
Abstract
Background:
Radioiodine ablation after total thyroidectomy is the generally accepted treatment for patients with widely invasive follicular thyroid carcinoma (FTC). The therapeutic strategy for minimally invasive FTC, on the other hand, is still a matter of controversy. The histological diagnosis of minimally invasive FTC is often made after lobectomy. The aim of this study was to determine the factors associated with the development of distant metastases in patients with minimally invasive FTC.
Methods:
Between 1989 and 2006, 251 patients with minimally invasive FTC underwent initial surgery at our hospital. Their median follow-up period was 7.2 years. There were 194 women and 57 men. Their mean age at the time of surgery was 46 years. Distant metastases were diagnosed in 54 patients (21.5%). In 22 of them distant metastases were diagnosed at the time of the initial surgery (M1), and in the other 32 they were diagnosed during the follow-up period. Age at initial surgery, sex, primary tumor size, histological findings (differentiation, and extent of vascular and capsular invasion), completion total thyroidectomy, and distant metastases at initial surgery were assessed as prognostic factors for distant-metastases-free survival (DMFS) and cause-specific survival (CSS). The Kaplan–Meier method and log-rank test were used to analyze time-dependent variables. The Cox proportional hazard model was used to perform the multivariate analysis.
Results:
Univariate analysis showed that age (45 years or older) and primary tumor size (4 cm or more) were significant prognostic factors related to postoperative distant metastases in the group of 229 patients without distant metastases at time of the initial surgery. The cumulative survival rate was significantly poorer in M1 patients, patients aged 45 years or older, and patients whose primary tumor size was 4 cm or more. Multivariate analysis showed that age was a significant prognostic factor both for DMFS and CSS.
Conclusions:
Age was the most powerful prognostic factor for patients with minimally invasive follicular thyroid cancer. The prognoses of patients younger than 45 years old were excellent and distant metastases rarely occurred. Routine completion total thyroidectomy and radioiodine ablation is thought unnecessary for these patients.
Introduction
Methods
Patients
Between 1989 and 2006, 9333 patients with thyroid carcinoma underwent initial surgical treatment at our institution, and 399 (4.3%) of them had been diagnosed with FTC. After excluding the 17 patients with concomitant PTC, the 60 patients with oxyphilic cell carcinoma, and the 5 patients with clear cell carcinoma, there were 317 patients with ordinary FTC. The 251 of them with minimally invasive FTC were the subjects of this study. The surgical specimens were all reexamined histologically by one of co-authors (K.K.) and the diagnoses were reconfirmed. The pathological diagnosis and classification of follicular carcinoma were based on the most recent WHO classification system (13). The presence of capsular and/or vascular invasion and the absence of nuclear features of papillary thyroid carcinoma defined the pathological diagnosis of FTC. Follicular variant of papillary thyroid carcinoma was strictly excluded on the basis of nuclear features of papillary thyroid carcinoma. Based on the extent of invasiveness of the tumor, follicular carcinomas were classified as widely invasive FTC or minimally invasive FTC. Widely invasive FTC showed widespread infiltration into blood vessels and/or adjacent thyroid tissue and often lacked complete encapsulation, whereas minimally invasive FTCs were completely encapsulated tumors that infiltrated the vessels located within or immediately outside the capsule and/or penetrated the full thickness of the capsule. One patient had been diagnosed with follicular adenoma postoperatively, but distant metastases were discovered 3 years after surgery, and another patient had neither vascular nor capsular invasion, but cervical lymph node metastases were diagnosed histologically. The final diagnosis in both of these patients was minimally invasive FTC.
The 251 subjects of this study consisted of 194 women and 57 men. Their median age was 46 years (range: 10–83 years old). The median follow-up period was 90 months. The median size of the primary tumor was 44 mm (range: 5–150 mm). The demographic data are summarized in Table 1. The standard initial surgical procedure used to treat patients with a follicular tumor in our institution has essentially been lobectomy. If a patient had a concomitant benign thyroid disease, that is, Graves' disease or a nodular goiter of the opposite lobe, or had distant metastases, total or subtotal thyroidectomy was performed.
p-Values were measured using Fisher's exact test unless otherwise indicated.
Excludes patients with distant metastases at presentation.
χ2 test.
Patients with neck dissection only.
M1, distant metastases at presentation; M2, distant metastases detected during the postoperative follow-up periods; LN, lymph node; ns, not significant.
All patients were followed up in the outpatient clinic of our hospital. A postoperative follow-up examination was usually performed at 1, 3, 6, and 12 months, and every 6 months thereafter. The serum Tg level was routinely measured at every hospital visit, and a chest computed tomography (CT) scan was routinely performed once a year for at least 5 years after initial surgery. Whenever a gradual increase in postoperative Tg level was observed, a chest CT scan and bone scintigraphy were performed. If these examinations resulted in the detection of metastases in patients who had undergone hemithyroidectomy alone at the initial surgery, completion total thyroidectomy was performed and followed by 131I scintigraphy and/or 18F-fluorodeoxyglucose positron-emission tomography/CT. Completion total thyroidectomy and RAI therapy were performed in all M0 patients in whom a recurrence was detected. All M1 patients underwent total thyroidectomy as the initial surgical procedure and subsequent RAI therapy. Usually patients were followed up without TSH suppression therapy and if hypothyroidism was observed after thyroidectomy, L-thyroxine was replaced. All patients with distant metastases were received TSH suppression therapy with L-thyroxine.
The data were analyzed with a statistical software program (JMP 8.0; SAS Institute, Inc., Cary, NC). Cumulative cause-specific survival (CSS) and cumulative distant-metastases-free survival (DMFS) were analyzed. A univariate analysis was conducted in relation to CSS and DMFS by the Kaplan-Meier method for the following variables: age at surgery (<45 vs. ≥45 years), sex, tumor size (<4 vs. ≥4 cm), histological type (minimally invasive vs. widely invasive), degree of capsular invasion, degree of vascular invasion, and initial distant metastases (M0 vs. M1, analyzed in relation to CSS only). Differences between groups were analyzed for significance by the log-rank test. Multivariate analysis was performed by using the Cox proportional hazard model. The significant factor was showed with the hazard ratio of each category, and p-values <0.05 were regarded as statistically significant.
The study was reviewed and approved by the Institution's Ethics Board and performed in accordance with the Declaration of Helsinki.
Results
The initial operation performed on the subjects of this study was lobectomy in 191 patients, subtotal thyroidectomy in 24 patients, and total thyroidectomy in 36 patients. Thirty nine patients underwent lymph node dissection because lymph node metastases were suspected on the basis of a preoperative ultrasound examination and lymph node metastases were confirmed histologically in 8 (20.5%) of them. Completion total thyroidectomy was performed in 46 patients. In 33 of them it was performed prophylactically and in the other 13 it was performed when recurrent disease was obvious. No patient had intrathyroidal metastases or spread of FTC histopathologically. Curative surgery was performed in all patients except those who were distant-metastases-positive preoperatively (M1), and no macroscopic residual tumor was observed in any of the patients who were distant-metastases-negative preoperatively (M0). Most M0 patients underwent less than total thyroidectomy, and RAI ablation or RAI scintigraphy was not performed in these M0 patients. Since 2000, we have performed RAI ablation after completion total thyroidectomy, mainly in elderly patients with minimally invasive FTC. RAI ablation was performed in 27 patients. In 24 of them it was performed prophylactically and in the other 3 patients it was performed after the distant metastases were detected.
As of a median follow-up time of 90 months, 54 patients (21.5%) had been diagnosed with distant metastases. In 22 (8.8%) of them distant metastases were present at the time of the initial surgery, and in the other 32 (12.7%) distant metastases were detected during the follow-up period (M2). Patients diagnosed with distant metastases less than 1 year after the initial surgery were classified as M1 patients, and patients diagnosed with distant metastases 1 year or more after the initial surgery were classified as M2 patients. The initial distant metastases in the M2 patients were detected at a median interval of 66 months after initial surgery, and the intervals ranged from 24 to 189 months. The sites of the distant metastases were bone alone (n=21), lung alone (n=20), both bone and lung (n=12), and lung, bone, and brain (n=1). Lung and/or bone were the most frequent sites of metastases. RAI therapy after completion total thyroidectomy was performed whenever distant metastases were detected during the follow-up period in patients who had undergone less than total thyroidectomy at their initial surgery. In 54 patients with distant metastases, post-therapeutic scintigraphy showed that 31 patients had radioiodine uptake in their metastases. However, after several courses of radioiodine treatment, complete response was observed in one patient and partial response was observed in two patients. The other patients had stable or progressive disease. Patients with bone metastases were usually sent for orthopedic surgery. Spinal metastatic disease and spinal cord compression were major causes of morbidity and mortality. Treatment of metastatic disease of the spine required surgical decompression, reconstruction, and stabilization in addition to external radiation. Patients with brain metastases were treated with gamma knife surgery and growth control was achieved.
A total of 14 patients (5 M1 patients and 9 M2 patients) died of their disease, and all 14 had distant metastases. All 14 of them had lung metastases, 5 had bone metastases, 3 had lung and bone metastases, 1 had brain metastases, and 1 had lung, bone, and brain metastases. Four patients were transferred to other hospitals near their home for follow-up, and the hospitals were asked for a report of their outcome.
There were significantly more patients with preoperative distant metastases in the group of patients who were 45 years or older and in the group of patients who were positive for capsular invasion (Table 1). After excluding the M1 patients, postoperative distant metastases were significantly more common in the group of patients who were 45 years or older and in the group whose primary tumor size was 4 cm or more (Table 1).
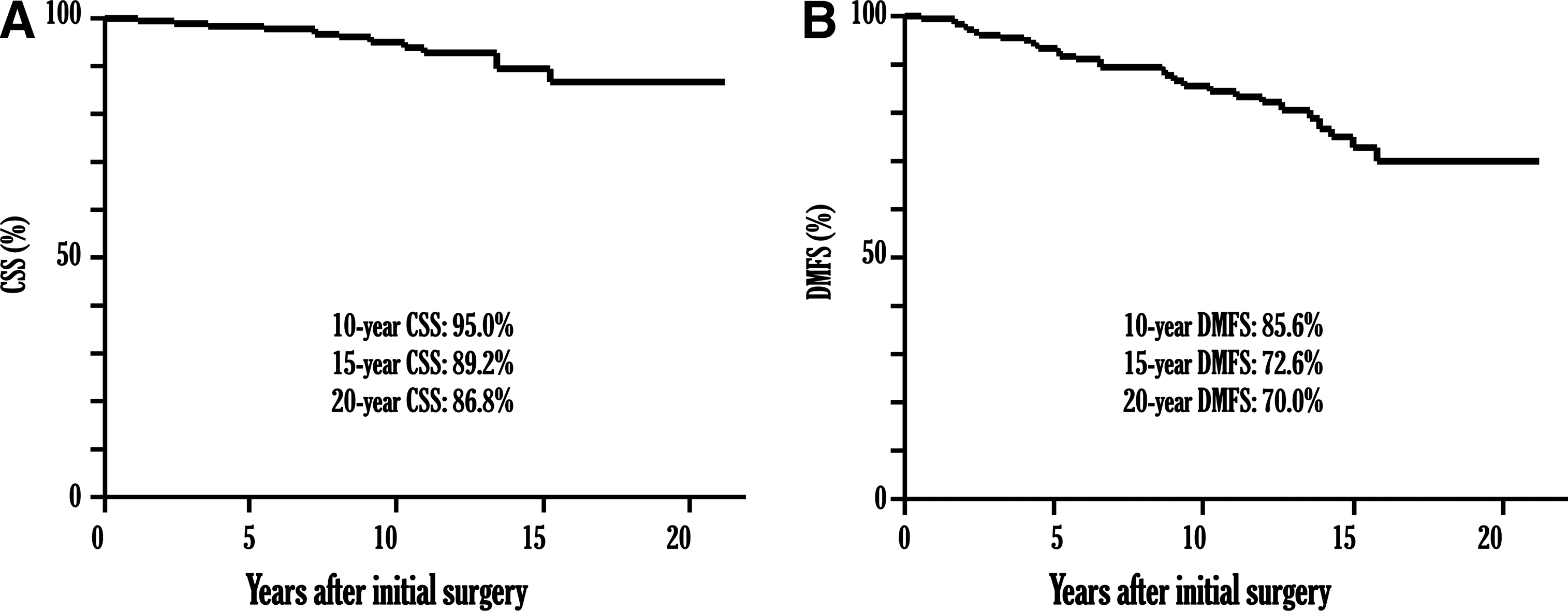
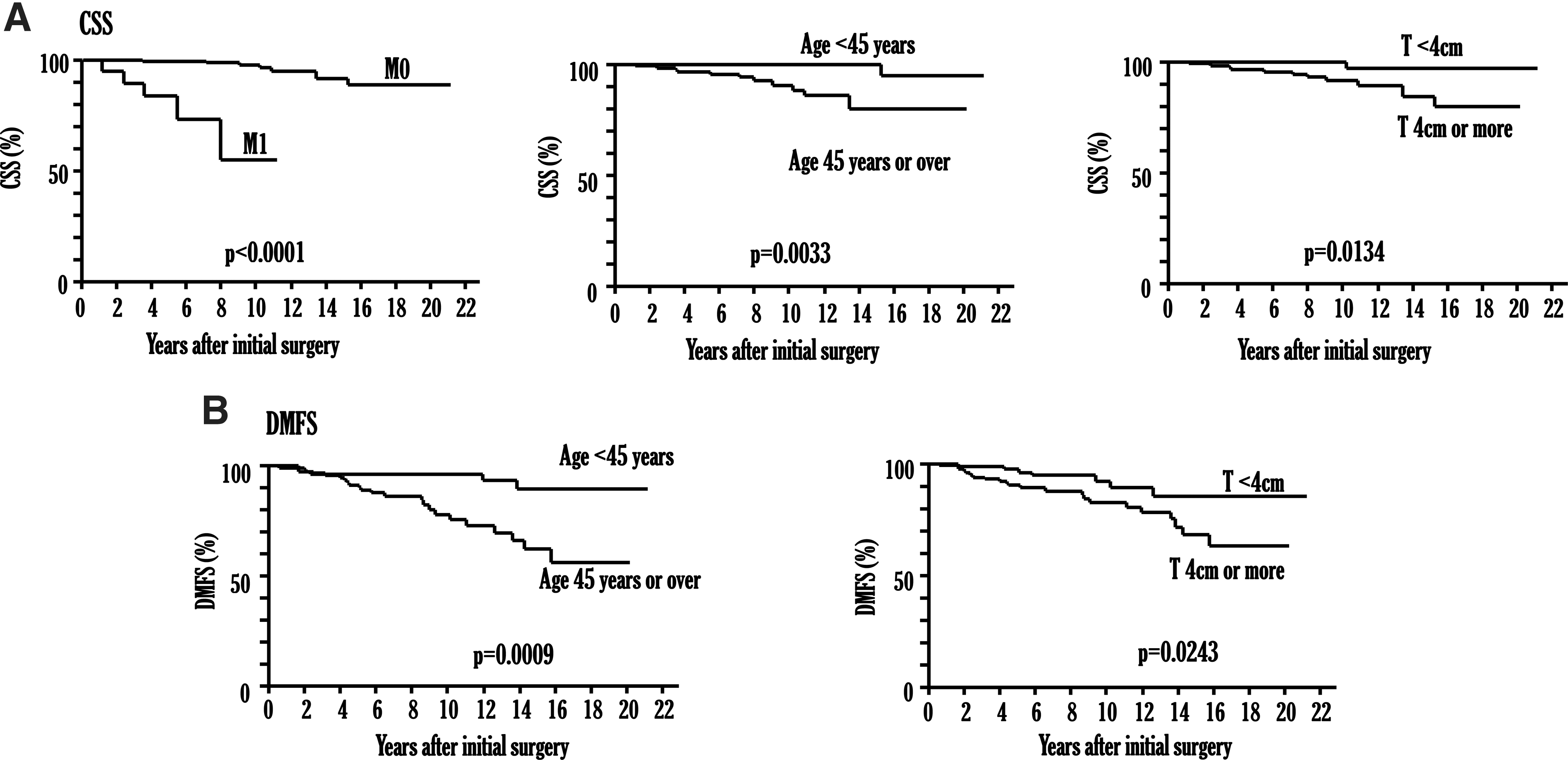
The CSS curve for all patients calculated by Kaplan–Meier method is shown in Figure 1A, and the 10-, 15-, and 20-year CSS rates were 95.2%, 89.5%, and 84.5%, respectively. CSS was significantly poorer in the group of patients who were ≥45 years, in the group whose primary tumor size was ≥4 cm, and in the M1 group (Fig. 2A). The 10-, 15-, and 20-year CSS rates of the M0 patients were 97.8%, 91.9%, and 86.8%, respectively, whereas the 5- and 10-year CSS rates of the M1 patients were 83.8% and 55%, respectively. The outcome of the group with distant metastases at presentation was significantly poorer than in the group without distant metastases at presentation. The DMFS curve of the 229 M0 patients calculated by the Kaplan–Meier method is shown in Figure 1B, and their 10-, 15-, and 20-year DMFS rates were 85.8%, 72.6%, and 70%, respectively. The DMFS rate was significantly lower in the group of patients who were ≥45 years and in the group whose primary tumor size was ≥4 cm (Fig. 2B).
Cumulative cause-specific survival (CSS) curve
Univariate analysis in relation to CSS
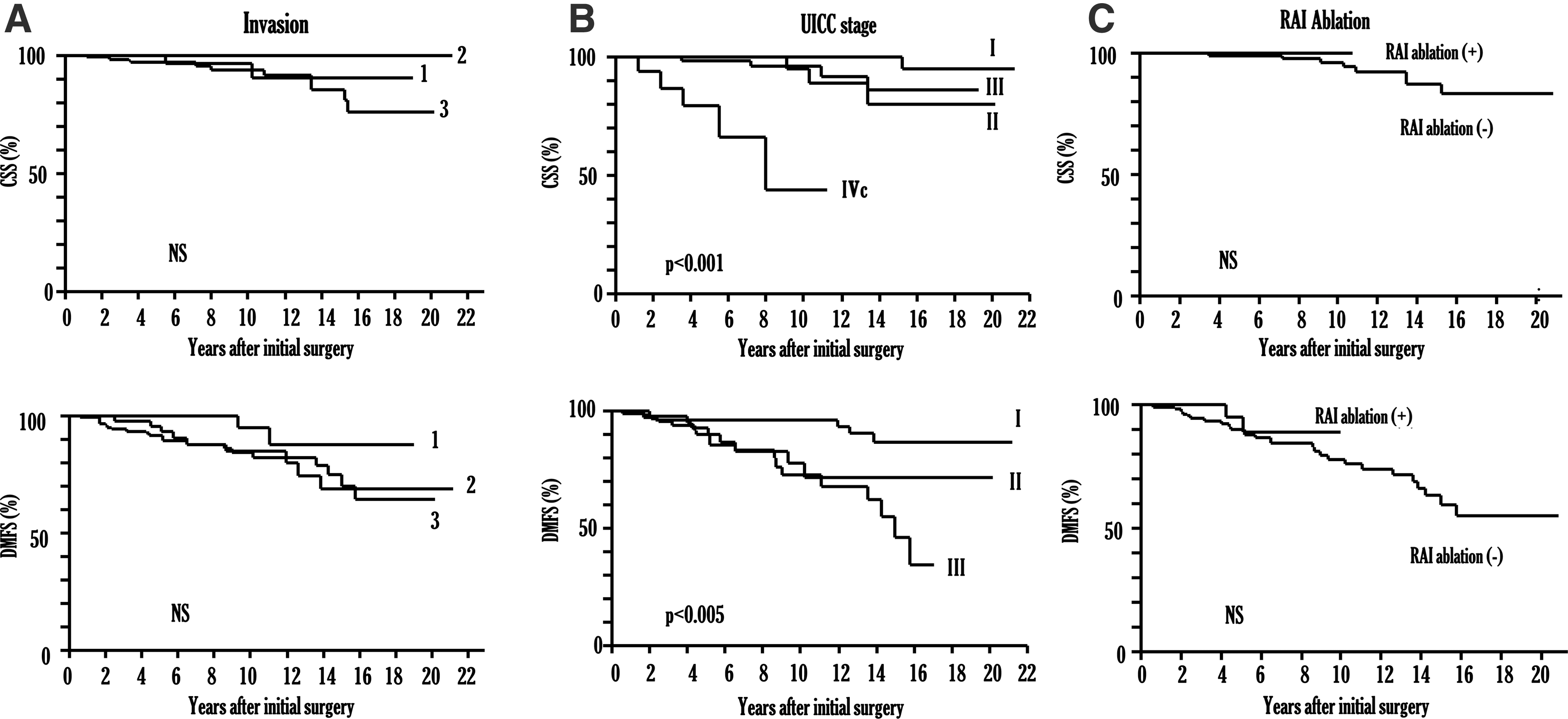
Forty patients had capsular invasion alone, 56 patients had vascular invasion alone, and 153 patients had both vascular and capsular invasion. Two patients had neither capsular nor vascular invasion; however, one of them had lung metastases and the other had lymph node metastases. Distant metastases were observed in 5 patients (12.2%) with capsular invasion alone, 10 patients (17.9%) with vascular invasion alone, and 38 patients (25%) with both vascular and capsular invasion. One patient who did not have capsular or vascular invasion developed distant metastases. The differences among DMFS rates of the group with capsular invasion alone, the group with vascular invasion alone, and the group with both capsular and vascular invasion were not significant (Fig. 3A). Nor were the differences among their CSS rates significant (Fig. 3A).
CSS curve and DMFS curve according to capsular invasion and vascular invasion
CSS and DMFS were evaluated (Fig. 3B) according to the American Joint Committee on Cancer/Union for International Cancer Control Tumor–Node–Metastases (TNM) classification staging system (14,15). There were 116 patients with stage I, 47 patients with stage II, 70 patients with stage III, and 18 patients with stage IV disease. Stage IV was significantly related to reduced CSS compared with stages I, II, and III (p<0.0001). Stages II and III were significantly related to reduced CSS compared with stage I (p<0.0001); however, there was no significant difference between stage II and III. Further, DMFS curves differed significantly between all three stages (Fig. 3B). Stage III was significantly related to reduced DMFS compared with stages I and II (p<0.005).
The results of the multivariate analysis in relation to CSS and DMFS are shown in Table 2. Age was identified as an independent significant prognostic factor for poorer CSS and was also a significant factor related to DMFS in the M0 group.
CSS, cause-specific survival; DMFS, distant-metastases-free survival.
Discussion
There is a great deal of controversy concerning the pathological diagnosis and treatment strategy for FTC, especially minimally invasive FTC. Minimally invasive FTC is difficult to diagnose prior to thyroidectomy unless distant metastases or lymph node metastases have been detected. A definite diagnosis is usually made after hemithyroidectomy. Based on the degree of invasiveness, follicular carcinoma is now classified into two categories: minimally invasive follicular carcinoma and widely invasive follicular carcinoma (13). However, considerable differences of opinion remain among endocrinologists, pathologists, and endocrine surgeons about the criteria for making the diagnosis of follicular carcinoma. Several reports proposed classifying follicular carcinoma into three categories: minimally invasive, intermediate (moderately) invasive, and widely invasive. In some histological classification schemes (10,11,16,17), the criterion for a histological diagnosis of minimally invasive FTC is microscopic penetration of the tumor capsule without vascular invasion, and it carries no excess mortality. According to the 2009 revision of the ATA guidelines for the management of patients with thyroid nodules and differentiated thyroid cancer, and because of the excellent outcome associated with surgical resection alone, RAI ablation may not be necessary for all patients with a small follicular thyroid cancer manifesting only capsular invasion histologically (1,18). The WHO classification of tumors of endocrine organs defines follicular carcinoma in which there is limited capsular and/or vascular invasion as minimally invasive (13). The pathological classification used in the present study was based on the WHO classification, and the results of this study showed that the outcome of minimally invasive follicular carcinoma are not always good, even in patients with capsular invasion alone. Three of the 42 patients with capsular invasion alone (7.1%) had distant metastases. The results of this study showed that vascular invasion was not a risk factor for distant metastases and patients with capsular invasion alone required further treatment.
Several prognostic indices for differentiated thyroid carcinoma have been proposed. They are usually applied to patients with papillary carcinoma, not follicular carcinoma. To our knowledge, only one study addressed this issue solely for patients with FTC. There were relatively few studies when comparing existing prognostic staging systems in only FTC patients. Age at presentation is a well-established strong prognostic factor for differentiated thyroid carcinoma (19 –24). In several reports, age at presentation was a strong and independent prognostic factor only for PTC (25 –27), and the fact that age at presentation is not of any prognostic importance in FTC has already been described by others (28 –31). On the other hand, some authors identified older age as a poor prognostic factor in patients with FTC (32 –35). There have been few studies that compared the staging system or prognostic indices in patients with FTC (10,11,16,17). In these studies, the 6th TMN staging system and MACIS system were reported to be commendable staging systems to predict the prognosis of patients with FTC. Our results showed that TNM staging system reflected the prognosis of patients with minimally invasive FTC to some extent. Distant metastases are thought to be an important factor related to the prognosis of patients with FTC and the patients with stage IV had a significantly poorer outcome. The 10- and 5-year CSS rates of the M1 patients in our study were 83.8% and 55%, respectively, percentages much lower than those of the M0 patients. However, since age was a more powerful prognostic factor than distant metastases, younger patients have a good prognosis even if they have distant metastases. Patients under 45 years old with distant metastases are classified as stage II in the TNM staging system. Age is a prognostic factor in the current TNM staging system for differentiated carcinoma, but histological findings, such as degree of invasiveness (widely invasive type or minimally invasive type), are not taken into account. It is well known that patients with widely invasive FTC have a poorer outcome than patients with minimally invasive FTC. The outcome and prognostic factors for minimally invasive FTC and widely invasive FTC should be analyzed and discussed separately. Further, the histological criteria for the diagnosis of FTC should be based on universal criteria. As stated previously, the histological diagnoses of FTC in earlier reports were based on the criteria at each institution.
The adequacy of iodine intake is thought to be related to the biological behavior of FTC. Many studies have shown that the incidences of FTC and anaplastic thyroid carcinoma are higher in iodine deficiency areas (36,37), and that PTC is predominant in iodine-replete populations. An increase in the ratio of PTC to FTC is seen in populations after the start of iodine prophylaxis. The distribution and characteristics of thyroid tumors in former iodine-deficient countries have approached those of iodine-sufficient countries. Japan is known to be an iodine-sufficient country, and the biological characteristics of FTC in formerly iodine-deficient countries are thought to be similar to the characteristics of FTC in Japan. The outcome of FTC in iodine-deficient areas has been reported to be poorer than in iodine-sufficient areas. Distant metastases ratio in patients with minimally invasive FTC (22%) was apparently high; however, cumulative DMFS ratio was almost similar to those of other recent reports (5,6,26).
In most Japanese institutions, routine RAI ablation after completion total thyroidectomy is not performed for all patients in whom FTC has been diagnosed histologically after lobectomy (6,38,39), because the use of RAI is strictly restricted by law in Japan and Japanese endocrine surgeons and endocrinologists do not consider FTC to have as poor a prognosis in Japan as it does in other countries. That is also why the treatment strategy for FTC is not as aggressive in Japan as it is in other countries.
It is not clear whether completion total thyroidectomy and radioiodine ablation prevent the occurrence of distant metastases, but these procedures make it possible to detect distant metastases at their early stage (1,40,41). Early detection of distant metastases and radioiodine treatment has been reported to improve disease-specific survival if the disease is functioning metastases (42 –44). Prognosis of patients without risk factors was excellent and distant metastases rarely occurred. Routine completion total thyroidectomy and radioiodine ablation is thought unnecessary for these patients. On the other hand, it is not clear from our study that prognosis of patients with risk factors will be improved by completion total thyroidectomy and RAI ablation before distant metastases are observed. However, according to previous reports, the prognosis of patients with these risk factors will be improved by radioiodine treatment at their early stage. Since 2000, RAI ablation after completion total thyroidectomy has been performed mainly for patients with minimally invasive FTC aged 40 or older. Because of the short follow-up periods, there were no significant difference in the outcome between patients who received RAI ablation and patients who did not (Fig. 3C). However, no patient who received RAI ablation died of the disease. With longer follow-up periods, RAI ablation after completion total thyroidectomy would bring better outcomes to patients with risk factors.
Conclusions
Age is the most powerful prognostic factor for minimally invasive FTC. The prognoses of patients younger than 45 years old were excellent and distant metastases rarely occurred. Routine completion total thyroidectomy and radioiodine ablation may be unnecessary for these patients.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.