
Abstract
Background:
Ectopic intrapulmonary thyroid is extremely rare, with only about two cases reported in the literature. These cases were found either during the work-up of a solitary pulmonary nodule or at autopsy. Here, we report a case of ectopic intrapulmonary thyroid mimicking multiple pulmonary metastases from an endometrioid adenocarcinoma of the uterus.
Patient Findings:
A 50-year-old woman presented with dysmenorrhea and menorrhagia. Endometrial curettage of the uterus revealed an endometrioid adenocarcinoma. During the staging, multiple pulmonary nodules were found. To exclude the possibility of lung metastases of the endometrioid adenocarcinoma from the uterus, video-assisted thoracic surgery (VATS) with wedge resection was performed for the largest nodule. The histopathology for that nodule was entirely consistent with normal thyroid tissue. The patient underwent surgery for uterine cancer and was discharged without further adjuvant chemotherapy. The remaining intrapulmonary nodules were unchanged in size on a serial computed tomography scan.
Summary:
In this patient, pulmonary metastases were initially considered the most likely cause of the multiple pulmonary nodules, but the diagnosis of the ectopic intrapulmonary thyroid was ultimately made based on VATS-wedge resection for the largest pulmonary nodule. The patient was able to avoid any unnecessary systemic chemotherapy.
Conclusions:
Ectopic intrapulmonary thyroid is extremely rare but can be confused with pulmonary metastases from other sites. We are unaware of similar cases in the literature.
Introduction
Patient
A 50-year-old woman was admitted to our hospital due to a one-year history of dysmenorrhea and menorrhagia with no significant previous medical history. She had no pulmonary symptoms, such as coughing, dyspnea, or hemoptysis. A thyroid mass was not palpated during the neck examination. Admission lab results revealed microcytic hypochromic anemia with a plasma hemoglobin level of 7.4 g/dL. Her thyroid function tests indicated that she was euthyroid. The serum thyrotropin was 2.49 mIU/L (0.30–5.00), and the free thyroxine was 0.91 ng/dL (0.89–1.76). A pelvic examination disclosed an enlarged uterus with no palpable adnexal mass. A pelvic ultrasound showed a thickened endometrium. The patient underwent a fractional dilation and curettage. Pathology revealed a well-differentiated endometrioid adenocarcinoma.
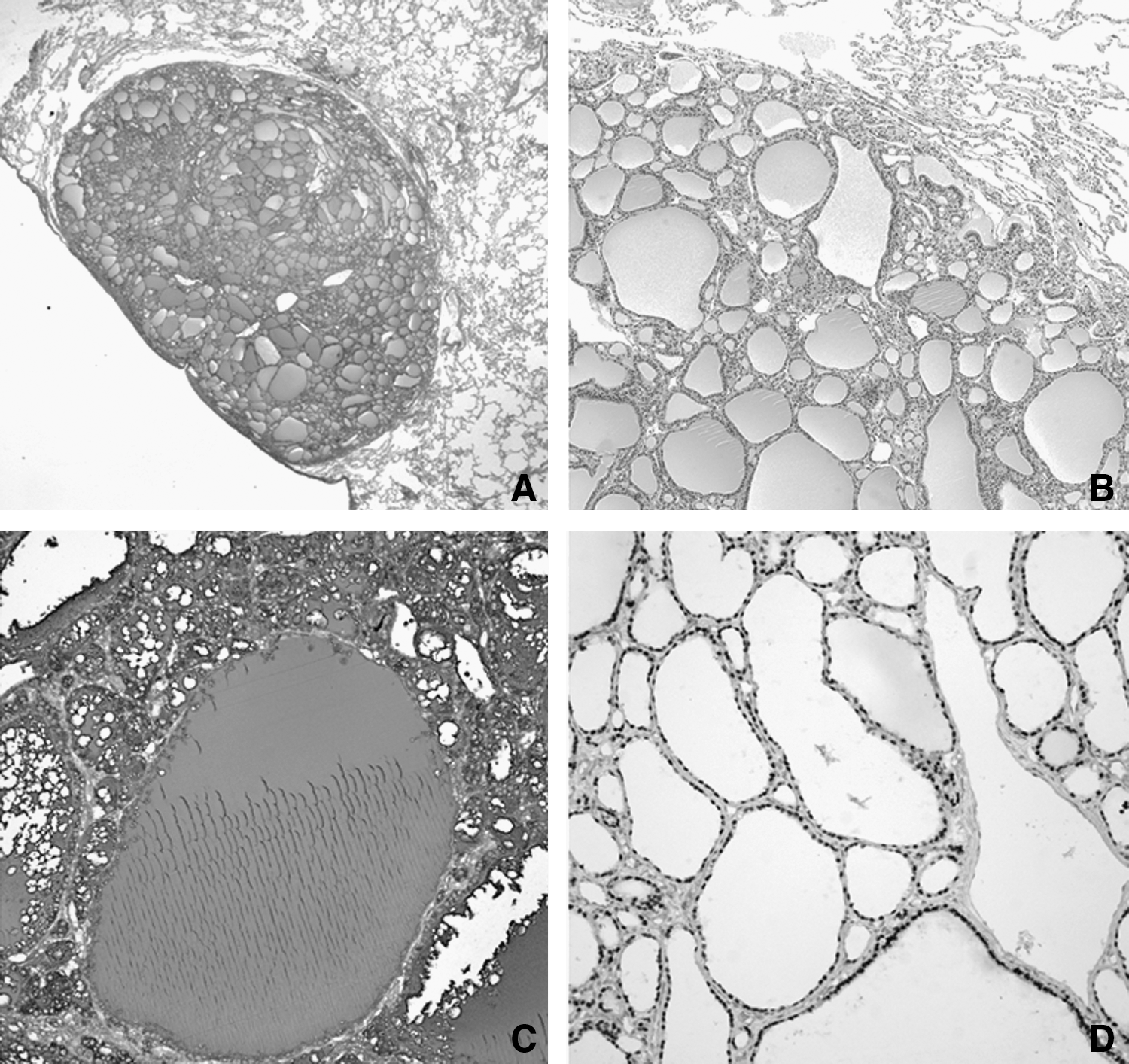
In the abdomen computed tomography (CT) scan, a 7-mm-sized, well-defined, round pulmonary nodule was incidentally found in the anterior basal segment of the right lower lobe. To evaluate the solitary pulmonary nodule, a chest CT scan was performed. Three well-defined, round, tiny nodules, ranging from 3 to 5 mm in size, were found in the anterior segment and in the lingular division of the left upper lobe in addition to the previous 7-mm-sized pulmonary nodule in the anterior basal segment of the right lower lobe (Fig. 1). The nodules showed high attenuation (40 HU [Hounsfield units]) on a nonenhanced chest CT image and strong enhancement (net enhancement, 54 HU) on a contrast-enhanced chest CT image (Fig. 2). To exclude the possibility of lung metastases from the endometrioid adenocarcinoma from the uterus, video-assisted thoracic surgery (VATS) with wedge resection was performed for the largest nodule in the anterior basal segment of the right lower lobe. Gross inspection revealed a well-demarcated, yellowish nodule measuring 0.9 cm×0.8 cm×0.7 cm in the lung parenchyma. On microscopic examination, the nodule had various-sized colloid-filled normal follicles lined with cuboidal to flattened cells (Fig. 3A, B). There was no evidence of malignancy in the microscopic findings. Immunohistochemical staining for both thyroglobulin and thyroid transcription factor-1 (TTF-1) showed strong reactions within the epithelial cells and the colloid within the follicles (Fig. 3C, D). However, staining results for both estrogen receptors and progesterone receptors were negative.

On lung window images of the chest computed tomography (CT) scans

On mediastinal images of nonenhanced
Neck ultrasonography was performed to exclude the possibility of a metastatic tumor from the thyroid. A 6-mm-sized thyroid nodule with macrocalcification was noted in the right thyroid lobe, and ultrasonography-guided fine-needle aspiration cytology and core biopsy were performed to rule out thyroid cancer. The biopsy results were compatible with a benign nodule without suspicious findings for papillary thyroid carcinoma or follicular neoplasm. The BRAF V600E mutation was not identified in the DNA extracted from the thyroid nodule by polymerase chain reaction amplification using a Multiplex BRAF ACE detection system (Seegene, Inc., Seoul, South Korea) (Fig. 4) (5).
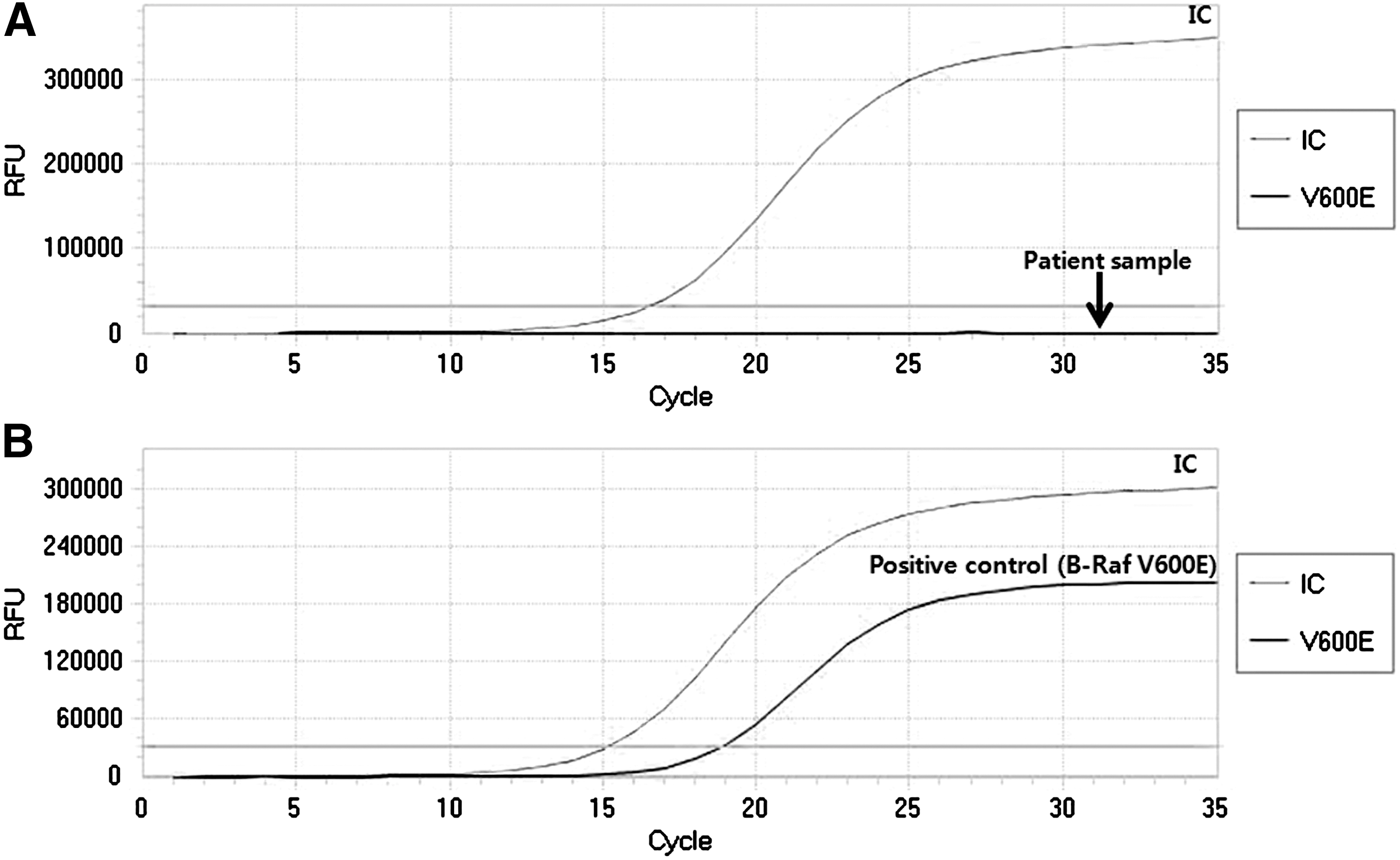
The BRAF mutation analysis by a real-time polymerase chain reaction was performed according to the manufacturer's instructions.
After the exclusion of lung metastases from the endometrioid adenocarcinoma from the uterus, the patient underwent a total abdominal hysterectomy, salpingo-oophorectomy, and pelvic lymph node dissection. A microscopic examination showed a well-differentiated endometrioid adenocarcinoma with an invasion to be less than half of the myometrium. The adnexa were grossly and microscopically normal, and there was no evidence of extra-uterine spread (International Federation of Gynecology and Obstetrics; FIGO stage IA).
The patient was discharged without further adjuvant treatment. A follow-up chest CT scan 6 months after the operation showed no interval changes for the three remaining pulmonary nodules in the left upper lobe and no new pulmonary nodules. The patient has had an uneventful course and is on follow-up without remarkable findings.
Discussion
Since Bando et al. reported the first case of the ectopic intrapulmonary thyroid (3), ectopic thyroid in the lung has been reported in at least one case and that was incidentally found during autopsy (4). Although this is not the first case of an ectopic intrapulmonary thyroid, there is a distinct difference, as well as clinical significance, in terms of medical history compared with the other two cases that were incidentally found without any notable medical history.
In the present case, the patient was diagnosed with endometrioid adenocarcinoma of the uterus and had multiple pulmonary nodules that were simultaneously found at the time of diagnosis. In the context of clinical practice, there was a high probability for pulmonary metastases. Whether the tumors were metastatic or not was a critical issue, because the treatment strategy and tumor staging are altered according to the histopathologic results from the pulmonary nodules. Contrary to our expectations, VATS with wedge resection for the largest pulmonary nodule of the right lower lobe surprisingly revealed normal thyroid tissue. Ancillary studies demonstrating the presence of thyroglobulin and TTF-1 further supported the thyroid tissue. Therefore, the tumor staging of the patient was FIGO stage IA, and adjuvant chemotherapy was not necessary.
After histologic confirmation of normal thyroid tissue, the exclusion of metastatic tumors from either a eutopic or an ectopic thyroid was needed to confirm the ectopic intrapulmonary thyroid. Although the patient had a small thyroid nodule in the right lobe, the nodule was diagnosed as a benign thyroid lesion on cytologic and histologic examinations. In addition, we could not find any evidence of metastatic tumors from the ectopic thyroid tissue, which can exist in the cervical midline structures (6) and various organs (7,8). In the present case, it was necessary to exclude the possibility of pulmonary metastasis from struma ovarii, because malignant struma ovarii is also able to display the pulmonary metastasis in women (9,10). However, there was no architectural or cytological evidence of malignant change in the ectopic intrapulmonary thyroid. Furthermore, the postoperative bilateral adnexal pathology did not show ovarian enlargement or any thyroid tissue with malignant changes in the ovarian parenchyma. Therefore, malignant struma ovarii could be excluded in this case.
In the case presented here, tissue biopsies for the three tiny nodules remaining in the left upper lobe could not be performed, because those nodules were very small, and the patient did not agree to a further evaluation of those nodules through the VATS with biopsy. However, the three tiny nodules showed the same CT findings as the biopsy-proven largest nodule in the right lower lobe; meaning that they had a higher density than the surrounding soft tissues due to their high concentration of iodine (11,12). In addition, the sizes of those nodules did not increase during the 6-month follow-up period. Taken together, we can consider that all the pulmonary nodules were ectopic intrapulmonary thyroid tissues.
In conclusion, we report an extremely unusual case of the ectopic intrapulmonary thyroid mimicking multiple pulmonary metastases from the endometrioid adenocarcinoma of the uterus.
Footnotes
Disclosure Statement
The authors have no financial conflicts of interest to be disclosed.