
Abstract
Background:
Transaxillary robotic thyroidectomy, developed by the Yonsei University group from Seoul, Korea, is a new approach that eliminates the need for a cervical incision. Originally, this technique was performed using a two-incision technique (ipsilateral axilla and anterior chest wall). More recently, the chest wall incision is being eliminated and a less invasive robotic thyroid procedure is being performed through a single axillary incision.
Summary:
The complexity of this new technique introduces the potential for new complications particularly during the initial learning curve that are not routinely or previously associated with conventional open thyroidectomy. This article will aide surgeons in overcoming the learning curve of transaxillary single-incision robotic thyroidectomy (TSI-RT), giving a detailed explanation of the robotic surgical procedure, the possible complications, and complication management.
Conclusions:
If surgeons have mastery of the multiple steps of the robotic surgical procedure and a good understanding of possible complications and how to prevent them, TSI-RT can be performed safely and offers numerous advantages over multi-incision robotic thyroidectomy as well as conventional open thyroidectomy.
Introduction
Recently, thousands of robotic thyroidectomies using a gasless, transaxillary approach have been performed by Dr. Chung's group in Seoul, South Korea over the last decade (10 –18). The procedure is now being introduced in the United States. It has been slower to catch on domestically due to the higher cost structure than conventional thyroid surgery. Moreover, for safe implementation of a new technique, surgeons should minimize perioperative complication rates and assure patient safety (19). Therefore, there is a need for familiarization of the “new” anatomy associated with the new approach. Traditional thyroid surgeons are comfortable with the anatomy of a conventional open approach, but in robotic transaxillary thyroidectomy using the remote approach to the gland, the view is from the inferior and lateral direction. For this reason, perioperative complication rates in robotic transaxillary thyroidectomy may increase during the initial segment of the learning curve.
In this article, the procedure of the transaxillary single-incision robotic thyroidectomy (TSI-RT) will be described to provide a better understanding of the technique as well as potential-related complications and their management.
Technique
Room setup
The da Vinci Surgical System comprises three components: a surgeon's console, a patient-side robotic cart with four arms manipulated by the surgeon (one to control the camera and three to manipulate instruments), and a high-definition three-dimensional (3D) vision system. Because this system is bulky and the console is located in the same operating room, it is recommended that the da Vinci System be accommodated in a large operating room. The surgeon's console is located in a fixed position, while the positioning of the patient-side cart can be changed depending on whether the axillary surgical incision is being made on the right or left side. The patient-side cart should be positioned on the contralateral side to the incision and be covered with sterile drapes. Initially, it should be away from the table so that an assistant on the contralateral side can hold a manual retractor to create the working space in preparation for placing the Chung transaxillary thyroidectomy retractor.
The table is oriented so that the anesthesiologist is at the head of the table and has access to the patient's airway, head, and neck. Another assistant on the ipsilateral side may hold an endoscopic camera or light source to provide the operator with a clear view of the operative field.
Robot arm setup
Before induction of anesthesia, the robot arms of the patient-side cart should be set up to configure the appropriate position depending on the incision site of the patient. For the right-sided approach, the number 2 arm, the camera arm, the number 1 arm, and the number 3 arm should be placed, respectively, in order from superior to inferior (Fig. 1). The camera arm is used for the 30° dual channel endoscope (Intuitive Surgical, Inc., Sunnyvale, CA), the number 2 arm is used for the Maryland dissector (Intuitive Surgical), the number 1 arm for the ProGrasp forceps (Intuitive Surgical), and the number 3 for the harmonic curved shears (Intuitive Surgical). For the left-sided approach, the number 1 arm, the camera arm, the number 2 arm, and the number 3 arm should be placed, respectively, in order from superior to inferior (Fig. 2). The number 1 arm is used for the harmonic curved shears, the number 2 arm for the ProGrasp forceps, and the number 3 for the Maryland dissector. Therefore, to reduce the docking time, it is essential that the surgical team preoperatively set up the proper position of the robot arms.
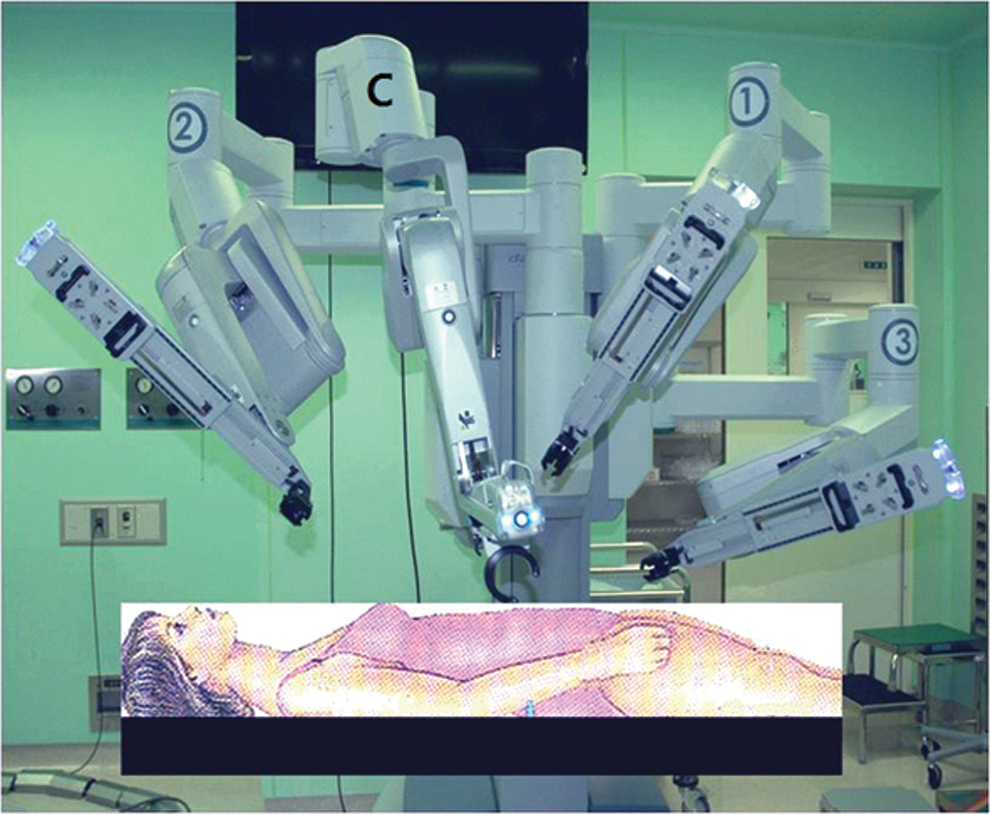
Right-sided approach to transaxillary single-incision robotic thyroidectomy. Color images available online at
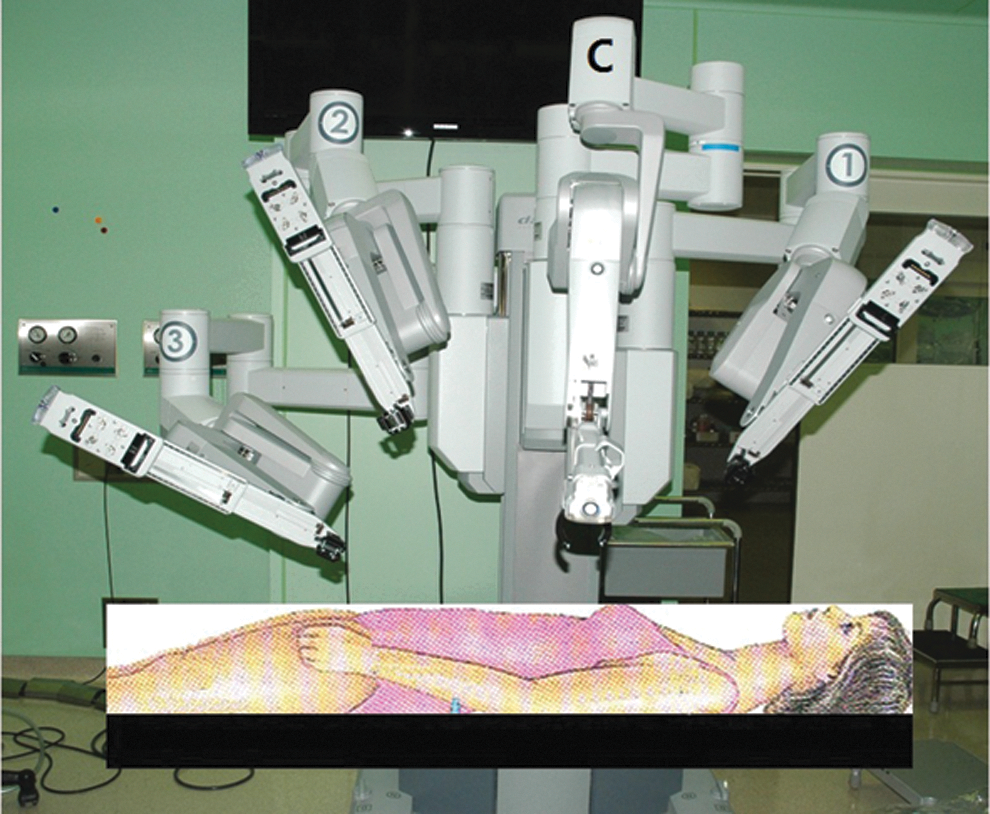
Left-sided approach to transaxillary single-incision robotic thyroidectomy. Color images available online at
Patient position
In the gasless, transaxillary approach, good positioning is essential for a secure adequate working space and clear exposure. The patient is placed in the supine position under general anesthesia. The neck is slightly extended using a shoulder roll, and the lesion-side arm is placed in an arm board extended cephalad to expose the axilla (Fig. 3).

Patient positioning and skin markings showing the incision line. Color images available online at
Marking the patient
A vertical line is drawn from the sternal notch to the hyoid bone in the midline. A 5- to 6-cm line is marked in the axilla at the posterior aspect of the pectoralis muscle. A diagonal line is marked to represent the anterior border of the sternocleidomastoid muscle (SCM). The arm should not be fixed in place until after the patient's incision is marked to assure that the marked incision will be hidden in the axilla postoperatively. The arm can then be secured in place with meticulous care to protect all pressure points and avoid undue stretching on the shoulder, elbow, or wrist joints. To define the extent of dissection, a line is then drawn from the superior aspect of the axillary incision line to the superior aspect of the midline marking, and from the inferior aspect of the axillary incision line to the inferior aspect of the midline marking.
Placement of the nerve monitoring system
Before preparing the patient, the laryngeal nerve monitor grounding electrode is inserted. The electrode can be placed slightly off the midline to the contralateral side, inserted into the field, and secured with a clear sterile adhesive dressing before starting the procedure.
Creating a working space
A 5- to 6-cm vertical skin incision is made along the lateral border of the pectoralis major muscle in the axilla, and a subplatysmal skin flap to the anterior neck area is made over the anterior surface of the pectoralis major muscle and clavicle. After exposing the SCM, the dissection is approached through the avascular space between the two heads of the SCM. The dissection plane of this avascular space enables the surgeon to preserve the sensory nerves to the anterior neck, and thus postoperative hypoesthesia of this region can be minimized. The carotid sheath is dissected down and away from the posterolateral border of the strap muscles taking care not to injure the internal jugular vein (IJV) or the common carotid artery. The omohyoid muscle is pushed superiorly. Further dissection proceeds in the space between the strap muscles and the thyroid gland, and is continued until the upper pole of the thyroid gland and medial one third of the contralateral lobe are exposed. An external retractor (Chung retractor or a comparable product) is then inserted through the axillary skin incision and elevated to expose the working field. Chung's retractor can be connected to continuous suction by a built in tube running down the midline of the retractor blade. To achieve an adequate working space, the incision should be large enough to provide a height of more than 4 cm and the retractor blade should be more than 1 cm from the anterior surface of the thyroid gland (12).
Docking and instrumentation
Previously, Chung and colleagues (20) described a novel method of robotic thyroidectomy using a gasless, transaxillary approach utilizing two skin incisions: an axillary incision for the camera, 1st, and 2nd robotic arm, and a small anterior chest wall incision for the 3rd robotic arm. However, according to the procedure described here, all four robotic arms are inserted through a single axillary incision. To prevent interference between the robotic arms, we offer several tips and rules about where to place the ProGrasp forceps and how to introduce the robotic arms at appropriate angles and interarm distances.
For the right-sided approach, a 12-mm trocar for the camera and a 30° dual-channel endoscope are positioned at the center of the axillary incision. The camera is inserted at an upward angle (the external 3rd joint should be placed in the lowest part, that is, floor, of the incision entrance and the camera tip should be directed upward). An 8-mm trocar for the ProGrasp forceps is then positioned to the right of the camera, parallel with the built in suction tubing on the Chung retractor blade. At this point, the ProGrasp forceps must be located as close as possible to the ceiling of the working space (under the retractor blade) (Fig. 4). In contrast with motion of the ProGrasp forceps in two-incision transaxillary robotic thyroidectomy (9), endowrist motion of the forceps is only used to hold the thyroid tissue and its external joint should be moved as little as possible to prevent collisions of the four robotic arms in a single-incision approach (12). It is also recommended to prevent collisions so that the 3rd joint of the robotic arm, which is holding the ProGrasp forceps is pulled maximally out of the axillary skin incision, and the tip of the ProGrasp forceps maximally slides into the working space (12). Consequently, the 3rd joint of the Prograsp forceps is located in a different plane than those of the other three robotic arms, which enable the ProGrasp forceps to secure the adequate working space and prevent external clash. The 5-mm trocar of a Maryland dissector is then positioned to the left of the camera (at the left edge of the incision), and the 5-mm trocar for the harmonic curved shears to the right side of the camera (at the right edge of the incision). Instruments should be as far apart as possible (Fig. 4).
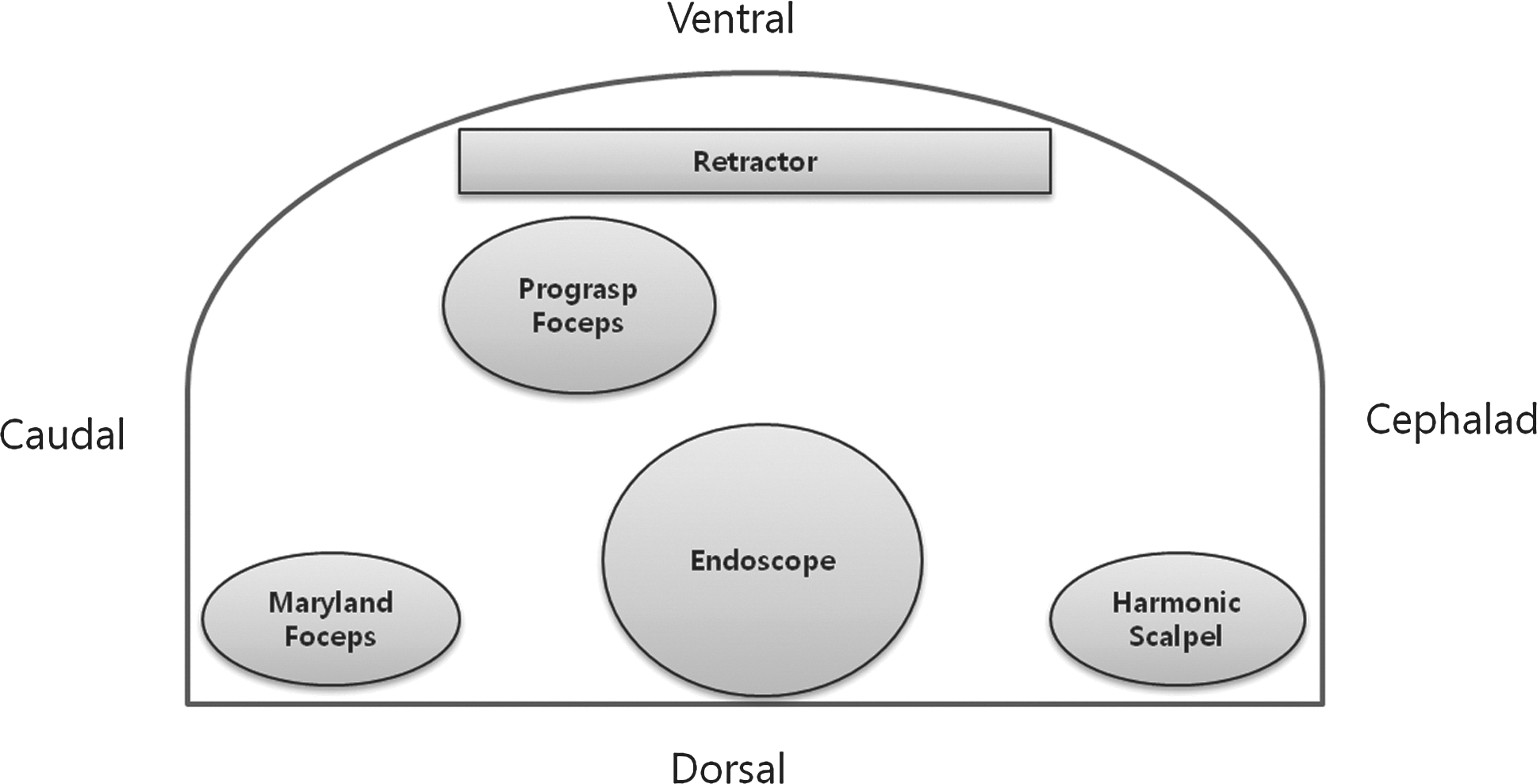
All the robotic instruments are introduced through the axillary skin incision.
Performing the ipsilateral lobectomy
Once access to the thyroid gland is obtained, the operation proceeds in a very similar fashion to conventional open thyroidectomy. However, in robotic thyroidectomy, the two robotic arms holding the endoscopic camera and the ProGrasp forceps replace the surgical assistant used in the conventional method. This enhances the surgeon's control because he always has a steady operative view and a tremor-free retraction as compared to the conventional open approach. All vessel ligation during the entire procedure is performed using the harmonic scalpel.
In robotic thyroidectomy, the surgeon uses three arms during the operation, which enables dissection of the thyroid tissue by traction and counter-traction maneuvers that is similar to the basic dissection technique in conventional open thyroidectomy. Traction and counter-traction can be also enhanced by the robot function of swapping arms between the ProGrasp forceps and the Maryland dissector. Frequent swapping of the arms can be helpful to maximize the effect of traction and counter-traction, and to obtain optimal dissection planes. The ProGrasp forceps and the Maryland dissector play the role of traction and counter-traction of the thyroid tissue, and the harmonic curved shears takes charge of dividing the vessels and tissue.
Under endoscopic guidance, the upper pole of the thyroid is retracted in the inferomedial direction with the ProGrasp forceps. The superior thyroid vessels are identified and divided individually close to the thyroid gland to avoid injury to the external branch of the superior laryngeal nerve (EBSLN) by use of the harmonic curved shears. The superior parathyroid gland is identified during the dissection and preserved. The lower pole is dissected from the adipose and cervical thymic tissue. The inferior thyroid artery is divided close to the thyroid gland to avoid injuring the inferior parathyroid glands or their blood supply. The thyroid gland then is retracted medially with the ProGrasp forceps, and the perithyroidal fascia is divided and sharply dissected using the harmonic curved shears and the Maryland dissector. Careful dissection is then performed to identify the inferior thyroid artery and the recurrent laryngeal nerve (RLN) in their usual anatomic relationship. The inferior thyroid artery is divided close to the thyroid gland using the harmonic curved shears, and the entire cervical course of the RLN is dissected. The thyroid gland then is dissected off the trachea to the midline and divided using the harmonic shears. In cases of thyroid cancer, central compartment node dissection (CCND) is performed after superior pole dissection. The RLN should be identified before undertaking the central lymph node dissection. Because the anterior surface of the carotid sheath is already dissected just below the strap muscles during creation of a working space, the surgeon can easily perform a complete ipsilateral CCND from the carotid artery to the substernal notch and the prelaryngeal area.
Performing the contralateral lobectomy
Approaching the contralateral thyroid lobe using this method can be more difficult because the contralateral nerve can be difficult to visualize. However, this drawback can be overcome with the ergonomically designed robotic system and sufficient experience. This surgical robotic system provides a 3D field of view and magnifies the target structure enabling the surgeon to perceive depth and space in the operative field more accurately. The use of a 30° scope also enhances visualization by peering over the trachea and downward to the recurrent nerve. Therefore, during dissection of the contralateral lobe of the thyroid gland, these images allow the surgeon to appreciate the 3D structures of the upper pole and of the ligament of Berry, and consequently perform sharp, precise endoscopic subcapsular dissections to preserve the contralateral recurrent and superior laryngeal nerve and the contralateral superior and inferior parathyroid glands.
Another advantage of the robotic system in performing contralateral lobectomy is that wristed instrumentation can be moved with 7° of freedom, which mimic that of the human wrist and fingers. The snake-like motion of the Maryland dissector and the availability of multi-jointed ProGrasp forceps allow surgeons to easily reach blind spots that normally cannot be reached with conventional endoscopic instruments.
Contralateral thyroidectomy is performed in a similar way as ipsilateral lobectomy. First, the cut isthmus of the contralateral lobe is drawn ventrally by the ProGrasp forceps and dissection is performed between the posterior aspect of the thyroid and the trachea using the Maryland forceps and harmonic shears (Fig. 5A). Then, the contralateral superior pole is retracted infero-medially with the ProGrasp forceps and transected using the harmonic shears (Fig. 5B). The inferior pole of the thyroid is also dissected subcapsularly to preserve the contralateral RLN and inferior parathyroid gland (Fig. 5C). After mobilization of the contralateral thyroid gland by dividing the superior and inferior pole, the posteromedial aspect of the contralateral lobe is only attached to the side of the cricoid cartilage by the posterior suspensory ligament of Berry. Because the contralateral RLN can be most consistently identified at the cricoid cartilage and is most vulnerable for injury in the vicinity of the ligament of Berry, special care should be taken to identify the contralateral RNL using the Maryland forceps (Fig. 5D). In some cases, to achieve better exposure of the contralateral tracheo-esophageal groove, the operating table can be tilted to 10–15° (contralateral side up).
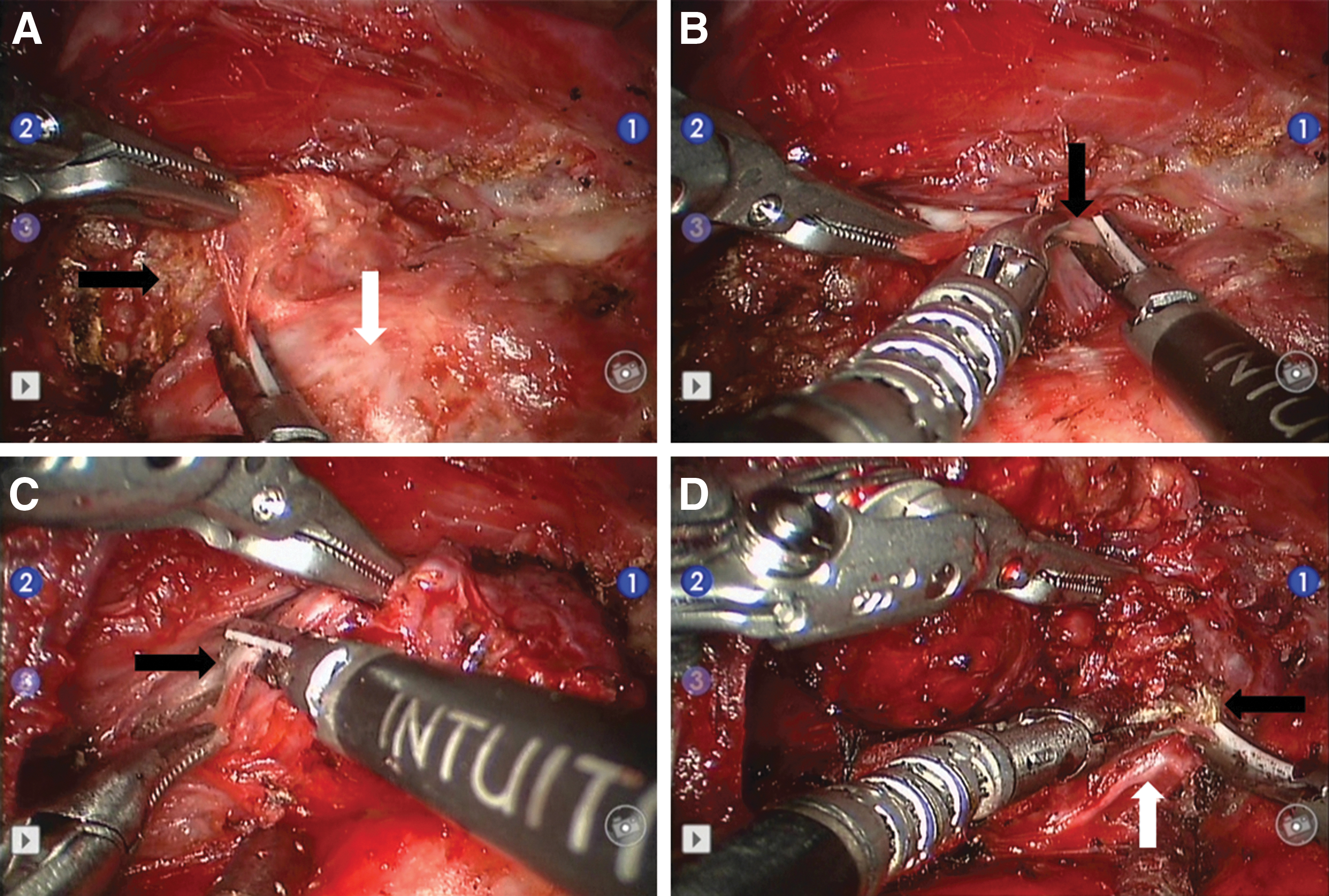
Robotic thyroidectomy of removing the contralateral lobe (right lobe) in left transaxillary approach.
Once the contralateral RLN has been identified and preserved, the contralateral thyroid lobe can be removed from its tracheal attachments by dividing the ligament of Berry.
Drain insertion and skin closure
Closed suction drainage after robotic thyroidectomy cannot replace good hemostasis and is of little benefit if severe postoperative bleeding occurs. After hemostasis is performed, a drain can be useful to remove a small hematoma and prevent seroma formation. Many groups favor routine drain insertion, however, at the Mount Sinai Endocrine Surgery program, closed suction drainage is used infrequently. The skin may be closed by subcuticular suture or by the surgeon's preferred method.
Prevention and Management of Complications
Skin flap injury
During the procedure of creating a working space in the gasless transaxillary procedure, the clavicle is the boundary between the anterior chest wall and neck and serves as the entrance to the neck. Because the skin over the clavicle is very thin with less fat and has indentation formed by the clavicle in nature, a meticulous dissection should be carried out taking special care not to perforate the skin or cause a subdermal burn over the clavicle by electrocautery.
Injury to the RLN
RLN injury is one of the most serious complications of thyroid surgery. It often leads to significant morbidity and frequent malpractice lawsuits (21). The current policy of visual identification of the RLN tracing the whole cervical course is the gold standard to reduce the risk of permanent RLN injury. Endocrine surgeons should be aware of the anatomic variability of the RLN. In instances of embryologic malformation of the aortic arch with a retroesophageal right subclavian artery, the nerve passes directly to the larynx branching off of the vagus in the carotid sheath (nonrecurrent laryngeal nerve). Although the reported incidence of the nonrecurrent laryngeal nerve is less than 1%, the surgeon performing a thyroidectomy, especially on the right should always bear in mind the possibility of a nonrecurrent laryngeal nerve.
Permanent RLN injury is very rare in robotic thyroidectomy if performed by an experienced surgeon, because visualization of these vital structures might actually be easier with the excellent magnification of the robotic camera, even though the nerve cannot be palpated directly as in conventional open thyroidectomy. Intraoperative electrical nerve stimulation in the surgical field in addition to visualization of the RLN can be used to delineate the presence, function, and the course of the RLN (22 –24).
Damage to the RLN may be caused by different mechanisms: cutting, clamping, or stretching of the nerve, nerve skeletonization, local compression of the nerve due to edema or hematoma, or thermal injury by electrocoagulation or harmonic scalpel. In a series of transaxillary robotic thyroidectomy, it was demonstrated that the rate of temporary RLN palsy is 4.2% (13). This incidence is in the comparable range compared with 2% transient palsy in the conventional thyroidectomy group (25).
It is necessary to be cautious when using the harmonic scalpel when the nerve is in close proximity because there is a potential collateral transfer of energy that may result in its injury. It is recommended that the RLN should not be touched directly with the blade just after it has been used, and that it is preferable to use the ultrasonic surgical devices at a distance of 3 mm from the RLN for less than 20 seconds at a high-power level (100 μm vibration) (26). To maintain these distances, the RLN must be endoscopically visualized during the robotic procedure.
When function of the RLN is not recovered within 6–12 months postoperatively, permanent damage to the RLN should be considered. If inadvertent cutting or clamping the RLN is encountered intraoperatively, primary repair of the nerve using microsurgical techniques and epineural sutures or a reinnervation from the ansa cervicalis nerve can be attempted (27). Even if the nerve is reanastomosed, the dysfunctional vocal cord will not completely recover though there may be an improvement in vocal cord tone (28,29).
Injection laryngoplasty is a good treatment option for unilateral permanent RNL palsy patients after remote robotic thyroidectomy. One advantage is that it does not require an external skin incision on the neck (30).
When creating a working space in gasless robotic transaxillary thyroidectomy, a beginning surgeon unfamiliar with the new anatomy may incorrectly dissect the carotid sheath and strap muscles leading to accidental injury to the vagus nerve or RLN (10). Therefore, surgeons should be well-acquainted with the anatomic location between SCM, strap muscles, and the thyroid gland.
Bilateral RLN injury is the most serious complication of thyroid surgery resulting in near midline position of the vocal cords and airway obstruction. As its rate has been reported to be 0.4% in conventional total thyroidectomy (25), it is also a possibility in transaxillary robotic total thyroidectomy. Importantly, because the procedure is conducted through only one axilla and the contralateral nerve can be difficult to visualize, it may have the risk of bilateral RLN palsy. The use of nerve monitoring may also decrease the incidence of bilateral RLN palsy, because if the signal is lost in an ipsilateral nerve, the contralateral dissection can be staged.
If bilateral RLN injury is not observed intraoperatively, it may be diagnosed immediately after extubation or during the early postoperative phase. The patient should be reintubated without delay and treated systemically with corticosteroids. In the presence of reversible nerve injury, extubation under controlled conditions may be possible in most cases after 24–72 hours with no further treatment. In case of persistent respiratory obstruction, reintubation must be carried out immediately and tracheostomy is indicated. If the vocal cords fail to recover after a waiting period of 9–12 months, permanent tracheostomy or transverse laser cordotomy can be considered (31).
Injury to the EBSLN
Because injury to the EBSLN manifests less severe symptoms than injury to the RLN, this complication is less easily recognized and difficult to assess (32).
The most accurate test for postoperative assessment of superior laryngeal nerve palsy is laryngeal electromyography. The superior laryngeal nerve, like the RLN, originates from the main trunk of the vagus nerve distal to the jugular foramen. It passes anteromedially over the thyroid membrane, where it is joined by the superior thyroid artery and vein. At about the level of the hyoid bone, it divides into two branches. The external laryngeal nerve innervates the cricothyroid muscle, whereas the internal branch provides sensory innervation to the supraglottic larynx. The internal laryngeal nerve separates into three branches that communicate with the RLN posterior to the cricoid cartilage. Injuries to the internal branch are rare during thyroid or parathyroid surgery.
Cernea's classification for the course of the EBSLN is widely accepted (33,34). A Cernea type 1 nerve crosses medially into the cricothyroid muscle more than 1 cm cephalad to the upper pole of the thyroid lobe; it occurs in about two thirds of cases. A Cernea type 2a EBSLN remains cephalad to the upper pole of the thyroid gland. A Cernea type 2b EBSLN is in the most caudal position of all variants laying below the upper pole of the thyroid gland—it occurs in 20% of cases. The Cernea type 2a variant poses an increased risk of injury during the dissection and ligation of the superior thyroid pedicle.
To avoid damage during ligation of the superior thyroid pedicle, the vessels of the upper pole should be dissected individually and be ligated as caudally as possible on the surface of the thyroid. In addition, the harmonic scalpel and electrocautery should not be activated directly on the cricothyroid muscle, and the cricothyroid muscle should be preserved intact whenever possible.
Since the cricothyroid muscle is a tensor of the vocal cord, injury to the EBSLN often results in voice weakness, loss of voice range and pitch control, and inability to perform high-pitch phonation. Especially in singers, injury to this nerve is a serious and a possible career-ending problem.
Hypoparathyroidism
Although the pathogenesis of post-thyroidectomy hypocalcemia is multifactorial, damage to the parathyroid glands in the form of direct injury, unrecognized inadvertent removal, or indirectly by devascularization of the gland are the most common causes. For these reasons, it is essential for preventing hypoparathyroidism that the surgeon should understand the anatomic variation of the parathyroid glands and identify the parathyroid glands during surgery.
The superior parathyroid glands are usually located more lateral and posterior to the RLN at the level of Berry's ligament and are usually the easiest to preserve during robotic thyroidectomy. The inferior parathyroid glands are almost always located anterior to the RLN and caudal to where the RLN crosses the inferior thyroid artery. The criteria that help differentiate the parathyroid glands are: (i) position; (ii) mobility independent of the thyroid gland; (iii) brownish color; (iv) smooth, finely granular surface; (v) presence of vascular pedicle; (vi) bleed easily on manipulation; (vii) the presence of a small fatty hood.
In conventional thyroidectomy, permanent hypoparathyroidism resulting in lifetime disability occurs in less than 1% of patients (35,36), whereas transient postoperative hypocalcemia, which resolves within 6 months after surgery, is much more common with a range of 4%–42% (37 –39). In a study of 1000 patients with thyroid cancer who underwent gasless transaxillary robotic thyroidectomy, transient and permanent hypoparathyroidism occurred in 38.8% and 0%, respectively (13). Based on this series, there is no evidence that robotic thyroidectomy has an increased incidence of permanent hypoparathyroidism. Even though transient hypocalcemia is the most common complication, it would seem that magnification by the robotic camera is rather helpful to identify the parathyroid glands. In addition, it should be pointed out that hypoparathyroidism is associated with thermal injury of the harmonic scalpel in robotic thyroidectomy (40). Therefore, it is recommended that the inactive blade be nearest to the parathyroid gland during cutting and coagulation.
If safe dissection of a parathyroid gland is technically not feasible or its viability has been compromised, the gland should be removed, cut into small fragments, and implanted into a muscle pocket in the pectoralis major muscle.
Bleeding
Thyroid surgeons have always been concerned with bleeding and hemostasis, since hematoma formation may have devastating consequences. Like all areas of surgery, meticulous hemostasis is critical in thyroid surgery because a small amount of bleeding can often obscure the operative field, making surgery more hazardous. Intraoperative bleeding can obscure structures, increasing the possibility of injury to the RLN and the parathyroid glands because of tissue staining, making identification more difficult.
While creating the working space, injury to external jugular vein (EJV) may occur. The EJV crosses the SCM muscle obliquely in the direction of a line drawn from the angle of the mandible to the middle of the clavicle at the posterior border of the SCM muscle. If the subplatysmal flap dissection to expose the avascular space between the two heads of the SCM muscle is oriented too widely in the direction of posterior neck, the surgeon may encounter the EJV. In case of EJV injury, the EJV can be ligated without any adverse effects.
After dissection of the working space the dissection proceeds through the avascular space between the two heads of the SCM muscle, the carotid sheath is separated down from the strap muscle, and then the IJV is exposed. If IJV injury were to occur during the robotic procedure, robot-assisted primary repair could be taken into consideration, as the ProGrasp forceps securely hold the injured portion of the IJV. In the case of a small tear of the IJV or of a branch, the bleeding can be controlled by application of an endoscopic hemostatic clip that the field surgeon at the bedside can easily perform under endoscopic visualization.
Hematoma formation after thyroid surgery is of particular concern as it may lead to life-threatening airway obstruction. This is due to the rapid rise in pressure within a closed space, with subsequent laryngeal edema and tracheal compression.
Postoperative bleeding is characterized by respiratory distress, pain, cervical pressure, dysphagia, and increased blood drainage. Perioperative bleeding may be decreased by having the patient in a reverse Trendelenburg position, with the head elevated 20°. If the surgeon is uncertain about the dryness of the operative field, a Valsalva maneuver, which elevates the intrapulmonary pressure to 40 cm H2O and facilitates recognition of bleeding vessels, can be performed by the anesthetist before wound closure. Postoperatively, patients should be placed in a low Fowler position with the head and shoulders elevated 10–20° to keep a negative pressure in the veins.
Symptomatic hemorrhage with evident tracheal compression occurs between 4 and 6 hours after the initial operation majority of the time (41). Since in ∼20% of cases the onset of hematoma symptoms is reported beyond 24 hours postoperatively, surgeons should warn patients who undergo ambulatory surgery of the risk of delayed bleeding (42). Although the incidence of symptomatic hemorrhage requiring reoperation amounts to 0.1%–1.5% in conventional thyroidectomy (25,37,41 –43), its incidence in transaxillary robotic thyroidectomy is very low and is reported to be 0.1% until now (16). In a study of 581 patients who underwent gasless transaxillary endoscopic thyroidectomy, chest wall hematomas, which originated from a tiny bleeder in the anterior surface of strap muscle and pectoralis major muscle occurred in 0.6% of the patients (44). These chest wall hematomas were easily controlled and evacuated at the bedside without difficulty. Because gasless transaxillary robotic thyroidectomy requires a wide operative space, through which intraoperative and postoperative bleeding may track, major hematoma formation confined to the thyroid bed with airway compression rarely occurs.
On the contrary, axillary and bilateral axillo-breast approach with gas insufflation has encountered conversion to open surgery due to intraoperative bleeding (45,46). This implies that a small amount of bleeding not only can obscure the operative field, but make the operation more difficult in the gas-utilizing approach. Moreover, a smaller hematoma may lead to a life-threatening airway obstruction due to a small operative space.
In case of significant respiratory distress emergency, bedside hematoma evacuation, if necessary in combination with endotracheal intubation, is required. The requirement for tracheotomy either in the emergency setting or due to persisting airway obstruction after hematoma removal is generally a rare event.
Tracheal injury
The prevalence of tracheal injury requiring primary repair of the tracheal wall amounts to 0.3% (16). Because tracheal injury in robotic thyroidectomy is mainly due to thermal injury by the harmonic scalpel, the surgeon should be cautious that the active blade does not directly touch the tracheal wall during cutting and coagulation. Tracheal injury can be managed by the robot-assisted primary suture (18). An air-leak test must be performed to confirm a secure closure before extubation.
Brachial plexus injury
In the reports by Chung and colleagues (10,12), the arm was extended in the superior direction to provide the shortest distance from the axilla to the anterior neck. However, this straight extension of the arm may cause inadvertent hyperextension and rarely results in transient brachial plexus palsy (18). Traditionally, brachial plexus injury has occurred after abdominal operations with the patient positioned on the operating table with the arm restrained on a board in abduction, external rotation, and extension (47 –49). Brachial plexus injury is often regarded as a stretch-induced neuropathy (50) due to malposition. Onset of symptoms is characterized by paresthesias and weakness, pain not being a prominent sign. The recovery typically starts 2–3 weeks later, with a gradual recovery of sensation, followed by lower and upper plexus strength recovery after conservative treatment (47). Kuppersmith modified the arm positioning so that the arm is extended at the shoulder, and then flexed at the elbow, after he encountered complications related to positioning (51). Especially in patients with limited motion of the shoulder or elbow joint, modified arm position should be considered. Therefore, it is recommended that the arm should be best positioned in the natural extension position to avoid stress or stretch on the nerves (Fig. 3). It is essential to place adequate padding around bony prominences on the arm, under the neck, shoulder, and small of the back to prevent skin ulceration due to position pressure. With awareness of risk factors which are likely to cause injury to the brachial plexus, careful positioning of the upper extremity can prevent injury and potential disability to the patient.
Seroma
Among the remote approach methods, the most common associated with seroma formation is the gasless transaxillary endoscopic thyroidectomy. This method is more invasive and needs more operative time than the conventional transcervical approach due to the wide dissection from the axilla to the anterior neck area. For this reason, chest wall seroma has occurred in 2% of patients (16). Seromas generally resolve with repeated needle aspiration, compression dressings on the chest wall, and the tincture of time.
Conclusion
Transaxillary single-incision robotic thyroidectomy can be performed safely and offers numerous advantages over other types of robotic thyroidectomy as well as conventional open thyroidectomy. A good understanding of possible complications (Table 1) and how to prevent them will help maximize patient safety.
RLN, recurrent laryngeal nerve.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.