
Abstract
Background:
Traumatic neuroma may be easily confused with recurrent lymphadenopathy in the neck, causing patient anxiety, need for fine-needle aspiration (FNA), and even surgery. The purpose of this study was to evaluate the ultrasound (US) features that differentiate traumatic neuroma from recurrent lymphadenopathy after lateral neck dissection (LND), focusing on direct continuity with the involved nerve.
Methods:
This study compared US features of 56 traumatic neuromas in 36 consecutive patients, with 56 recurrent lymphadenopathies in 34 consecutive patients who had a previous history of total thyroidectomy and LND for thyroid cancer. Direct continuity of a nerve with a nodule and other US factors of a nodule (the short axis diameter, short-to-long axis ratio, location, shape, margin, echogenicity, vascular flow, hilar line, cystic portion, and echogenic dots) were evaluated in the two groups.
Results:
Traumatic neuromas after LND had a prevalence of 17.8% (36/202) on US. Direct continuity with the involved nerve was visible in 98.2% (55/56) of the traumatic neuromas. The involved nerves in these traumatic neuromas were either terminal type (4/55, 7.3%) or spindle type (51/55, 92.7%). The short axis diameters, short-to-long axis ratio, location, shape, margin, and echogenicity were significantly different (p<0.001) in these two groups. None of the traumatic neuromas had a hilar line, vascular flow, or cystic portion.
Conclusions:
Direct continuity with the cervical plexus may be a characteristic US feature of traumatic neuroma after LND. This feature, along with ancillary findings, may prevent unnecessary surgery as well as painful FNA.
Introduction
Traumatic neuroma has been reported to occur in 1.1%–2.7% of patients who undergo neck dissection (8 –10). Although painful hypersensitivity or paresthesia is a characteristic symptom of traumatic neuroma, some patients are asymptomatic. Traumatic neuromas may therefore be easily confused with recurrent lymphadenopathy, causing patient anxiety and the need for fine-needle aspiration (FNA) (8 –10). Since FNA results may be nondiagnostic, some patients require surgical excision for a confirmative diagnosis (11,12). Unnecessary surgery and/or FNA can be avoided by an accurate ultrasound (US) diagnosis of traumatic neuroma (4 –6,8,9).
US examination of traumatic neuromas occurring after knee amputation has demonstrated that an echogenic nerve running into the mass is characteristic (1,2). In the neck, US features distinguishing traumatic neuroma from recurrent lymphadenopathy often include a central hyperechoic area, a smaller short axis diameter, and a smaller short-to-long axis ratio, or an isoechoic mass with internal parallel heterogeneous hyperechogenicity. To date, however, direct continuity of a neck nerve with a traumatic neuroma has not been reported, perhaps due to the small sizes of transected nerves in the neck (8,9). Recently, however, we described a patient who developed a traumatic neuroma after total thyroidectomy with modified radical neck dissection; on US examination, this neuroma showed direct continuity with the C4 nerve root (13).
Since traumatic neuromas in the neck usually arise from branches of the cervical plexus after neck dissection (8 –10), understanding the course of the cervical plexus and its related anatomy can allow the visualization of the direct continuity of the nerve with a traumatic neuroma. We therefore evaluated the US features differentiating traumatic neuroma from recurrent lymphadenopathy after total thyroidectomy with lateral neck dissection (LND). We focused on the ability of US to determine the direct continuity of the traumatic neuroma with the involved nerve. Differentiating between these two conditions may avoid unnecessary surgery and painful FNA experiences.
Materials and Methods
Patients
The protocol of this retrospective study was approved by our Institutional Review Board of the Asan Medical Center, which did not require patient approval or informed consent for review of images and medical records. However, all patients undergoing US examination and US-guided FNA provided written informed consent before each procedure. The decision to perform FNA on nodules in the dissected neck regions was based on the presence in the nodules of the following US criteria: an echogenic portion, cystic changes, echogenic dots, abnormal vascularity, round shape, loss of hilar line, and short axis diameter exceeding 6 mm (14 –19).
From January to April 2011, we examined 202 consecutive patients who were undergoing US of the neck after total thyroidectomy with LND due to thyroid cancer. We diagnosed 56 traumatic neuromas in 36 patients using the following criteria: (i) acute exacerbation of pain when the needle penetrated the nodule and relief of pain when the needle was removed from the nodule (n=56; Fig. 1), and (ii) cytohistologic confirmation of traumatic neuroma by FNA or core needle biopsy, with undetectable thyroglobulin (Tg) concentrations in FNA washout fluid (n=32) (8,9,12).
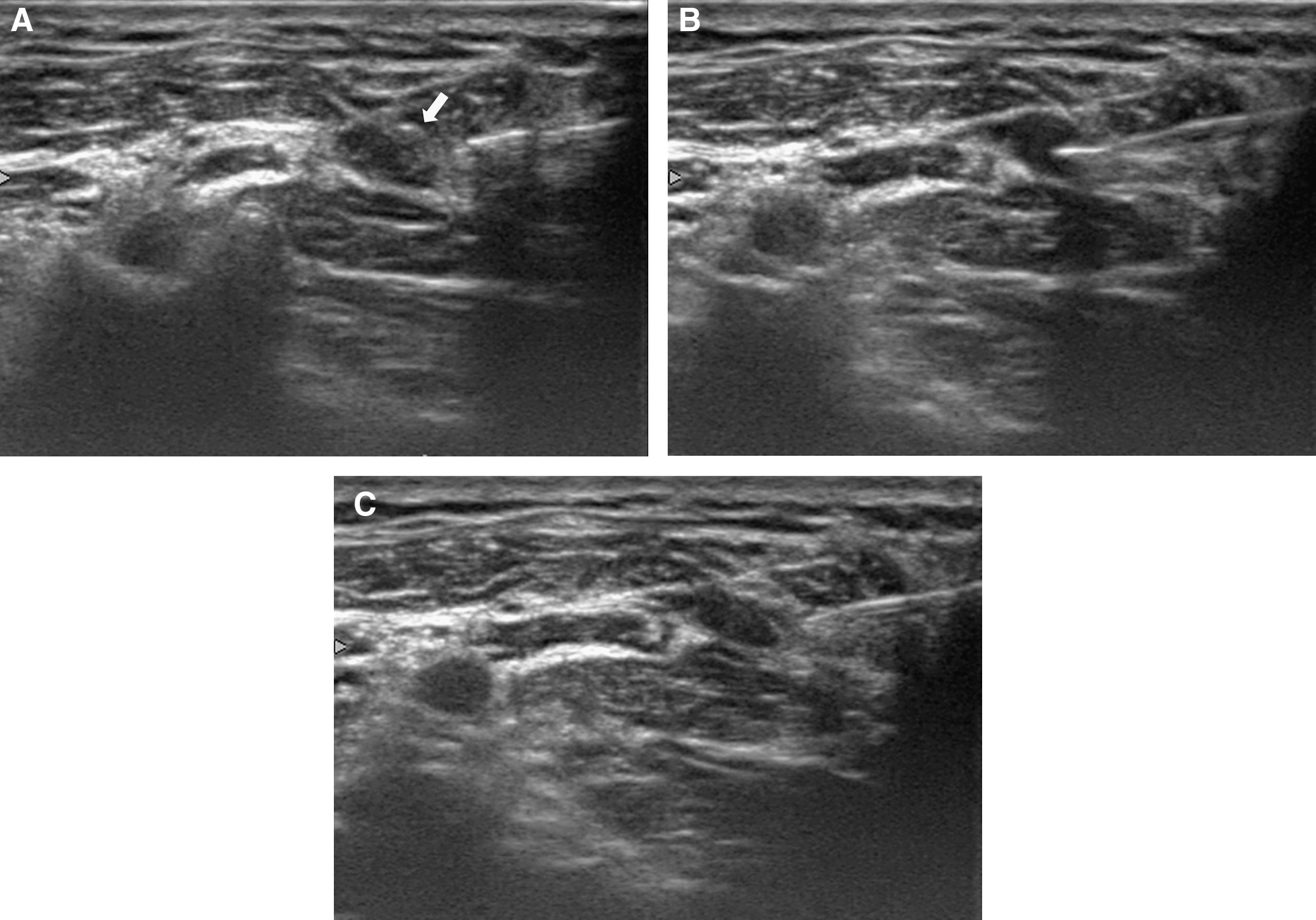
A 46-year-old woman with traumatic neuroma after left modified radical neck dissection for thyroid carcinoma.
During the same period, 10 recurrent lymphadenopathies were diagnosed by US-guided FNA and FNA-Tg in 6 of 202 consecutive patients who were undergoing US of the neck after total thyroidectomy with LND. Patients with recurrent lymphadenopathy in the central neck or at a nonoperated site were excluded. None of these patients complained of exacerbation of pain during the penetration of the nodule. For comparisons of recurrent lymphadenopathy with traumatic neuroma statistically, we retrospectively extended the chart review to the previous year. In the process, we found 56 recurrent lymphadenopathies in 34 patients between December 2009 and April 2011.
Clinical and demographic characteristics of the patients with traumatic neuroma and recurrent lymphadenopathy are summarized in Table 1. The intervals between LND and diagnosis were not significantly different in the two groups. Pain or paresthesia was noted in only four patients with traumatic neuroma.
Interval between lateral neck dissection and diagnosis.
Imaging and analysis
All US examinations were performed using one of three US systems, an iU22 unit (Philips Healthcare, Bothell, WA), an EUB-7500 (Hitachi Medical System, Tokyo, Japan), or an HDI-5000 (Philips Healthcare) equipped with a linear high-frequency probe (5–14 MHz). US examinations were performed by one of the two board-certified radiologists (B.J.H. or H.E.J. with 15 and 6 years of experience, respectively, in thyroid US).
The direct continuity of a nerve with a nodule was evaluated by real-time US. Based on the appearance of a nerve as a thin cord-like hypoechoic structure on US (5,20), we traced the nodule in several directions, and identified a continuous hypoechoic structure entering the nodule. Doppler US did not reveal blood flow in the immediate vicinity of this structure, which helped to differentiate it from small vascular structures. If the involved nerve was well visualized, its cervical level was determined by following it to the groove, between the anterior and posterior tubercles, of the transverse process. The transverse process of the C7 vertebra was used as an anatomic landmark to assess the cervical level (21,22). From the appearance of involved nerves on US, we categorized each as an injured nerve terminating in a traumatic neuroma with bulbous enlargement of the nerve end, or as a nondisrupted nerve passing through the traumatic neuroma with fusiform enlargement. We also assessed the diameters of the nodule and its location (zone 1, medial to the internal jugular vein [IJV] and zone 2, lateral to the IJV).
To evaluate basic US features, three US images of each nodule were selected and randomly and independently reviewed by two investigators (H.E.J. and K.Y.J. with 6 and 5 years of experience, respectively, in thyroid US). Disagreements were resolved by a third investigator (B.J.H.). The three investigators were blinded to each patient's clinical history, and cytohistologic and laboratory results. The basic US features of the nodules evaluated included shape, margins, echogenicity, vascular flow, hilar line, cystic portion, and echogenic dots. Shape was categorized as ovoid to round, fusiform, or taller than wide; margins as well-defined smooth, ill-defined, or spiculated; echogenicity as homogeneously hypoechoic (>90%), homogeneously hyperechoic (>90%), or a mixed pattern, with the latter subcategorized as intermingled, internal linear hypoechoic structures, or a focal hyperechoic pattern (10%–90%). Vascular flow was defined as none, hilar, peripheral, or mixed on power Doppler scan. Power Doppler scans were performed by using the standard equipment settings for thyroid glands. Doppler amplification was set to a level that normal thyroid tissue did not display any noise and just under the level that random noise appeared. Hilar line, cystic portion, and echogenic dots were classified as present or absent.
Statistical analysis
Statistical analysis was performed using a software package (SPSS, version 18.0 for Windows; SPSS, Chicago, IL). Differences in US characteristics of traumatic neuromas and recurrent lymphadenopathy were statistically compared using the chi-squared test or Fisher's exact test for categorical variables and the Mann–Whitney U test for quantitative variables. A significant difference was defined as p<0.05.
For each characteristic, interobserver agreement between the two investigators (H.E.J. and K.Y.J.) and intraobserver agreement (H.E.J.) (between the initial assessment and a second 2 weeks later) were assessed using Cohen's kappa analysis.
Results
Of the 202 patients, 36 patients (17.8%) had a total of 56 traumatic neuromas. Of these, 55 (98.2%) showed direct continuity of a nerve with a traumatic neuroma (Fig. 2 and Supplementary Video S1; available online at
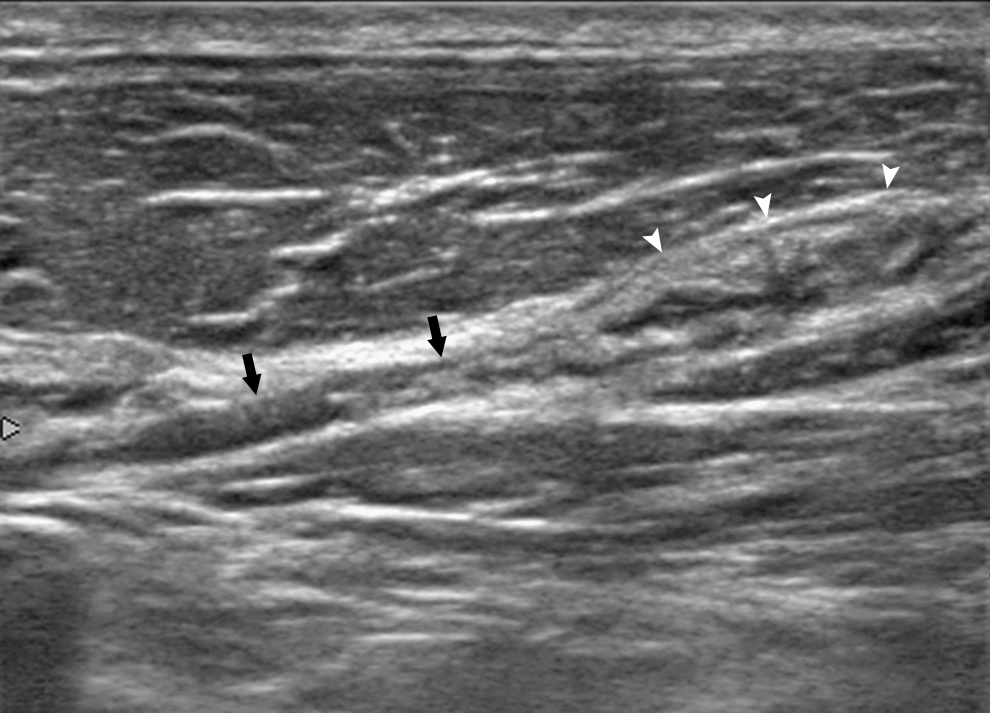
A 31-year-old woman with traumatic neuroma after left modified radical neck dissection for thyroid carcinoma. The direct continuity of the involved nerve (black arrows) with a nodule (white arrowheads) was visible. See also Supplementary Video S1.
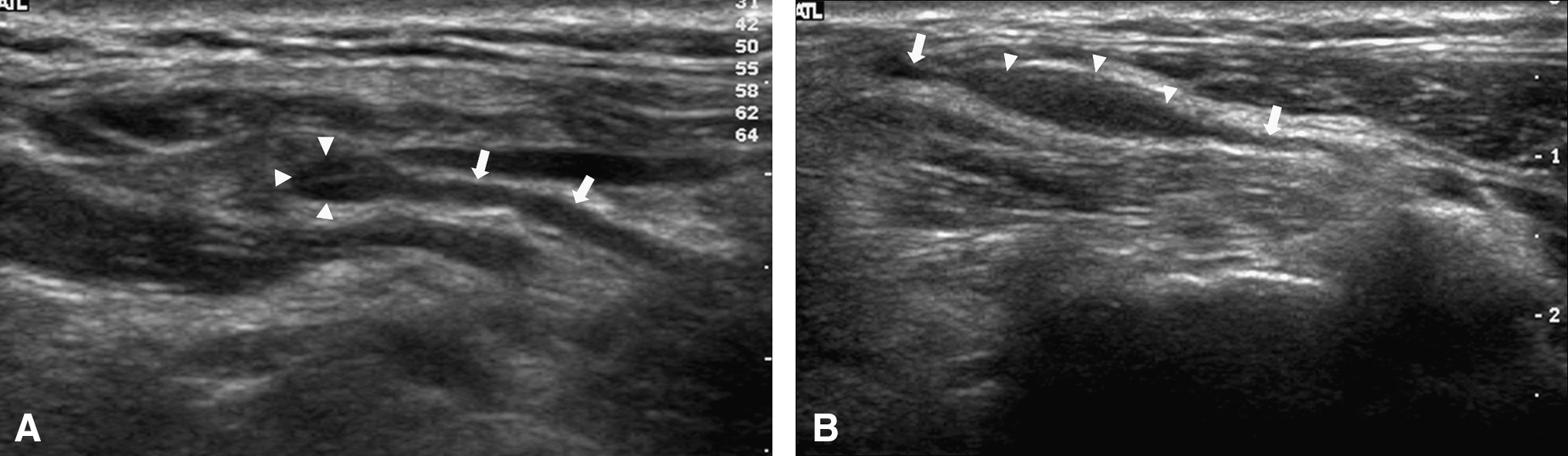
Two types of traumatic neuroma.
The US characteristics of traumatic neuromas and recurrent lymphadenopathies are summarized in Table 2. Traumatic neuromas had significantly smaller short axis diameters than recurrent lymphadenopathies (0.36 cm vs. 0.61 cm, p<0.001), as well as having a significantly smaller short-to-long axis ratio (0.31 vs. 0.61, p<0.001). Many recurrent lymphadenopathies, but none of the traumatic neuromas, were located medial to the IJV (p<0.001). Several US features, such as fusiform shape (p<0.001), ill-defined margins (p<0.001), mixed echogenicity (p<0.001), absence of vascular flow (p<0.001), absence of cystic portion (p=0.006), and absence of internal echogenic dots (p<0.001), significantly differentiated these two conditions. None of the traumatic neuromas showed evidence of a hilar line, vascular flow, or cystic portion.
Numbers in parentheses are ranges.
Zone 1: medial to the lateral margin of the IJV; zone 2: lateral to the lateral margin of the IJV.
IJV, internal jugular vein.
The interobserver and intraobserver agreements for basic US characteristics are summarized in Table 3. All showed substantial to high agreement.
Discussion
We found that 98.2% (55/56) of the traumatic neuromas that developed after total thyroidectomy with LND showed direct continuity with an involved nerve on US, a feature shown to be a characteristic finding of traumatic neuroma in other regions (1 –5). Identification of this characteristic US feature in the neck regions may prevent unnecessary surgery as well as painful FNA. Other ancillary US features may also help differentiate traumatic neuroma from recurrent lymphadenopathy.
Traumatic neuromas almost always arise from branches of the cervical plexus after neck dissection (8 –10). Indeed, all of the traumatic neuromas in our patients arose from branches of the cervical plexus. To determine the direct continuity of traumatic neuromas with involved nerves, it is important to understand the course of the cervical plexus and its related anatomy. The cervical plexus arises between the anterior and posterior tubercles of the transverse process and then moves posterolaterally in a downward direction. The branches of the cervical plexus are located deep inside the sternocleidomastoid muscle, between the longus capitis and scalene medius muscles in upper cervical levels or between the scalene anterior and scalene medius muscles in lower cervical levels (21 –23). By positioning the US probe in an oblique plane, that is, in the postero-infero-lateral direction, this anatomic relationship makes determination of the direct continuity of traumatic neuroma with branches of the cervical plexus more feasible (Fig. 4). In addition, this technique may be also useful in identifying the origin of the cervical plexus between the anterior and posterior tubercles of the transverse process, and then following its course to the periphery.
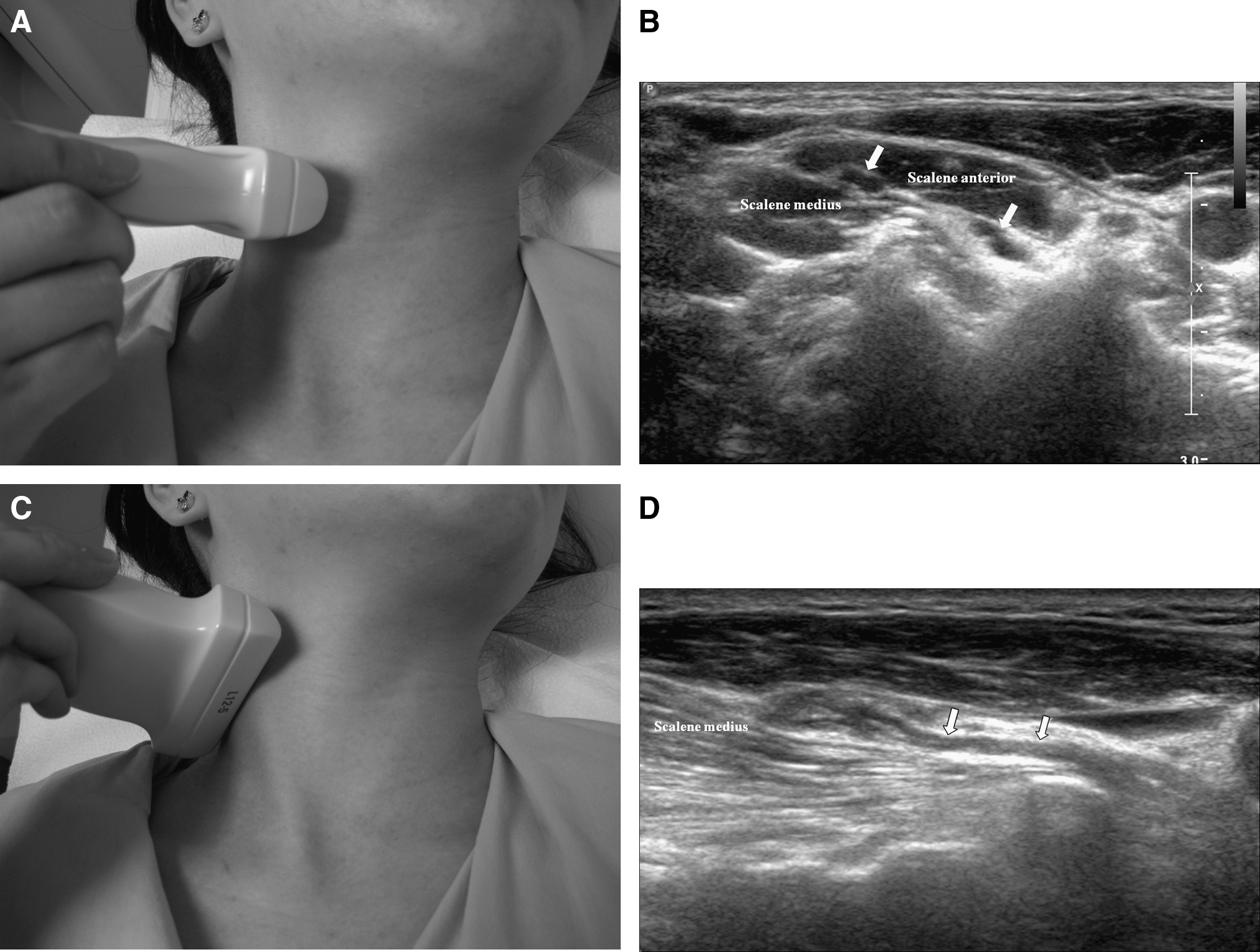
The course of the cervical plexus on ultrasound examination.
The direct continuity of the involved nerve with traumatic neuromas showed two different appearances on US, terminal or spindle type. These two features can also be distinguished by CT or MRI in other regions (3,4,24,25). On the basis of the findings of the present study, we concluded that spindle neuromas are more commonly developed in patients who undergo total thyroidectomy with LND. When considering the mechanism, partial nerve injury during or after surgery seems account the most developments of traumatic neuroma. Using an electrocautery instead of a conventional hand-tied ligation for hemostasis in thyroid surgery may be one of the possible causes of spindle-type neuroma development by neural injury beyond the cauterized site (26 –28).
Previous US studies of traumatic neuroma and recurrent lymphadenopathy assessed their size, echogenicity, and location (8,9). However, since there were overlaps in the range between the two, all of these US features were suggestive rather than diagnostic. In this study, we found that internal linear hypoechoic structures were very specific to traumatic neuroma. Because a traumatic neuroma originates from the nerve itself, this pattern seems to correspond to the neural fascicles. We also found that almost all the traumatic neuromas were located lateral to the IJV (zone 2), suggesting that a suspicious nodule located medial to the IJV (zone 1) is likely a recurrent lymphadenopathy. Other ancillary US features, including the absence of a hilar line, no vascular flow on power Doppler scan, and the lack of a cystic portion, were also significantly associated with traumatic neuroma. But none of these features were present in any of the traumatic neuromas assessed here.
This study has several limitations. Some of the traumatic neuromas were diagnosed by the acute exacerbation of pain during needle penetration into the nodule only. Due to the severe pain, it was difficult to obtain sufficient materials during FNA. However, since traumatic neuroma is a benign reparative process of the injured nerve, it is not appropriate to perform surgery to confirm a traumatic neuroma and it has generally been acceptable to make a diagnoses of traumatic neuroma based on the occurrence of typical severe pain during FNA (8,9,12). In this respect, the characteristic US feature of traumatic neuroma that we have described may have a great clinical significance, by allowing patients to avoid a painful procedure.
In conclusion, direct continuity with the cervical plexus may be a characteristic US feature of traumatic neuroma after neck dissection, and this feature, along with ancillary US findings, may prevent unnecessary surgery as well as painful FNA experiences.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.