on selection of subjects for 18F-FDG PET/CT (17,28). Application of CT varied among studies (see Table 1).
Of the 125,754 individuals in total, who had an 18F-FDG PET with or without CT scan performed, 1994 (1.6%) had a focal incidentaloma in the thyroid gland. Fourteen studies did not evaluate diffuse uptake (6,7,9,14,15,19 –26,28). Nine studies, one (15) of which did not provide analysis of the data, described both focal and diffuse uptake. In the remaining eight studies, diffuse uptake was seen in 999 of 48,644 (2.1%) individuals (4,5,8,10,17,18,27,29).
There were 1051 out of the 1994 (52.7%) patients with a focal uptake who had a follow-up. Of them, 1025 had a diagnosis assigned and 26 had an indeterminate lesion. A diagnosis was assigned in 168 of the 999 (16.8%) patients with diffuse uptake and none had an indeterminate lesion. There were 1774 patients with an 18F-FDG uptake in the thyroid gland who did not have an evaluation. This was either because they refused evaluation, or were lost to follow-up, or due to the advanced nature of the primary malignancy hindering further examination.
Focal uptake
The prevalence of focal uptake, evaluated in all 22 studies, varied from 0.1% (21) to 4.8% (14,29) (mean 2.0%). Among individuals with an assigned diagnosis, 366 of 1051 with follow-up (34.8%) were malignant, 659 (62.7%) were benign, and 26 (2.5%) were indeterminate. In 90.1% (924 of 1025) of patients with a benign or malignant diagnosis it was established by cytology or histology, whereas only 29.3% (271 of 924) were confirmed by operation (see Fig. 2). Two studies, Chen et al. (17) and Ishimory et al. (24), only provided the total number of patients with FNA and operation. Therefore, the number of patients operated in these two studies is unknown. Accepting FNA as a minimum requirement for diagnosis, the positive predictive value (PPV) of focal uptake by 18F-FDG representing malignancy would be no higher than 39.4% (364 of 924). PTC and follicular variant of PTC were the most prevalent thyroid cancer type (297 out of 366, corresponding to 81.1%). Fifteen (4.1%) patients had follicular cancer, 5 (1.4%) had medullary cancer, 3 (0.8%) had Hürthle cell carcinoma, 31 (8.5%) had unspecified thyroid cancer, 5 (1.4%) patients had lymphoma, and 10 (2.7%) had metastatic disease from other primary malignancies. One study did not disclose the subtype of cancer (23). Based on the above, in an incidentally found thyroid lesion with focal uptake, as evaluated in these studies, the prevalence of thyroid cancer varied from 10.0% (19) to 63.6% (17) (mean 36.0%).
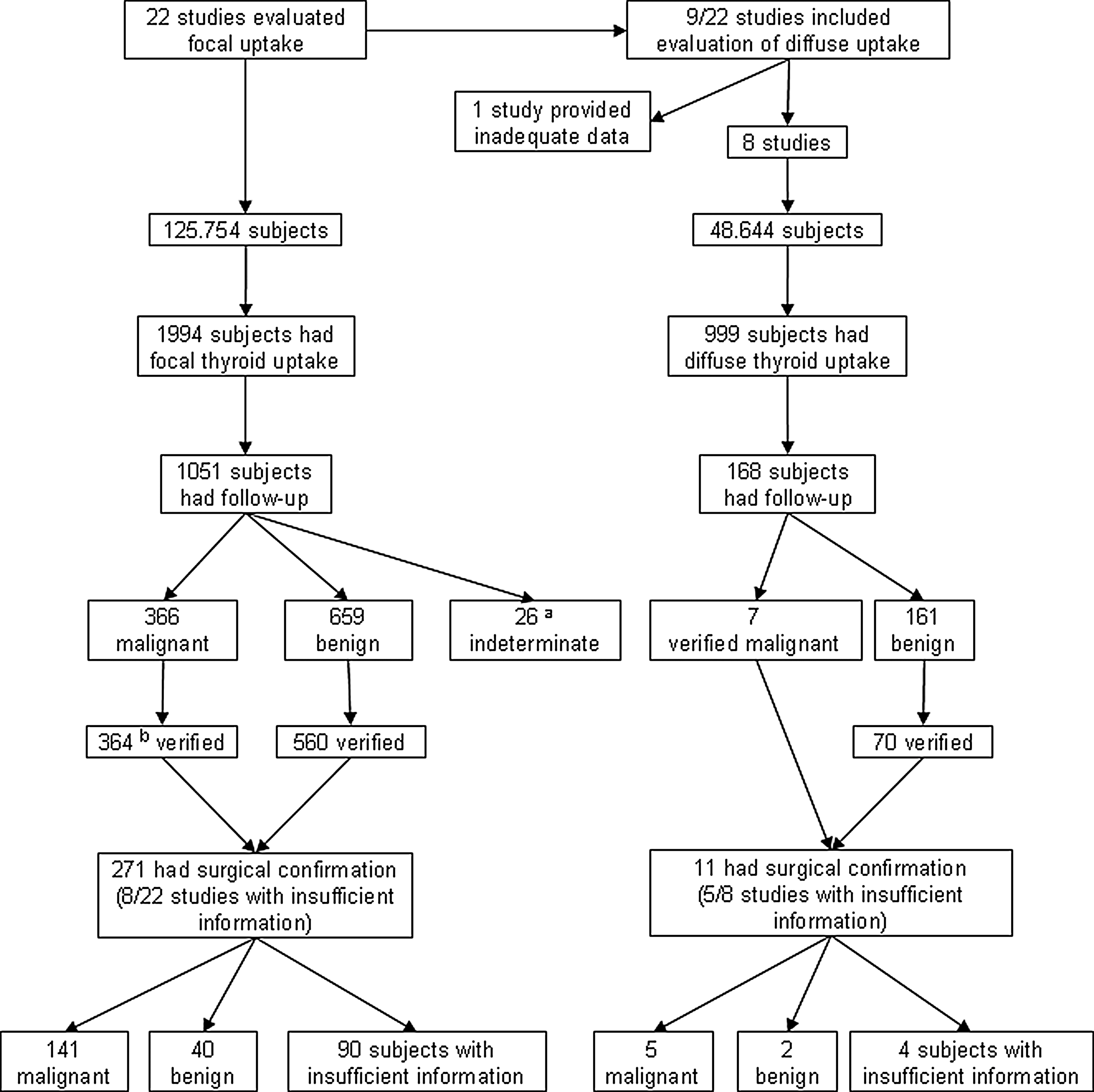
Patient attrition flowchart. “Verified” means that the diagnosis (benign or malignant) is based on either cytological or histological specimens. aClassified as indeterminate by fine-needle aspiration; bBogsrud et al. (20) had two malignant patients with no cytology.
In the 11 studies (5,6,8,9,19,22,25 –29) conducted in Asia the prevalence of focal uptake was 2.2% (1335 of 59,868) and rate of thyroid cancer was 34.6% (257 of 743 with follow-up). In the nine studies (4,7,14,15,17,18,20,21,24) conducted in North America the prevalence of focal uptake was 1.1% (564 of 52,486) and the rate of cancer was 35.5% (82 of 231 with follow-up). The remaining two studies (10,23) were performed in Europe. In these, the prevalence of focal uptake was 0.7% (95 of 13,400) and the rate of cancer was 35.0% (27 of 77 with follow-up). Thus, in Asia, the prevalence of focal uptake was more than twice that in the studies from North America and Europe while the risk of cancer was similar.
Diffuse uptake
The prevalence of diffuse uptake, evaluated in the eight studies (4,5,8,10,17,18,27,29), varied from 0.1% (10) to 4.5% (27) (mean 1.9%). In 77 of the 168 individuals (45.8%) with an assigned diagnosis this was established by cytology or histology. Only 14.3% (11 of 77) were confirmed by operation (see Fig. 2). Of the 168 patients, 7 (4.2%) had cancer (3 PTC, 2 FTC, and 2 unknown), 78 (46.4%) had chronic thyroiditis, and 83 (49.4%) had unspecified benign disorders. The prevalence of cancer in these eight studies varied from 0.0% (4,5,8,17) to 13.3% (18), with a mean of 3.9%.
Four out of eight studies (5,8,27,29) were performed in Asia. The prevalence of diffuse uptake was 3.4% (744 of 21,685) and rate of cancer was 3.5% (4 of 115 with follow-up). Three out of eight studies (4,17,18) were carried out in America. Here, the prevalence of diffuse uptake was 1.5% (239 of 15,919) and the rate of cancer was 5.4% (2 of 37 with follow-up). The remaining study (10) was performed in Italy. The prevalence of diffuse uptake was 0.1% (16 of 11,040) and the rate of cancer was 6.3% (1 of 16).
SUVmax for focal uptake
Eighteen of the 22 studies reported SUVs (4 –6,8 –10,14,15,17 –20,22,25 –29). Cohen et al. (4) and Chen et al. (25) reported individual SUVmean rather than SUVmax, and the latter reported SUVmean only for cancer patients. Bae et al. (27) and Are et al. (18) reported SUVmax as a combination of diffuse and focal uptake values. Six studies (6,17,22,26,28,29) did not list the individual SUVmax, but a mean SUVmax for all patients. Thus, only the remaining eight studies (5,8 –10,14,15,19,20) that listed individual SUVmax were included in the SUVmax analysis. In the study by Bogsrud et al. (20), two of the lesions suspected of malignancy were not included in the calculation of SUVmax since they were considered as extreme outliers. Nishimori et al. (15) and Pagano et al. (10) only provided an individual SUVmax for the malignant lesions.
The procedure for using 18F-FDG PET varied considerably between studies. The period of fasting before radiotracer administration varied from a minimum of 4 hours (14,17,23,24,26) to at least 8 hours (5,8,25). In only 10 of 18 studies (10,14,17,18,22,23,26 –29) information was available regarding the allowed maximum fasting serum glucose level. This level varied from 120 to 200 mg/dL. The time from the radiotracer administration to the PET imaging also varied between individuals (19,25,28) and between the studies, ranging from 40 minutes (4) to 90 minutes (20). Four studies (7,9,21,23) did not provide information on this variable.
A total of 80 assigned benign and 78 assigned malignant lesions were identified in the eight eligible studies. The mean SUVmax was 4.8 (3.1 standard deviation [SD]) for the 80 benign lesions and 6.9 (4.7 SD) for the 78 malignant lesions (p<0.001 between groups).
Discussion
Until not too long ago, the use of 18F-FDG PET—with or without CT, in the management of thyroid disease—was limited primarily to the postoperative staging of remnant disease in patients with known differentiated thyroid carcinoma (30). But the expanding use of PET in clinical practice stresses the need to clarify the clinical significance of incidental findings in the thyroid gland. Thus, the aim of this review was to determine the proportion of incidental thyroid cancers found by 18F-FDG PET—with or without CT of the thyroid gland—in individuals with no suspicion of thyroid disease, and to estimate the ability of PET—with or without CT—to determine whether the 18F-FDG uptake can differentiate between malignant and benign tumors. However, before trying to amalgamate the data, a number of essential factors need to be critically assessed.
Dissimilarities among studies
Comparing the studies is not straight forward, since there is pronounced heterogeneity regarding a number of crucial variables, such as inclusion and exclusion criteria, selection bias, study size, study origin and thereby differences in background risk of thyroid cancer, genetic and environmental/nutritional differences, and health status—whether known preexisting nonthyroidal malignancy or normal healthy volunteers were studied. On top of this, our interpretation is clouded by methodological differences related to performing the 18F-FDG PET—with or without the CT—and estimating the SUV, including observer-variation in relation to whether uptake is focal or diffuse. Generally, these issues have been given little attention although they most certainly influence the recorded data to a degree that is not clarified. Thus, while using a clear set of inclusion and exclusion criteria for this review, in order to obtain a more homogeneous group of studies, it is clear from the following that considerable inhomogeneity remains. Finally, as evident from Table 1, some studies lack crucial information, which—although authors were contacted—could not be retrieved. The studies were performed in different parts of the world where the incidence rate of thyroid cancer varies, as exemplified when comparing Asia and America. Thus, the incidence of thyroid cancer during 2004–2008 per 100,000 persons was 10.9 in Asia and 6.3 in America (31). Interestingly, the studies showed that the prevalence of focal uptake in Asia was twice as high as in the studies from America, while the rate of cancer was almost the same. Additionally, the studies vary regarding the health status of the subjects. Two studies included only healthy volunteers (9,25) whereas the other studies reviewed patients with known malignancy. Based on the above, it is clear that any conclusions drawn from these very inhomogeneous studies can only be very crude ones.
Focal uptake
On average 34.8% of individuals with focal uptake were found to have thyroid malignancy with PTC and follicular variant of PTC being the most prevalent. Of these thyroid malignancies, 95.9% were new primary malignancies, while the remaining were metastases from other cancers. In 15 studies (6,10,14,15,17,18,20 –25,27 –29) PET/CT was used. Choi et al. (6) found that 16 of 18 (88.9%) of the malignant thyroid lesions had low attenuation on CT. All focal thyroid lesions with a diffuse increase in surrounding thyroid uptake, or very low attenuation on CT, were benign. Focally increased 18F-FDG uptakes in the thyroid gland without a corresponding discernible focal anatomic lesion on CT also indicated a benign lesion with 100% certainty (6). Therefore, uptake of 18F-FDG PET in incidental findings in combination with CT should be regarded as a more precise method than 18F-FDG PET alone, for differentiating between malignant and benign findings.
The ultimate goal of the evaluation of uptake in the thyroid, using 18F-FDG, is to differentiate between benign and malignant lesions. Ideally, a gold standard (e.g., surgical removal) should be available to assess sensitivity and specificity of 18F-FDG uptake for the diagnosis of thyroid disorders. Only 29.3% (271 of 924) of focal uptake lesions were confirmed by operation. Thus, only a minority had a definitive diagnosis, in part probably explained by 20 of 22 studies being retrospective. Accepting FNA as a minimum requirement for diagnosis, the PPV of focal uptake by 18F-FDG representing malignancy would be no higher than 39.4%. One cannot exclude that surgical confirmation was most likely obtained in those patients with the highest likelihood of malignancy and therefore the malignancy risk in focal uptake is overestimated. Most importantly, it is unclear whether there is a true variation as for rate of thyroid malignancy [10.0%–63.6% (17,19)], or if this is related to methodological variation.
Diffuse uptake
Fourteen out of 22 studies did not evaluate diffuse uptake at all. Seven studies (15,19,21 –24,26) gave no reason for only investigating focal uptake, while seven studies (6,7,9,14,20,25,28) did not investigate diffuse uptake because previous reports indicated that the majority represented benign disease, such as chronic thyroiditis or Graves' disease.
Based on the overall data from eight studies reporting on diffuse 18F-FDG uptake, the prevalence of thyroid malignancy is 4.2%. Kim et al. (5) found that 34 of 45 patients with diffuse thyroid 18F-FDG uptake had chronic thyroiditis. In support, Chen et al. (17) reported the same diagnosis in 21 of 21 patients. Karantanis et al. (32) investigated 133 patients with diffuse thyroid uptake and found that 63 (47.4%) of them had the clinical diagnosis of hypothyroidism or autoimmune thyroiditis. None had thyroid cancer. Hence, diffuse 18F-FDG uptake rarely indicates thyroid cancer, but cannot exclude it. It is important to note that in the eight studies that evaluated diffuse uptake, only 16.8% (168 of 999) of patients had a final diagnosis, of whom only 45.8% (77 of 168) had a cytological or histological confirmation. It follows that sensitivity and specificity are affected with considerable uncertainty, and risk of malignancy potentially overestimated. The data cannot clarify whether patients with diffuse uptake on 18F-FDG PET need FNA or surgery.
SUV evaluation
The 18 studies (4 –6,8 –10,14,15,17 –20,22,25 –29) that evaluated SUVs compared their findings with the results of earlier studies. 18F-FDG is a radioactively marked glucose analogue that has a half-life of 110 minutes. The 18 studies varied considerably regarding the method for calculation of the SUV. This concerned length of fasting period before the examination, level of fasting serum glucose, volume of injected 18F-FDG, and the time from the radiotracer administration to the PET imaging. It follows that there is not only an individual patient or technique variation but also a procedure variation and therefore a direct comparison of SUV between studies may be heavily biased.
Nine studies (6,8,14,17,20,22,26,28,29) have reported mean SUVmax and investigated whether they could be used to differentiate between malignant and benign lesions. Five of these studies (6,8,22,28,29) found a significant difference. In the present review, we collected the SUVmax from eight studies and calculated the mean SUVmax, as being 4.8±3.1 for benign lesions versus 6.9±4.7 for malignant lesions. This suggests a potential utility of SUVmax in differentiating malignant lesions from benign lesions, although there is pronounced overlap. Using a high SUVmax as the sole indicator of cancer may be misleading, since both benign Hürthle cell adenomas and follicular adenomas have higher SUVmax compared with other benign conditions (18,20). In patients with known thyroid nodules, Mitchell et al. (33) investigated 31 patients with 48 thyroid lesions who underwent FNA and 18F-FDG PET/CT before surgical resection. A total of 15 of 48 (31%) lesions were malignant. In that study the mean SUVmax was significantly higher in malignant lesions than in benign nodules (6.5 vs. 2.4).
The high rate of malignancy in thyroid PET incidentalomas has been explained in two ways (34). First, 18F-FDG uptake often reveals malignant tumors because neoplastic cells exhibit increased rates of glycolysis and glucose consumption with accelerated production of glucose transport proteins (35). Second, most subjects submitted to 18F-FDG PET studies are patients who are having cancer staging, restaging, or assessment of treatment responses of various malignancies, in which the pretest probability for secondary tumors may be higher (34). Yet another explanation might be the increasing use of advanced technology in the diagnosis of a variety of illnesses, whereby otherwise unrecognized microcarcinomas are discovered.
A large-scale retrospective study from the United States looked at the incidence and mortality of thyroid cancer over a 30-year period (36). This review found that, although the incidence of thyroid cancer had more than doubled during this period, mortality from the disease had remained stable. Further, Ito et al. (37) performed a study over an 8-year period during which 732 patients had an ultrasound-guided FNA diagnosis of papillary carcinoma, 162 of whom chose observation. During the follow-up period, 70% of the tumors in the observational group remained the same size or decreased in size.
Patients suspected of having a new thyroid cancer, based on increased focal uptake of 18F-FDG, are facing a new diagnosis, a new set of concerns, and diagnostic as well as therapeutic choices. Since it is unclear whether thyroid cancers detected in this way, compared with any other way, have a different prognosis it is pertinent to investigate whether the detection mode affects prognosis, quality of life, and mortality.
Conclusion
We found that, despite the inhomogeneity in the studies, the risk of cancer seems markedly higher when patients have a focal uptake compared with a diffuse uptake on 18F-FDG PET. The overall risk is probably overestimated since pathological confirmation was obtained in patients with the highest probability of malignancy. The potential value of SUV determination, although higher in malignant than in benign lesions, needs more study with standardized methodology. It remains to be clarified whether malignancy detected by 18F-FDG PET alters prognosis, mortality, and most importantly quality of life of the patients.
Footnotes
Disclosure Statement
None of the authors have received any financial or other type of compensation related to the subject of this article. There are no competing financial interests.