
Abstract
Background:
A low-iodine diet (LID) is usually recommended for a week or two before radioactive iodine (RAI) ablation therapy in papillary thyroid cancer (PTC) patients after total thyroidectomy. However, it is still controversial whether an LID affects ablation outcomes. We therefore evaluated the association between urinary iodine excretion and the rate of successful ablation and investigated the determinants of successful RAI ablation outcomes.
Methods:
We retrospectively reviewed the records of 295 consecutive patients with PTC who received 1110 MBq RAI remnant ablation therapy with thyroid hormone withdrawal after total thyroidectomy. Successful ablation was defined as either no visible or faint uptake on a follow-up scan (definition 1), or no visible or faint uptake on a follow-up scan and a stimulated thyroglobulin level <2 ng/mL (definition 2).
Results:
The proportion of patients with appropriate LID status (defined as a urinary iodine concentration [UIC] <66.2 μg iodine/g creatinine [μg/gCr]) was significantly higher in the successfully ablated group (81% vs. 67%, p=0.03). Based on definition 1, 80.3% (237/295) of patients were successfully ablated. The ablation rate was significantly lower in patients who had a UIC >250 μg/gCr at the time of RAI ablation (p<0.05). In multivariate analysis, a UIC >250 μg/gCr was the only significant variable associated with ablation failure (p=0.002, odds ratio [OR] 4.74 [95% confidence interval (CI) 1.78–12.63]). Based on definition 2, 74.9% (221/295) of patients were successfully ablated. A UIC >250 μg/gCr at RAI administration showed a significant association with ablation failure (p<0.05). The OR of a UIC >250 μg/gCr for ablation failure was 3.88 [CI 1.42–10.57] (p=0.008).
Conclusion:
Excessive iodine intake (UIC >250 μg/gCr) was associated with poor RAI ablation outcomes. Because this amount of iodine is very high, we propose that the level of strictness of the LID protocol should be modified according to the region that the patient is from and the food that the patient is accustomed to eating. Even in those areas where iodine intake is high, overly strict compliance with an LID protocol is not necessary and simple recommendations to avoid iodine-rich foods would be appropriate.
Introduction
In this study, we evaluated the association between the iodine content in the body, expressed as UIC, and the success of RAI ablation in patients resident in iodine-sufficient areas. We also investigated the determinants of successful RAI ablation outcomes.
Patients and Methods
Patients
We retrospectively reviewed 295 papillary thyroid cancer (PTC) patients who underwent a total thyroidectomy and received 1110 MBq of 131I RAI-RX for remnant ablation between February 2009 and June 2010 at Samsung Medical Center. Samsung Medical Center is one of the largest tertiary referral centers in South Korea. A total thyroidectomy was performed by a team of four head and neck surgeons who each perform >300 cases of thyroid surgery per year and who used the same total thyroidectomy technique to manage PTC. Enrolled patients had low to intermediate risk of recurrence based on their clinical and pathologic features according to the 2009 revision of the American Thyroid Association guidelines (14). Patients with distant metastasis and antithyroglobulin antibodies (TgAbs), and those with a peak TSH concentration <30 mIU/L at the time of ablation, were excluded. Patients who were exposed to iodine-containing drugs such as intravenous contrast for computed tomography (CT) scan or amiodarone within 4 months are excluded from RAI-RX in our center. The Institutional Review Board at Samsung Medical Center approved this study.
RAI ablation and whole-body scan
Four weeks before RAI administration, patients stopped levothyroxine (L-T4) replacement therapy and switched to triiodothyronine (T3) for 2 weeks, followed by the withdrawal of T3 for 2 weeks. RAI remnant ablation was performed with an activity of 1110 MBq. A post-therapy whole-body scan (WBS) was performed 2 days after RAI administration using a dual-head gamma camera (E-CAM; Siemens Medical Solutions, Erlangen, Germany). Six to 12 months after RAI-RX, a diagnostic (Dx) WBS using 185 MBq of 123I or 111 MBq of 131I was performed. The DxWBS results were interpreted by an experienced nuclear physician without knowledge of the UIC levels of the patients. Scan interpretations were classified as negative when the uptake in the bed was absent or insignificant compared to the background activity on DxWBS. Patients were advised to follow an LID for 2 weeks before RAI-RX and the diagnostic scan, as described previously (15,16). Briefly, they were educated and encouraged by specially trained dieticians before the start of the LID. They were informed about the foods and drugs that were allowed and not allowed (Table 1). They were given a 3-day sample menu specifically designed for patients living in Korea and the contact information for dietary questions. Based on our previous report, we defined a spot urine iodine/creatinine (I/Cr) ratio of <66.2 μg/gCr as an indicator of an effective LID (15). Blood samples for serum TSH, free T4, thyroglobulin (Tg), and TgAb measurements, and urine samples for I and Cr measurements were obtained from all patients on the same day of RAI administration for RAI-RX or DxWBS.
Laboratory methods
Serum Tg was measured by an immunoradiometric assay (Tg+ RIA; BRAHMS, Hennigsdorf, Germany). Serum TgAb was measured by radioimmunoassay (anti-Tg RIA; BRAHMS). TgAb values of <60 U/mL were considered negative. Serum TSH was measured using an immunoradiometric assay (IRMA TSH; Immunotech, Marseille Cedex, France). Serum free-T4 was quantitated by radioimmunoassay (FT4 RIA KIT; Immunotech). UIC was measured by inductively coupled plasma mass spectrometry using an Agilent 7500 series instrument (Agilent Technologies, Inc., Tokyo, Japan), which has been demonstrated to provide extremely accurate measurements of UICs (17,18). For iodine measurements, the intraday coefficient of variation (CV) was 0.3–1.2%, and the interday CV was 1.4–3.3%. We reported previously that the I/Cr ratio from spot urine can serve as a useful and reliable alternative to 24-hour urine collection, and in this study, the cutoff I/Cr ratio for a poor LID preparation was >66.2 μg/gCr, which approximates a 24-hour urine excretion of >150 μg/day (15). Urine Cr was measured using a Cobas Integra 800 instrument (Roche Diagnostics, Basel, Switzerland).
Definition of successful ablation
We used two definitions of successful ablation. Definition 1 was the absence of significant visible uptake above background activity in the neck on DxWBS. Definition 2 was the absence of significant visible uptake above background activity in the neck on DxWBS, plus a stimulated serum Tg of <2 ng/mL.
Statistical analysis
All statistical analyses were performed using PASW 17.0 software (SPSS, Inc., Chicago, IL). The Student's t test and the Mann–Whitney test were used to assess the significance of differences in continuous variables between groups, while the chi-squared test was used for categorical variables. The Mantel–Haenszel chi-squared test was used to analyze the association between UIC and successful ablation. Multivariate logistic regression analysis was used to study variables associated with successful ablation. A p-value <0.05 was considered significant.
Results
Patient characteristics
Two hundred ninety-seven patients (49 males, 246 females) with a mean age (±standard deviation [SD]) of 45.8±9.5 years were included. All patients had histologically confirmed PTC. At initial presentation, 60.7% (179/295) of patients had lymph node metastasis, mostly in the central region only (177/179), because we used a higher dose of RAI to treat patients with lateral neck lymph node metastasis and those who received >1110 MBq were not included in this study. The mean size of the tumor was 0.88±0.4 cm, and gross extrathyroidal invasion was detected in 13.2% (39/295) of patients. The mean TSH concentration at the time of RAI-RX was 100.8±42 μIU/mL and the mean stimulated Tg level was 1.3±2.3 ng/mL. The UIC at RAI-RX was 88.7±192.3 μg/gCr (median 33.5, range 9–1357; Table 2).
SD, standard deviation; LN, lymph node; TSH, thyrotropin; Tg, thyroglobulin; RAI, radioactive iodine; LID, low-iodine diet.
Successful ablation as defined by a DxWBS only (definition 1)
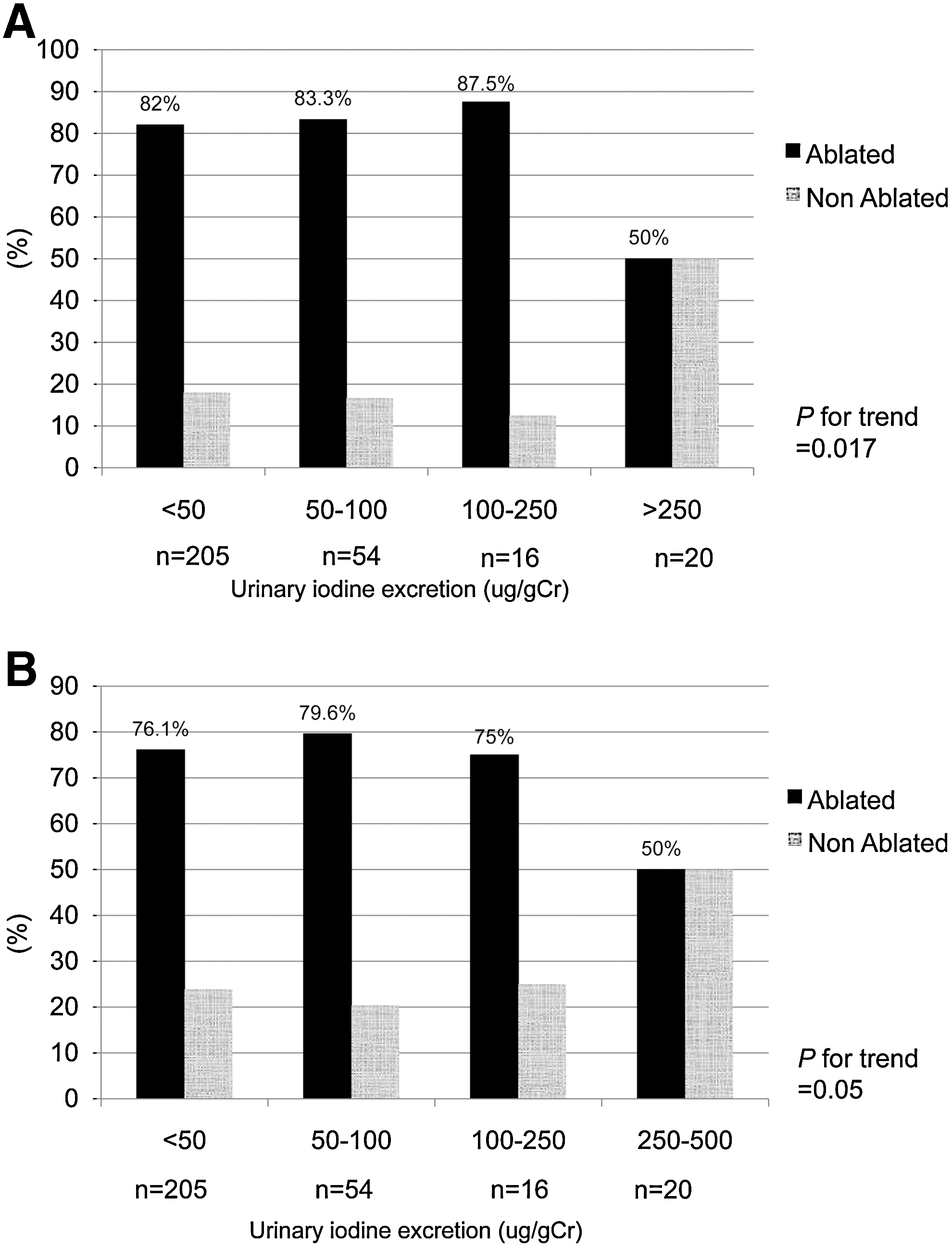
When we defined successful ablation based on definition 1, 80.3% (237/295) of patients were successfully ablated with 1110 MBq of RAI. When we compared the clinical and pathological characteristics of the successfully ablated and nonablated groups, we found no differences in age, sex, extrathyroidal invasion, lymph node (LN) invasion, TSH, or Tg levels at ablation (Table 3). Median or mean UIC values at the time of ablation were not significantly different between the ablated and nonablated groups (Fig. 1A). However, the proportion of patients who achieved the appropriate LID status according to our previously reported cutoff value (<66.2 μg/gCr) was significantly higher in the successfully ablated group (p=0.03). When we stratified the patients into four groups according to UIC, the ablation rate was significantly lower in patients who had a UIC >250 μg/gCr at the time of RAI-RX (p=0.017 for trend; Fig. 2A). In multivariate analysis, a UIC >250 μg/gCr was the only significant variable associated with ablation failure (p=0.002, odds ratio [OR] 4.74 [95% confidence interval (CI) 1.78–12.63]; Table 4).

Successful ablation as defined by a DxWBS and stimulated Tg levels (definition 2)
When we defined successful ablation according to definition 2, 74.9% (221/295) of patients were successfully ablated with 1110 MBq of RAI. Age, sex, extrathyroidal invasion, LN invasion, and TSH levels at ablation were not significantly different between the successfully ablated and nonablated groups (Table 5). Mean or median UIC levels at the time of ablation were also not significantly different between the ablated and nonablated groups (Fig. 1B). The proportion of patients who achieved an appropriate LID status according to our previously reported cutoff value (<66.2 μg/gCr) was marginally different between the successfully ablated group and the nonablated group (p=0.065). The level of stimulated Tg was significantly higher in the nonablated group. When we stratified the patients into four groups according to UIC levels, the ablation rate was significantly lower in patients who had a UIC >250 μg/gCr at the time of RAI-RX (p=0.05 for trend; Fig. 2B). In multivariate analysis, a UIC level of >250 μg/gCr was a significant variable associated with ablation failure (p=0.008, OR 3.88 [CI 1.42–10.57]) along with the level of stimulated Tg at RAI ablation (p<0.001, OR 1.36 [CI 1.17–1.59]), which is inherent in the definition of successful ablation in this analysis (Table 6).
Discussion
Our data show that excessive urinary iodine excretion is associated with RAI remnant ablation failure. However, the level of UIC associated with ablation failure is so high (I/Cr ratio, >250 μg/gCr) that the strictness of the LID guidelines should be adjusted according to the region where the patients are residing and the food that they eat.
Iodine uptake by remnant thyroid tissue or a DTC depends on several factors, including the amount of remnant thyroid tissue, adequate TSH stimulation, expression of NIS, and a low body iodine pool (8,9). Adequate depletion of the body iodine pool for RAI-RX can be achieved by limiting iodine intake using the LID guidelines (10,11,15). Most guidelines for the management of thyroid cancer recommend that patients preparing for RAI-RX should be on an LID, preferably <50 μg iodine/day, for about 1–2 weeks pretreatment, and emphasize the importance of measuring UIC to evaluate the body iodine pool before RAI-RX (5,7,14,19). In this study, we provide evidence to support the common belief that the success of RAI remnant ablation decreases with increasing UIC levels, which is based on the increased uptake and half-life of RAI after an LID but not on outcome studies such as evaluation of the rate of ablation or recurrence (9,20). Unexpectedly, however, the level of UIC associated with increased ablation failure was 250 μg/gCr. This is equivalent to an estimated 24-hour iodine excretion of 518 μg daily, based on an equation we proposed in a previous study (15). This daily UIC level is a status of iodine excess according to the World Health Organization criteria (21,22). When we consider that 90% of ingested iodine is absorbed in healthy adults and >90% of ingested iodine is excreted in the urine, we propose that the strictness of the LID guideline should be modified according to the region where the patients live and the food that they eat. For example, patients living in an iodine-deficient area require almost no dietary modifications to prepare for RAI-RX. Patients who live in an iodine-sufficient area can follow simple guidelines to avoid seaweeds, fishes, and high-iodine-containing food of that region, rather than being required to strictly follow an LID.
Recently, Tala Jury et al. reported quite different results to our study findings (13). They retrospectively reviewed 201 patients with DTC who received RAI-RX in Sienna, Italy, which is a moderately iodine-deficient area, either after THW (n=125) or rhTSH (n=76). They found no significant difference in UIC between the ablated versus nonablated patients in either the THW or rhTSH groups, and in multivariate analysis, the UIC level was not associated with the success of ablation. However, there are significant differences between our study and theirs that may explain these discrepancies. First, unlike our study where a strict LID protocol was implemented, the patients in their study were not prescribed a specific LID protocol but were simply told to avoid iodine-containing supplements and drugs in the 4 weeks before ablation (13). Second, while Sienna is an area of moderate iodine deficiency, our subjects were enrolled in Korea, where the average estimated iodine intake is very high—as much as 479 μg/day—and the average UIC level is 674 μg/gCr (23). Consequently, very few patients with excessive UIC (>500 μg/L) were included in the study of Tala Jury et al. (13). Because we only found a difference in the rate of ablation success in patients with a UIC >250 μg/gCr (I/Cr ratio)—which is approximately equivalent to a daily iodine excretion of 518 μg/day—it is quite likely that Tala Jury et al. (13) did not find statistical significance in UIC levels between ablated and nonablated groups because of the small number of patients with excessive UIC enrolled in their study. Third, we enrolled consecutive patients treated with the same dose of RAI (1110 MBq) to rule out possible bias caused by different levels of RAI activity on ablation outcome, while Tala Jury et al. (13) included patients treated with various levels of RAI activity (1110–5550 MBq), which might have affected their results, although they demonstrated that there was no significant difference in RAI dose between the ablated and nonablated groups. Morris et al. reported a 68.2% (30/44) ablation rate for LID patients compared to a 62% (31/50) rate for regular diet patients, a nonsignificant difference (p=0.53) for patients treated postsurgically with 3700–7400 MBq of RAI and followed up with diagnostic scan (12). However, they reported that significantly more patients were treated with >150 mCi in the regular-diet group than in the LID group; therefore, different levels of RAI administered at ablation might have influenced their results. Furthermore, they only measured UIC in a subset of the enrolled patients (14.9%, 14/94) (12). Pluijmen et al. examined stimulated Tg levels and follow-up RAI scans in 120 DTC patients without distant metastasis (LID group, n=59, and control group, n=61) 6 months after remnant ablation (11). Although an LID did not have a significant effect on the success of ablation when successful ablation was defined as no visible uptake on the follow-up WBS, the rate of successful ablation was significantly higher in the LID group than in the control group (65% vs. 48%, respectively) when they used the criteria of visible uptake and stimulated Tg levels <2 ng/mL for successful ablation (11). This is in accordance with our study; furthermore, we found statistical significance even when we used the criterion of the follow-up WBS results only.
Our study has several limitations. First, this study was not a prospective study comparing a regular diet and an LID, but a retrospective analysis of consecutive patients who were instructed to follow a strict LID protocol before RAI-RX using 1110 MBq. Although consecutive patients were selected and a specific dose of radioactivity was chosen to reduce bias, the results of this study should be reproduced in a future prospective study. Second, we did not determine the specific causes of excessive UIC in the patient group with a urinary I/Cr ratio >250 μg/gCr. Although the main cause could be a failure to comply with the LID protocol and we excluded the patients who were exposed to iodine-containing medications, such as intravenous contrast for CT and amiodarone, other unknown causes of excessive intake that interfere with RAI-RX success should be sought in future studies.
In conclusion, we found that excessive iodine content in the body is associated with poor RAI ablation outcomes in patients with PTC after total thyroidectomy. However, the level of excessive iodine content in the body measured by UIC was so high that this kind of excess body iodine is only likely to be problematic in regions where iodine intake is high or excessive, such as Korea and Japan. Based on our results, we propose that the strictness of the LID protocol should be modified according to the region that the patients are from and the food that they commonly consume. Even in areas where iodine intake is high, patients do not necessarily have to follow a strict LID protocol, but can simply be advised to avoid food that could result in excessive iodine intake. A prospective study comparing the ablation success between a strict LID group and less strict LID groups or regular-diet groups is warranted.
Footnotes
Acknowledgment
This research was supported by a grant from Samsung Biomedical Research Institute (#SBRI C-A9-303).
Disclosure Statement
The authors have nothing to declare.