
Abstract
Background:
Lithium is widely used to treat bipolar disorders. Lithium toxicity is generally caused by inappropriately high doses of lithium or impaired lithium excretion. Most lithium is eliminated via the kidneys and, since thyroid hormone increases tubular reabsorption of lithium, thyrotoxicosis could contribute to the development of lithium toxicity. We report a case of severe lithium toxicity that was apparently precipitated by the onset of thyrotoxicosis resulting from silent thyroiditis and dehydration.
Patient Findings:
The patient was a 64-year-old woman who was admitted for muscle weakness in the lower extremities, diarrhea, and palpitations. She had bipolar disorder and was being treated with lithium carbonate, which she discontinued one week before admission. Her circulating lithium levels had been monitored yearly. Early in her admission she was dehydrated and had febrile episodes, paroxysmal atrial fibrillation, and muscle weakness. Initially, fluid therapy was started, but she lost consciousness and had a cardiac arrest for 2 minutes due to prolonged sinus arrest. Chest compression and manual artificial ventilation were performed, and body surface pacing was started. Serum lithium was markedly elevated to 3.81 mEq/L (therapeutic range, 0.4–1.0 mEq/L), and thyroid hormone levels were increased (free triiodothyronine, 8.12 pg/mL; free thyroxine, 4.45 ng/dL), while thyrotropin (TSH) was suppressed (<0.01 μIU/mL). Hemodialysis was performed, and a temporary pacemaker was inserted for severe sinus bradycardia. The serum thyroglobulin was 4680 ng/mL (reference range, <32.7 ng/mL). A TSH receptor antibody test was negative. Glucocorticoid therapy and inorganic iodine (100 mg) were administered and continued until day 11. However, her neurological symptoms deteriorated with floppy quadriplegia and deep coma. She gradually recovered. On day 36, she was discharged without any neurological symptoms or thyrotoxicosis.
Summary:
A 64-year-old woman taking lithium for bipolar disorder developed lithium toxicity in the setting of what seemed likely to be a recent onset of thyrotoxicosis due to silent thyroiditis.
Conclusions:
Thyrotoxicosis may be a contributing cause of lithium toxicity, particularly if it is abrupt in onset and even with cessation of lithium therapy if renal function is compromised. Thyroid function should be assessed immediately in patients with suspected lithium toxicity.
Introduction
Thyroid hormone is known to upregulate transepithelial voltage and Na–K–ATPase activity in the renal tubules, resulting in increased sodium transport (5,6). In 1993, it was reported that reduced lithium clearance and increased tubular reabsorption of phosphate are observed in patients with hyperthyroidism and that these phenomena return to normal in the euthyroid state (7). Therefore, lithium toxicity might easily be observed when patients treated with lithium develop thyrotoxicosis, unless the lithium dose is reduced in order to maintain the serum lithium in the normal range (8). In this report, we present a case of severe lithium toxicity precipitated by thyrotoxicosis resulting from silent thyroiditis. This study was approved by the review board of Fujiyoshida Municipal Hospital (Yamanashi, Japan). Informed consent by the patient was provided.
Patient
The patient was a 64-year-old woman with bipolar disorder who had been taking lithium carbonate for 9 years and had been hospitalized in the past for intractable depression. In recent years, the blood lithium concentration was maintained at a therapeutic level. Lithium concentrations measured annually had been in the range of 0.29–0.65 mEq/L (reference range, 0.4–1.0 mEq/L) before admission. About 3 weeks before admission, she complained of mild diarrhea, malaise, and low-grade fever, symptoms that gradually worsened. A week before admission, she was unable to continue taking lithium carbonate. Two days before admission, she complained of drowsiness and was unable to stand due to weakness of the lower extremities. On the day of admission, she was confused, disoriented, and agitated, and there was a history of fever and chills.
She presented with tachycardia, diarrhea, and dehydration. Her temperature was 39.4°C. The skin turgor was poor; there was no goiter or neck tenderness. Chest examination revealed diffuse expiratory wheezing and late-inspiratory coarse crackling. Muscle tonus and deep tendon reflexes were diminished. Laboratory tests revealed arterial blood gas values as follows: pH 7.41; arterial oxygen tension (PaO2), 73.4 mmHg; arterial carbon dioxide tension (PaCO2), 28.3 mmHg; and HCO3, 17.5 mEq/L. The serum creatinine level was 2.56 mg/dL; blood urea nitrogen concentration was 92.2 mg/dL (Table 1). Chest X-ray showed mild but diffuse pulmonary edema and cardiomegaly. Electrocardiography (ECG) showed atrial fibrillation with rapid ventricular response (Fig. 1A).
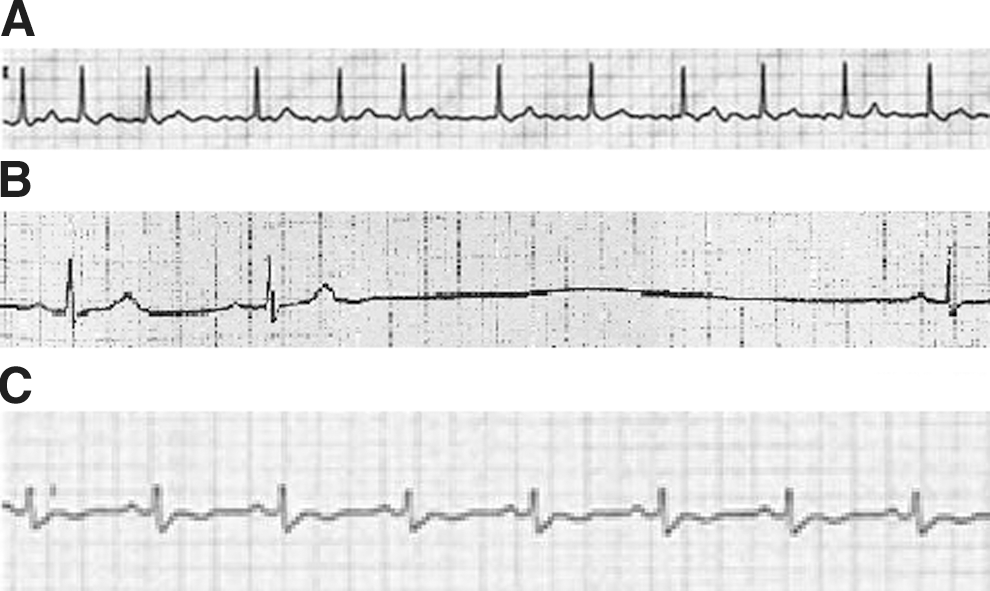
Electrocardiography (ECG) showed
Values presented in
BUN, blood urea nitrogen; RR, reference range; Cre, creatinine; BNP, brain natriuretic peptide; T3, triiodothyronine; T4, thyroxine; TSH, thyrotropin; TRP, tubular reabsorption of phosphate; NA, not available; +, indicates presence of symptom or administration of treatment.
Fluid therapy was started, but her symptoms worsened and coma, quadriplegia, and anuria developed with worsening renal function (Table 1). A repeat chest X-ray showed pulmonary edema. Emergency dialysis was started.
The patient developed severe bradycardia. Continuous isoproterenol infusion therapy was started, but cardiopulmonary sinus arrest occurred and continued for 2 minutes. (Fig. 1B). Cardiopulmonary resuscitation was promptly started, and insertion of a pacemaker helped achieve successful resuscitation (Fig. 2), but coma, quadriplegia, severe diarrhea, and high fever persisted. On day 3, tests revealed increased thyroid hormone levels (free triiodothyronine, 8.12 pg/mL; free thyroxine, 4.45 ng/dL) and a suppressed thyrotropin (TSH) level (<0.01 μIU/mL) (Table 1). A serum lithium concentration obtained from a blood sample predialysis on day 2 was markedly increased to 3.81 mEq/L (reference range, 0.4–1 mEq/L).
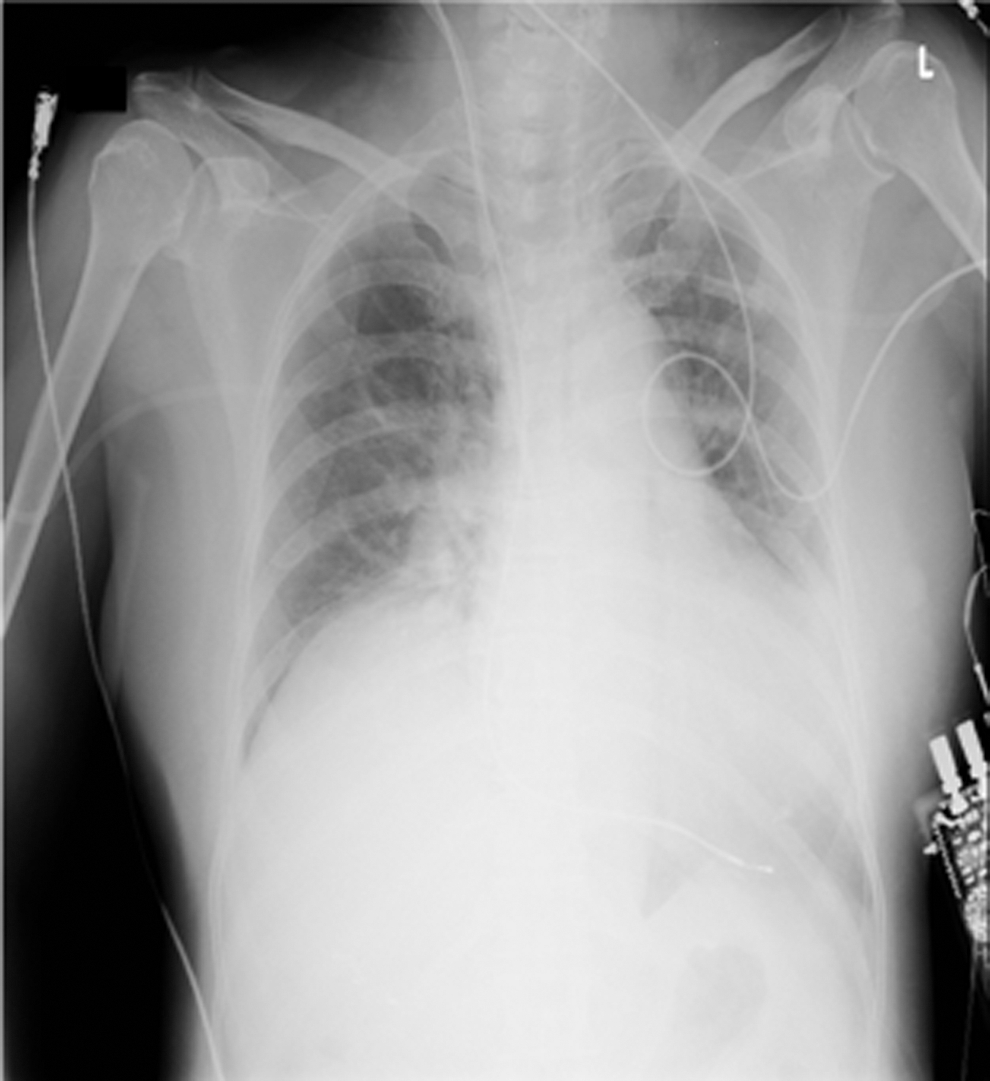
Chest X-ray showing insertion of external pacemaker.
On day 3, renal parameters were almost normal, but hemodialysis was continued until day 7 for lithium removal as no fractional excretion of lithium (FELi) occurred, although tubular reabsorption of phosphate (TRP) significantly increased (Table 1). Dialysis was discontinued after confirmation of diminished lithium levels (Table 1).
As treatment for thyrotoxicosis, prednisolone (20 mg/day) was administered and inorganic iodine (100 mg) was started and continued until day 11 in an effort to block the release of thyroid hormone. An ultrasonogram of the thyroid gland showed mild surface roughening, denoting diffusely decreased intrathyroidal blood flow (Fig. 3). By day 6, the patient's febrile state and severe diarrhea had gradually improved, and her thyroid hormone levels had also decreased (Table 1). Normal sinus rhythm developed. On day 11, tests for anti–thyroid peroxidase antibodies (TPOAb), TSH receptor antibodies (TRAb), and thyroid-stimulating antibodies (TSAb), obtained on day 2, were returned. Both TRAb and TSAb were negative (1.0 IU/L, reference range [RR] <1.0 IU/L; 143%, RR <180%, respectively). TPOAb was 5.3 U/mL (RR <0.3 U/mL). However, serum thyroglobulin (Tg) was markedly elevated to 4680 ng/mL (RR <32.7 ng/mL). A diagnosis of silent thyroiditis was made.
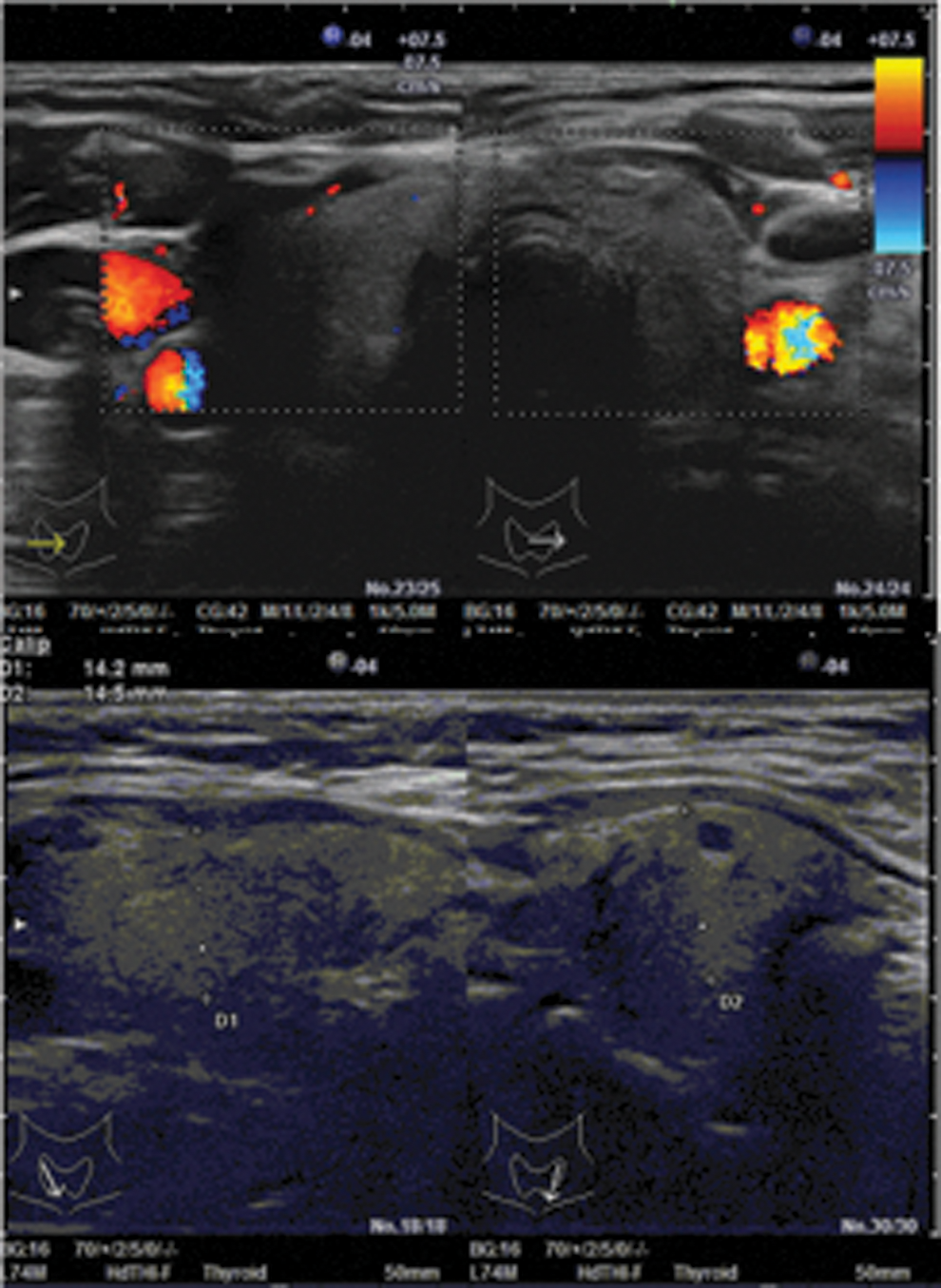
Ultrasonogram of the thyroid gland. Color images available online at
Although thyroid crisis and bradyarrhythmia had improved by day 6, her quadriplegia persisted and her coma deepened. Head computed tomography and magnetic resonance imaging scans showed no abnormalities. An electroencephalogram showed diffuse and global slow waves (Fig. 4). On day 10, her neurological symptoms began to improve and eventually resolved. She was discharged on day 36 without neurological abnormalities, arrhythmia (Fig. 1C), or thyrotoxicosis. Two months after discharge, her general status improved, but she was transferred to a psychiatric hospital for worsening depression. Thyroid function tests were completely normal by this time (Table 1). Her serum Tg level had decreased to a near-normal value of 42.5 ng/mL (Table 1).
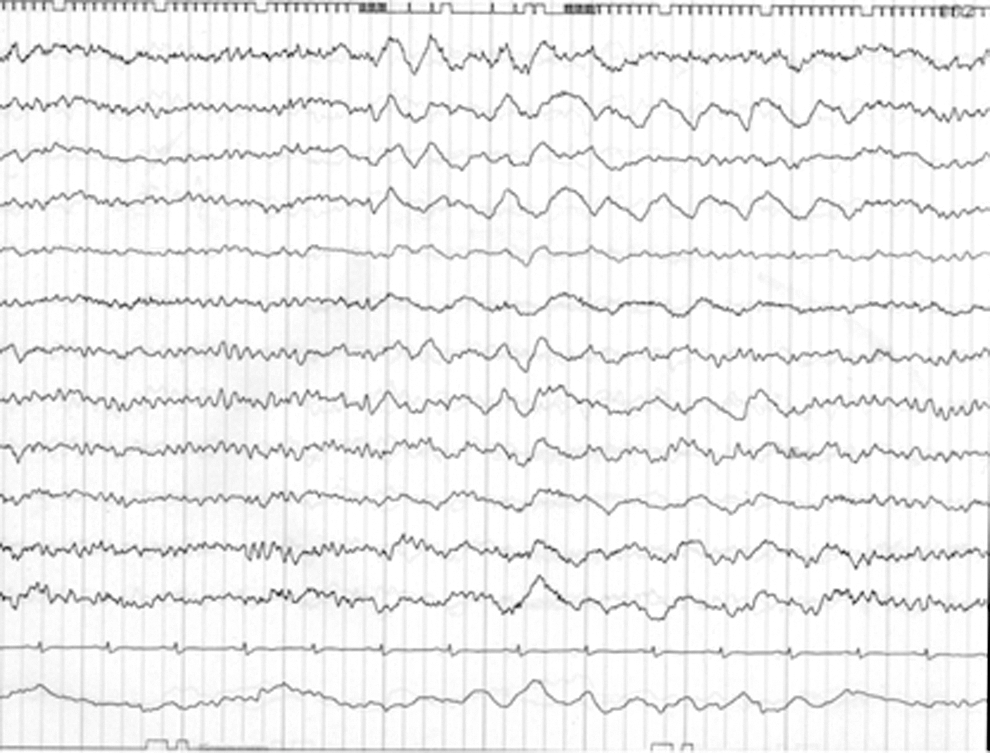
Electroencephalogram on admission.
Discussion
Lithium is the most widely studied and recommended first-line drug for treating bipolar disorder (9,10). The therapeutic range for serum lithium concentrations is narrow, and excessive lithium levels may lead to severe side effects and may be fatal with terminal multisystem dysfunction. The half-life of lithium in the circulation of healthy adults is ∼18 hours. Approximately 95% of lithium and phosphate are filtered by the kidneys (11). In a similar dynamic state to phosphate, 67% of lithium fraction reabsorption in tubules and ∼90% of tubular reabsorption take place in the proximal tubules (3). Volume depletion accelerates the reabsorption of lithium and leads to increased blood concentration (12). The types of lithium poisoning are classified as acute, acute on chronic, and chronic. In our patient, acute on chronic poisoning is an appropriate classification. Acute on chronic lithium toxicity typically presents with gastrointestinal symptoms, such as diarrhea and vomiting, and neurological symptoms, including ataxia, delirium, involuntary movement, and loss of consciousness. Cardiac symptoms are rare, but prolonged QTc intervals and/or severe bradycardia have been reported (13).
Owada et al. (7) reported that increased TRP and decreased FELi were observed in patients with hyperthyroidism and reverted to normal after antithyroid drug therapy. Therefore, it is quite likely that an important reason why the patient's lithium level increased and remained persistently high, particularly early in her course, was her thyrotoxicosis—which was probably recent in onset, as she had features that were consistent with silent thyroiditis. Furthermore, volume depletion after severe diarrhea and acute decompensated heart failure probably led to a decrease in the glomerular filtration rate and restricted lithium removal.
Hypothyroidism may be observed during lithium therapy, in the presence or absence of goiter, due to inhibition of thyroid hormone secretion from thyrocytes (14). However, Miller and Daniels (15) also reported an association between lithium therapy and thyrotoxicosis due to silent thyroiditis. In general, silent thyroiditis is considered a variant form of Hashimoto's thyroiditis, exhibiting positive tests for TPOAb in nearly all patients (16). Interestingly, it has also been reported that positive TPOAb tests may be associated with bipolar disease, as was the case for our patient (17). Volpe (18) considered silent thyroiditis as having a heterogeneous pathogenesis that usually was not of an autoimmune origin. Dang and Hershman (19) reported a case of lithium-associated thyroiditis without positive antithyroid antibodies. In our patient, the presence of TPOAb and the ultrasonography findings showing a rough surface of the thyroid suggested that she had underlying Hashimoto's thyroiditis as a background of her silent thyroiditis. Notably, there are several reports of lithium-associated thyroiditis without positive TPOAb tests (19,20).
It has been suggested that lithium treatment, by its ability to inhibit thyroid hormone secretion, could mask a tendency to developing overt hyperthyroidism, but that hyperthyroidism could become apparrent when lithium is stopped (21). Several hypotheses have been advanced to explain the mechanism of lithium-associated silent thyroiditis, but at this time, they remain conjectural (22 –24).
Only three patients with thyrotoxicosis and lithium toxicity have been reported, all of whom were treated with hemodialysis (Table 2). Oakley et al. (8) reported two cases of lithium toxicity associated with thyrotoxicosis. They suggested that the pathogenesis of thyrotoxicosis in case 1 was silent thyroiditis related to Hashimoto's thyroiditis, and in case 2, it was Graves' disease. Another patient reported by Bandyopadhyay and Nielsen (25) had destructive thyroiditis. In these patients, early dialysis was probably important in preventing serious or even fatal outcomes (Table 2).
Other important aspects of the patient reported here include her atrial fibrillation on admission and the prolonged sinus arrest that occurred later. Her paroxysmal atrial fibrillation at the time of admission was probably due to her thyrotoxicosis. Offerman et al. (13) reported that lithium could cause sinus node dysfunction or sinoatrial block, especially in people older than 60 years. In that study, two bradycardic arrests, including one fatal case, occurred among 282 cases of admitted “lithium exposure cases.” The change of our patient's ECG supports the hypothesis that advanced sinoatrial block or sinus arrest, which appeared to be caused by lithium toxicity against a background of atrial fibrillation, is reversible.
In conclusion, we report the case of a 64-year-old woman who experienced sudden-onset cardiac arrest, quadriplegia, and coma after silent thyroiditis despite cessation of lithium therapy. Thyrotoxicosis itself could enhance reabsorption of lithium from the renal tubules in a setting of prerenal failure. Clinicians should be aware of the increased risk of thyrotoxicosis in lithium-treated patients and the fact that this has the potential to induce lithium intoxication. Patients with features of lithium toxicity should have their thyroid function tested and lithium levels determined as a part of their initial evaluation, even if they discontinued lithium several days earlier. In thyrotoxic patients, lithium use presents added hazards requiring, at the very least, more frequent monitoring of circulating lithium levels.
Footnotes
Acknowledgment
The authors thank Enago (
Disclosure Statement
The authors declare no conflicting interests.