
Abstract
Background:
Thyroid carcinoma with tracheal invasion is uncommon; however, this is significantly more prevalent than primary tracheal tumors. Rare tracheal tumors at the level of the thyroid can be misinterpreted as invasive thyroid cancer upon initial diagnosis. We present a series of tumors within the tracheal wall that were initially misdiagnosed as isolated, but aggressive, thyroid cancer, and later diagnosed to be different histopathologic entities.
Methods:
The series consisted of four women and five men, all but two age 60 or older, who were initially diagnosed with tracheal invasion from differentiated thyroid carcinoma (DTC). Eight had obstructive airway symptoms and one experienced gagging and choking sensations. Preoperatively, the patients underwent fine-needle aspiration (FNA) and imaging studies. A complete resection of the involved airway in combination with the thyroid gland was performed in all patients.
Results:
In this series of patients, the final diagnosis was tracheal stenosis, recurrent laryngeal nerve schwannoma, papillary thyroid carcinoma (PTC) with benign intratracheal thyroid tissue, adenoid cystic carcinoma, and squamous cell carcinoma, each in one patient. Two patients had a tracheal chondrosarcoma, and two patients had collision tumors (PTC with laryngeal squamous cell carcinoma). All patients were misunderstood preoperatively as having isolated DTC with aggressive involvement of the trachea. An accurate diagnosis in these cases was difficult due to misleading FNA readings, thought due to the FNA needle passing through the thyroid before reaching the trachea or a tumor that abuts both structures on imaging. Primary tracheal tumors and a nontumorous lesion, as well as benign thyroidal masses, mimicked invasive thyroid carcinoma in this preoperative setting.
Conclusions:
Various entities other than thyroid cancer can masquerade as invasive thyroid cancer. In patients with an FNA showing thyroid tissue or suggesting PTC, but also have obstructive or other airway symptoms, physician awareness is needed to consider the distinct possibility of a primary tracheal lesion. Obtaining the correct preoperative diagnosis is essential for accurate surgical planning for patients with tracheal tumors.
Introduction
Commonly ultrasonography, magnetic resonance imaging (MRI), or computed tomography is used to diagnose and evaluate the presence of tracheal invasion; however, not all abnormal findings necessarily reflect invasive thyroid carcinoma. A fine-needle aspiration (FNA) biopsy is frequently used to evaluate the presence of thyroid cancer in patients with abnormal physical or radiologic findings. This diagnostic test has a specificity as high as 90.1%, yielding a small, but significant, number of false-positive results (3).
When diagnosing a potential invasive thyroid carcinoma, it is important to keep in mind the wide differential of tracheal tumors. However, to date, there is very little literature on primary tracheal lesions presenting as thyroid carcinoma to aid the surgeon in this diagnosis. Thirteen cases have been previously reported, with the largest two studies containing only four patients (4 –9). Herein, we report nine cases that were originally diagnosed as being highly suspicious for thyroid carcinoma with tracheal invasion, but were later redefined based on final histopathology or FNA. To our knowledge, this is the largest case series of patients presenting with signs and symptoms suspicious for thyroid cancer with tracheal invasion, which were later diagnosed as rare tracheal tumors, a tracheal lesion, collision tumors, or benign thyroid rests.
Methods
A retrospective chart review was performed for nine patients who presented to our senior surgeon with an initial diagnosis of metastatic thyroid cancer with tracheal invasion. Hospital records were reviewed, and data were collected regarding each patient's initial presentation, FNA, imaging studies, and final pathology report. The FNA and/or final pathology for all of these patients showed rare tracheal tumors, benign rests of thyroid tissue, or tracheal stenosis. This research was approved by the Beth Israel Medical Center Institutional Review Board (IRB 044-12). It adheres to all legal requirements of this institution and State.
Results
Nine patients were retrospectively identified who had preoperative findings suggestive of an invasive thyroid cancer of the trachea, but were later found to have a different diagnosis. This cohort included five men and four women, two of which were previously reported in the literature (19, 20). One patient was in her 20s, while the rest were in their sixth through ninth decades of life.
Of the nine patients, eight initially presented with obstructive airway symptoms, while one complained of dysphagia. Three of these patients had a paralyzed vocal fold, and two had palpable neck masses. The two patients with collision tumors both presented with hoarseness. Eight of the nine patients underwent an FNA, of which seven were interpreted as either papillary thyroid carcinoma (PTC) or highly suspicious for a thyroid neoplasm, while the last was interpreted as an adenoid cystic carcinoma. Cross-sectional imaging studies were performed on all patients, which revealed an intraluminal tracheal soft tissue mass adjacent to the thyroid gland. The initial interpretation of the radiographic images included invasive thyroid cancer. All patients were later found to have a different histologic diagnosis than what had been presumed preoperatively. The final diagnoses in this series (Table 1) were tracheal stenosis (n=1) with unknown etiology, recurrent laryngeal nerve schwannoma (n=1), thyroid cartilage chondrosarcoma (n=1), tracheal chondrosarcoma (n=1), collision tumor–PTC and laryngeal squamous cell carcinoma (n=2), PTC with benign intratracheal thyroid tissue (n=1), adenoid cystic carcinoma (n=1), and squamous cell carcinoma (n=1).
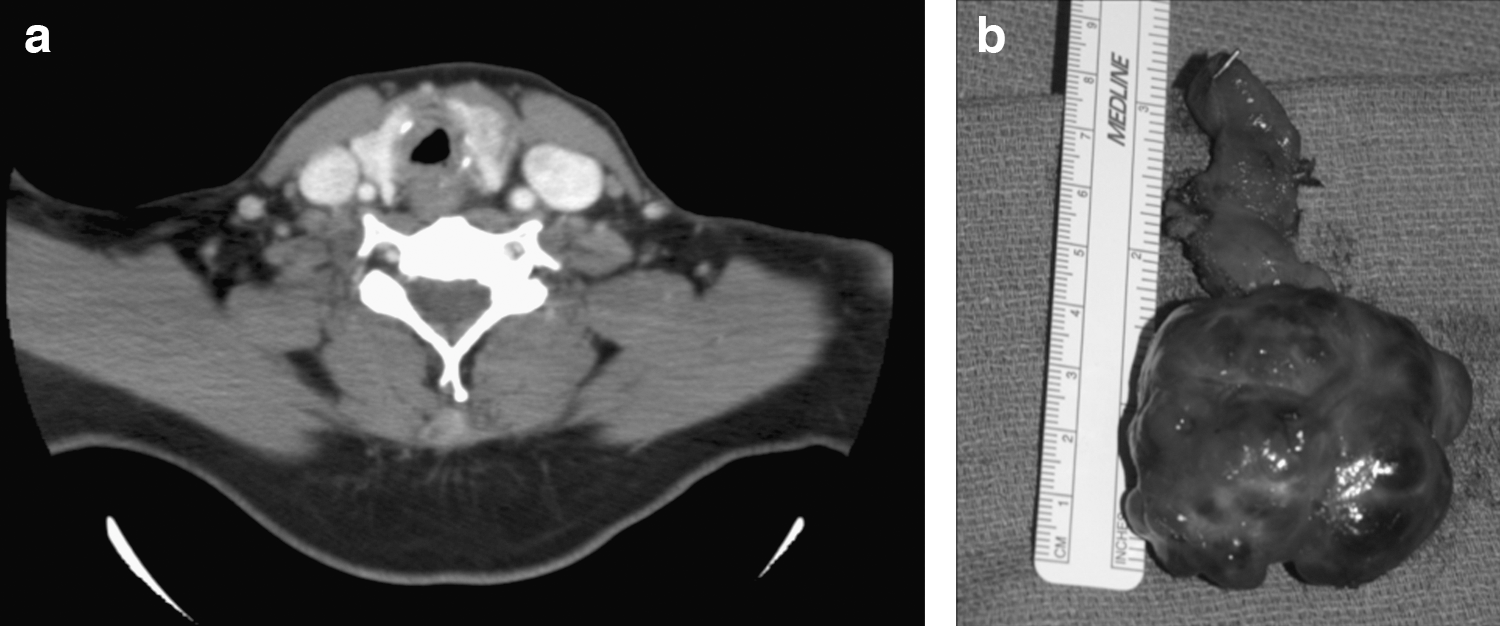

Axial CT of the neck with contrast shows a bulky lesion of the right lobe of the thyroid gland with destruction of the right one-half of the cricoid cartilage and associated paralaryngeal extension (corresponds with patient 6 from Table 1).
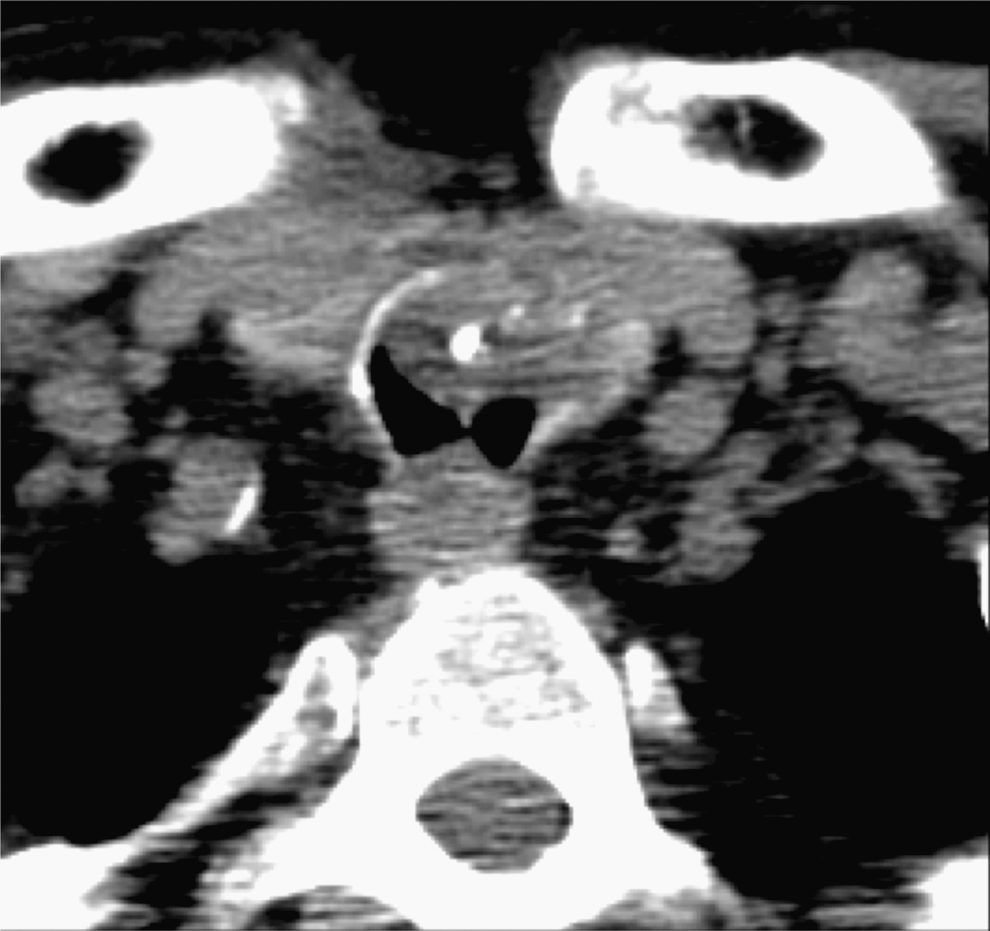
Axial CT of the neck without contrast shows a bulk soft tissue mass with internal calcification involving the left lateral and anterior walls of the cervical trachea with both extra- and intraluminal components (corresponds with patient 7 from Table 1).
AW, airway; ca, cancer; F, female; M, male; ND, neck dissection; Pt, patient; PTC, papillary thyroid carcinoma; SCCA, squamous cell carcinoma; TEP, tracheoesophageal puncture; TL, total laryngectomy; Tx, thyroidectomy.
Discussion
The correct distinction of invasive thyroid cancer from other pathological entities is crucial for appropriate preoperative and operative surgical planning. The prognosis for survival is excellent among patients with benign processes such as a tracheal thyroid rest, tracheal stenosis, and a recurrent laryngeal nerve schwannoma, as compared to those with thyroid carcinoma invading the trachea. Nevertheless, these patients with benign intratracheal masses would have still required a partial resection of the trachea due to obstructive airway symptoms with the exception of patient 5. This patient presented with symptoms of gagging and choking, and would have undergone a thyroidectomy for PTC, without a tracheal resection, if the correct diagnosis had been identified before surgery. Tracheal resections were necessary for the remainder of the patients in this study.
Adult tracheal tumors are exceedingly rare. A review of tracheal tumors revealed that 80%–90% are malignant (10). The reported incidence of primary tracheal tumors is two cases per million, per year (11). The most common primary malignant tumors are squamous cell and adenoid cystic carcinoma (12); however, a variety of other benign and malignant neoplasms have been reported (Table 2). The incidence of thyroid carcinoma is 110 per 1 million per year (13), with as low as 1% of patients having tracheal involvement (1). Therefore, secondary invasion of the trachea by invasive thyroid carcinoma is significantly more prevalent than primary tracheal tumors (14). This can lead clinicians astray in the initial findings of patients presenting with tracheal masses.
Boldface indicates patient diagnosis on final pathology within this case series.
In cases in which there is a mass compressing or invading the trachea, patients often present with similar obstructive airway symptoms regardless of the etiology of the mass. Physical findings that raise the suspicion for significant laryngotracheal involvement include hoarseness and signs of airway narrowing. When there is only tracheal wall involvement without compromise of the lumen or the recurrent laryngeal nerve, invasion may be diagnosed preoperatively with visualization using bronchoscopy or through imaging. Bronchoscopic findings suggestive of tracheal involvement include localized mucosal redness, telangiectasia, mucosal elevation, mucosal edema, or mucosal erosion (15). Ultrasonography may also be used, and in one report by Tomoda et al., the sensitivity and specificity of ultrasonography for tracheal invasion were 91% and 93%, respectively (16). Wang et al. also found that tracheal invasion was evident on MRI if the images demonstrated soft tissue signal in the tracheal cartilage, an intraluminal mass, or a tumor abutted a circumference of 180° or more of the trachea (17).
Laryngotracheal invasion by a thyroid carcinoma is a negative prognostic indicator for overall survival as demonstrated by McCaffrey (18). Identifying laryngotracheal invasion and determining the extent of disease play a major role in the preoperative discussion with the patients and their surgical planning. It is generally accepted that luminal involvement of the trachea will require either window or complete circumferential resection with primary closure. When only partial thickness of the tracheal wall is involved, there is no consensus as to the most appropriate surgical approach, with a tracheal shave procedure representing a more conservative approach to surgical management.
In the seven cases where FNAs were read as highly suspicious for thyroid carcinoma or as PTC, five were incorrectly diagnosed preoperatively. The two that did demonstrate PTC on final pathology were found to have collision tumors in conjunction with squamous cell carcinoma. Therefore, it is important to recognize that the cytopathological interpretation may be misguided if the path of the needle used to perform the FNA took a course through a portion of the thyroid gland, thereby including thyroid cells in the specimen. If the biopsy needle did pass though the thyroid gland to reach the mass, it should be reported with the sample, as thyroidal tissue present in the sample may confuse the diagnosis. Since the preoperative needle aspiration passed through thyroid tissue, the benefit of thyroglobulin assays is diminished and potentially misleading.
In conclusion, while the majority of cases of tracheal invasion at the level of the thyroid appear to be aggressive thyroid cancer, it is important for the clinician to consider alternative diagnoses. We have presented a series of cases of patients with intraluminal neoplasms that mimicked invasive thyroid cancer, but ultimately proved to be caused by a different pathologic etiology. Considering a wide differential and obtaining a correct preoperative diagnosis should benefit the patient with a more precise, targeted resection of the tumor, as well as the tracheal component. This report is intended to provide the clinician with an awareness of the range of histopathologic entities that may be misinterpreted as invasive thyroid cancer.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.