
Abstract
Background:
Ectopic thyroid tissue (ETT) is a rare embryological abnormality characterized by the occurrence of thyroid tissue in a site other than its usual location. Thyroid hemiagenesis (HA) is also a very rare abnormality in which one thyroid lobe does not develop properly during embryology. We report a patient with left HA, submandibular ETT, and persistent mildly suppressed serum thyrotropin (TSH).
Patient:
A 38-year-old female patient was admitted with complaints of sweating and palpitations. She had no symptoms of neck compression. Thyroid ultrasonography revealed heterogeneity and hypoechogenicity of the right lobe and absence of the left lobe, the latter being confirmed by computed tomography. There was no ETT in the neck. A thyroid Tc-99m pertechnetate scan demonstrated two distinct areas of radiotracer uptake, one in the right lobe of the thyroid gland and one in the right submandibular region and lobe, but no uptake in the left thyroid bed. The serum free triiodothyronine was 2.89 pg/mL (2.5–3.9 pg/mL), and the serum free thyroxine was 0.86 ng/dL (0.61–1.12 ng/mL). The serum TSH was 0.11 mIU/L (0.34–5.60 mIU/L).
Conclusions:
This may be the first reported patient with HA and submandibular ETT. The patient probably also had thyroiditis with mild intermittent thyrotoxicosis based on her suppressed TSH and ultrasonography imaging of the right thyroid lobe.
Introduction
Patient
A 38-year-old woman was admitted to the outpatient clinic with the complaints of sweating and palpitations for 3 months. There was no hoarseness, dyspnea, or dysphagia. She had no symptoms of thyrotoxicosis except sweating and palpitation. No palpable masses or other abnormalities were noted during neck examination. The serum free triiodothyronine (fT3) was 2.89 pg/mL (2.5–3.9 pg/mL), and free thyroxine (fT4) was 0.86 ng/dL (0.61–1.12 ng/mL). The serum thyrotropin (TSH) was 0.11 mIU/L (0.34–5.60 mIU/L). Tests for serum antibodies against thyroglobulin (anti-TG) and thyroid peroxidase (anti-TPO) were negative, and the test for antibodies against the TSH receptor was negative with the value being 0.13 IU/L (0–1 IU/L). An electrocardiogram revealed sinus tachycardia with a pulse rate of 103 beats/min. Thyroid ultrasonography revealed absence of the left thyroid lobe and heterogeneity and hypoechogenicity in the right thyroid lobe consistent with thyroiditis. Computed tomography (CT) of the neck confirmed absence of the left thyroid lobe (Fig. 1). Next, thyroid scintigraphy (TS) using Tc-99m pertechnetate was performed. This showed absence of uptake in the region where the left lobe of the thyroid should have been and uptake in the right submandibular region (Figs. 2 and 3). The patient was followed for 6 months on no medications, at which time thyroid function tests were repeated. The serum fT3 was 2.93 pg/mL (2.5–3.9 pg/mL); the fT4 was 0.88 ng/mL (0.61–1.12 ng/mL), and the TSH was 0.20 mIU/L.

The arrow indicates the right thyroid lobe on computed tomography.
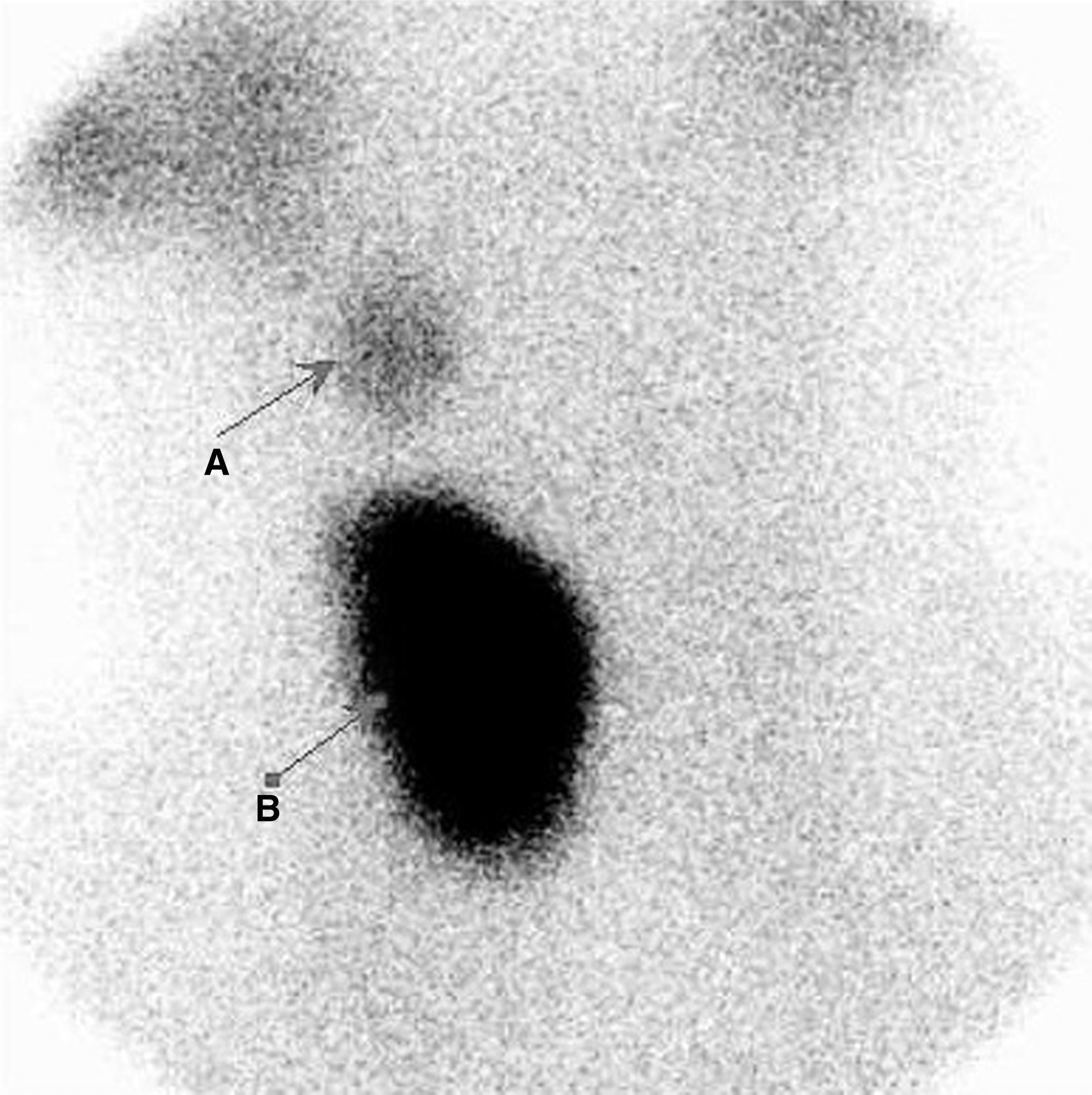
Tc-99m pertechnetate thyroid scan shows left thyroid hemiagenesis and right submandibular ectopic thyroid tissue:
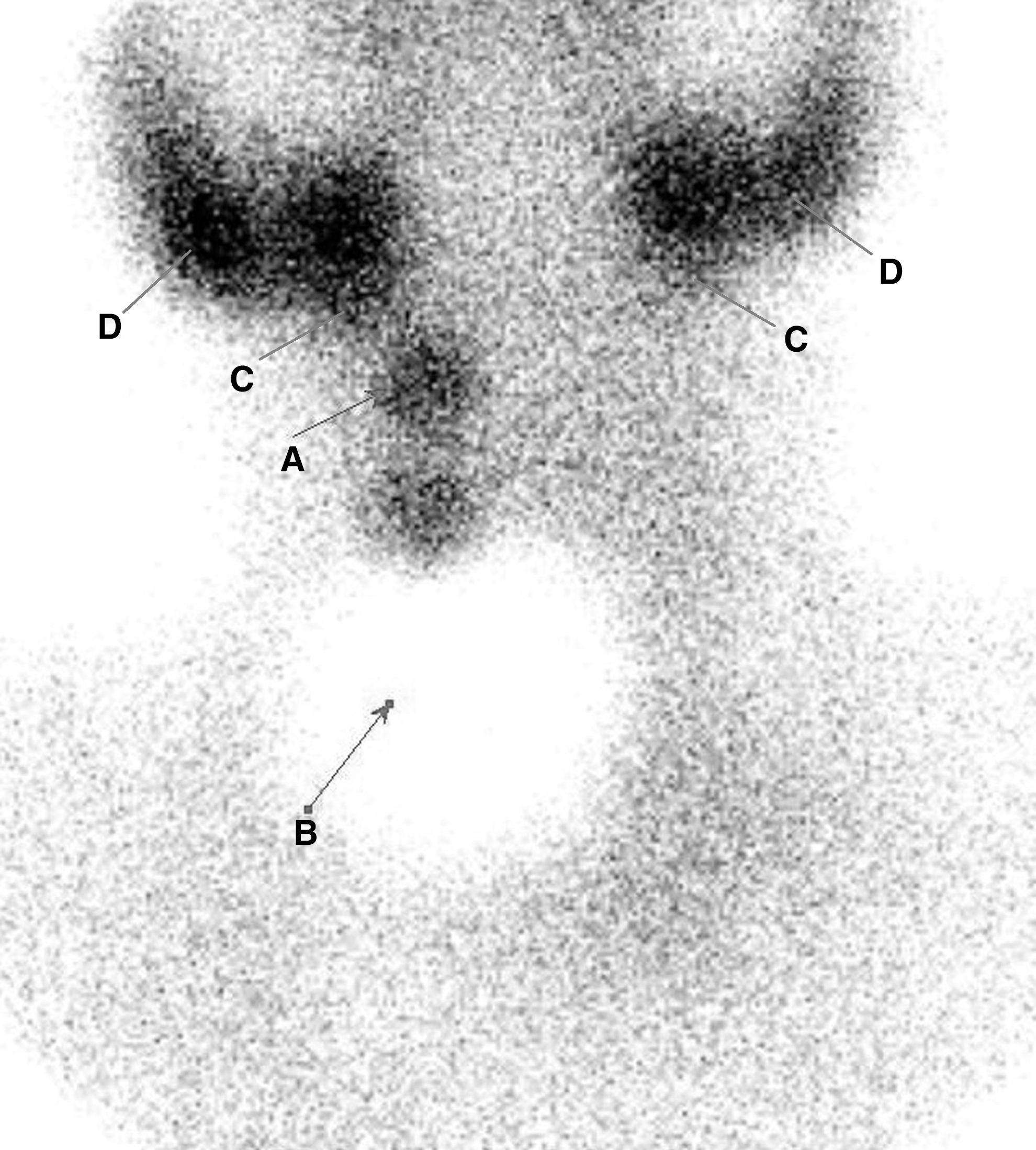
Tc-99m pertechnetate thyroid scan. Ectopic thyroid tissue becomes better visualized after the coverage of two-thirds of the thyroid by a lead layer.
Discussion
A median epithelial proliferation at the base of tongue, the foramen caecum, forms the thyroid anlage during embryonal development (5). The thyroid gland, as a bilobed diverticulum, migrates inferiorly to the anterior pharyngeal gut, but remains connected to the pharyngeal floor via the thyroglossal duct (6). As the gland descends, atrophy of the thyroglossal duct occurs, and eventually, the duct disappears (7). The gland moves anterior of the hyoid bone and laryngeal cartilages, arriving by the seventh gestational week at its ultimate location, anterior to the trachea (5 –7).
Congenital anomalies of the gland are divided into three categories. These are (i) developmental deficiency of the gland (agenesis or hemiagenesis), (ii) ectopic thyroid gland as a result of migration failure, and (iii) thyroglossal duct cyst as a result of persistence of the thyroglossal duct (8).
The prevalence of HA ranges between 0.05% and 0.2% (9). The frequency of hemiagenesis of the left lobe is 80%, and the absence of the isthmus is found in 50%. The prevalence of HA is greater in women than in men (75% vs. 25%) (9,10).
HA is usually asymptomatic. The diagnosis is often made when the patient presents with other thyroid conditions, such as Graves' disease, subacute thyroiditis, simple goiter, a colloidal nodule, Hashimoto's thyroiditis, or thyroid carcinoma (11,12). Our patient presented with symptoms of mild thyrotoxicosis, and she had a persistently suppressed serum TSH with normal fT3 and fT4 values. She was not taking thyroid hormone, and she had negative tests for anti-TG, anti-TPO, and TSH receptor antibodies. She did not have signs of Graves' orbitopathy. Her thyroid ultrasonography was consistent with thyroiditis of the right lobe. Therefore, with this ultrasound finding and the suppressed TSH, we believe that she had mild thyroiditis.
The vast majority of ETT is in the sublingual region (90%) (13). ETT has also been located in the high cervical area, the intratracheal and esophageal areas, lung, heart, and even in the duodenum. ETT lateral to the midline in the submandibular region is unusual (14).
The presence of ETT with HA is very rare. The three cases previously reported had the localization of ETT in the sublingual, lingual, and prelaryngeal regions. Only one of the cases had subclinical hypothyroidism; the other two patients exhibited normal thyroid function (Table 1) (15 –17). Therefore, the present case appears to be unique in the literature.
The patient was a newborn.
F, female.
A lateral location of ETT is difficult to explain. Radkowski et al. suggested that thyroid tissue could be displaced from the midline as a result of previous inflammation (18). Most patients with ETT are asymptomatic if they have sufficient normal thyroid tissue. Treatment of ETT may be required in the case of malignant disease or for cosmetic reasons. Surgical excision of the ETT is rarely necessary, but may be required in cases where there is noticeable swelling causing pressure symptoms, or if there is malignancy.
CT of the neck may detect HA and may also detect ETT. In our patient, CT revealed left HA, but we did not detect ETT with this imaging modality. The very small volume of our patient's ETT may explain this. TS is a highly sensitive and specific method for detecting normal thyroid tissue and ETT (5,19). It can distinguish tongue and neck ETT from other entities such as thyroglossal duct cyst, lipoma, enlarged lymph node, epidermoid cyst, vascular malformation, mucous retention cyst, and malignant tumors. The salivary glands (submandibular and parotid) concentrate Tc-99m during TS, and this may cause a misdiagnosis of ETT. However, in contrast to ETT, the tracer accumulation in the salivary glands is bilateral (20). In our case, the TS clearly revealed bilateral parotid and submandibular glands, and unilateral ETT (Fig. 2).
In conclusion, we report what appears to be the first patient with HA and ETT in the submandibular region. The patient was also unusual because of probable thyroiditis in her only thyroid lobe. Disturbance of her thyroid function would probably have been greater if she had a normally formed thyroid gland.
Footnotes
Disclosure Statement
The authors warrant that there is no conflict of interest.