
Abstract
Background:
Graves' disease (GD), including Graves' ophthalmopathy or orbitopathy (GO), is an autoimmune disease with an environmental and genetic component to its etiology. The genetic contribution to the GO clinical phenotype remains unclear. Previous data from our laboratory and others have suggested that GO has no specific genetic component distinct from GD itself, while other reports have occasionally appeared suggesting that polymorphisms in genes such as CTLA4 and IL23R specifically increase the risk for GO. One of the criticisms of all these reports has been the clinical definition of the GO phenotype as distinct from hyperthyroid GD devoid of clinically significant eye involvement. The objective of this study was to take advantage of a phenotypically pure group of GD patients with GO and examine a series of genes associated with GD to determine if any were more definitively associated with GO rather than Graves' thyroid disease itself.
Methods:
To further examine whether specific susceptibility genes are associated with GO, we have performed further genetic association studies using highly characterized GO patients, many of whom had undergone orbital decompression surgery for their exophthalmos. We genotyped HLA, CTLA4, IL23R, and TSHR genes in a group of 256 Caucasian patients with severe GO (n=199) and less severe GO (n=57), and 90 patients with GD but no clinically apparent GO.
Results:
We found that the allele and genotype frequencies were not statistically different between GO and non-GO patients for any of the genes and gene combinations assessed.
Conclusions:
These results provide further evidence that patients with GO do not have a distinct genetic susceptibility to their eye disease and again suggest that environmental and/or epigenetic influences are at play.
Introduction
A variety of gene polymorphisms have been found to be linked and/or associated with GD, and the genes involved have fallen into two distinct groupings. The first group is those genes common to many autoimmune diseases and involving immune regulatory and response genes. These include HLA-DR3 (7,8), CTLA4 (9,10), PTPN22 (11,12), CD40 (13,14), IL2RA (CD25) (15,16), FCRL3 (17,18), and the IL23R (19). The second group includes genes that are specific to the thyroid gland: the TSHR (20 –24) and thyroglobulin (TG) (25,26). However, the distinct factors predisposing GD patients to the development of GO remain unclear (27). While claims for preferential genetic associations with GO (19,28) have been made, our own data have not substantiated such reports (23,27).
To further examine whether any of the known gene associations are more likely to be associated with GO rather than just GD, we have re-examined the association of some of the gene polymorphisms claimed to be associated with GO. We have used a group of well-defined patients with GD including almost 200 patients who had undergone orbital decompression surgery. In this group of GO patients, there can be no doubt about the severe clinical phenotype and no doubt about the diagnosis—a criticism made against many earlier genetic studies of patients with GD. Nevertheless, our conclusions remain unchanged. There is no evidence to date that patients with GO have a genetic signature any distinct from patients with GD who do not develop GO.
Methods
Subjects
DNA was obtained from 346 Caucasian patients with GD as described in Table 1. These studies were approved by the Mount Sinai Institutional Review Board. A total of 199 patients with severe GO had undergone orbital decompression cosmetic surgery for their disease, and 57 had less critical GO but all had Werner class IIIa or higher GO (4,29), as well as 90 patients who had no clinical signs of eye disease (non-GO, or GD without GO). All patients had over a 2-year history of AITD. GD was defined as the presence of chemical hyperthyroidism and a normal or increased diffuse thyroid radioiodine uptake and/or the presence of TSHR antibodies. GO (also known as thyroid eye disease and dysthyroid/thyroid-associated orbitopathy) was defined clinically as a chronic autoimmune inflammatory disorder impacting the orbit around the eye, presenting various eye features as described (30). A group of Caucasian controls (n=402) was available from commercial sources (Coriell Institute, Camden, NJ).
The numbers represent individual subjects.
GO, Graves' ophthalmopathy; GD, Graves' disease.
HLA-DR3 typing
Positive or negative HLA-DR3 was typed by the method of group-specific polymerase chain reaction (PCR) amplification followed by restriction enzyme digestion as described by Westman et al. (31).
Genotyping
TSHR single-nucleotide polymorphism (SNP)—TSHR-SNP-rs2268458, which we have previously found to be associated with GD (23)—is located in intron 1, and was measured using standard PCR-RFLP procedures. The protocol was the same as described in the previous study (23). Human genomic DNA (∼25 ng) was amplified by PCR and 415-bp products were generated. Primer 1 was 5′-CCAGCAGAGGGAGCA CAA-3′, and primer 2 was 5′-TAGAGAATAGAGCAGCAA GAGACT-3′.
These primers flank the DNA fragment in TSHR gene intron 1. The PCR (25 μL) containing 1U Platinum Taq polymerase was carried out as directed by the manufacturer (Invitrogen Corporation, Carlsbad, CA). The PCR parameters were as follows: 95°C for 5 minutes, 35 cycles (95°C for 1 min, 52°C for 1 min, and 72°C for 1 min), followed by 72°C for 10 minutes. Then, 8 μL of PCR products were digested for 2 hours in 10 μL total volume with the restriction endonuclease AluI according to the manufacturer's instructions (New England BioLabs, Inc., Beverly, MA) along with a nondigested DNA control. After digestion, the digested fragments were mixed with a gel loading buffer, separated on a 3% agarose gel, visualized by ethidium bromide and UV light, documented with FluorChem®HD2 Imaging System (Alpha Innotech Corporation, San Leandro, CA), and analyzed by the genotype patterns. Since AluI digestion determines AGTT versus AGCT, this allowed the determination of each individual hetero- or homogenotype. The patterns were recorded as TT with one 333-bp DNA fragment, TC with one 333-bp and one 275-bp fragments, and CC with one 275-bp fragment.
CTLA4 SNP
The CTLA4 exon 1, A49G SNP was assayed by the same method as described above, but using a different primer pair and the BbvI restriction enzyme (New England BioLabs, Inc., Beverly, MA) (32). The forward primer was 5′-GCTCTAC TTCCTGAAGACCT-3′, and the reverse primer was 5′-AGTC TCACTCACCTTTGCAG-3′.
The A allele resulted in an undigested PCR product of 162 bp; the G allele resulted in a digested PCR product, showing 90- and 72-bp fragments viewed as one bold band on the agarose gel, and representing each individual hetero- or homogenotype.
IL23R SNP-rs10889677
The IL23R SNP-rs10889677 (located in the 3′ untranslated region 309 bases downstream the stop codon) was genotyped by the same method as described above, but using a different primer pair and the MnlI restriction enzyme (New England BioLabs, Inc., Beverly, MA) (19). The forward primer was 5′-AGGGGATTGCTGGGCCATAT-3′, and the reverse primer was 5′-TGTGCCTGTATGTGTGACCA-3′.
The A allele resulted in an undigested PCR product of 216 bp; the C allele resulted in a digested PCR product, showing 154- and 62-bp fragments on the agarose gel, and representing each individual hetero- or homogenotype.
IL23R SNP-rs2201841
The IL23R SNP-rs2201841 (located in intron 7) was genotyped by the same method as described above, but applying a fluorescent-based restriction fragment length polymorphism method and using a different primer pair and the HpyF3I restriction enzyme (19). The forward primer was 5′-GGCC TATGATTATGCTTTTTC
The forward primer was fluorescently labeled. The A allele resulted in an undigested PCR product of 188 bp; the G allele resulted in a digested PCR product, showing 163 and 25 bp fragments; and the 163-bp fragment contained the fluorescently labeled forward primer. The PCR products were separated and visualized on an ABI 3130xl genetic analyzer, and finally analyzed by GeneMapper software (Applied Biosystems, Foster City, CA) in order to assign each allele.
Statistical analyses and power calculations
Patient groups were clearly defined for the association studies. Differences in allele frequencies and genotypes between the groups were analyzed by the Chi-square test (χ 2) and Fisher's exact test (where appropriate). All tests were two tailed, and p<0.05 was considered as significant. Using the Centers for Disease Control (CDC) simulation software (Epi Info v.3.5.3.), we were able to define the limits of our analyses. This indicated that a sample patient group size of 256 GO and 90 non-GO subjects would enable detection of genetic associations, with 80% power, with odds ratios of >1.74, >1.74, >1.80, >1.87, and >1.91 for HLA-DR3, CTLA4, TSHR, IL-23R-rs10889677, and IL-23R-rs2201841, respectively, with an alpha of 0.2.
Results
Comparing GD patients with and without GO
To determine a genetic basis for the clinical phenotype known as GO, we compared patients with and without this clinical manifestation of GD. For the well-established polymorphisms associated with GD, we found no difference in the prevalence between those patients having GO and those without clinical evidence of GO. This observation applied to the presence of HLA-DR3, CTLA4, IL-23R, and the TSHR (Table 2). No significant differences were observed for any of the measured polymorphisms.
SNP, single-nucleotide polymorphism; TSHR, TSH receptor.
HLA-DR3
About 45.4% (n=346) of patients with GD had HLA-DR3 compared with 22.9% (n=402) of controls (p<10−7). There was no significant difference in the percentage of HLA-DR3-positive patients in the GO group (44.9%) (n=256) compared to the non-GO group (46.7%) (n=90) (Fig. 1, Table 2). The non-GO group also had significantly more HLA-DR3-positive members than the control group (p=0.0000046).
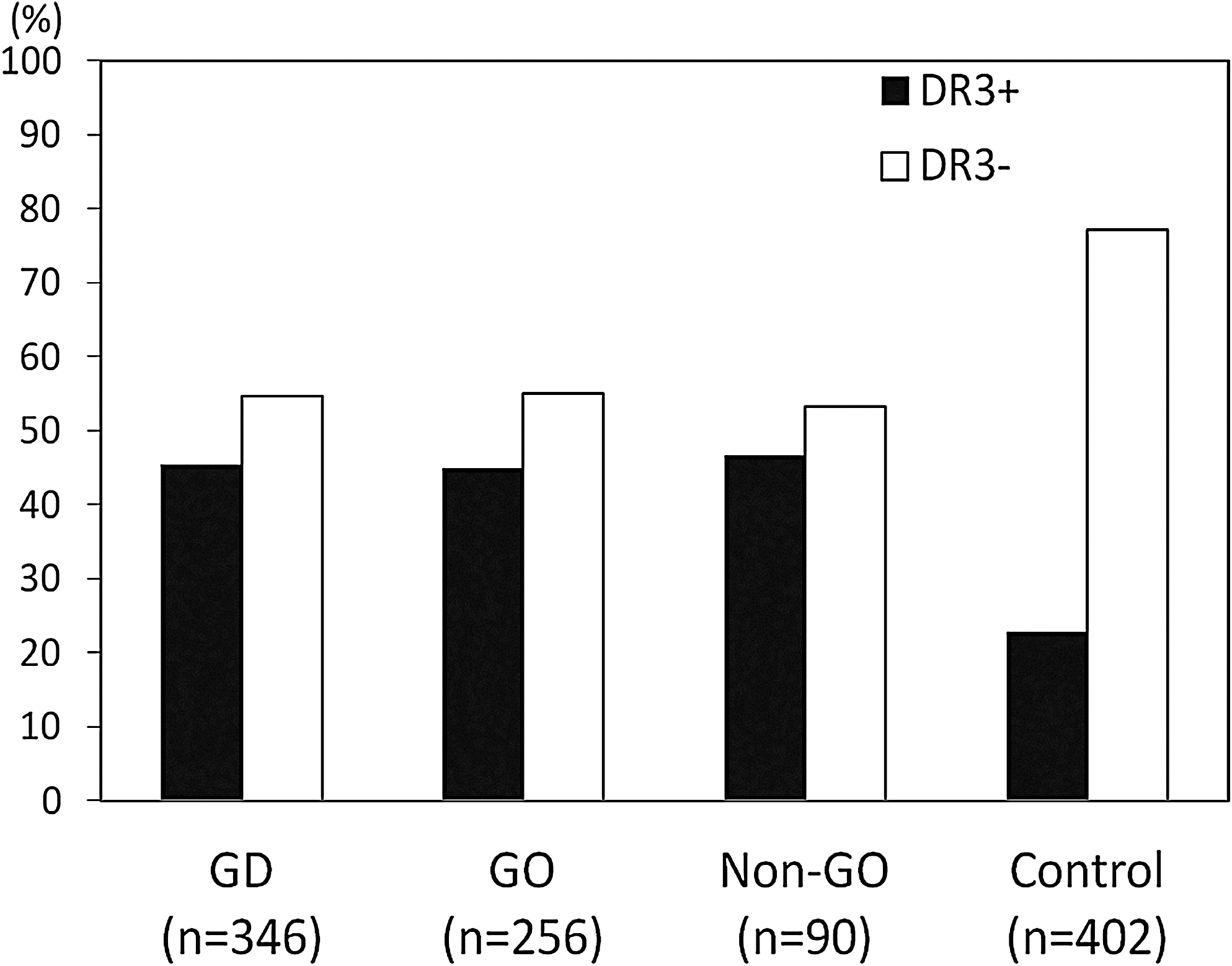
HLA-DR3 in autoimmune thyroid disease. The X axis shows the genotyping results of HLA-DR3-positive (DR3+) and HLA-DR3-negative (DR3−) samples from patients with all Graves' disease (GD), Graves' ophthalmopathy (GO), GD without GO (Non-GO), and control. The Y axis shows the HLA-DR3 genotyping frequency (%) in tested samples. They were significantly different when comparing GD, GO, and Non-GO with control, respectively (p<1×10−8, p<1×10−8, and p=0.0000046). There is no significant difference between GO and non-GO (p=0.775).
CTLA4 and IL23R
The G allele of the CTLA4 A49G SNP, previously reported as more significantly associated with GO rather than non-GO patients (28), was found in 41.2% of the GO patients, which was not different from the prevalence of this polymorphism in the group of patients without GO (40.6%) (Table 3). Similarly, examining two SNPs in the IL23R gene, which have also been previously reported to be associated with GO rather than non-GO (19), were again similar with no significant differences in the prevalence of the alleles of these SNPs or their genotypes (Tables 2 and 3).
TSHR
Polymorphisms in TSHR have been widely associated with GD but not Hashimoto's thyroiditis, and we have previously failed to observe a preference for patients with GO (23). The present report found the same result in this larger patient cohort dominated by patients with severe disease (Tables 2 and 3).
Comparing GD patients with severe GO and less severe GO
When severe GO was defined as only those patients undergoing decompression surgery, we also found no difference in any of the gene polymorphisms comparing such patients with those not requiring surgery and defined as less severe disease although this also most likely included patients who refused surgery (Table 4).
Genetic profiling of patients with GD
Examining patients for the presence of multiple GD-associated polymorphisms showed that <1% of GD patients harbored none of the selected gene polymorphisms examined. In contrast, ∼10% of patients showed all five of the GD-associated polymorphisms (Table 5). There was no significant difference in the number of measured polymorphisms between GO and non-GO patients. The number of patients with all five polymorphisms was also similar in those groups of patients with GO and those without GO (Table 5).
Gene/SNP: HLA-DR3, CTLA4, IL23R-rs10889677, IL23R-rs2201841, and TSHR.
Gender
When the patients were divided by gender, there were no significant differences in any of the measured polymorphisms between GO and non-GO in exclusively male or female patient groups (Table 2).
Relationship of HLA-DR3 with other susceptibility genes
We further analyzed whether HLA-DR3 was directly associated with the other susceptibility genes examined. Supplementary Table S1 (Supplementary Data are available online at
Discussion
We now know that GD is a complex genetic disease with significant genetic and environmental influences that may exert their effects via epigenetic mechanisms (26,33 –35). The susceptibility genes have been identified both by the candidate gene approach and by whole genome linkage and association studies (36). The identified genes have, to date, each provided only a small contribution to genetic susceptibility, including the TSHR gene (22,23), indicating that many genes must be involved. However, the concept of major, or necessary, gene polymorphisms that have to be inherited to develop the disease does not appear to apply to GD (37,38). A further conclusion from such information is that the same clinical phenotype of GD may be obtained by the conjunction of different susceptibility genes in different individuals and in different populations.
One of the most obvious clinical phenotypes of GD is the orbitopathy. GO may be a most disabling condition with very unsatisfactory treatment approaches (30,39,40). The primary antigen appears to be the TSHR expressed on fibroblasts and adipocytes throughout the body, but they find themselves in a retroorbital environment that exacerbates the immune response to their presence (40 –42). The argument over whether GO is a disorder distinct from GD and simply inherited at the same time appears less impressive now that the TSHR has been identified as an important antigen and that titers of TSHR antibodies correlate with the disease (40,41). In the present study and in our previous observations (23), TSHR gene polymorphisms were no more prevalent in the population of patients with GD and GO compared to patients without GO. Nevertheless, the thought has persisted that particular susceptibility must bias a patient toward the development of the eye phenotype rather than such patients simply having a worse form of the same disorder. While some studies have suggested that all patients with GD have a degree of eye involvement (2,27,43,44), others have suggested that GO has a genetic etiology rather than the more likely environmental cause, whether it be orbital anatomy, smoke, or trauma (19,28). Hence, CTLA4 gene polymorphisms were claimed as the immune mechanism pushing patients to a more severe retro-orbital inflammatory response (28), while most recently IL23R has been said to be responsible (19).
The CTLA4 gene is an immune regulatory molecule that is expressed on the surface of Helper T cells and transmits an inhibitory signal to T cells. Hence, deficient CTLA4 activity is associated with exacerbated T cell reactivity. CTLA4 gene polymorphisms have been shown to confer susceptibility to several autoimmune diseases, including AITD. However, CTLA4 was not demonstrated as a specific GO-associated gene in the present study in keeping with our previous observations (27) and those of others (45,46). The IL-23R is a type I transmembrane protein that binds with the IL-23 cytokine to activate Janus kinases. This leads to transcription of key pro-inflammatory genes, including IL-17, and interferon-γ from T regulatory cells and when defective impairs T regulatory cell function. It is already known that polymorphisms in the IL23R gene confer susceptibility to several autoimmune diseases, including Crohn's disease, psoriasis, rheumatoid arthritis, ankylosing spondylitis, and multiple sclerosis (47 –50), and it was not unreasonable to expect the AITDs to show a similar risk. Although the IL23R gene was previously reported to be specifically associated with GO (19), this specific association was not seen in the present study. This may have been because this was a well-defined Caucasian group of severe GO patients. Of note, the association has also not been seen in a Japanese population (51). These results, therefore, provide no evidence that the IL23R gene confers an important specific genetic susceptibility to GO. In addition, the IL23R gene has also been shown to not confer susceptibility to several other autoimmune diseases, such as systemic sclerosis, systemic lupus erythematosus, and Sjögren's syndrome (50).
The strongest genetic association for the AITDs has been with the MHC region (8,52). For GD, the risk ratios associated with the HLA-DR3 haplotypes have been larger than the gene risk ratios for all the other known or suspected genes (8,52) and particularly high when analyzed on the basis of the presence of Arg 74 in the DR-binding pocket (8,35). The MHC contains an assortment of immune-regulatory genes, but the HLA-DR and DQ regions have been most consistently associated although Class I genes have also been implicated (8,52,53). Past reports have suggested that HLA-DR3 was more prevalent in patients with GO, while others were unable to confirm this (54 –58). Our results simply showed that HLA-DR3 was highly associated with GD, but there was no significant predilection for the GO patients rather than the non-GO patients, indicating that HLA-DR3 is not a specific GO-associated gene. Our data also suggested that HLA-DR3 does not work in association with CTLA4, IL23R, and TSHR genes in GO.
Our attempts at genetic profiling showed that very few patients failed to show any associated genes, while 10% showed all five of the at-risk polymorphisms. Nevertheless, this was not different when comparing GO with non-GO patients. While it is possible that other minor genes or some modified genes are involved in the development of GO, we found no evidence for this opinion in this study of selected susceptibility genes.
In summary, our study demonstrated that four major reported GD-associated genes (HLA-DR3, CTLA4, IL23R, and TSHR) or gene combinations were not specifically associated with GO. The evidence continues to point to GO being a manifestation of GD exacerbated by stochastic environmental or anatomical influences (42).
Footnotes
Acknowledgments
This work was supported in part by DK052464 and DK69713 from NIH-NIDDK the David Owen Segal Endowment, the James J. Peters VAMC, and the VA Merit Award program. We thank our colleague Dr. Yaron Tomer for his help and advice.
Disclosure Statement
T.F.D. is a Board Member of Kronus, Inc., Star, Idaho (a distributor of thyroid antibody test kits). The other authors have no conflicts of interest to disclose.