
Abstract
Background:
Hypothyroidism may be a risk factor for obesity, because metabolic rates tend to be decreased in this disorder. Currently, it is under debate whether smoking may modify the association between hypothyroidism and obesity. Against this background, the aims of our study were to investigate whether there is an association between serum thyrotropin (TSH) and body mass index (BMI) in children and adolescents and whether smoking mediates this association.
Methods:
Data from 6435 children (ages 3–10) and 5918 adolescents (ages 11–17) from the “The German Health Interview and Examination Survey for Children and Adolescents” (KiGGS) were analyzed. Smoking status was classified into two categories: smokers and nonsmokers. A subject was classified as being exposed to environmental tobacco smoke (ETS) if someone in the parental home smoked more than 1 day a week. Serum TSH levels were measured with an ELISA method. Serum TSH levels were associated with BMI and obesity by multivariable linear regression stratified by smoking status and exposure to ETS.
Results:
In adolescents, there was an association between serum TSH levels and BMI, and it was stronger in smokers (β=0.62; 95% confidence interval [CI 0.38–0.85]) than in nonsmokers (β=0.18 [CI 0.09–0.28]). Likewise, it was stronger in adolescents exposed to ETS and adolescents not exposed to ETS. In children, who were either exposed or not exposed to ETS, there was an association between serum TSH levels and BMI. In them, however, the strength of this association was similar in those exposed and those not exposed to ETS.
Conclusions:
Active and passive smoking may mediate the association between thyroid function and BMI in adolescents. In smoking adolescents, hypothyroidism may lead to an increase of the BMI, whereas this is not the case in nonsmoking adolescents.
Introduction
Currently, it is under debate whether smoking may mediate the association between low thyroid function and obesity. Smokers are on average less overweight than nonsmokers, whereas individuals who quit smoking tend to gain weight (7). It has also been reported that current smokers have lower serum TSH levels than lifetime nonsmokers (8,9). Two previous studies showed an association between serum TSH levels and BMI in lifetime nonsmokers only (4,10), whereas a large population-based study from Norway demonstrated a significant association between hypothyroidism and obesity in both current smokers and lifetime nonsmokers (2).
Previous investigations conducted on the association between serum TSH levels and BMI in children and adolescents provide conflicting results. Three studies (11 –13) conducted in obese children and adolescents detected positive associations between serum TSH levels and BMI, whereas one study (14) including apparently healthy subjects did not. None of these studies (11 –14) was population-based, so that they might not be representative of their background populations. Moreover, the influence of smoking on the association between serum TSH levels and BMI has not been quantified in these studies (11 –14).
Against this background, the aims of our study were to investigate whether there is an association between serum TSH levels and BMI in children and adolescents and whether smoking mediates this association. For this investigation, we used data from a population-based German study with 12,353 children and adolescents.
Materials and Methods
Study population
The German Health Interview and Examination Survey for Children and Adolescents (KiGGS) is based on a nationally representative sample of children and adolescents 0–17 years of age with their main residence in Germany (15). The sampling procedure was performed according to a two-stage protocol developed in co-operation with the Center for Survey Research and Methodology (ZUMA), Mannheim, Germany. First, a systematic sample of 167 primary sample units was drawn from an inventory of German communities stratified according to a sociostructural classification of German regions of residence (BIK classification) (16). In the BIK classification, urban versus rural area of living, region, and proportions of commuters are considered. At the second stage, an equal number of addresses (n=24) per birth cohort was randomly selected (simple random sample) from local population registries within selected primary sample units 8 weeks before the commencement of examinations. Finally, a random sample was drawn at the Robert Koch Institute, Berlin, Germany, including a total of 8, 9, or 10 children and adolescents per birth cohort, depending on community size. The total KiGGS sample included 28,299 children and adolescents. The study was approved by the Charité/Universitätsmedizin Berlin ethics committee and the Federal Office for Data Protection (15).
Parents of eligible children and adolescents were contacted by letter and invited to participate in the survey. Following a random route plan, 167 personal sample units were covered by four study teams within 3 years (19 May 2003–6 May 2006). Personal contact was sought from those who had not responded to the invitation letter. In total, 17,641 children and adolescents participated in the study (response 66.6%). The parents of all the participants gave informed written consent.
From the 17,641 participants, we excluded all children <3 years (n=2805) from the present analysis, because no blood samples had been obtained from these children. Furthermore, we excluded 239 subjects with intake of thyroid medication and 2259 subjects with missing data in any of the considered variables, resulting in a study population of 12,353 children and adolescents.
Assessments
Study participants 3–10 and 11–17 years were classified as children and adolescents, respectively. Age, sex, and, in adolescents, active smoking status were determined according to computer-assisted personal interviews. Smoking status was classified into two categories: smokers and nonsmokers. A study participant was considered a smoker if he/she answered “Yes” to the question whether he/she had smoked one or more cigarettes during the past 4 weeks before the interview. Nonsmokers were respondents who had not smoked during the past 4 weeks. A subject was classified as being exposed to environmental tobacco smoke (ETS) if someone in the parental home smoked more than 1 day a week. Height was measured to the nearest 0.1 cm using calibrated stadiometers (Holtain Ltd., Crosswell, United Kingdom). Electronic scales (SECA Ltd., Hamburg, Germany) were used to measure body weight to the nearest 0.1 kg. From these measures, BMI was calculated: BMI=weight (kg)/height2 (m2). Obesity was defined according to the z-score BMI using the LMS method (17).
Blood samples were drawn with evacuated serum gel tubes between 9 a.m. and 7 p.m. and processed within 45 minutes according to a highly standardized protocol (18). TSH levels were measured with the ECLIA method on an Elecsys E2010 (Roche Diagnostics, Mannheim, Germany). During the study, the inter-serial coefficients of variation were 3.9% for TSH, 5.9% for free triiodothyronine, and 5.3% for free thyroxine. High and low serum TSH levels were defined according to age-specific reference limits established by Kratzsch et al. (19). From that study, we used the reference limits derived from the population, which included individuals with thyroid peroxidase and thyroglobulin antibodies >100 IU/mL. Hyperthyroidism was defined according to low serum TSH levels, whereas hypothyroidism was defined according to high serum TSH levels. Normal thyroid function was defined as serum TSH levels within the reference range.
Statistical methods
The study population was divided into three groups according to serum TSH levels. Data on quantitative characteristics are expressed as mean and standard deviation. Data on qualitative characteristics are expressed as percent values or absolute numbers, as indicated. Continuous as well as categorized serum TSH levels were associated with BMI and obesity by linear and logistic regression models, respectively, adjusted for age, sex, smoking status, exposure to ETS, as well as systolic and diastolic blood pressure. In regression models with continuous serum TSH levels, fractional polynomials were applied to explore and graph nonlinear associations (20). The dose-response relation was found using fractional polynomials up to degree 2 with all possible combinations of powers selected from the set (−2, −1, −0.5, 0, 0.5, 1, 2, 3) and compared by the log likelihood to determine the best-fitting model. If none of the fractional polynomial models fitted the data significantly better than the linear model, untransformed serum TSH levels were used in the calculation. Analyses were performed for children and adolescents separately. A p-value <0.05 was considered statistically significant. All analyses were performed using Stata 11.1 (Stata Corporation, College Station, TX).
Results
Characteristics of the study population
Among the sample, 6132 children (95.3%) had serum TSH levels within the reference range, 111 children (1.7%) had low levels, and 192 children (3.0%) had high serum TSH levels. The prevalence of increased [decreased] serum TSH levels in the specific age ranges were 2.2% [0.6%] (3–5 years), 3.8% [1.1%] (6–8 years), 2.3% [4.5%] (9–11 years), 2.6% [0.7%] (12–14 years), and 8.2% [0.3%] (≥15 years). Children with low serum TSH levels were older than children with serum TSH levels within the reference range. Children with high serum TSH levels had a higher BMI than children with serum TSH levels within the reference range (Table 1).
Continuous data are expressed as mean±standard deviation, and statistical significance was calculated using the Kruskal–Wallis-test. Categorical data are expressed as number and percentage, and statistical significance was calculated using the χ2 test.
Defined by low/high serum TSH levels using reference limits published by Kratzsch et al. (19).
Obesity was defined according to Cole (17).
BMI, body mass index; ETS, environmental tobacco smoke; TSH, thyrotropin.
There were 5608 adolescents (94.8%) with serum TSH levels within the reference range, 82 adolescents (1.4%) with low levels, and 228 adolescents (3.9%) with high serum TSH levels. Adolescents with low serum TSH levels were younger, included fewer smokers, and had a lower BMI than adolescents with serum TSH levels within the reference range (Table 1). Adolescents with high serum TSH levels were older and had a higher BMI than adolescents with serum TSH levels within the reference range (Table 1).
Multivariable analyses: association between serum TSH levels and BMI in children and adolescents
The statistical interaction between serum TSH levels and sex was not significantly associated with BMI in children (p=0.271) or adolescents (0.405). Thus, we opted not to perform sex-stratified analyses. The best fractional polynomial that fit the association between serum TSH levels and BMI was of degree 1 and of power 0 (Table 2). Log-transformed serum TSH levels were positively associated with BMI in both children and adolescents. Moreover, serum TSH levels were positively associated with obesity in a linear fashion in both children and adolescents (Table 2).
All models are adjusted for age, sex, smoking status, and ETS.
p<0.05.
Obesity was defined according to Cole (17).
CI, 95% confidence interval.
Multivariable analyses: association between serum TSH levels and BMI in adolescents stratified by smoking status
Stratified analyses revealed that untransformed TSH values fit the association between serum TSH levels and BMI best in adolescent smokers and adolescent nonsmokers. Serum TSH levels were significantly associated with BMI both in adolescent smokers and in adolescent nonsmokers (Table 2 and Fig. 1), but the effect size was thrice higher in adolescent smokers than in adolescent nonsmokers. Furthermore, serum TSH levels were significantly associated with obesity in adolescent smokers and adolescent nonsmokers, but the effect size was stronger in adolescent smokers. In children, smoking status was not available; so, we could not perform analyses stratified by smoking status in children.
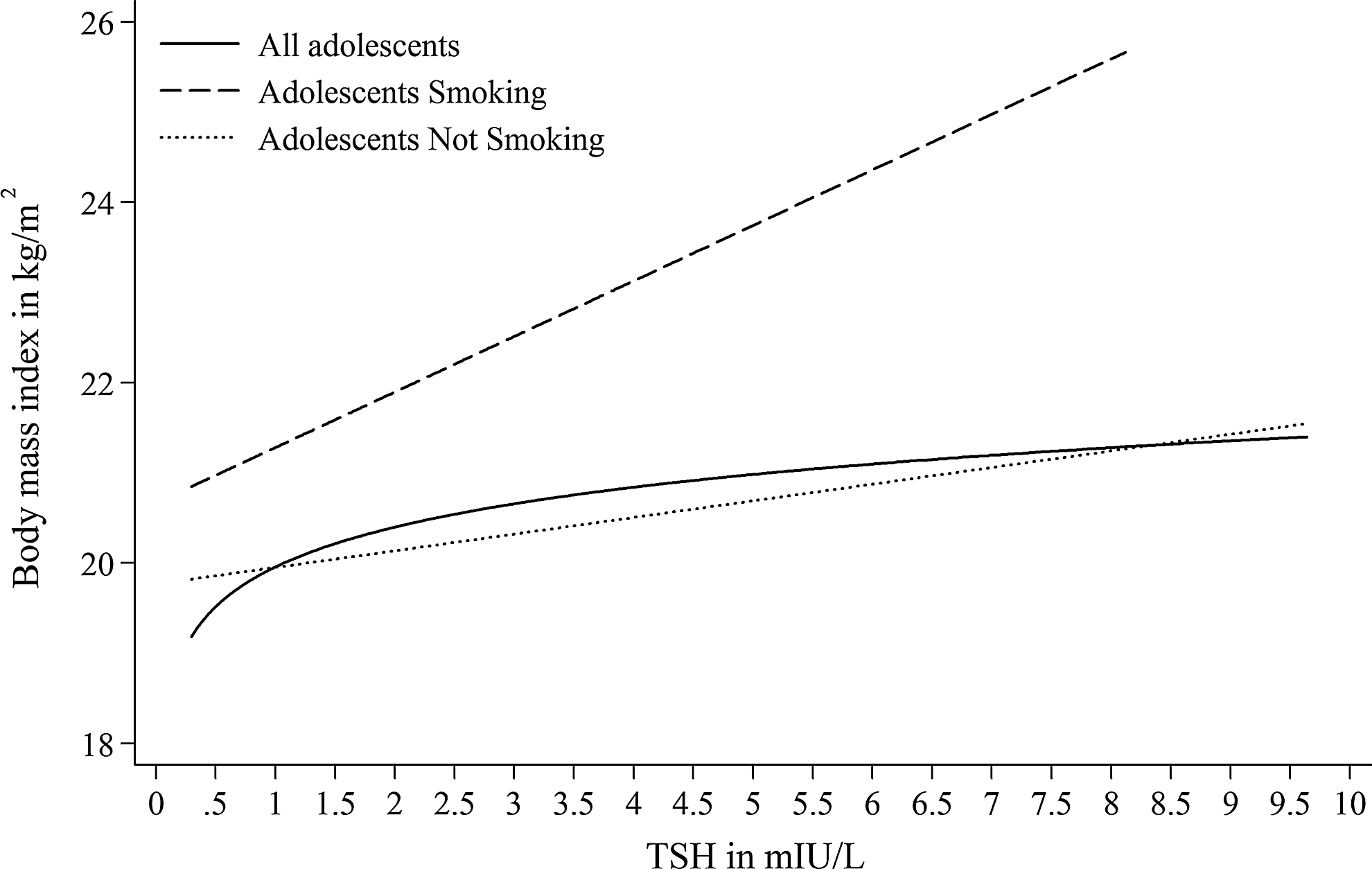
Association between serum thyrotropin (TSH) levels and body mass index (BMI) in adolescents stratified by smoking status. For comparability to adolescent smokers, regression curves for all adolescents and adolescent nonsmokers were cut at 0.3 mIU/L.
Multivariable analyses: association between serum TSH levels and BMI in children and adolescents stratified by exposure to ETS
Untransformed TSH fitted the association between serum TSH levels and BMI best in subjects exposed to ETS, whereas log-transformed TSH fitted the latter association best in subjects not exposed to ETS. Serum TSH levels were positively associated with BMI in children and adolescents exposed to ETS (Fig. 2), and log-transformed serum TSH levels were significantly associated with BMI in children and adolescents not exposed to ETS (Fig. 2). Furthermore, serum TSH levels were significantly associated with obesity in children and adolescents not exposed to ETS, whereas there was no significant association between serum TSH levels and obesity in children and adolescents exposed to ETS.
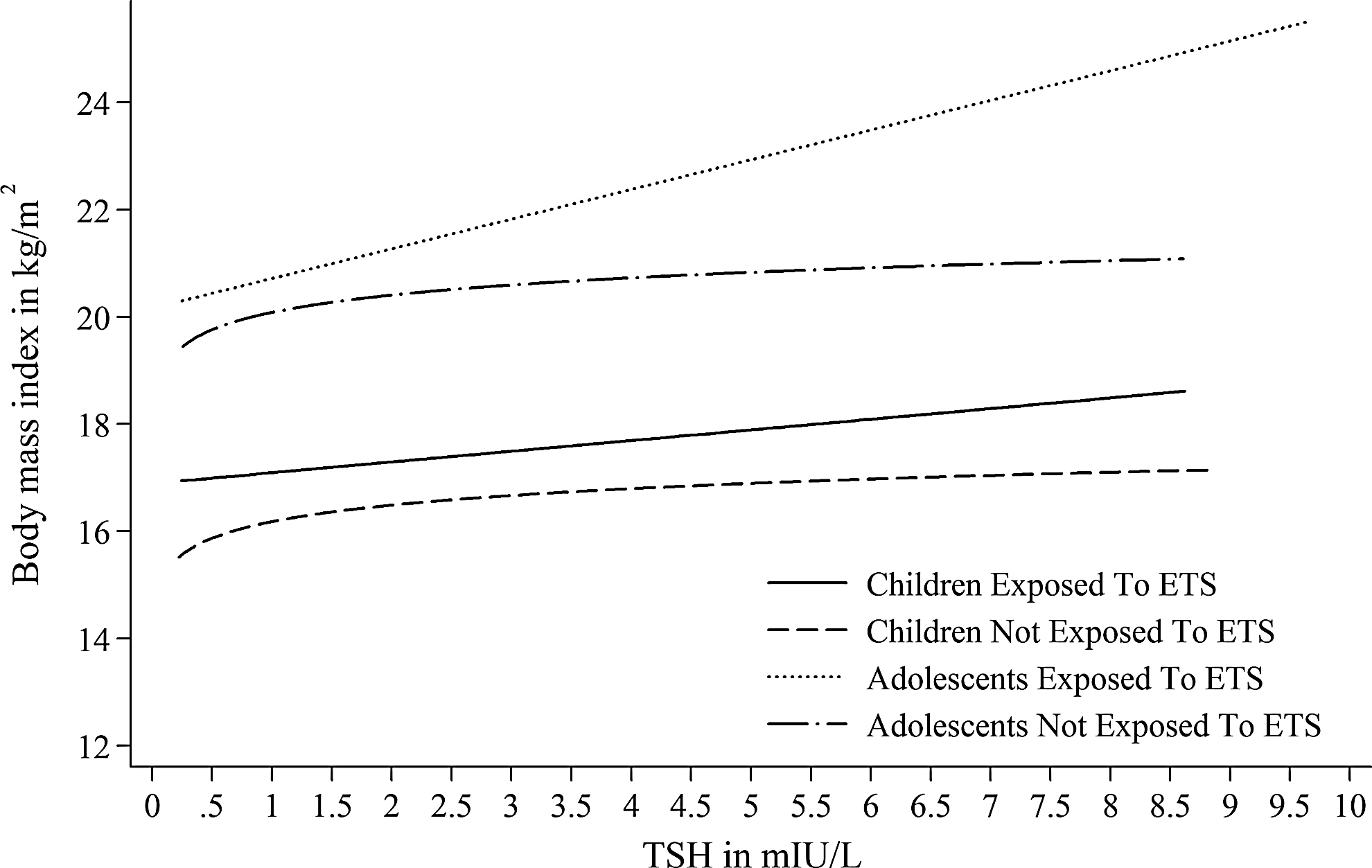
Association between serum TSH levels and BMI in children and adolescents stratified by exposure to environmental tobacco smoke (ETS). For comparability to children exposed to ETS and adolescents not exposed to ETS, regression curves for children not exposed to ETS and adolescents exposed to ETS were cut at 0.3 mIU/L.
Categorization of serum TSH levels
Children with low serum TSH levels had a significantly lower BMI than children with serum TSH levels within the reference range (Table 3). This association was also present in children not exposed to ETS. We detected no further significant associations between categorized serum TSH levels and BMI or obesity in children.
All models are adjusted for age, sex, smoking status, and ETS.
Reference: serum TSH levels within the reference range.
Defined by low/high serum TSH levels using reference limits published by Kratzsch et al. (19).
p<0.05.
Obesity was defined according to Cole (17).
In adolescents, low serum TSH levels were associated with BMI only in the group exposed to ETS. Adolescents with high serum TSH levels had a significantly higher BMI. Among them, more were obese than among adolescents with serum TSH levels within the reference range. Moreover, high serum TSH levels were associated with BMI in adolescent smokers and adolescents not exposed to ETS. Furthermore, high serum TSH levels were significantly associated with obesity in adolescents not exposed to ETS.
Serum TSH levels within the reference range
To explore the association between serum TSH levels in the reference range and BMI, we excluded 303 children and 310 adolescents with serum TSH levels outside the reference range. In children, serum TSH levels within the reference range were significantly associated with both BMI and obesity (Table 4). Subgroup analyses revealed that serum TSH levels within the reference range were significantly associated with BMI in both children exposed and those not exposed to ETS. Furthermore, serum TSH levels within the reference range were significantly associated with obesity in children not exposed to ETS.
All models are adjusted for age, sex, smoking status, and ETS.
p<0.05.
Obesity was defined according to Cole (17).
In adolescents, serum TSH levels within the reference range were associated with BMI in the total population and in all subgroups with regard to smoking and exposure to ETS (Figs. 3 and 4). The effect sizes were stronger in adolescent smokers and adolescents exposed to ETS than in nonsmoking adolescents and adolescents not exposed to ETS, respectively. Serum TSH levels within the reference range were associated with obesity in all considered subgroups with one exception. In the subgroup of smoking adolescents, the association between serum TSH levels within the reference range and obesity barely missed statistical significance (p=0.070).
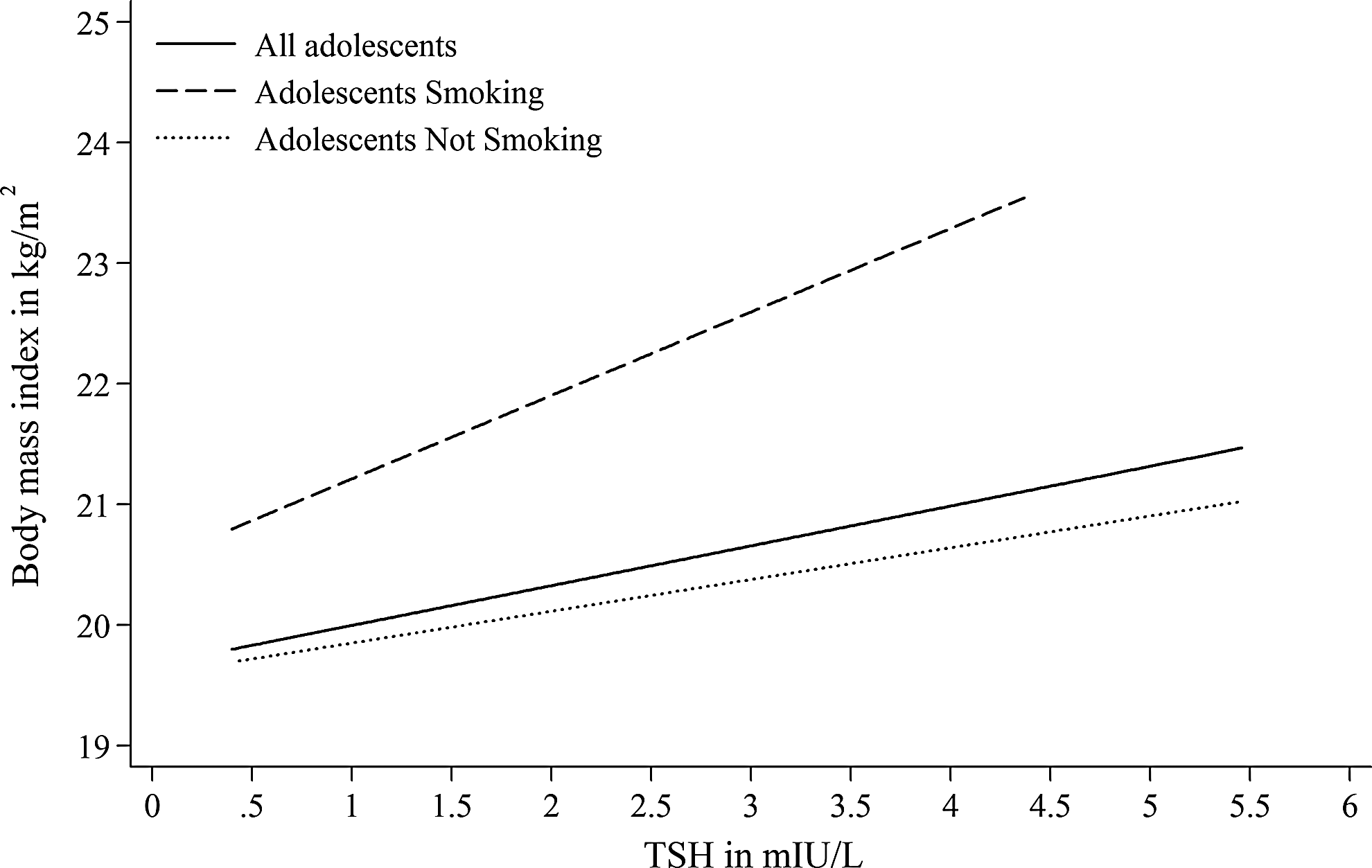
Association between serum TSH levels within the reference range and BMI in adolescents stratified by smoking status.
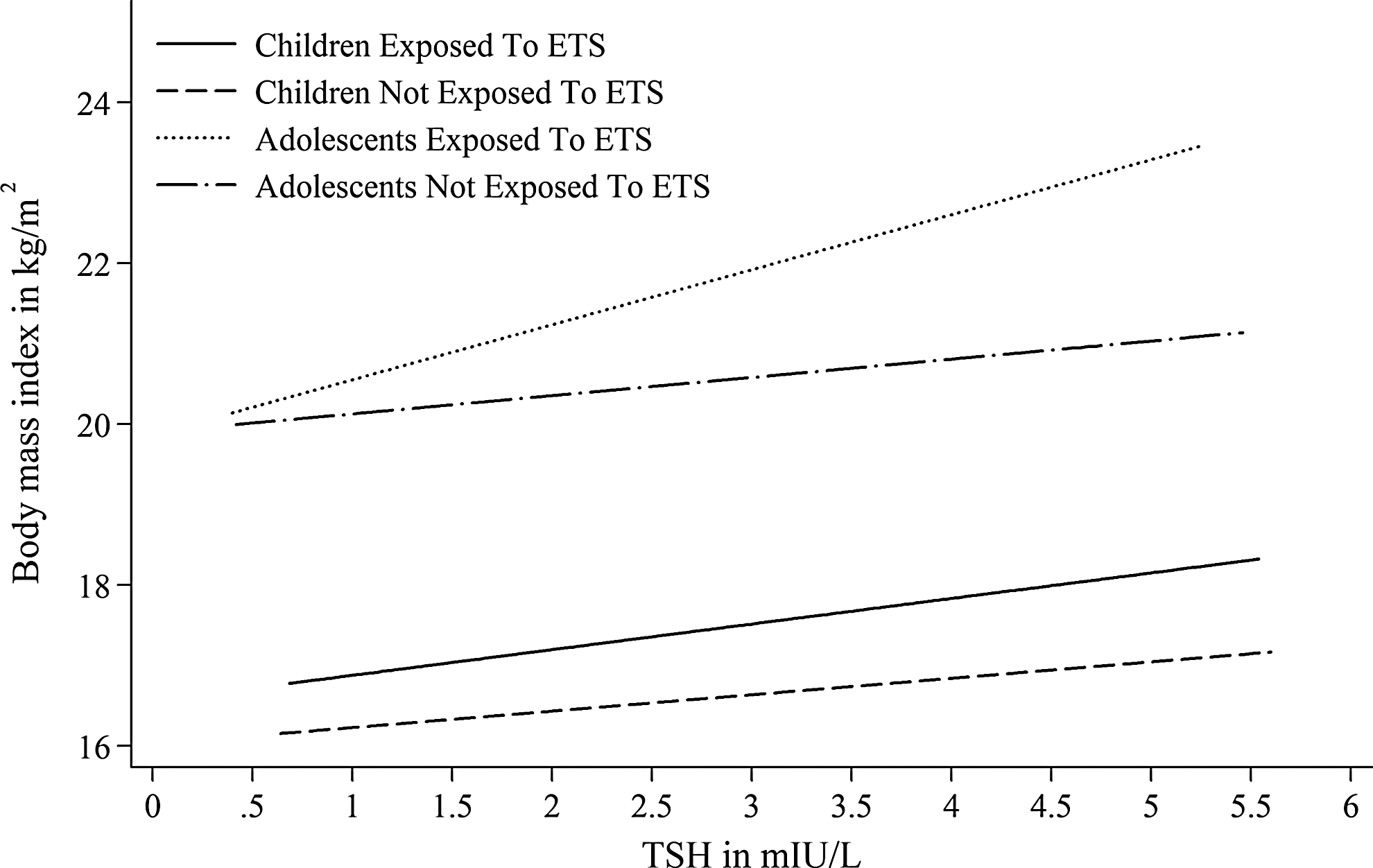
Association between serum TSH levels within the reference range and BMI in children and adolescents stratified by exposure to ETS.
Defining children as individuals <10 years did not significantly change the results. For instance, the association between log-transformed serum TSH levels and BMI in all children was still highly significant when using 10 years as threshold (β=0.36; 95% confidence interval [CI 0.23–0.48]; p<0.001).
Relation of smoking and exposure to ETS with serum TSH levels and BMI
In multivariable linear regression, smoking was inversely associated with serum TSH levels in adolescents (β=−0.28 [CI −0.36, −0.21]; p<0.001); whereas exposure to ETS was not associated with serum TSH levels in children (β=−0.03 [CI −0.12, 0.06]; p=0.549) and adolescents (β=−0.03 [CI −0.09, 0.04]; p=0.455). In adolescents, smoking and exposure to ETS were positively associated with BMI (β=0.61 [CI 0.36, 0.86]; p<0.001 and β=0.85 [CI 0.63, 1.07]; p<0.001). After further adjustment for total household income, the association between smoking and BMI in adolescents was still statistically significant, albeit with a lower effect size (β=0.52 [CI 0.26, 0.78]; p<0.001). Likewise, exposure to ETS was positively associated with BMI (β=0.60 [CI 0.44, 0.76]; p<0.001) in children.
Discussion
In the present study, we detected significant associations between serum TSH levels and BMI in a nationwide population sample of children and adolescents. Our findings are in concordance with other studies (11 –13) conducted in obese children and adolescents, but in discordance with one study conducted in apparently healthy children (14). In the latter study (14), subjects were not selected in a population-based design, and analyses were not adjusted for main confounders such as age, which might have biased the results. Our findings support the results of four studies from adult populations (1 –4).
We demonstrated significant relations of serum TSH levels over the full range, high serum TSH levels, and serum TSH levels within the reference range with BMI in smoking adolescents. These associations, however, were less strong in nonsmoking adolescents. Likewise, serum TSH levels were stronger associated with BMI in adolescents exposed to ETS than in adolescents not exposed to ETS. The results are in contrast to two previous reports from population-based studies conducted in adult populations (4,10), where associations between serum TSH levels and BMI were only reported in lifetime nonsmokers; while they are in agreement with data from another adult population (2), where a positive association between serum TSH levels within the reference range and BMI was reported in smokers and nonsmokers. An obvious explanation for the discrepant results might be that smoking affects thyroid function and BMI differently in adolescents compared with adults.
Moreover, socioeconomic factors might help explain the difference in association between serum TSH levels and BMI in smoking and nonsmoking adolescents. It has been previously reported that students from schools with a lower educational level are more likely to smoke than students from schools with a higher educational level (21). Likewise, it has been demonstrated that adolescents from families with low socioeconomic status or a low educational level are at high risk of obesity (22). Thus, a low educational level is a common predictor for both smoking and obesity. Educational level might explain the positive association between smoking and BMI in our study and, in consequence, also the difference in the magnitude of the associations between serum TSH levels and BMI between smoking and nonsmoking adolescents, because smoking was also associated with serum TSH levels in our study. The effect size for the association between smoking and BMI was decreased after adjustment for total household income, which might support this notion.
In children, the association between serum TSH levels and BMI was similar in individuals exposed to ETS and in those not exposed to ETS; whereas in adolescents, this association was stronger in individuals exposed to ETS than in individuals not exposed to ETS. These differences in results between children and adolescents might be referred to the missing association between ETS exposure and serum TSH levels in children and adolescents. In contrast, we showed an inverse association between smoking and serum TSH levels in adolescents and strong relations of smoking and exposure to ETS with BMI in children and adolescents. Thus, the association between serum TSH levels and BMI in adolescents exposed to ETS might be referred to the association between serum TSH levels and BMI in smoking adolescents, because adolescents exposed to ETS are more likely to start smoking than adolescents from households with a smoking ban (23,24). This might provide an explanation for the conflicting results between children and adolescents with regard to environmental smoking.
The strengths of our study include its population-based design, which is representative of the children and adolescent population of Germany. Furthermore, to the best of our knowledge, this is the first study that investigates the influence of smoking on the association between thyroid function and BMI in children and adolescents. Limitations arise from the cross-sectional design of the study, allowing only limited validity according to causality. In addition, data on smoking and ETS are based on self-statements only. However, data revealed that in a general population the degree of underreporting is small and, thus, does not carry a substantial information bias on results (25). Finally, from our data, it was not possible to define former smoking.
In conclusion, we demonstrated that active and passive smoking mediates the association between thyroid function and BMI in adolescents. In smoking adolescents, hypothyroidism may lead to an increase of the BMI; whereas this is not the case in nonsmoking adolescents.
Footnotes
Acknowledgment
Analyses were supported by the German Research Foundation (DFG Vo 955/5-2).
Disclosure Statement
The authors have nothing to disclose.