
Abstract
Background:
No study has examined the malignancy rate and the color Doppler pattern of solid, round, isoechoic thyroid nodules (SRINs) without coexistent malignant sonographic features. We aimed to assess the cytopathological results and color Doppler patterns of SRINs through a prospectively designed study.
Methods:
Between January and December 2010, a total of 727 patients underwent consecutive ultrasound (US)-guided fine-needle aspirations (US-FNAs), and 27 patients who had SRINs with the largest diameter ≥5 mm at US were prospectively selected and enrolled in the study. The color Doppler pattern of each nodule was classified into one of four categories: scant, peripheral, central, or mixed type.
Results:
Out of 27 SRINs, 14 were histopathologically confirmed, and 13 were nonsurgically diagnosed by 2 consecutive US-FNAs. Among the 14 surgical SRINs, there were 7 papillary thyroid carcinomas, 2 follicular adenomas, and 5 nodular hyperplasias. All 13 nonsurgical SRINs were finally determined to be benign on the basis of results of US-FNAs and/or long-term US follow-up; thus, the malignancy rate of the SRINs was 25.9% (7/27). There was no significant correlation between the color Doppler pattern and the malignancy rate of SRINs.
Conclusion:
We recommend that US-FNA should be performed for SRIN to rule out malignancy, regardless of its color Doppler pattern.
Introduction
To the best of our knowledge, no study has examined the malignancy rate of solid, round, isoechoic thyroid nodules (SRINs) without malignant sonographic features and calcifications. In this study, we assessed the cytopathological results of SRINs and their color Doppler patterns.
Materials and Methods
Patients
From January to December 2010, a single radiologist (D.W.K., ≥3000 thyroid US scans/year and ≥1200 US-guided fine-needle aspirations [US-FNAs]/year for 8 years) performed a thyroid US and consecutive US-FNAs to diagnose thyroid nodules with the largest diameter ≥5 mm in 727 patients (622 females and 105 males; age range, 8–87 years; mean age, 50.2 years) and prospectively selected SRINs. Among them, 27 patients (24 women and 3 men; age range, 19–79 years; mean age, 49.0 years) who had a SRIN on thyroid US were prospectively selected in this study: a SRIN was defined as a thyroid nodule with a round shape (ratio of anteroposterior diameter to either transverse or longitudinal diameter between 0.9 and 1), a solid composition (purely solid or predominantly solid with a cystic component, accounting for <10% of the total volume), isoechogenicity, no malignant sonographic feature, and no calcification. Written informed consent was obtained from all patients and the study was approved by the Institutional Review Board (IRB: 11-130).
Thyroid US
Thyroid US was performed using a high-resolution US instrument (iU 22; Philips Healthcare, Andover, MA) equipped with a 5–12-MHz linear probe. During the color Doppler US examination, a low-pulse repetition frequency, 700 Hz, and constant Doppler gain were used. The color Doppler pattern of thyroid nodules was subjectively evaluated under a real-time examination and classified as follows: scant type (only a few vascular spots), peripheral type (the vascular signal in the peripheral portion was higher than that in the central portion), central type (the vascular signal in the central portion was higher than that in the peripheral portion), and mixed type (the vascular signal in the peripheral portion was similar to that in the central portion). Examples of the different classes are presented in Figure 1.
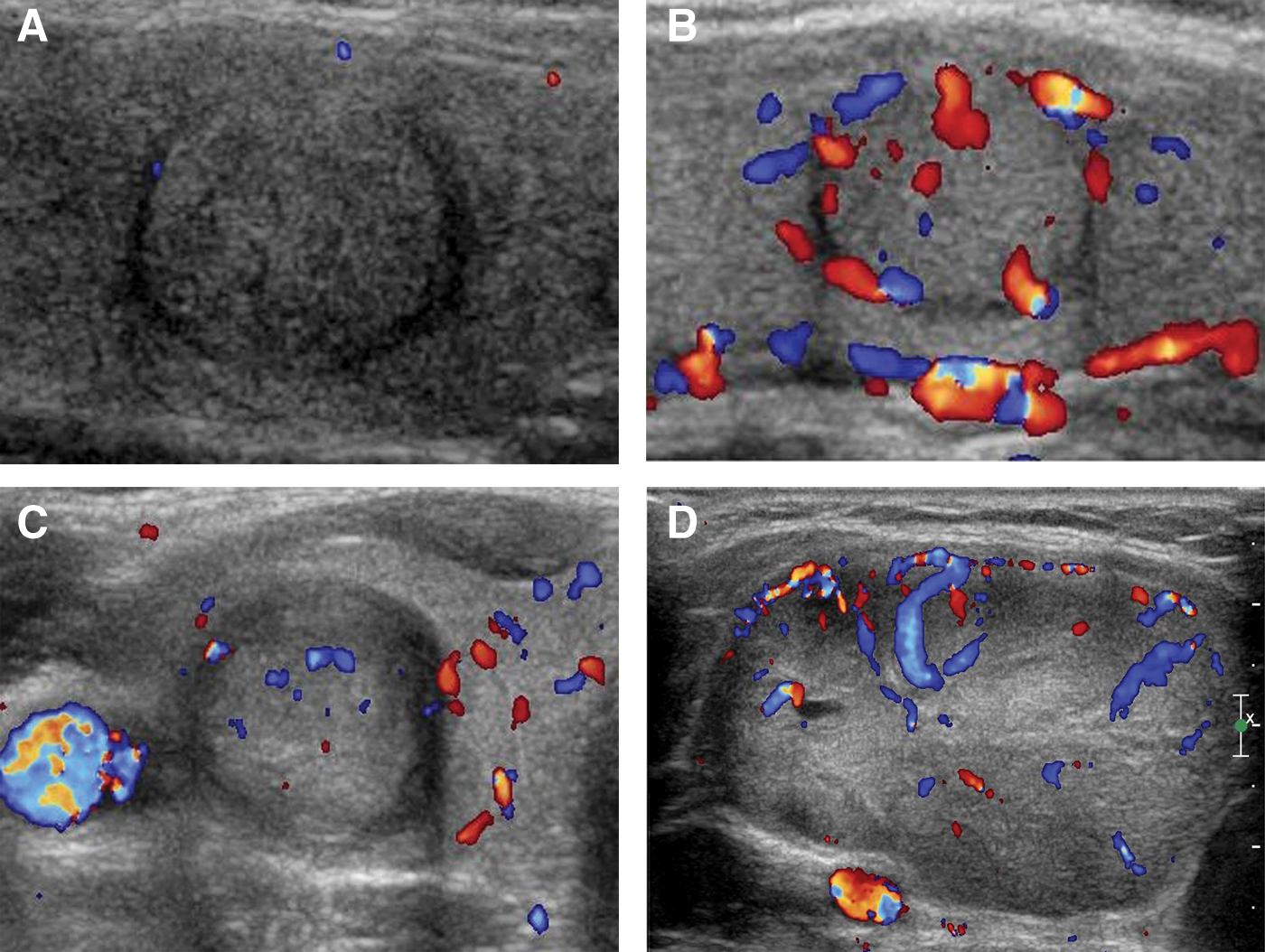
Four classifications of color Doppler patterns for solid, round, isoechoic thyroid nodules without coexistent malignant sonographic features. According to the degree and predominance of vascularity in the peripheral and/or central portions, a thyroid nodule was classified as scant
US-FNA and cytological analysis
US-FNA was performed after the thyroid US examination by the same radiologist, with the use of the one-sampling technique (i.e., through a single needle puncture and multiple to-and-fro needle motions, only one specimen was obtained during the US-FNA procedure on each thyroid nodule), no aspiration device, and no local anesthesia (15). For each sample, a smear was prepared on 4–6 slides, fixed in 95% ethanol, and examined after Papanicolaou staining.
For the cytological analysis, the Bethesda classification was used (16) and the cytological categories were as follows: nondiagnostic (Bethesda class I), benign (class II), atypia of undetermined significance or follicular lesion of undetermined significance (class III), follicular neoplasm or suspicious for follicular neoplasm (class IV), suspicious for malignancy (class V), and malignant (class VI).
Statistical analysis
Benign or malignant SRINs were compared according to their vascular patterns by using the chi-square test. Statistical analysis was performed using SPSS (version 17.0.1; IBM, Armonk, NY), and p<0.05 was considered statistically significant.
Results
In the 727 patients, a total of 27 SRINs (largest diameter: range 5.0–27.3 mm, mean 12.7 mm) were identified in 27 patients, resulting in a SRIN prevalence of 3.7% (27/727). The location, size, color Doppler pattern, cytological results, and pathologic results of these SRINs are summarized in Table 1.
APD, anteroposterior diameter of the nodule; TD, transverse diameter of the nodule; LD, longitudinal diameter of the nodule; NH, nodular hyperplasia; FA, follicular adenoma; PTC, papillary thyroid carcinoma; F, female; M, male.
Fourteen of these nodules (largest diameter: range 6.2–27.3 mm, mean 13.4 mm) were surgically removed for the following reasons: malignant cytology by US-FNA (n=5), the presence of a coexisting thyroid malignancy (n=7), and patient request (n=2). Among these 14 surgical nodules, there were 7 papillary thyroid carcinomas (classic type [n=3] and follicular variant [n=4]), 2 follicular adenomas, and 5 nodular hyperplasias (Figs. 2 and 3). Of the 13 nonsurgical SRINs (range of the largest diameter, 5.0–22.9 mm; mean size, 11.7 mm), 10 had benign cytological results in the 2 consecutive US-FNAs and 3 had Bethesda class III in the initial US-FNA. Of the 3 nonsurgical nodules with initial Bethesda class III, 2 had benign cytological results in the repeat US-FNA and no interval change at the follow-up US after 12 months, whereas 1 had the same cytological results in the repeat US-FNA and a moderate decrease (∼50%) in nodule volume at the follow-up US after 12 months. Therefore, all 13 nonsurgical SRINs were considered to be benign, resulting in an SRIN malignancy rate of 25.9% (7/27).
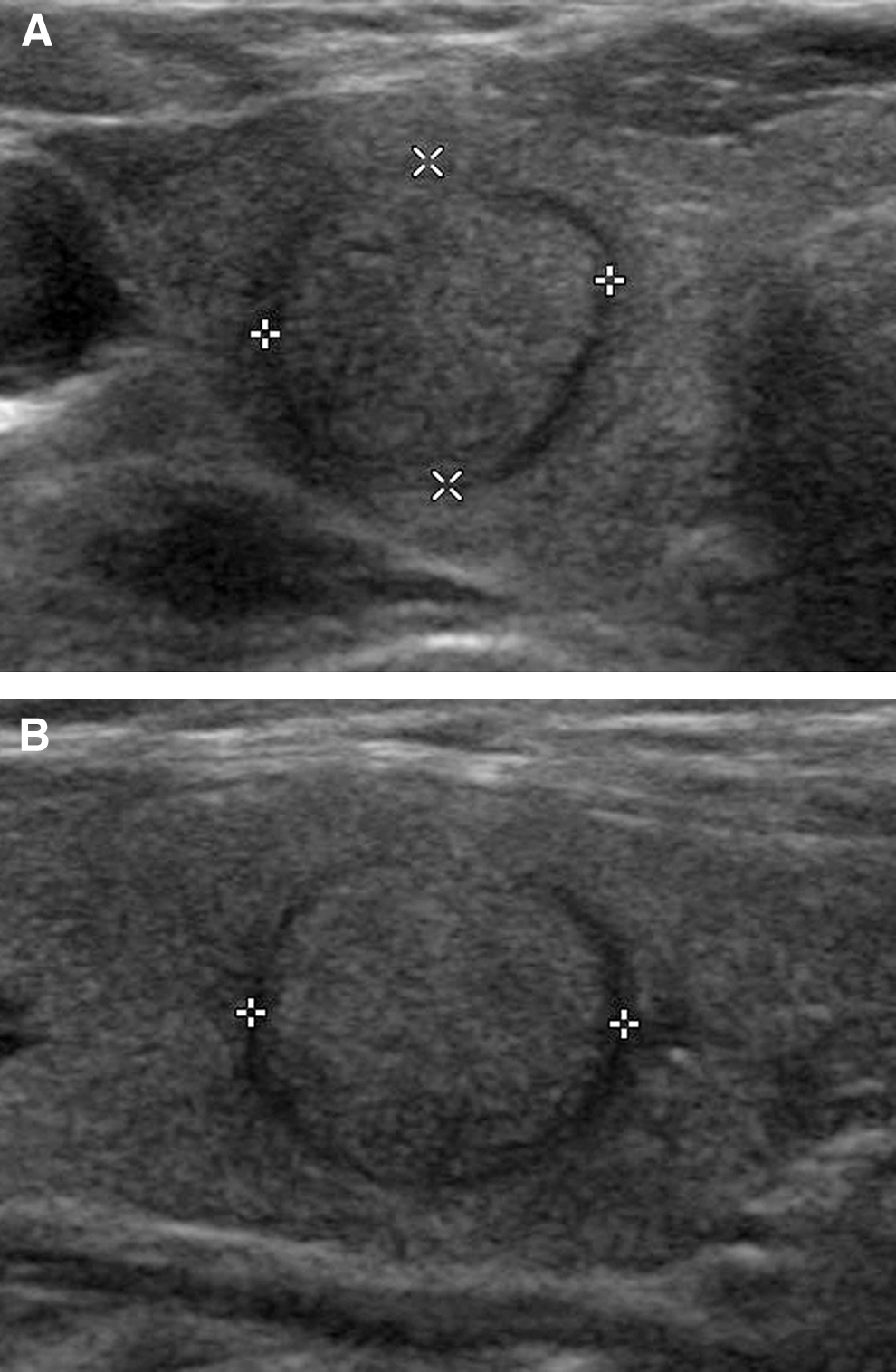
Transverse and longitudinal gray-scale sonograms of a right thyroid nodule in a 62-year-old woman showing isoechogenicity, a smooth margin, and a round shape (11.1 mm×11.9 mm×12.9 mm)
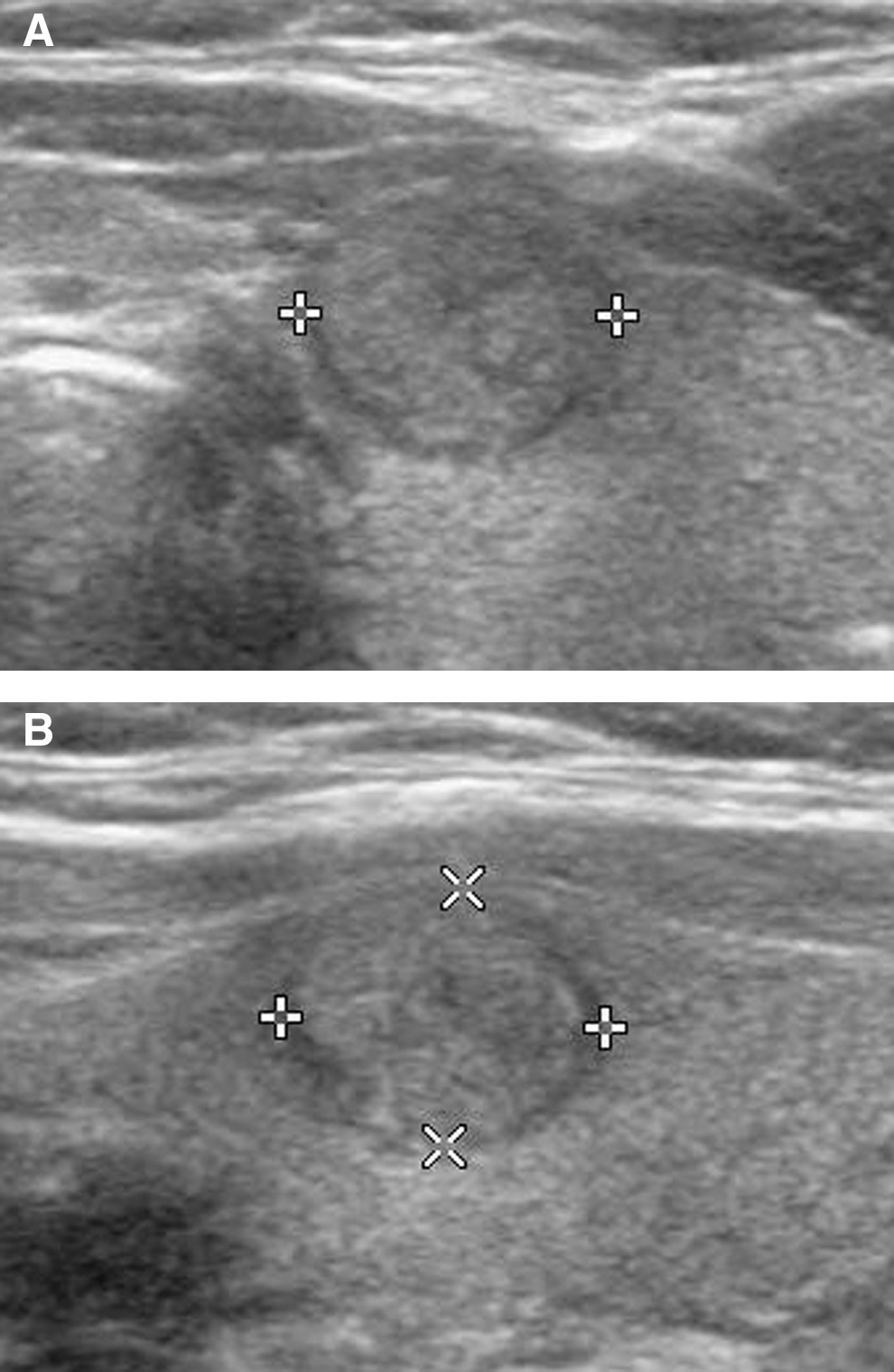
Transverse and longitudinal gray-scale sonograms of a right thyroid nodule in a 30-year-old woman showing isoechogenicity, a smooth margin, and a round shape (6.7 mm×7.2 mm×8.1 mm)
The number of scant, peripheral, central, and mixed type on color Doppler US for SRINs was 6, 2, 2, and 17, respectively. The number of color Doppler patterns in malignant and benign SRINs included 1 and 5 scant type, 1 and 1 peripheral type, 1 and 2 central type, and 4 and 12 mixed type, respectively. There was no significant difference in the prevalence of the color Doppler patterns between malignant and benign SRINs (p>0.05, chi-square test).
Discussion
High-resolution thyroid US has been widely used in the evaluation of thyroid nodules, resulting in the establishment of certain characteristics that mark benign and malignant thyroid nodules; however, the ability of high-resolution thyroid US to distinguish benign from malignant nodules is still a matter of debate (2,4 –7,12). The significance of several US features, including a solid composition, macrocalcifications, hypoechogenicity, and centrally predominant vascularity, is still unclear (8 –11). In particular, several studies have suggested that a solid composition represents a malignant sonographic feature (6,13,17), but these studies did not subclassify solid thyroid nodules according to the presence and absence of coexisting malignant sonographic features or calcifications. In the present study, we investigated the malignancy rate of solid thyroid nodules without coexisting malignant sonographic features, hypoechogenicity, and calcifications. Although the prevalence of SRINs was very low (3.7%, 27/727), the malignancy rate of these SRINs was not low (25.9%, 7/27) compared with the overall malignancy rate in the patients with thyroid nodules, ranging from 9.2% to 13.0% (3,8).
Blood flow, oxygen, and nutrient delivery are essential components for tumor cell growth (18). Hypothetically, malignant tumors may make their shape to maximize oxygen exposure and consumption of nutrients, and thus the surface area–to–volume ratio is mathematically maximized by a spherical shape, allowing the greatest number of cells access to crucial nutritional factors in their ambient environment (14). In the present study, the malignancy rate of SRINs was not low, and this finding corresponds to Vaupel's hypothesis(18). In addition, all seven of the malignant SRINs were papillary thyroid carcinomas: three classical types and four follicular variants. We cannot explain the high prevalence of the follicular variant of papillary thyroid carcinoma in our study.
We attempted to analyze the correlation between the color Doppler pattern of SRINs and malignancy. We found no statistically significant difference in the color Doppler pattern between benign and malignant nodules, despite the fact that several studies have reported that central vascularity may predict thyroid malignancies (9). In this study, central and peripheral color Doppler patterns in malignant and benign SRINs were seen in only one nodule each. However, only a small number of cases were included in this study, and further large-scale studies may be required to clarify this finding.
This study has several limitations. First, all 13 nonsurgical SRINs were diagnosed as benign by using only consecutive US-FNAs and a long-term US follow-up, which may represent a confirmation bias. In particular, three nonsurgical nodules with initial Bethesda class III were classified into the benign category without histopathological confirmation. Second, all thyroid US scans and US-FNAs for each SRIN were performed by a single radiologist. Third, a quantitative analysis for the vascularity of SRINs in color Doppler US was not performed. Finally, the presence or absence of underlying diffuse thyroid disease was not evaluated.
In conclusion, the results of this study show that SRINs are associated with a relatively high malignancy rate, but that the color Doppler pattern of SRINs was not useful for predicting the malignancy of SRINs. Therefore, US-FNA for SRINs should be performed to rule out malignancy, regardless of the color Doppler pattern.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.