
Abstract
Background:
Thyroidectomy is a standard treatment for thyroid cancers. Hoarseness due to the paralysis of the recurrent laryngeal nerve is one of the most common postoperative complications, and has been studied by many investigators. However, voice quality after thyroidectomy in patients in whom recurrent laryngeal nerves were preserved and vocal cord morbidity was endoscopically normal has not been well studied. To understand voice quality after thyroidectomy further, we conducted a time-course analysis of voice quality in patients who had thyroidectomy with normal cord morbidity by various measures.
Methods:
We evaluated voice parameters including the Voice Handicap Index-10 (VHI-10), the vocal efficacy index, the fundamental frequency (F0), the maximum phonation time (MPT), the mean air flow rate (MFR), jitter, shimmer, and the noise-to-harmonics ratio (NHR) before and after total thyroidectomy (TT) or lobectomy (LO) for thyroid cancers in 110 patients in whom the recurrent laryngeal nerves were preserved without apparent injury and normal vocal cord mobility was confirmed by endoscopic examination. Thirteen patients who underwent parotidectomy were enrolled as controls.
Results:
Immediately after surgery, significant decreases in MPT (p=0.003) and significant increases in jitters, shimmers, and NHR (p=0.0002, 0.02, and 0.03, respectively) were observed in the patients who underwent TT. In comparison with the controls, jitters and NHR were significantly higher in the patients who had a TT (p=0.03, 0.04). MFR was significantly higher in the patients who had an LO than in the controls (p=0.02). As compared with the patients who had an LO, MPT was significantly shorter (p=0.0004) and MFR and NHR were significantly higher (p=0.004, 0.03) in the patients with a TT. In the patients who had a TT, the MPT immediately after the surgery was significantly longer in the patients who had simultaneously neck dissection (ND) in comparison with the patients who did not have ND. However, all these differences gradually decreased and were not significant at one month after surgery.
Conclusions:
Our results suggest that TT and ND have a distinct impact on voice quality after surgical treatment for thyroid cancer, probably due to slight and transient nerve conduction disorders induced by the manipulation around recurrent laryngeal nerves and/or laryngeal edema induced by the disturbance of venous and lymphatic drainages. However, these changes appear to be temporary, lasting only a few weeks.
Introduction
To date, a number of studies have been reported on voice dysfunction after thyroidectomy in patients without apparent paralysis of the RLN or EBSLN (5,8
–12). In these articles, many factors are proposed as possible causes of voice alternation, in particular: 1. Transient neural conduction disorder of the RLN; 2. Transient neural conduction disorder of the EBSLN; 3. Movement disturbance of the cricothyroid muscle; 4. Temporary malfunction of the strap muscles (5), resulting from the surgical approach; 5. Laryngotracheal fixation by scar-impairing vertical movement (5); 6. Mucosal damage, hematoma, inflammation, and consolidation of the vocal folds (10, 11); and 7. Laryngeal edema induced by the disturbance of venous and/or lymphatic drainages.
Furthermore, sex (12), emotional and behavioral conditions (13), and mental stress (14) have been pointed out as potentially influential factors.
However, most of the studies did not demonstrate the impact of these factors on the voice quality in patients without injury of the RLN or EBSLN. Several studies (9,12,15,16) failed to demonstrate a significant impact of surgical procedures for thyroid cancer on the postoperative voice, and most of these studies had a small sample size. To clarify the mechanism of voice dysfunction in patients who underwent surgical treatment for thyroid cancer without injury to the RLN or EBSLN, we evaluated the voice of the patients who had surgical treatment for thyroid cancer by means of mental, acoustic, and aerodynamic analysis.
Materials and Methods
Subjects
A total of 110 patients who underwent surgical treatment for thyroid cancer at Kuma Hospital from July 2009 to February 2010 were enrolled in this study. In all patients, the RLN and the EBSLN were anatomically preserved without injury, and no apparent vocal fold palsy was observed on the postoperative endoscopic examination. Age ranged from 19 to 85 years with a mean age of 53 years. Nineteen patients were men and 91 patients were women. Thirteen patients who underwent parotidectomy at Kobe University Hospital from November 2010 to June 2011 were used as controls, as we considered that this would not affect the voice. All subjects had no history of voice disease or previous neck surgery. The characteristics of the subjects are shown in Table 1. Total thyroidectomy (TT) and lobectomy (LO) were each performed on 55 patients. Lateral neck lymph nodes were simultaneously dissected on 17 patients with TT. No patient undergoing LO had lateral neck dissection (ND). Assessment of voice was performed preoperatively, immediately after surgery, and again at one and three months after surgery.
Surgical technique
Kuma Hospital is a specialized hospital for thyroid diseases, and surgeons are well-trained in thyroid surgery. The RLNs were routinely identified and preserved if these were not affected by the cancers. The EBSLNs were not necessarily identified, but surgery was carefully performed so as not to damage these nerves and cricothyroid muscles. The sternohyoid muscles were preserved in most cases. The sternothyroid muscles were dissected in cases where there was an enlarged thyroid gland (estimated weight was >200 g) or invasion. Modified lateral ND was performed in patients with lymph node metastases.
Pre- and postoperative voice assessment
For acoustic voice analysis, the patients' voices were recorded using a 24-bit WAVE/MP3 recorder (Edirol R-09, Roland, Tokyo, Japan). The sampling frequency was set at 44.1 kHz. A microphone was set at a distance of ∼20 cm from the mouth. The patients were asked to pronounce the sustain vowel “a” at their self-selected comfortable pitch and intensity. All samples were recorded in a soundproof room. Praat (17) was used for acoustic voice analysis. A middle stationary segment with a length of 2.5 sec was chosen for analysis of fundamental frequency (F0), the lowest vibration rate of vocal folds, jitter, shimmer, and noise-to-harmonics ratio (NHR). Maximum phonation time (MPT) and mean air flow rate (MFR) were obtained by the sustained vowel “a” at a comfortable pitch and intensity for as long as possible. The vocal efficacy index, measured as the alternating current/direct current (AC/DC) ratio (18), was obtained by a middle stationary segment of each sustained vowel production using Phonation Analyzer PA-1000 (Minato Medical Science Co., Osaka, Japan).
The Voice Handicap Index-10 (VHI-10), a mental assessment battery published by Rosen et al. (19), was used as mental assessment. The VHI-10 consists of 10 questions that are rated according to a five-point ordinal scale: 0, never; 1, almost never; 2, sometimes; 3, almost always; and 4, always. The total score ranges from 0 (no problem perceived) to 40 (maximum perceived disability due to voice difficulties).
Statistical analysis
The values of each parameter, except VHI-10, were divided by their own preoperative value to demonstrate the time-related change from baseline. JMP version 8.0 (SAS Institute, Cary, NC) was used for the statistical analysis. For comparison of the preoperative data with the postoperative data, Dunnett's multiple comparison test was applied. A Tukey–Kramer multiple comparison test was used to compare the values among the groups at the same period. p<0.05 was determined as significant.
This study was approved by the ethical committees of Kuma Hospital and Kobe University Graduate School of Medicine. Informed consent was obtained from all the participants of this study.
Results
Impact of thyroidectomy on the quality of voice
To investigate the impact of TT and ND on voice quality, we first analyzed the voice quality of the patients who had only a TT (n=38) or LO (n=55), but did not have an ND, measuring the following parameters: VHI-10, vocal efficacy index, F0, MPT, MFR, jitter, shimmer, and NHR.
Despite the significant changes in several objective parameters (see below), the values of VHI-10 were not significantly different among the patients who had a TT or LO, or the controls at any postoperative time point. Also, no significant difference was observed in each group before and at any postoperative time point (Fig. 1A). Values of vocal efficacy index and F0 were not significantly different among the patients undergoing TT, LO, and the control group at any postoperative time point. Also, no significant difference was observed in each group before and at any postoperative period (Fig. 1B, C). Immediately after surgery, a significant decrease of the MPT (p=0.003, Fig. 1D) was observed in comparison with the preoperative values in the patients who had a TT. In comparison with the patients who had a LO, immediately after surgery, the MPT was significantly shorter (p=0.0004, Fig. 1D), whereas the MFR (p=0.004, Fig. 1E) was significantly higher in the patients who had a TT. Comparing the control group with the patients who had a TT or LO, the MFR of patients having an LO was significantly lower than that of the control group (p=0.02, Fig. 1E). These differences gradually decreased and were not present at one month after surgery.
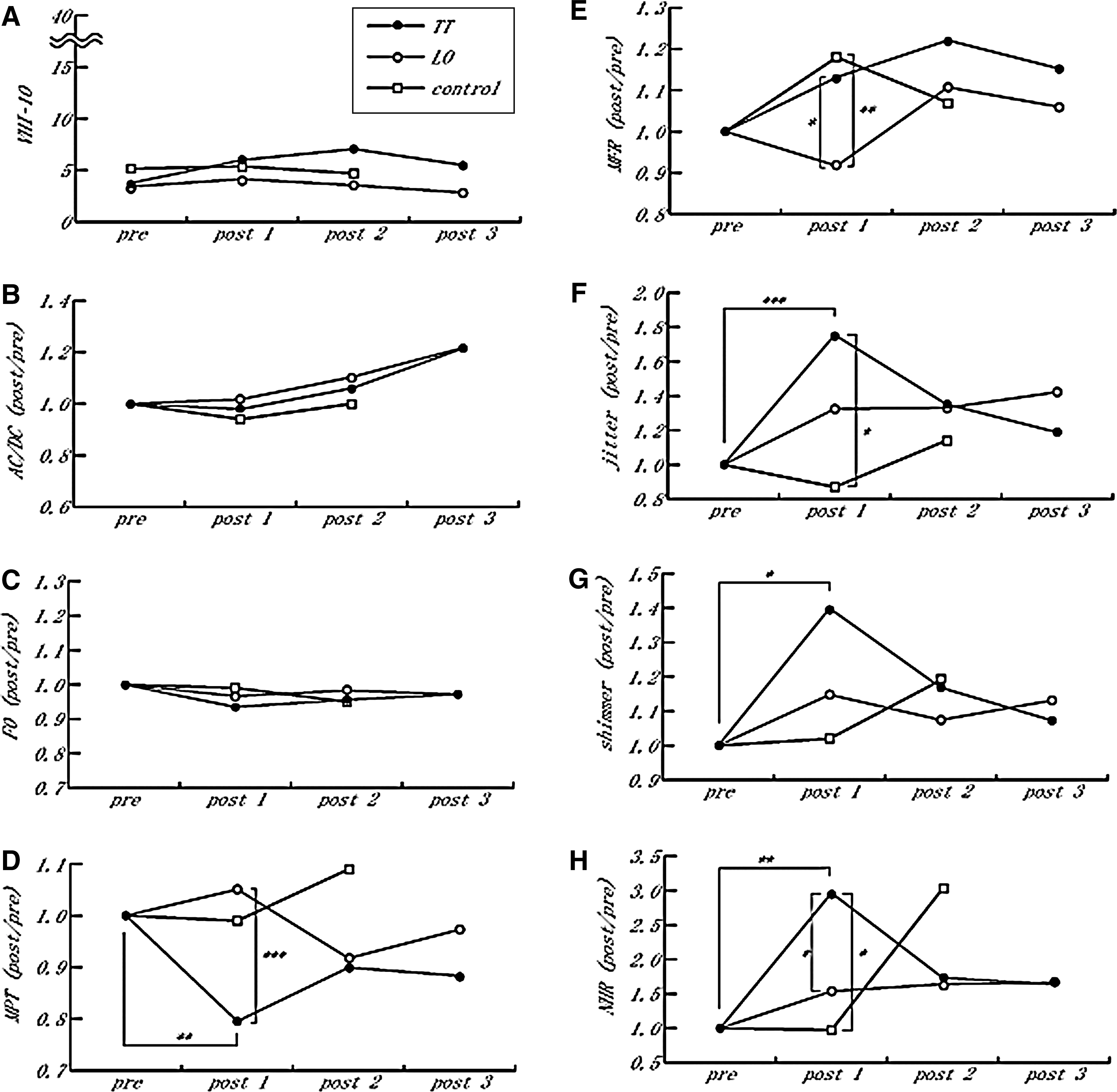
Time-dependent change of subjective and objective parameters of the patients with a TT (•) or LO (○), and those of control patients (□).
Immediately after surgery, significant increases in jitter (p=0.0002, Fig. 1F) and shimmer (p=0.02, Fig. 1G) were observed in comparison with the preoperative values in the patients who had a TT. Comparing the control group with the patients who had a TT or LO, jitter (p=0.03, Fig. 1F) was significantly higher in the patients who had a TT compared with control patients. Similarly, immediately after the surgery, significant increases of the NHR (p=0.001, Fig. 1H) were observed compared with the preoperative values in patients who had a TT. In comparison with patients who had an LO, the NHR values (p=0.03, Fig. 1H) were significantly higher in the patients who had a TT. Comparing the control group with patients having a TT or LO, the NHR values (p=0.04, Fig. 1H) of the patients with a TT were significantly higher than those of control patients. These differences gradually decreased and were not present one month after surgery.
Impact of neck dissection on voice quality
To evaluate the impact of neck dissection on the postoperative quality of voice, we compared the patients who had an ND (n=17) to the patients who did not have an ND (n=38). All patients in this analysis had a TT. Immediately after the surgery, the MPT was significantly longer in the patients who had an ND in comparison with the patients who did not have an ND (p=0.004, Fig. 2D). This difference gradually decreased and was not present one month after surgery. No other significant differences were observed between the patients who had an ND and the patients who did not have an ND.
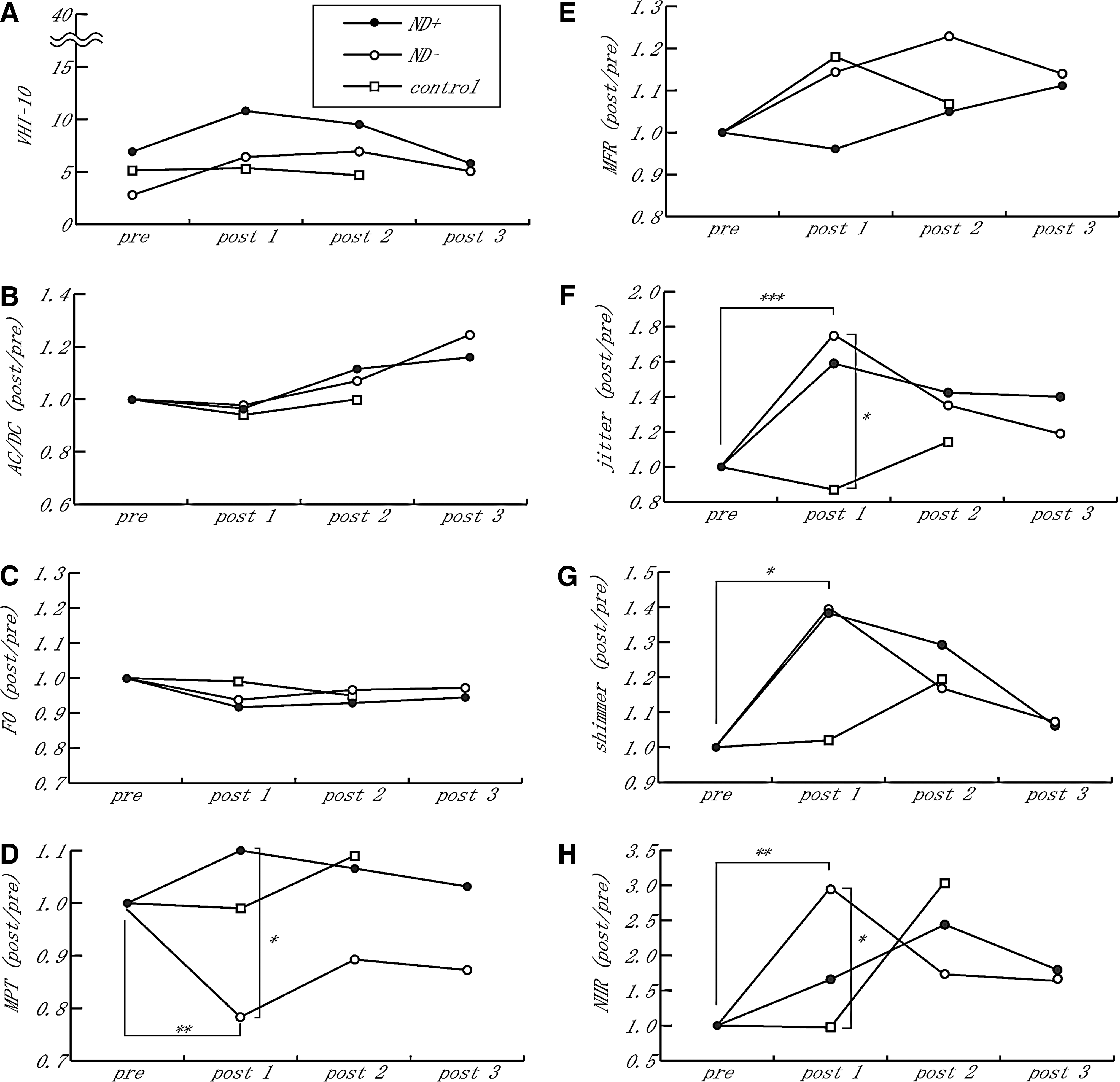
Time-dependent change of subjective and objective parameters of the patients with (•) or without (○) neck dissection, and those of control patients (□).
Impact of intubation on voice quality
The average intubation time of the patients who had a TT was significantly longer than that of the patients who had an LO (110.1 vs. 76.5 min; p=0.0009). The average intubation time of the subjects in the control group was even longer than that of the patients who had a TT and ND (226 vs. 192.4 min; not statistically significant). Despite the significant longer intubation time of the control patients (Tukey–Kramer multiple comparison test, TT vs. control: p<0.0001; LO vs. control: p<0.0001), the values for F0, MPT, jitter, shimmer, and NHR in the control patients were better than those in the patients who had a TT or LO (Fig. 1).
Discussion
The main goal of this study was to clarify the mechanism of voice dysfunction in patients who had surgical treatment for thyroid cancer without apparent injury of the RLN or EBSLN. For this purpose, we analyzed voice quality in patients who had surgical treatment for thyroid cancer according to the types of surgical treatment for thyroid and cervical lymph nodes. The major findings were: (i) several voice parameters in the patients who had a TT deteriorated significantly immediately after thyroid surgery; (ii) these changes recovered within one month; and (iii) ND might interfere with the decrease of the MPT in the patients who had a TT.
Several researchers investigated the impact of thyroidectomy on voice quality (9,12,15,16) and concluded that there was no significant difference in voice quality according to the types of surgical procedure for thyroid cancer. The most probable reason for the difference between these studies and our study might be the sample size, since the number of patients in most of these studies was limited. The difference between the study of Stojadinovic et al. (16) and ours might come from the statistical procedures. We used the values of postoperative data divided by their own preoperative data for analysis in order to eliminate the effect of differences among individuals.
The VHI-10 is a mental assessment battery published by Rosen et al. (19), which is a shortened version of the Voice Handicap Index (VHI) published by Jacobson et al. (20). Irrespective of the diagnosis, the correlation between the VHI and the VHI-10 was >0.90 (p=0.01) (19). In the present study, despite the significant changes in several objective parameters, values of the VHI-10 were not significantly different among the patients who had a TT or LO, or during the postoperative periods of each patient group. These results indicate that subjective changes in voice after thyroidectomy were so minimal that the patients did not recognize the differences, as long as the RLN and the EBSLN were anatomically preserved by the well-experienced surgeons and no apparent recurrent palsy or subjective changes in the vocal cord were observed at the postoperative endoscopic examination.
In the present series, the F0 values were also not significantly different among the patients who had a TT, LO, or the controls, or during the postoperative periods of each patient group or between the patients who had or who did not have an ND. The F0 is the lowest vibration rate of vocal folds and is influenced by the length, size, and tension of the vocal folds. Movement disorder of the cricothyroid muscle and laryngotracheal fixation by scar-impairing vertical movement lead to a decrease of F0 (5). Thus, no significant change of F0 in this series indicated that the EBSLN and cricothyroid muscles were not damaged during the surgical treatment for thyroid cancer in all subjects in this series.
The vocal efficacy index (18) is the AC/DC ratio, reflecting the difference between modulated AC flow and unmodulated DC flow (21). In cases of glottal closure insufficiency, the AC/DC ratio is considerably reduced due to the decrease of modulated AC flow (22). The MPT is a measure of the ability to regulate ventilator and laryngeal systems for voice production independent of a frequency or intensity target (16). The MFR is the average flow rate of air through the vocal folds (in L/sec). In cases of vocal dysfunction or laryngeal pathology, a decrease of MPT and an increase of MFR are predicted. In the present study, the MPT was significantly lower and the MFR was significantly higher in the patients who had a TT immediately after the surgery, comparing with the preoperative status of the patients having an LO or the control patients. Although no significant differences were observed in the vocal efficacy indices, these results suggest insufficient glottic closure, especially in the patients who had a TT.
Possible explanations for these changes are (i) slight and transient damage of the RLN, EBSLN, and/or cricothyroid muscle, or (ii) vocal cord stiffness due to inflammation and edema (10,11,23). Indeed, a TT has a higher potential to affect these nerves and muscles than a LO. Because the F0 was not significantly different in all the patients in the present study as mentioned above, the possibilities of injury to the EBSLN and/or the cricothyroid muscles were considered minimal. While no apparent vocal fold palsy was observed on the postoperative endoscopic examination in the present series, partial RLN dysfunction may be missed by standard endoscopic examination. Thus, the greater changes in the MPT and the MFR in the patients who had a TT suggest that total surgical thyroidectomy has a possibility to induce slight and transient nerve conduction disorders, which might result in a slight glottal closure insufficiency. However, postoperative cricothyroid muscle EMG should be performed to draw a definitive conclusion since cricothyroid muscle EMG is the only method to provide objective information as to the functioning of the external branch of the superior laryngeal nerve (24).
Vocal cord stiffness due to inflammation and edema after surgery might also be responsible for these results. The surgical area in patients who had a TT is obviously wider than in patients who had an LO. Thus, immediately after surgery, venous return and/or lymphatic drainage should be damaged more severely, and greater vocal cord stiffness might tend to occur, in patients who had a TT than in patients who had an LO. Rigid vocal cords might shorten the glottal closure time and demand redundant air flows during phonation, causing irregular variation of frequency and peak amplitude.
Jitter is the pitch perturbation quotient and shimmer is the amplitude perturbation quotient. The NHR is calculated as the ratio of noise and harmonics components. Simply speaking, jitter, shimmer, and the NHR indicate irregular frequency, irregular amplitude, and increasing noise component of voice respectively (25). Thus, a significant deterioration of these parameters in the patients who had a TT compared with patients who had an LO, as shown above, also suggest that thyroidectomy spontaneously causes mucosal stiffness of the vocal cord.
Few studies discuss the influence of neck dissection on voice after thyroidectomy. Van Lierde et al. (9) reported the possibility that slight modifications of the vascular supply and/or disturbance of venous drainage of the larynx promote postoperative voice alteration. Storper et al. (26) reported severe laryngeal edema secondary to a circulation disturbance. Based on these reports, we assumed that neck dissection during thyroidectomy might influence postoperative voice parameters. In the present study, there was a significant difference in the MPT between patients having an ND and those not having an ND. As expected, the MPT immediately after surgery of patients who had an ND was significantly longer than that of patients who did not have an ND. The difference gradually decreased in the month after surgery. Laryngeal edema, due to disturbance in venous and lymphatic drainage after ND, might fill in a slight glottal closure insufficiency caused by the subclinical transient recurrent laryngeal nerve conduction disorders related to TT.
Another explanation for the deteriorated subjective parameters of voice of the patients undergoing TT and ND is the influence of longer endotracheal intubation. However, despite the significantly longer intubation time of the control group, the values of F0, MPT, jitter, shimmer and NHR of the control were better than those of the patients who had a TT or LO. Peppard et al. (10) reported that 30 (6.3%) of 475 patients following general endotracheal anesthesia were found to have traumatic lesions of the larynx or hypopharynx, and 20 of 30 patients (66.7%) complained of hoarseness, but no correlation could be drawn between the injured and uninjured groups with respect to length of intubation. Hamdan et al. (23) performed an acoustic analysis of 35 patients who were admitted for non-ear, nose, and throat surgery. In this study, the MPT was increasing and the F0 became higher 24 h after surgery, but other indexes (jitter, shimmer, and NHR, among others) did differ significantly. Beckford et al. (27) reported the voice changes of 10 gynecological patients and concluded that, although jitter increased postoperatively, no consistent difference was observed in the F0 and laryngeal endoscopy, stroboscopic laryngoscopy, and EGG. On the basis of these reports and our present results, glottic contribution to postintubation vocal changes is rather minimal, and other extralaryngeal factors may be responsible.
In conclusion, we investigated the voice changes after thyroidectomy using the following parameters: VHI-10, vocal efficacy index, F0, MPT, MFR, jitter, shimmer, and NHR. The major findings are: (i) several voice parameters in the patients who had a TT deteriorated significantly immediately after surgery; (ii) these changes recovered within one month; and (iii) neck dissection might interfere with the decrease of the MPT resulting from TT. These voice changes might be due to slight and transient damages of the RLN, and from mucosal stiffness of the vocal cords following laryngeal edema. Laryngeal edema due to the disturbance of venous and lymphatic drainages after neck dissection might improve the decrease of MPT induced by TT. In our series, EBSLNs and cricothyroid muscles were not considered to be damaged by surgical treatment for thyroid cancer.
Footnotes
Acknowledgments
The authors thank Hisashi Ota, chief clinical laboratory technologist, and all the members of the laboratory in Kuma Hospital for their assistance in the measurement of the voice parameters in this study.
Author Disclosure Statement
No competing financial interests exist.