
Abstract
Background:
Metastases of thyroid carcinomas to the choroid and/or orbit are infrequent. PubMed was searched for English-language articles and case reports published from 1977 to 2012. In our survey, we looked for reports of orbital and/or ocular metastases from the thyroid and found 31 reported cases from 1979 to 2012
Summary:
At the time of onset of ocular symptoms, the vast majority of patients had a long history of thyroid malignancy and evidence of widely disseminated metastatic disease. The age of the reported patients ranged from 29 to 83 years. Among the 22 reported cases of thyroid carcinomas with metastases to the choroid from 1979 to 2012, the most common primary tumor was papillary thyroid carcinoma (PTC); this occurred in seven patients. This was followed by medullary thyroid carcinoma in six cases and follicular thyroid carcinoma (FTC) in five cases. Orbital metastases were reported in nine patients with thyroid carcinomas (PTC=4, FTC=3, Hürthle cell=1, not specified=1). Patients with choroidal metastases presented with decreased or blurred vision, eye pain, and flashes in 81%, 5%, and 5% of cases, respectively. The diagnosis of a choroidal tumor was usually based on noninvasive diagnostic techniques such as ultrasonography, transillumination, computer tomography (CT), and/or magnetic resonance imaging (MRI) scanning. 131I scanning revealed uptake in the orbit in 26% of cases with choroidal and/or orbital PTC or FTC. For a metastasis that causes a definitive loss of vision and/or persistent pain, the treatment of choice was enucleation. The other treatment options were brachyradiotherapy using 125I episcleral radioactive plaque insertion, external beam radiation, 131I therapy, chemotherapy, and/or targeted therapy with small molecules.
Conclusions:
The orbit and globe are not common sites for metastatic thyroid carcinomas. Diagnosis of a choroidal tumor is usually based on clinical judgment and results of noninvasive diagnostic techniques such as ultrasonography, transillumination, CT, and/or MRI scanning. Fundoscopic examination and ocular ultrasonography by an ophthalmologist are recommended for identification and monitoring of choroidal metastatic deposits.
Introduction
Method of Literature Search
PubMed was searched for English-language articles and case reports published from 1977 to 2012. The search was conducted using various combinations of the following keywords: thyroid carcinoma, papillary thyroid carcinoma (PTC), anaplastic thyroid carcinoma (ATC), insular thyroid carcinoma, medullary thyroid carcinoma (MTC), follicular thyroid carcinoma (FTC), HCTC, uveal metastasis, choroid, choroid metastasis, orbital metastases, iris metastasis, and ocular metastasis. In our survey, we looked for reports of orbital and/or ocular metastases from the thyroid and found 31 reported cases from 1979 to 2012.
Results
Epidemiology of choroidal and orbital metastases from all types of cancer
Metastases to the orbit and/or eye from all types of cancer are infrequent (1 –6). As noted by Bernstein-Lipschitz et al. (7), “Metastases of cancer to the orbit and choroid are often found in terminally ill patients with widespread disease. Since in many cases there are no visual symptoms and an autopsy is not performed, the exact incidence of choroidal and orbital metastases in cancer patients is hard to determine.” In a series of 1264 consecutive patients referred for a suspected orbital mass over a 30-year period, Shields et al. (5) found only 91 (7%) metastatic tumors. Char et al. (6) noted just 36 such lesions among 612 (6%) patients with an orbital mass. Among solid tumor malignancies, the ones most commonly found to metastasize to the eye and/or orbit were from the breast and lung, followed by prostatic carcinomas (4). In a series of 950 uveal metastases that were diagnosed in 520 eyes of 420 consecutive patients over a 20-year period among solid tumor malignancies, the ones from the breast (47%) and lung (21%) were most common to metastasize to the eyes (3).
Epidemiology of choroidal metastases from thyroid cancer
In a series of 950 uveal metastases that were diagnosed in 520 eyes of 420 consecutive patients among solid tumor malignancies, only 0.5% of metastases were derived from thyroid carcinomas (3). Similarly, in a series of 227 cases of carcinomas metastatic to the eye or orbit, Font and Ferry (1) reported only one case that had its origin from the thyroid gland. In a review of the English literature, Arat and Boniuk (8) found reports of 12 clinically well-documented cases of choroidal metastases and 2 cases of iris metastases from thyroid carcinomas.
We found that among 22 reported cases of thyroid carcinomas with metastases to the choroid from 1979 to 2012, the most common primary tumor was PTC, occurring in seven patients. This was followed by MTC in six cases and FTC in five cases. Only one case report of choroid metastasis was published describing a patient with HCTC, clear cell carcinoma, insular carcinoma, or squamous thyroid carcinoma. The age of the patients with choroidal metastases reported in Table 1 (4,8 –28) ranged from 29 to 83 years; the median age was 56 years. The median age of the patients with choroidal metastases of PTC, MTC, and FTC was 55, 42.5, and 74 years, respectively.
Age at initial presentation to the ophthalmologist.
Time to eye symptoms from initial diagnosis.
FTC, follicular thyroid carcinoma; HCTC, Hürthle cell carcinoma; MTC, medullary thyroid carcinoma; MEN 2B, multiple endocrine neoplasia type 2B; LN, lymph nodes; PTC, papillary thyroid carcinoma; TC, thyroid carcinoma; W, woman; M, man; RTX, external-beam radiation; init., initial presentation; NA, data not available.
Most of the patients with choroidal metastases from our review (Table 1) had a known history of thyroid carcinomas that occurred between 0.2 and 36 years (mean 10.4; median 4.5 years) after the thyroid carcinoma diagnosis. The vast majority of patients with choroidal metastases from our review had evidence of widely disseminated metastatic disease (4,9 –20). However, the initial presentation of choroid metastasis originating from a thyroid carcinoma was reported in four cases (8,14,19,20), and one of them had only an occult thyroid carcinoma with a diameter of 2 mm (14). Bilateral choroidal involvement was reported in six cases (27%): three cases of MTC, two cases of PTC, and one case of FTC.
Epidemiology of orbital metastases from thyroid cancer
In the review by Slamovits et al. (4) from 1979, thyroid metastases to the eye or orbit were reported in 16 cases, 11 of which were orbital metastases. However, in our review, we found 22 cases (4,8 –28) of well-documented thyroid eye metastases and only 9 cases of orbital metastases (PTC=4, FTC=3, HCTC=1, not specified=1). Orbital metastases (Table 2) affected bone (2,7,29 –32), muscle (33 –35), and lacrimal gland (7) in six cases, three cases, and one case, respectively.
Age at initial presentation to the ophthalmologist.
Time to eye symptoms from initial diagnosis.
NS, not specified (follicular cell origin); FV, follicular variant.
The age of the patients with orbital metastases ranged from 16 to 75 years; the median age was 59 years. The patients with orbital metastases of PTC or FTC had median ages of 62.5 and 56 years, respectively.
An orbital metastasis was the initial presentation of thyroid carcinomas in seven of nine cases (78%). None of the patients with orbital metastases had MTC. This probably reflects a lower incidence and propensity of MTC to cause bone metastases compared to differentiated carcinomas of the follicular epithelium.
Symptoms and signs of choroidal metastases
As noted by Shield et al. (3), decreased vision is the common symptom if a choroidal metastasis involves the optic nerve or macula
Symptoms and signs of orbital metastases
The metastatic involvement of the orbit originating from any malignancy is a common cause of unilateral proptosis (5). Unilateral proptosis can be of neoplastic origin, even if thyroid function tests suggest hyperthyroidism, and it necessitates investigation with a computer tomography (CT) scan of the orbit (33). Char et al. (6) reported on 31 patients treated because of orbital metastases of various origins. Their patients presented with diplopia (48%), proptosis (26%), pain (19%), decreased vision (16%), and ptosis (10%). Patients with orbital metastases from our report (Table 2) presented with diplopia (44%), proptosis (56%), pain (22%), decreased vision (22%), and ptosis (11%). Only one of our patients was asymptomatic.
Diagnostics of choroidal and orbital metastases from cancers
After abrupt changes in visual acuity, a fundoscopic examination and ocular ultrasonography by an ophthalmologist are recommended for the identification and monitoring of choroidal metastatic deposits (9). Diagnosis of a choroidal tumor is usually based on clinical judgment and results of noninvasive diagnostic techniques such as ultrasonography, transillumination, CT, and/or MRI scanning (11).
Shields et al. (3), in a survey of 520 eyes with uveal metastases from various solid tumor malignancies, reported that the posterior choroid accounted for most metastatic foci (88%), while metastatic foci were detected also in the iris (9%) and ciliary body (2%). Furthermore, choroidal metastases assumed a yellow color in 94% of cases when viewed through the ophthalmoscope (3). However, choroidal metastases in PTCs, FTCs, or HCTCs were red, yellow, or orange color in only 40% of cases based on our review (Table 1). Furthermore, choroidal metastases in FTCs assumed a yellow color in only one of four cases. On the other hand, metastases were yellow in all three cases with MTCs in whom the color was described.
Diagnostics of choroidal and orbital metastases of thyroid cancer
Choroidal metastases are diagnosed mostly based on clinical examinations and ultrasonography (11). When the initial presentation of a malignancy is a choroidal or orbital metastasis, a fine-needle aspiration biopsy (FNAB) may be performed to find out the origin of the primary tumor (11). It is the most useful diagnostic tool (6), because it is safe and reliable. Instead of an FNAB, a biopsy using a 25-gauge vitrector may be carried out in selected cases, performing a transretinal choroidal biopsy to confirm the diagnosis (16). Using a 25-gauge vitrector is regarded as a safe procedure (16).
The diagnosis of orbital metastases also can be established by an open biopsy. Usually, an open biopsy was performed if the correct diagnosis was not determined when a focal mass was present, or if a metastasis had to be therapeutically debulked regardless of the histology (6). An open biopsy was performed in six of the nine patients in the reviewed literature; only one patient had a core biopsy, and none had an FNAB.
Positive immunochemical staining for the presence of thyroglobulin in metastatic cells is the most conclusive diagnostic evidence that the origin of a metastasis is the thyroid (7). Follicular thyroid cells are the only ones that have the ability to produce thyroglobulin, and most differentiated tumors of follicular cell origin retain this ability (36). In addition, the accumulation of 131I shown by scintigraphy is specific for metastases of differentiated thyroid carcinomas. The uptake of 131I in the choroidal metastasis of PTCs, FTCs, or HCTCs (Table 1) was reported in 3 of 14 patients (21%). On the other hand, uptake of 131I in orbital metastases was reported in three of nine (33%) patients with PTCs, FTCs, or HCTCs (Table 2).
Treatment of choroidal metastases from thyroid cancer
Enucleation is the treatment of choice for metastases of thyroid carcinomas to the eye that cause a definitive loss of vision and/or persistent pain (14,20,21,23). The other treatment options are 131I therapy (8,9,11,13,23), external beam radiation (4,12,15 –17,19,22 –24,27), brachyradiotherapy using 125I episcleral radioactive plaque insertion (10,11), chemotherapy (16,23,24), and targeted therapy with monoclonal antibodies (16) and/or small molecules (23).
Treatment with 131I
The treatment of choroidal metastases with 131I was reported in 5 of 13 patients with PTC, FTC, or HCTC (8,9,11,13,23). The 131I treatment had no effect on only one of them (23). Anteby et al. (13) found that choroidal metastasis from PTC responded to 131I treatment. The choroidal metastasis height decreased from 2.7 to<1 mm four months after the 131I treatment (13). Furthermore, therapy with 131I may be followed by a decrease in the size of the lesions as well as improvement of vision (9). Arat and Boniuk (8) observed a complete resolution of an iris metastasis and a regression of one of the choroidal metastases from PTCs after 131I therapy. Unfortunately, only Arat and Boniuk (8) reported the duration of effect of the 131I treatment; this was longer than 18 months. Because thyroxine withdrawal causes prolonged thyrotropin (TSH) stimulation, it may lead to accelerated progression of metastatic lesions, with important clinical consequences, especially for patients with brain and choroidal metastases (9). Therefore, administering 131I therapy after recombinant human TSH (rhTSH) stimulation should be considered to minimize tumor progression and clinical sequelae (9).
External beam radiation
In the case of nonradioactive iodine–avid tumors, ocular external beam radiation remains a therapeutic option (24). External beam radiation is a good treatment option because it is noninvasive and can produce a long-lasting effect. Ocular external beam radiation was effective in six of the ten patients with choroid metastases (4,12,15 –17,19,22 –24,27). Beneficial effects of radiation lasted from 5 to 16 months. However, total retinal detachment occurred in two cases, and the progression of choroidal metastases was reported in three other cases (one immediate, one after 5 months, and one after 16 months).
125I episcleral radioactive plaque insertion
Another effective approach is brachyradiotherapy using 125I episcleral radioactive plaque insertion (10,11). Ritland et al. (11) reported that tumor thickness decreased from 11 to 6.4 mm 3 months after the 125I plaque insertion therapy. Duton et al. (10) reported that the effect lasted 24 months.
Tran et al. used chemotherapy as a palliative procedure (23). Advances in the understanding of molecular biology in metastases originating from DTC enabled recent favorable results with small-molecule therapy in patients with metastatic thyroid carcinoma (37 –39). Tran et al. (23) used sorafenib, while Scott et al. (16) used bevacuzimab in their patients.
Treatment of orbital metastases of thyroid cancer
As noted by Char et al. (6), in a patient with orbital metastases and suddenly decreased vision due to a mass compressing the optic nerve, surgical debulking of the tumor is the optimal treatment, and vision may be restored in such cases. Surgical debulking was performed in two cases in the reviewed literature (9,34), while orbital exenteration was performed in one case (35).
Bougattas et al. (31) reported uptake of 131I in orbital metastases on postablative 131I imaging. Three patients were treated with 131I; in two of them, a good response was observed in the orbital metastasis (2,29).
External beam radiation is another treatment used in patients with a solitary orbital metastasis that was diffuse or that involved an important structure, such as the muscle, globe, or nerve (6). It was performed in three patients (30,32,34), but it was reported to be effective in only one of these cases (32). As emphasized by Char et al., it is imperative to obtain a brain MRI scan before irradiating a metastatic orbital tumor, because often patients have silent brain lesions when they present with an orbital disease (6). Failure to obtain these imaging studies can result in patients having the same anatomical area re-irradiated with resultant increased morbidities (6).
Illustrative Case: Metastatic HCTC to the Choroid Detected by Post-Therapeutic 131I Scintigraphy
In July 2010, a 69-year-old woman was referred to the Institute of Oncology Ljubljana for further diagnosis and treatment because of a CT-proven 5th lumbar vertebral metastasis of unknown origin. FNA cytology of the left thyroid nodule was suspicious for PTC. The serum thyroglobulin level and the anti-thyroglobulin antibody concentration were elevated to >5000 μg/L (reference <80 μg/L) and 165 kU/L (reference <30 kU/L), respectively.
In August 2010, she underwent a total thyroidectomy, with exploration of the cervical lymph nodes. Histopathology revealed moderately differentiated HCTC. The dominant lesion in the left lobe measured 6.3 cm×4 cm and was widely invasive. Furthermore, focal vascular invasion was present. According to the TNM classification, the tumor was staged as pT3N1M1.
After thyroid surgery, the patient received suppressive doses of
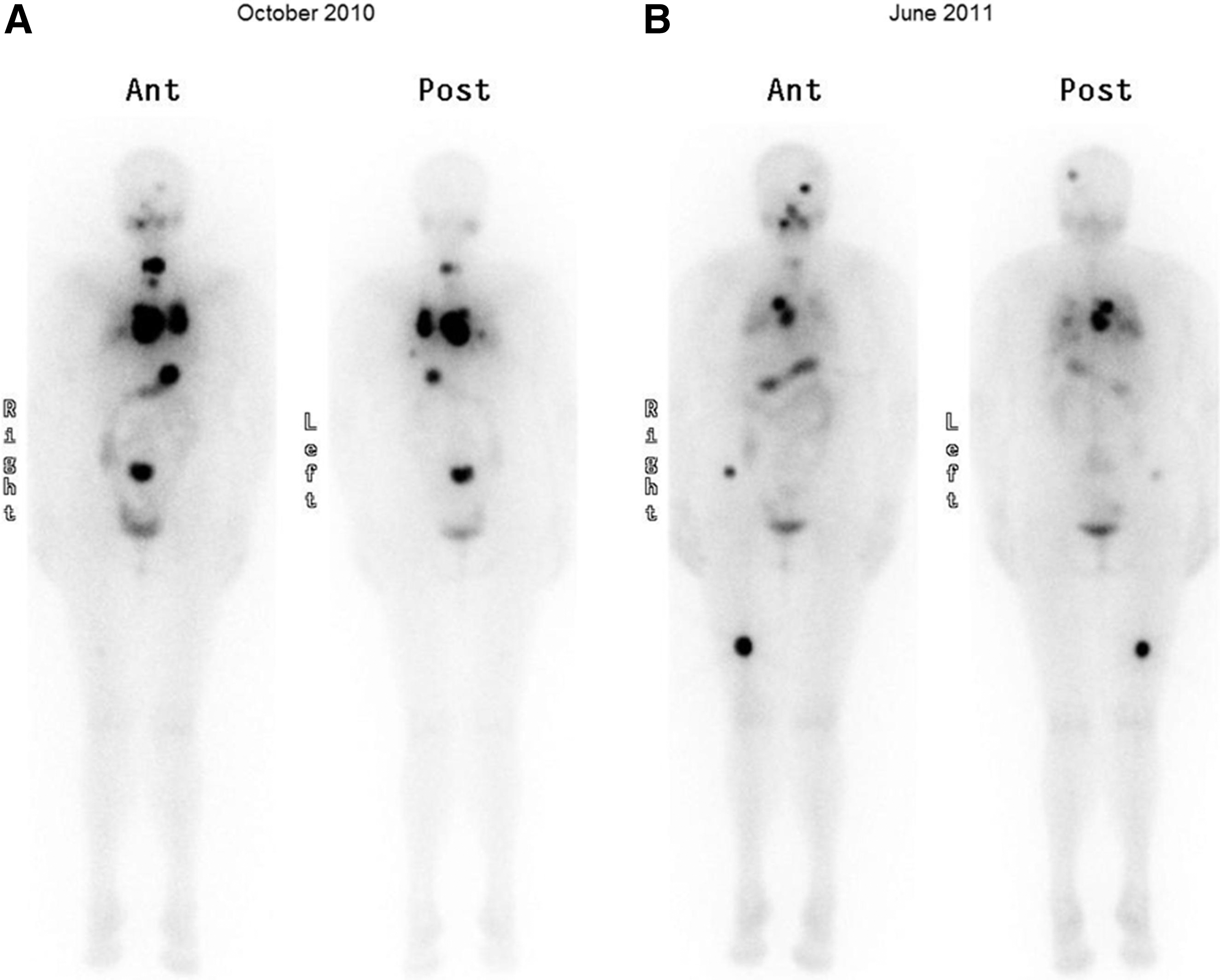
Comparison of whole-body scintigraphies obtained in October 2010
In February 2011, the patient noted impaired vision in her left eye. During the next month, half of her left visual field became progressively blurred. An ocular examination was unremarkable apart from an early stage of nuclear and cortical cataract formation in both eyes. Fundoscopy of the left eye revealed an exudative retinal detachment in the upper nasal quadrant with a solid lower detachment, which covered part of the papilla. A developing macular detachment was also present. Ophthalmoscopy of the right eye was normal. The fluorescein angiogram showed hyperfluorescence in the upper part of the left retina above the papilla. The echography of the left eye revealed an irregular solid choroidal lesion, measuring ∼6.5 mm in diameter, with some circular hypoechogenic regions, causing exudative retinal detachment above the papilla. The echographic image was typical of an ocular metastasis. The MRI scan of the head confirmed a mass in the choroid of the left eye (Fig. 2). Since 131I accumulated in this lesion, it was diagnosed as a thyroid carcinoma metastasis to the eye. However, 131I treatment of the choroid metastasis was not an option, as the uptake of 131I in the choroid metastasis was minimal, while multiple 131I-avid metastases were present elsewhere. Therefore, external-beam radiation with a total dose of 40 Gy was performed, as it was considered to be noninvasive and could produce a long-lasting effect. This was followed by administration of a therapeutic dose of 7.55 GBq of 131I after rhTSH application. Only a trace of 131I accumulated within the ocular metastasis. The control eye echography performed in July 2011 showed a partial regression of the metastatic choroidal lesion (measuring 5 mm in thickness). The last ophthalmologic examination in June 2012 revealed no increase in metastasis. However, a complete loss of vision in the left eye, because of total exudative detachment of the retina, was present.
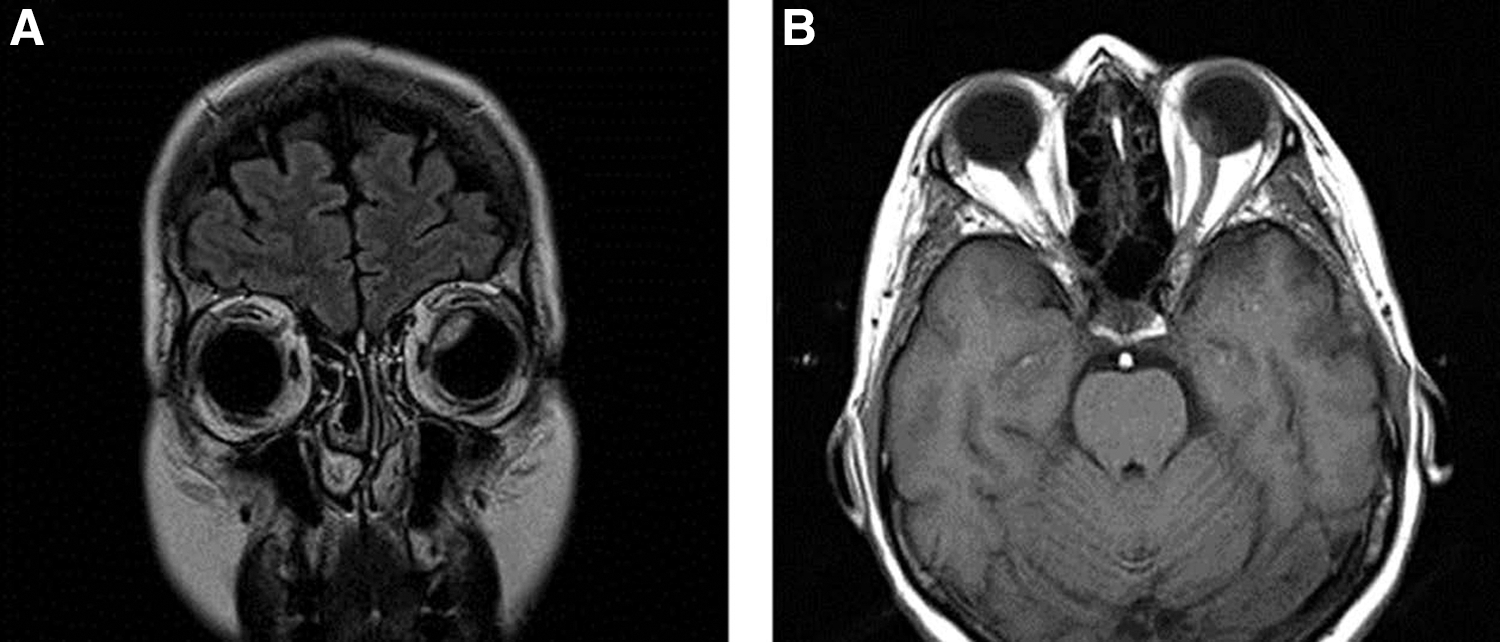
Magnetic resonance-imaging (T1) coronal
Unfortunately, despite good uptake of the administered 131I, new metastatic lesions in the right femur and cranium were detected by a post-therapeutic 131I scintigraphy (Fig. 1B). Another MRI scan of the head was performed in August 2011, which excluded brain metastases and showed a new metastatic lesion in the cranium. An MRI scan performed in June 2012 provided evidence that the lesion had begun to grow, and therefore it was treated with external radiation. In September 2012, a rapid progression of multiple metastatic lesions systemic was detected; therefore chemotherapy was initiated in accordance with our institutional guidelines.
Conclusion
In conclusion, the orbit and globe are not common sites for metastatic thyroid carcinomas. The diagnosis of a choroidal and orbital metastasis from thyroid carcinoma is usually based on clinical judgment and results of ultrasonography, transillumination, CT, and/or MRI scanning. Effective treatment options for a metastasis of thyroid carcinomas to the eye include external-beam radiation, 131I therapy, and brachyradiotherapy using a 125I episcleral radioactive plaque insertion. Enucleation is the treatment of choice for the minority of patients with a metastasis that causes a definitive loss of vision and/or persistent pain.
Footnotes
Disclosure Statement
The authors declare that there are no commercial associations that might create a conflict of interest in connection with this article.