
Abstract
Background:
Despite surgical treatment, chemotherapy, and/or radiotherapy, the vast majority of patients with anaplastic thyroid carcinoma (ATC) have a dismal prognosis. Better knowledge of the frequency of metastases to different sites might help us to perform the appropriate diagnostic tests before treatment and during the course of the disease. The aim of this study was to determine the frequency of metastases from ATC in different sites as found at autopsy.
Methods:
Altogether, 205 patients were treated for ATC at our institute during the years 1972–2008. Autopsy was performed in 45 cases (30 females, 15 males; median age 66 years). The relative frequencies of metastases in different sites were analyzed using descriptive statistics.
Results:
Altogether, 41 cases (91%) had metastases at autopsy. The most common sites of metastases were the lungs (78%), intrathoracic lymph nodes (58%), neck lymph nodes (51%), pleura (29%), adrenal glands (24%), liver (20%), brain (18%), heart (18%), and retroperitoneal lymph nodes (18%). Less common sites of distant metastases were the pericardium (13%), bones (13%), kidneys (13%), mesentery or peritoneum (13%), skin (9%), pancreas (4%), stomach (4%), diaphragm (4%), pituitary gland (2%), ovary (2%), jejunum (2%), axillary lymph nodes (2%), and gingival mucosa (2%). Both distant and regional metastases were present in 23 cases, while only distant metastases were present in 18 cases. An extensive local infiltration of the primary tumor was found in 76% of the cases. The total number of the involved organs and lymph node basins were 123 and 58, respectively. The mean number of metastatic sites was 4.02±2.75. Lung metastases were present in 34 of 38 (89%) of our patients who had distant metastases found at autopsy. Of these 34 patients, 27 were known to have lung metastases when they were alive.
Conclusion:
Two or more metastatic sites were found at autopsy in 84% of cases. The most common metastatic sites are lungs, followed by the intrathoracic and neck lymph nodes.
Introduction
The presence of distant metastases has an impact on the treatment of patients. In patients with good performance status, systemic therapy with chemotherapy with or without external beam radiotherapy may be used to prolong survival and prevent rapid tumor progression (4,20). On the other hand, palliative therapy to control symptoms is used in older patients with poor performance status and/or concomitant diseases (4,19). Better knowledge of the frequency of metastases to different sites might help us to perform the appropriate diagnostic tests before treatment and during the course of the disease. More than 200 patients with ATC have been treated at the Institute of Oncology in Ljubljana (21). Among 188 patients with ATC, only 4% were alive without disease, 2% were lost from follow-up, and 1% died of causes unrelated to ATC, while 93% died of ATC (19). The cause of death was distant metastases, locoregional tumor with distant metastases, locoregional tumor only, and not determined in 51%, 22%, 13%, and 7% of patients, respectively (19). Autopsy was performed in 45 cases. The main purpose of this study was to determine the frequency of metastases in different sites as detected at autopsy. The other aim of the study was to find out if there are any patient characteristics that correlated with the number of metastatic sites or localization of metastases.
Materials and Methods
Altogether, 205 patients (140 females, 65 males; median age 69 years, mean age 67.9 years) were treated for ATC in the years 1972–2008. The data about the treatment and prognostic factors of our patients have been reported (13,19,22). During this period, 45 deceased patients (30 females, 15 males; median age 66 years, mean age 66.2 years) had an autopsy. The characteristics of 45 cases and their treatment are presented in Table 1.
CH, chemotherapy; RT, radiotherapy; S, surgery.
In patients with ATC in the terminal phase of the disease, extensive diagnostic tests to determine the extent of the disease at different metastatic sites were not performed. Thus, only those diagnostic tests that would change the therapeutic or palliative treatment of a patient were performed. Based on these tests, distant metastases were found in the lungs (27 cases), mediastinum (13 cases), pleura (4 cases), brain (4 cases), skin (1 case), bones (1 case), small intestine (1 case), and adrenal glands (1 case). Furthermore, it was evident that 33 patients had locally advanced disease, and 17 patients had cervical lymph node involvement.
Autopsy was performed to obtain the information about the effectiveness of treatment of ATC with chemotherapy and/or external radiotherapy. Another purpose of the autopsy was to determine the extent of the disease. In only two of our cases was ATC diagnosed at autopsy, while in 43 patients, ATC was diagnosed in biopsy specimens by cytology, histopathology, and both cytology and histopathology in 21, 7, and 15 cases, respectively. All cases and autopsy reports were reviewed by a pathologist experienced in thyroid pathology (B.G.).
The study was reviewed by the appropriate Ethics Committee and was conducted in accordance with the ethical standards laid out in the appropriate version of the 1964 Declaration of Helsinki. The Institutional Review Board approved the study.
The frequencies of metastases in different sites were analyzed using methods of descriptive statistics. The correlation of patients' characteristics with the number of metastatic sites and localization of metastases was analyzed statistically using the chi-test and contingency tables in SPSS 16.0 for Windows (SPSS, Chicago, IL).
Results
At autopsy, metastases were detected in 41 cases (91%). Both distant and regional metastases were present in 23 cases, while only distant metastases were present in 18 cases. Only four of our cases were without metastases. All four patients succumbed due to locally very advanced local tumor infiltration into the trachea and surrounding structures.
An extensive local infiltration of the primary tumor into surrounding structures was found in 33 cases (80%). In addition, cervical lymph node metastases were present in 19 of 33 cases (58%).
Lateral neck lymph nodes only, central compartment lymph nodes only, and both lateral and central lymph nodes were affected with metastases in 9, 2, and 12 cases, respectively. Supraclavicular lymph nodes were affected by ATC in 8 cases. Metastatic intrathoracic lymph nodes were found in 26 cases: upper mediastinal only in 7 cases, both upper mediastinal and other (paratracheal, tracheoesophageal, tracheobronchial, or hilar) lymph nodes in 12 cases, and only other lymph nodes in 7 cases.
The frequency of metastases in different sites is presented in Table 2. The total number of the involved organs and lymph node basins was 123 and 58, respectively. The mean number of metastatic sites was 4.02±2.75. Two or more metastatic sites were found at autopsy in 84% of cases. The number of metastatic sites in our cases is presented in Figure 1.
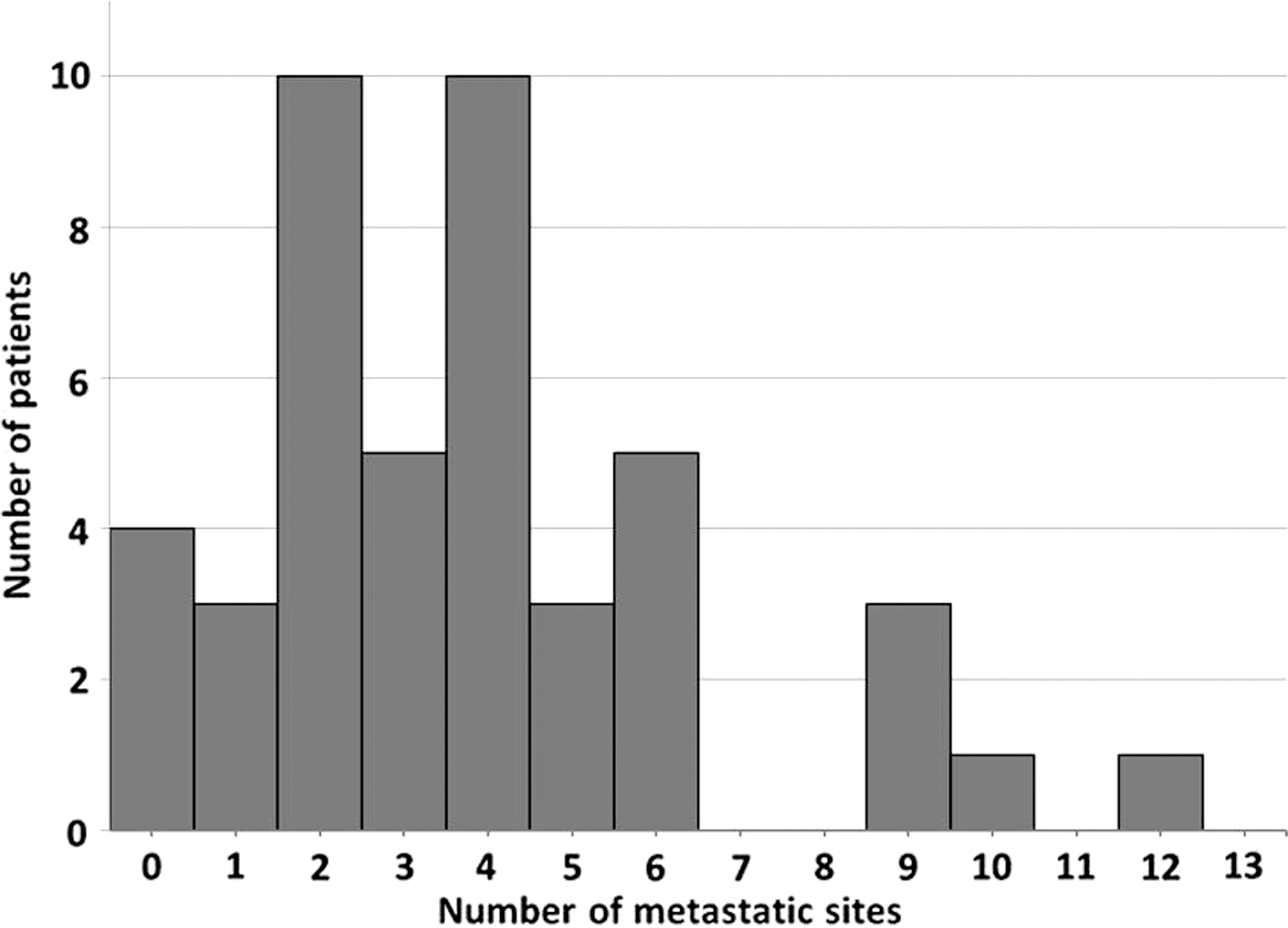
Number of patients and number of metastatic sites at autopsy of 45 cases with anaplastic thyroid carcinoma.
Bilateral 7 and unilateral 4.
In 10 cases of ATC, a coexistent differentiated thyroid carcinoma was also present. The presence of a coexistent differentiated tumor did not correlate with a higher frequency of metastases in any specific organ. Sex, age of patients, previous thyroid enlargement (>1 year), rapid tumor growth (<3 months), primary tumor size, initial local extension of the tumor, or coexistence of a differentiated carcinoma were not correlated with a larger number of metastatic sites or a higher frequency of metastases in a specific organ as shown by the chi-square statistical test (p>0.05).
Discussion
Knowledge of the sites and extent of distant metastases in the terminal phase of ATC is important to provide the optimal palliative care to the patient in the terminal phase of the disease. Positron emission tomography/computed tomography appears to be the reference imaging modality for ATC at initial staging and seems promising in the early evaluation of treatment response and follow-up (18). However, this expensive and time-consuming diagnostic test is rarely used in the terminal phase of the disease. Therefore, despite the effectiveness of modern diagnostic tests to diagnose the site and extent of metastatic disease, it is very unlikely that the data about the extent of the disease in the terminal phase of ATC will be determined by using these tests.
The main purpose of this study was to determine the frequency of metastases in different sites detected at autopsy. Distant metastases, extensive local infiltration, and regional lymph node metastases were found at autopsy in 91%, 76%, and 51% of cases, respectively. Both distant and regional metastases were present in 51% of cases, while only distant metastases were present in 40% of cases. The most common sites of metastases were the lungs (78%), intrathoracic lymph nodes (58%), neck lymph nodes (51%), pleura (29%), adrenal glands (24%), liver (20%), brain (18%), and heart (18%). Lung metastases were present in 34 of 38 (89%) of our cases with distant metastases found at autopsy, and were known in 27 patients while they were alive. In the majority of these 27 patients, lung metastases were detected by a simple chest X-ray.
The largest published autopsy series of ATC included 13 and 20 cases (23,24). Ibanez et al. (24) reported the following sites of metastases in 13 cases: lungs (61%), lymph nodes (46%), gastrointestinal tract (38%), heart (31%), adrenal glands (31%), pericardium (31%), pleura (31%), skin (31%), liver (23%), peritoneum (23%), brain (23%), bone (23%), kidneys (15%), pancreas (15%), diaphragm (15%), pituitary gland (8%), and breasts (8%). Tan et al. (25) reported the following sites of metastases in 12 cases: cervical lymph nodes (83%), lungs (75%), mediastinum (50%), adrenal glands (33%), supraclavicular lymph nodes (25%), mesenteric lymph nodes (17%), pelvic lymph nodes (17%), bone (8%), and brain (8%). These data are very similar to the results of our 45 autopsies. In our cases, metastases were found in the lungs, lymph nodes, pleura, adrenal glands, liver, brain, heart, bones, pericardium, kidneys, peritoneum, gastrointestinal tract, skin, pancreas, diaphragm, pituitary gland, ovary, and gingival mucosa (Table 1).
The other aim of the study was to find out if there are any patients' characteristics that correlated with the number of metastatic sites and localization of metastases. Coexistent differentiated thyroid carcinoma was found in nine (20%) of our cases. Among six (13%) of our cases with bone metastases, four were without a coexistent differentiated carcinoma, while two cases had a coexistent differentiated carcinoma. Similarly, Tickoo et al. (26) reported that 5 of 10 cases with bone metastases of ATC were solely undifferentiated, while the other five also had a well-differentiated component. To continue, the presence of well-differentiated carcinoma was not correlated with the occurrence of brain metastases in our cases. Brain metastases of anaplastic carcinoma were found in eight (18%) of our cases: in six cases without a coexistent differentiated carcinoma, and in two cases with a coexistent differentiated carcinoma. We found no patients' or pathomorphologic characteristics correlating with a larger number of metastatic sites or specific metastatic sites.
Widespread distant dissemination of ATC was present in the majority of our cases. ATC is a systemic disease in the majority of cases in the terminal phase. However, the real question is whether ATC is a systemic disease from its very beginning, or only in the terminal phase. Sugino et al. (27) reported that 1-year survival was 73% in 11 patients with only focal and incidentally surgically treated ATC. None of them had systemic therapy (27). Obviously, very small ATC is usually not a systemic disease. Unfortunately, 96% of our patients with ATC did not have focal ATC (19). Short survivals of our 188 patients indicate that ATC is a systemic disease when ATC is clinically evident (19). Therefore, our view is that patients in the early stage of the disease should have systemic treatment initially to prevent progression of initially undetected micrometastases (13,28). There have been a number of reports that suggest that the postoperative administration of adriamycin and hyperfractionated radiation therapy increase the local control rate and prolong survival (29), while others have suggested that thyroidectomy after neoadjuvant chemotherapy may be more feasible (13,30). Higashiyama et al. observed clinical benefit rates after induction chemotherapy by weekly paclitaxel in stage IVB and stage IVC in 56% and 75%, respectively (20). Adjuvant chemotherapy was applied after surgical treatment to prevent systemic progression of disease and external radiotherapy to avoid locoregional recurrence. This approach was very effective: the 12-month survival rate of stage IVB patients was 44% after induction chemotherapy. On the other hand, in patients with stage IVc, shrinkage of lung metastasis was initially observed in three of four cases, but unfortunately, in all of them, distant metastases subsequently progressed and all of them succumbed in 8 months (20). Nowadays, metastatic ATC is an incurable disease. Further studies are necessary to obtain long-lasting effective systemic treatment for patients with distant metastases of ATC.
In conclusion, in the majority of patients, ATC metastasizes into many organs. Two or more metastatic sites were found at autopsy in 84% of cases. The most common metastatic sites are lungs, followed by the intrathoracic and neck lymph nodes.
Footnotes
Acknowledgment
This article is a part of the Research Study No. P3-0289 supported by the Ministry of Higher Education, Science, and Technology of the Republic of Slovenia.
Disclosure Statement
The authors have no commercial associations that might pose a conflict of interest in connection with this article.