
Abstract
Background:
It is believed that chemotherapy (ChT) is ineffective in papillary thyroid carcinoma (PTC). The aim of our retrospective chart review was to find out if neoadjuvant ChT before thyroid surgery had any effect on the size of primary tumors in patients with PTC.
Methods:
The study included 16 patients (13 women, 3 men; median age 63.5 years) with PTC, who were treated with neoadjuvant ChT from 1988 to 2005. Poorly differentiated PTC, classical PTC, a follicular variant of PTC, and a Hürthle cell variant of PTC were diagnosed in 5, 5, 3, and 3 cases, respectively. The mean tumor diameter was 9.67 cm. Seven patients had a pT4 tumor. Regional and distant metastases were detected in 10 and 7 patients, respectively. ChT consisted of vinblastine in 11 cases, vinblastine with adriamycin in 2 cases, and other schedules in 3 cases. Four patients were also treated with preoperative external irradiation.
Results:
Altogether, 40 cycles of ChT were given. After ChT, the tumor size decreased in all 16 patients: by >50% in 7 (44%) patients and by <50% in 9 patients. R0, R1, and R2 resection was performed in 2, 10, and 4 cases, respectively. The median survival time of our patients was 88 months. Six patients are still alive; two died of causes not related to carcinoma, while eight patients died of PTC.
Conclusions:
Neoadjuvant ChT before thyroid surgery may be effective in patients with locally advanced PTC. After neoadjuvant ChT, in 44% of patients, the tumor size decreased by >50%.
Introduction
Slovenia is in the region of endemic goiter, and adequate iodination of salt to prevent goiter has only been used for the last 13 years (4,5). Before adequate iodination of salt, a high goiter prevalence was found in the population (4). Searching for thyroid carcinoma among the goiter population could be compared to searching for a needle in a haystack (4). Therefore, it was not surprising that, in Slovenia, there used to be patients with locally advanced PTC (6). In some of them, the tumor invaded the surrounding organs; therefore, only mutilating surgery would have been possible. Based on our good experience with preoperative ChT in patients with inoperable head and neck carcinoma (7), anaplastic thyroid carcinoma (8), and follicular or Hürthle cell thyroid carcinoma (9), a nontoxic neoadjuvant ChT was used in 16 patients with locally advanced PTC. The aim of our retrospective study was to determine if neoadjuvant ChT before thyroid surgery had any effect on the size of the primary tumor in patients with PTC.
Patients and Methods
Patients
Data were collected on patients with PTC treated at the Institute of Oncology in Ljubljana, Slovenia, in the years from 1976 to 2006. During this period, 1207 patients were treated for PTC at the Institute. The study included 16 patients (13 women, 3 men; median age 63.5 years) among 801 patients with PTC, who were treated with neoadjuvant ChT from 1988 to 2005. Poorly differentiated PTC, classical PTC, a follicular variant of PTC, and a Hürthle cell variant of PTC were diagnosed in five, five, three, and three cases, respectively. The locoregional tumor caused symptoms (compression on airway, hoarseness, dysphagia, and respiratory distress) in 12 cases. In all patients in the primary ChT group, the tumor was considered inoperable because of infiltration into the surrounding tissues. Altogether, 12 patients were treated with neoadjuvant ChT, while 4 patients were treated with preoperative ChT and external irradiation. Surgery was performed whenever the tumor was reduced after ChT and/or external irradiation, and the surgeon judged it resectable. The median interval between the beginning of ChT and a surgical procedure was 28 days (range 7–161 days).
Data regarding the patients' sex, age, history and extent of disease, morphological characteristics, therapy, locoregional control, and survival were collected. The tumor size, presence of regional or distant metastases, and residual tumor after surgery were assessed by the TNM clinical classification according to the Union for International Cancer Control (UICC) criteria (10) from 2009. The patients' characteristics and therapy of patients in the ChT group are presented in Table 1.
ChT, chemotherapy; RAI, radioactive iodine.
The study was approved by the Institutional Review Board and the appropriate ethics committee and performed in accordance with the ethics standards laid down in an appropriate version of the 1964 Declaration of Helsinki. Our study was conducted with the understanding and consent of the involved human subjects.
Tumor morphology
All histological slides for this study were reviewed by one pathologist. The tumor differentiation was determined by the grading system of Akslen (11) as follows. Well-differentiated tumors had no extensive vascular invasion, nuclear atypia, or tumor necrosis. Conversely, the tumor was classified as a poorly differentiated tumor if extensive vascular invasion and/or nuclear atypia and/or tumor necrosis was evident.
Surgery
It is well known that a natural course of PTC is not uniform. Surgery has been considered as the most effective treatment of PTC, and has therefore remained its mainstay. Therefore, surgical treatment was performed whenever possible. Each case of advanced PTC is presented to a team of physicians at our institution, who take part in treating thyroid carcinoma patients: a surgical oncologist, a specialist in nuclear medicine and a radiotherapist. The treatment depends on the decision of the team. Whenever needed, other specialists were also included in diagnostics and treatment (cytopathologist, pathologist, radiologist, medical oncologist, neurosurgeon, orthopedic surgeon, and thoracic surgeon). Our patients were treated with repeat surgery, RAI, external irradiation, ChT, or a combination of these modalities as circumstances dictated. Of course, over the 17-year period, various physicians with various preferences of treatment were a part of our thyroid team. Therefore, it is understandable that various proportions of patients were treated with RAI ablation of the thyroid remnant, external irradiation, ChT, and RAI therapy after L-thyroxine withdrawal or using recombinant human thyrotropin (TSH).
ChT and radiotherapy
Various chemotherapeutic schedules were used for PTC in preoperative and metastatic settings over the period of 17 years as a part of the research protocol sponsored by the Slovenian Ministry of Science and Technology (principal investigator M. Auersperg). The treatment was started with a schedule with relatively low toxicity (i.e., vinblastine 2 mg over 12- or 24-hour infusions in 1000 mL of 0.9% saline). Vinblastine administered according to this schedule (i.e., low dose and long infusion) does not cause nausea, vomiting, alopecia, cardiomyopathy, or hematopoietic side effects. However, it may cause cardiac arrhythmia, so we did not use vinblastine in patients with ischemic heart disease. None of our patients from this study group experienced any cardiac toxicity. Vinblastine was used in the majority of cases from the present study, because it is a potent modulator of cellular kinetics in poorly differentiated carcinoma as already reported by Auersperg et al. (8). If the tumor size increased, more aggressive schedules were used. As an alternative to vinblastine, 20 mg of adriamycin in 2-hour infusion was used once a week. In such doses, adriamycin does not cause nausea, vomiting, alopecia, hematopoietic side effects, or cardiomyopathy.
The local effect of ChT used to be assessed by clinical findings only. The size of the primary tumor was measured clinically each day during the first week after ChT and once a week thereafter during the visit to the outpatient clinic and before the next cycle of ChT. Resectability of a tumor was clinically evaluated by a surgeon once a week. The extent of the disease and possible effectiveness of ChT were evaluated before the first ChT and before a surgical procedure by clinical examination, X-ray, computed tomography (CT) scan, ultrasonography, and/or serum thyroglobulin (Tg) concentration measurements as circumstances dictated. The overall effect of ChT on the primary tumor size (product of the longest perpendicular diameters) was defined as (i) progression if the tumor enlarged; (ii) stagnation if the tumor size remained the same or decreased by <50%; (iii) regression if the tumor size decreased by 50%–99%; and (iv) complete response if the tumor disappeared.
According to our study protocol, if the primary tumor progressed after ChT, the patient was treated with a combination of external irradiation and ChT. Four patients had preoperative external irradiation with a median dose of 33 Gy (range 17.5–39.6 Gy) in 2–4 weeks. In two patients, it was performed after nasotracheal intubation because of respiratory distress caused by a compression of the tumor on the trachea. In another patient, an intubation was necessary one week after the initiation of external irradiation with a daily dose of 2.5 Gy. Altogether, 12 patients had preoperative and/or postoperative external irradiation of the neck and superior mediastinum with a total tumor dose of 27.7–60.4 Gy (median 50.4 Gy). The radiation field included the entire neck up to the level of the mastoid process, bilateral supraclavicular and infraclavicular regions, and the superior mediastinum using a 60Co unit and two opposed fields.
Follow-up and survival
For all patients, follow-up check-ups were performed at the Institute at least once a year. They consisted of obtaining a thorough medical history, a physical exam, and determination of the serum Tg concentration. Whenever the Tg concentration was elevated, imaging (X-ray, ultrasound, RAI scintigraphy, CT, magnetic resonance, bone scintigraphy, and/or positron-emission tomography–CT scan) was performed to determinate the location and extent of residual disease or suspected recurrence.
Survival was defined as the period from the first day of treatment with preoperative ChT to the death or last follow-up of the patient. The disease-free interval was defined as the period from the beginning of ChT to a recurrence or to the last follow-up. The disease-free interval excludes those patients with distant metastases at initial presentation.
Statistical analysis
Characteristics of patients and treatments were compared by Fisher's exact or chi-square test where appropriate. The age of the patients and the size of their tumors were compared using a Mann–Whitney rank-sum test. Survival and disease-free intervals were compared using a log-rank test. Survival curves were calculated according to the Kaplan–Meier method (12). For statistical analysis, SPSS 16.0 for Windows was used.
Results
In the 16 patients receiving neoadjuvant ChT, the median tumor diameter was 9 cm. Extrathyroid growth of tumor was present in 13 surgical specimens. Distant metastases were detected on admission in seven patients. All had single-organ metastases; the lung was involved in six patients and the skeleton in one patient.
ChT consisted of vinblastine only in 11 cases, vinblastine with adriamyin in 2 cases, or other ChT regimens in 3 cases. Altogether, 40 cycles of ChT were given. After ChT, the tumor size decreased in all 16 patients: by >50% in 7 (44%) patients and by <50% in 9 patients. In none of our patients were there any ChT-related side effects.
Histopathology revealed that ChT (i.e., wide areas of tumor necrosis) was present in two patients (12.5%). A decrease in the serum concentration of Tg was not observed in any of our patients after ChT and/or external irradiation,.
Resection of the tumor after primary ChT and/or external irradiation could be performed in all of the patients in the study. In patients treated only with ChT, the median interval between ChT and surgery was 4 weeks. Surgery was performed 4–13 (median 9) weeks after external irradiation.
Transient and permanent hypoparathyroidism occurred in three (19%) and one (6%) patients, respectively. Preoperative and permanent vocal cord palsy was present in four (25%) patients. A temporary tracheostomy was performed in one patient, while in another patient, a permanent tracheostomy and jejunostomy were performed because of preoperative mediastinitis and tumor extension to the trachea and esophagus.
There was no correlation between the effect of ChT and disease-free interval or cause-specific survival. Table 2 presents data about the effect of ChT, clinicopathological features, and the treatment. The 5- and 10-year cause-specific survival of patients treated with neoadjuvant ChT was 75% and 40% respectively. Figure 1 presents the effects of ChT and disease-free interval; Figure 2 presents the effects of ChT and cause-specific survival time.
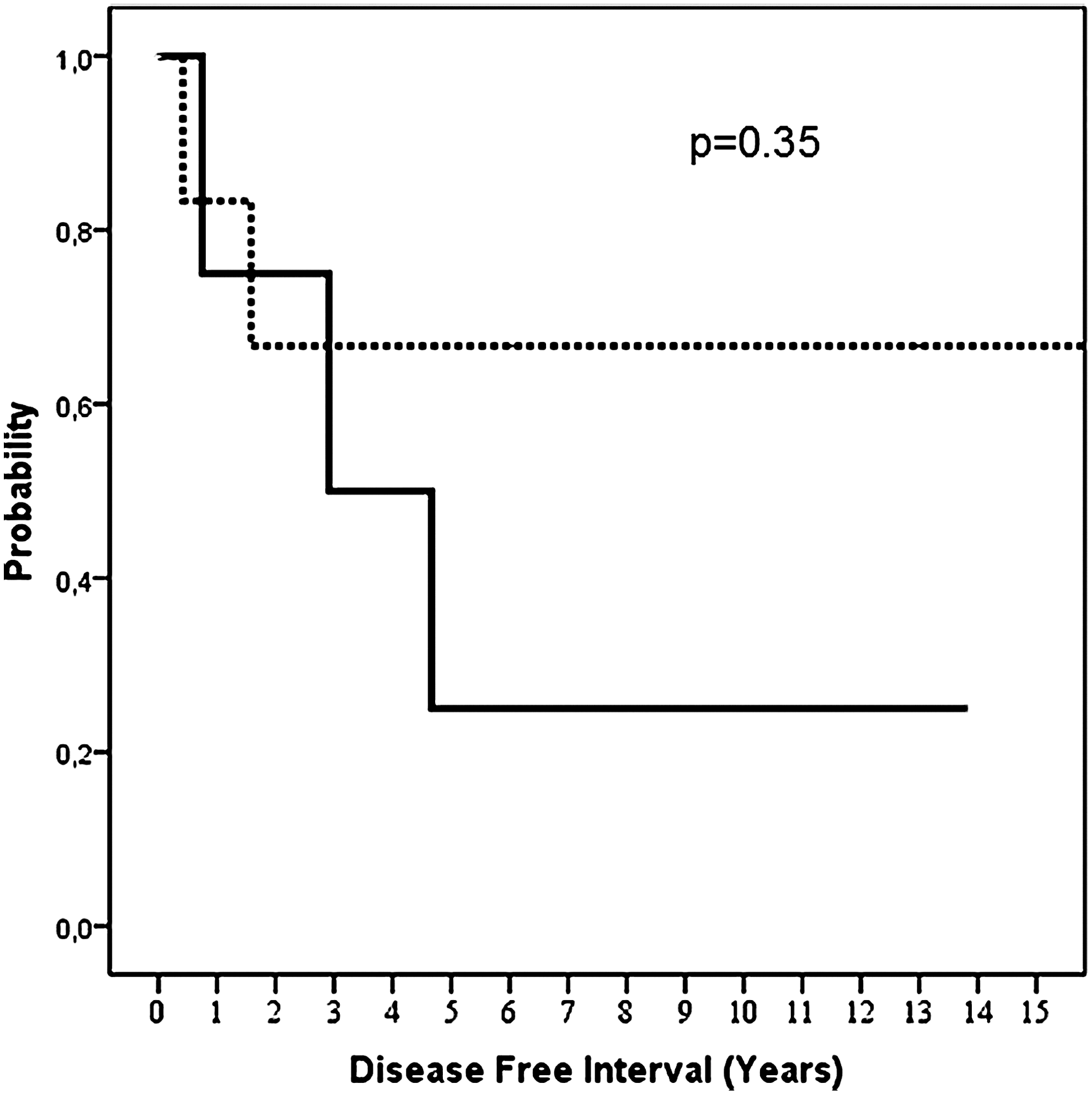
Disease-free interval and effect of chemotherapy (ChT) (bold line, effect 50%–99%; dashed line, effect <50%).
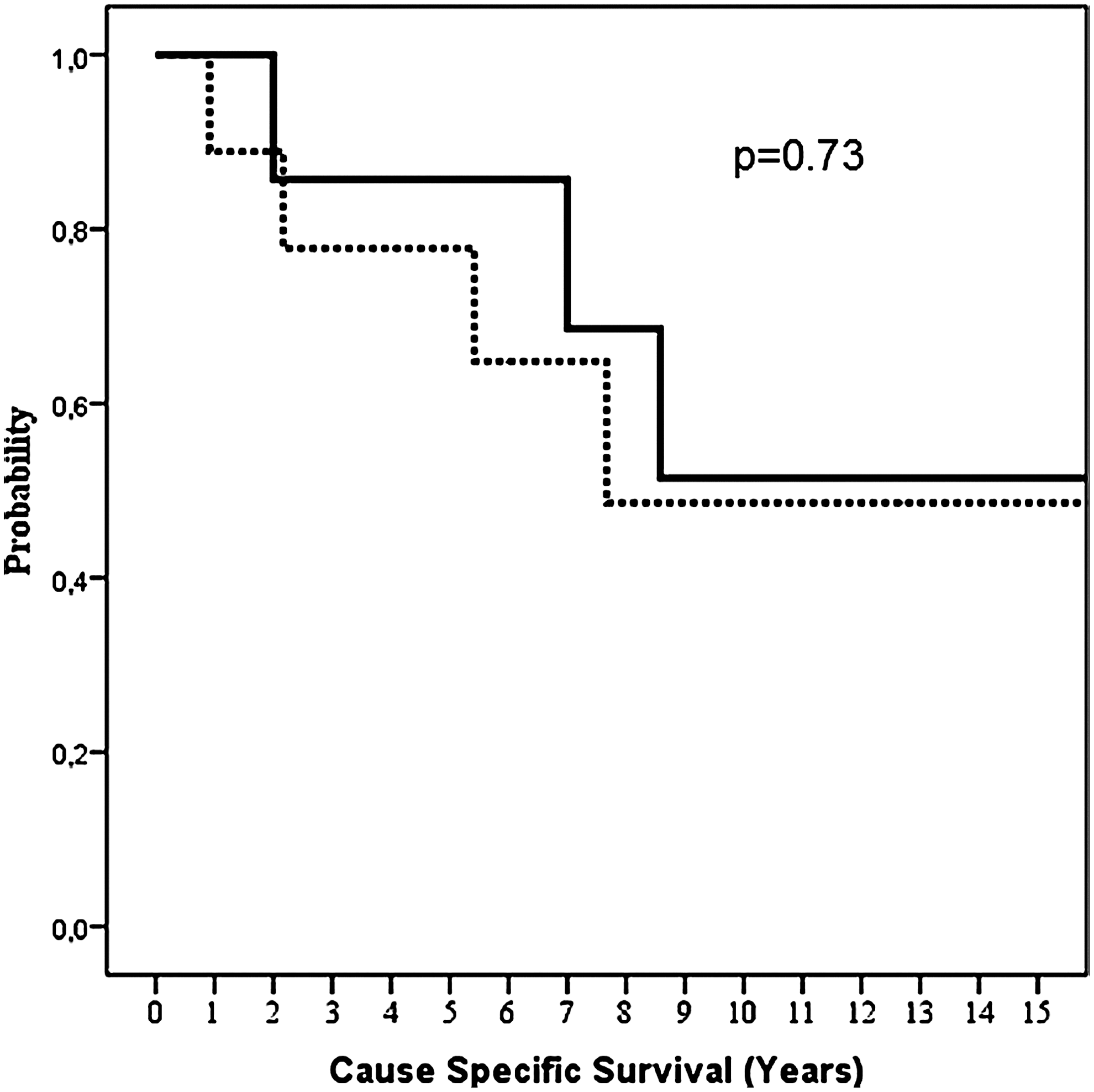
Cause-specific survival and effect of ChT (bold line, effect 50%–99%; dashed line, effect <50%).
By the end of the study, six patients were alive, and two of them had no evidence of disease. Two patients died of other causes, while eight patients died of PTC. Among the latter patients, five died of distant metastases, and two succumbed to a locoregional recurrence and distant metastases, while one died of a locoregional tumor recurrence.
The median survival time of patients without distant metastases and with distant metastases was 103 (range 11–240) and 72 (range 24–213) months, respectively. The 5- and 10-year cause-specific survival times of patients with metastases were 60% and 28%, respectively.
The 5-year disease-free interval was 44%. Among the nine patients who were initially without distant metastases, locoregional recurrence and distant metastases occurred in 2 and 4, respectively.
Discussion
A neoadjuvant setting is a logical choice to prove that ChT has an effect on PTC. This has many advantages in comparison to a metastatic setting. However, the vast majority of studies about the effectiveness of ChT in differentiated thyroid carcinoma were performed in a metastatic setting, many times in patients pretreated with RAI and/or external irradiation.
Typically, the numbers of patients in studies about ChT in differentiated thyroid carcinoma are very small (22 patients or less) (8,9,13 –21). To our knowledge, our study is one of the largest published series of patients with ChT in PTC. We report on 16 patients with PTC who were treated with neoadjuvant ChT. In our study, altogether, 40 cycles of neoadjuvant ChT were given, and the tumor size decreased by >50% in seven patients (44%). Our patients with PTC and metastases had a comparable response rate (i.e., 43%) to that of patients treated with high-dose adriamycin in a metastatic setting, which is from 30% to 40% (20). However, in contrast to our patients who did not have any side effects after ChT, those treated with high-dose adriamycin experienced high-grade toxicity (20). Santini et al. (13) reported that after ChT consisting of carboplatinum and epirubicin, all of their patients had alopecia and some of them also experienced major toxicity.
There are several limitations in our retrospective study. It was nonrandomized, and different ChT schedules were used. Another limitation of our study is that it is not known how long the effect of ChT lasts. The patients had a surgical procedure as soon as a tumor was considered operable, and the median interval between the beginning of ChT and the surgical procedure was only 28 days. Moreover, long-lasting locoregional tumor control was a consequence of multimodal treatment consisting of, besides ChT, also preoperative and/or postoperative external irradiation in 75% of patients and the use of RAI in 88% of patients.
Santini et al. reported a 37% response rate after a combination of carboplatinum, epirubicin and TSH stimulation in 14 patients with poorly differentiated thyroid carcinoma and RAI-resistant diffuse lung metastases (13). Their rationale for TSH stimulation was that cell-cycle-active antineoplastic drugs are most effective in tumors for which the growth fraction is maximal (13). As in theirs, our treatment strategy also has its basis in cell-cycle kinetics (22,23). In one of our former studies, Auersperg et al. reported that sequential fine-needle aspiration biopsies of tumors were performed for monitoring the drug-induced changes in tumor cells after ChT (8). Cytomorphological studies and DNA measurements were performed in 34 patients with poorly differentiated thyroid carcinoma, and six of them had PTC. During the period of accumulation of cells in the S or G2/M phases, drugs particularly effective in the respective phases were used (8). However, for the purposes of the present study, ChT was applied in empirical schedules based on the results of a study reported by Auersperg et al. (8).
There is an important difference in cytostatic drugs and their dosage between those that were used for differentiated thyroid carcinoma in the reports from the literature (14 –21) and ChT schedules used in our patients. In 1977 O'Brian et al. (17) had already observed that low doses of ChT may also be effective in differentiated thyroid carcinoma. Based on our good experience in the treatment of other types of carcinomas (7 –9), vinblastine in low doses and long infusions was used in our patients from the present study. This schedule was selected, because it has a low degree of toxicity and it is effective (7 –9). Of note, none of our patients with PTC treated with vinblastine reported any side effects. Moreover, a majority of patients noticed a relief of symptoms related to local tumors and/or pain caused by bone disease in a few days. Therefore, we conclude that a low dose of vinblastine in a long infusion is a safe treatment, which can be effective in PTC.
Our study is comparable to the study published by Kim and Leeper (14), who treated their patients who had inoperable primary thyroid carcinomas. They used a low dose of adriamycin 10 mg/m2 once weekly and external irradiation of the neck region and superior mediastinum in patients with PTC or follicular thyroid carcinomas. They achieved a response in 20/22 patients and a long-lasting local effect in 77% of cases (14). Our multimodal approach in patients with initially inoperable follicular or Hürthle thyroid carcinoma was even more effective (9). Locoregional control of the disease was achieved in 97% and only one of 29 patients succumbed to a locoregional recurrence and distant metastases (9). Also, our treatment results in inoperable PTC are superior to data reported by Kim and Leeper. Long-lasting locoregional control was achieved in 82% of our cases. Only three of our patients with PTC had a locoregional recurrence, and two of them succumbed to concomitant progression of distant metastases. Neoadjuvant ChT followed by multimodal treatment likely resulted in longer survival times in our patients with PTC in comparison to patients reported by Kim and Leeper (14) with median survival times of 88 and 48 months, respectively. Based on results of our present study we think that, in patients with inoperable primary thyroid carcinoma, external irradiation in combination with ChT should only be reserved for those cases in which there is tumor enlargement after neoadjuvant ChT.
Ito et al. found, in patients with PTC and metastatic disease, that an age of 55 years or older (24,25), massive extrathyroid extension (24,25) and a tumor size larger than 4 cm (25) were independent prognostic factors that correlated with a shorter survival time. The 5-year cause-specific survival time in patients age 55 years or older, or who had massive extrathyroid extension, or whose tumor sizes was larger than 4 cm, was 60%, 56%, and 58%, respectively (25). Similarly, the majority of our patients with distant metastases had bad prognostic factors: all seven had tumors larger than 5 cm (median 8 cm), five of them were older than 55 years of age, and two had massive extrathyroid extensions. However, the 5- and 10-year cause-specific survival times of our patents with initially distant metastases and locoregionally advanced PTC were 60% and 28%, respectively. We believe that this long survival time despite bad prognostic factors is a consequence of better systemic treatment of this selected group of patients in comparison to the patients reported in the literature (25,26). Even in the patients reported from the Memorial Sloan-Kettering Cancer Center in New York, the 10-year survival time of patients with metastatic PTC was only 21% (26).
We believe that ChT should be a part of the treatment of patients with advanced PTC, because, many times, a primary tumor or metastases also consists of poorly differentiated cells. As RAI therapy is effective in well-differentiated thyroid tumors (27), ChT may be effective in poorly differentiated components of tumors (8,13). Different, possibly effective, systemic treatments, which have a potential influence on various types of tumor cells, should be used in advanced PTC as already shown in follicular or Hürthle cell thyroid carcinoma (9). External irradiation in patients with ChT-resistant tumors may increase the resectability rate. A long-lasting locoregional control rate of 83% in our patients with very advanced PTC confirms that our multimodal treatment approach is effective.
Conclusion
Neoadjuvant ChT may be effective to decrease the tumor size in PTC before thyroidectomy and tumor resection. After neoadjuvant ChT, the tumor size decreased by more than half in 44% of patients studied in this series.
Footnotes
Acknowledgment
The article was supported by a research program, P3-0289, by the Ministry of Higher Education, Science and Sport of Slovenia.
Disclosure Statement
The authors declared that no competing financial interests exist.