
Abstract
Background and Purpose:
Understanding the computed tomography (CT) characteristics of the pyramidal lobe and other thyroid variations and detecting them accurately using preoperative neck CT will minimize unnecessary remnant thyroid tissue after total thyroidectomy in patients with thyroid cancer. The purpose of the present study was to assess the frequency, location, and size of the pyramidal lobe and other thyroid variations using a large-scaled, multicenter study.
Methods:
Neck CT scans for 200 patients were selected from 11 institutions; a total of 2200 patients were included in the study. The patients underwent neck CT for the following reasons: trauma, known thyroid malignancy, cervical lymphadenopathy, palpable neck mass, oropharyngolaryngeal malignancy, vocal cord palsy, postchemotherapy CT follow-up, inflammatory or infectious neck lesion, parathyroid abnormality, and patient request. A single radiologist at each institution retrospectively analyzed 200 neck CT scans. Each radiologist investigated the presence, location, length, volume, and upper end of the pyramidal lobe and its separation or continuity with the main thyroid gland as well as the presence, location, length, and volume of the accessory or ectopic thyroid using a picture archiving and communication system.
Results:
A pyramidal lobe was present in 44.6% (981/2200) of the patients. The prevalence for the pyramidal lobe at the participating institutions ranged from 28.0% to 55.0% (mean, 44.6%). Pyramidal lobes originating from the left side of the thyroid were most common, and the number of pyramidal lobes showing separation from the main thyroid gland was 90 (9.2%). The mean anteroposterior diameter, transverse diameter, and length of the pyramidal lobe were 2.3, 5.9, and 20.8 mm, respectively. Among both men and women, the most common level of the upper end of the pyramidal lobes was the thyroid cartilage, but there was a significant difference in the frequency of the pyramidal lobe between males and females (p<0.0001). The rate of the pyramidal lobe detection in the 2-mm-slice-thickness group was higher than those in the 2.5- and 3-mm groups (p=0.0003).
Conclusion:
Neck CT is useful for detecting the presence, size, configuration, and location of the pyramidal lobe and other thyroid variations.
Introduction
Materials and Methods
Patients
This study was approved by the Institutional Review Board (IRB) of each of the 11 participating institutions (Ansan, Seoul St. Mary's, Seoul National University, Boramae, Human Medical, Severance, Daerim St. Mary's, Asan Medical Center, Haeundae Paik, Kangbuk Samsung, and Busan Paik Hospitals; IRB: 11–174). Starting in January 2011, 200 CT scans of the neck were selected from each institution. Ultimately, 2200 patients (1389 women and 811 men; age 19–70 years; average age, 46.6 years) were included in this study. Exclusion factors for this study included patient age <19 years or >70 years and a neck CT showing previous thyroidectomy or other neck operations an inappropriate CT protocol, or poor image quality.
Neck CT scanning
Neck CT was performed in the axial planes from the skull base to the upper mediastinum with intravenous administration of a contrast medium using a 16-channel multidetector CT scanner (Sensation; Siemens Medical Solution, Erlangen, Germany/Lightspeed Ultra; GE Medical Systems, Milwaukee, WI), a 64-channel multidetector CT scanner (Brilliance 64, Philips, Tel Aviv, Israel; Aquilion One, Toshiba Medical Systems, Otawara, Japan; Somatom Sensation 64, Siemens; Discovery CT750 HD, GE), or a 128-channel multidetector CT scanner (LightSpeed, GE; Somatom Definition AS, Siemens). Nonenhanced axial, contrast-enhanced axial, and contrast-enhanced coronal reformatted CT images were acquired in all cases (slice thickness, 2, 2.5, and 3 mm; reconstruction increment, 2, 2.5, and 3 mm), and contrast-enhanced sagittal reformatted CT images were acquired as necessary in each institution.
Image analysis
Using a picture-archiving and communication system, image analysis was independently carried out by 11 radiologists with different experience (range 6–16 years, mean 11.6 years) in head and neck CT interpretation. A single radiologist in each institution retrospectively analyzed 200 neck CT scans. In this study, the pyramidal lobe was defined as a longitudinally arranged accessory thyroid lobe protruding from the upper margin of the isthmus or the medial aspect of the right or left thyroid lobe on three or more serial axial images (Figs. 1 –3). The accessory thyroid was defined as a supernumerary thyroid when the main thyroid was located in a normal thyroid fossa (Figs. 4 and 5); ectopic thyroid was defined as an aberrant thyroid when the main thyroid was not located in a normal thyroid fossa. Superficial cervical veins can be differentiated from the pyramidal lobe on neck CT scans, because they show greater longitudinal arrangement, uniform size, small diameter, and different attenuation than the thyroid gland. Differentiation between the pyramidal lobe and perithyroidal lymph nodes, including the Delphian node, is not difficult using CT, because lymph nodes show as a short segment, bean or ovoid shape, low attenuation, and mild enhancement in comparison to those of the pyramidal lobe.
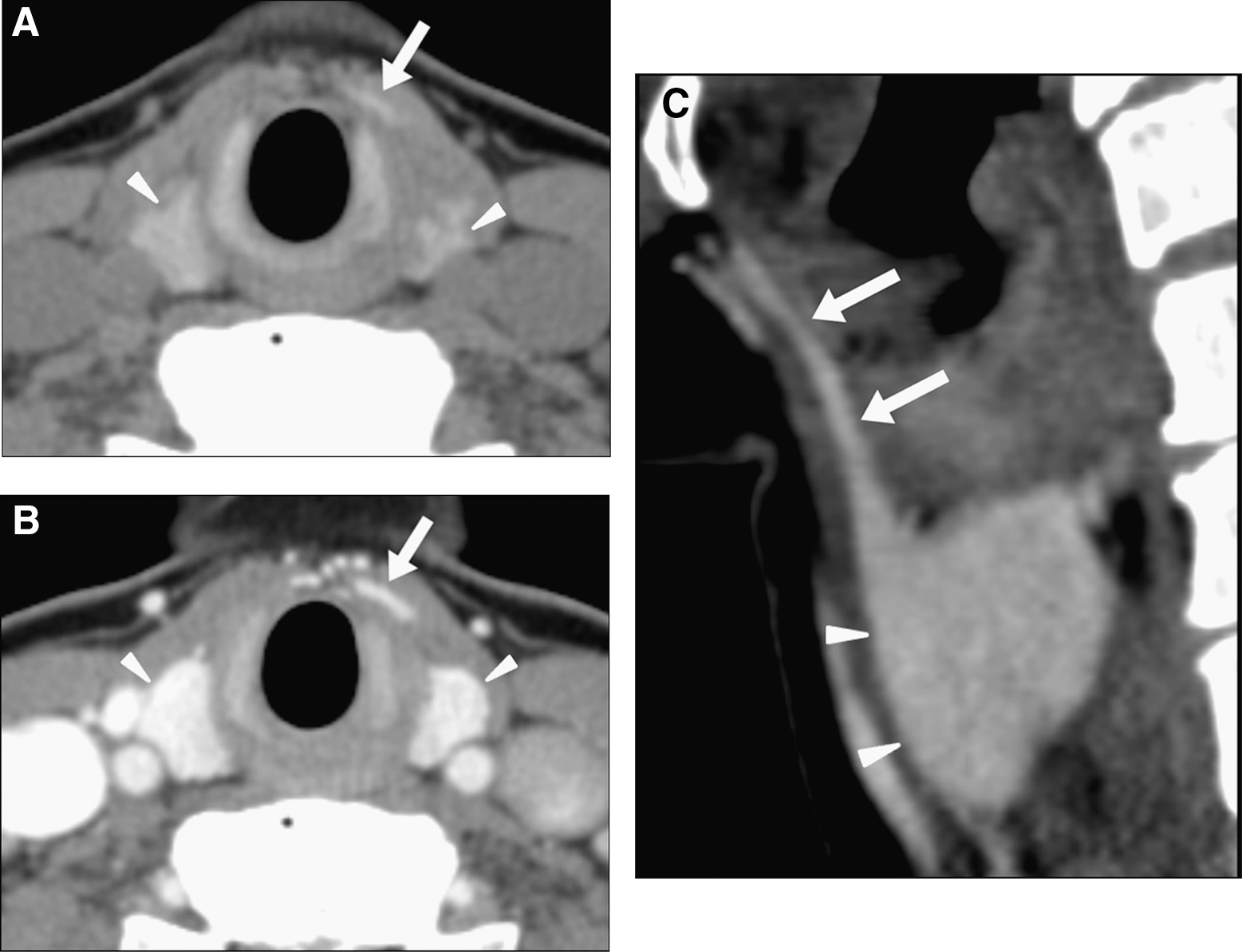
Left pyramidal lobe showing continuity with the main thyroid gland in a 50-year-old woman. Nonenhanced axial
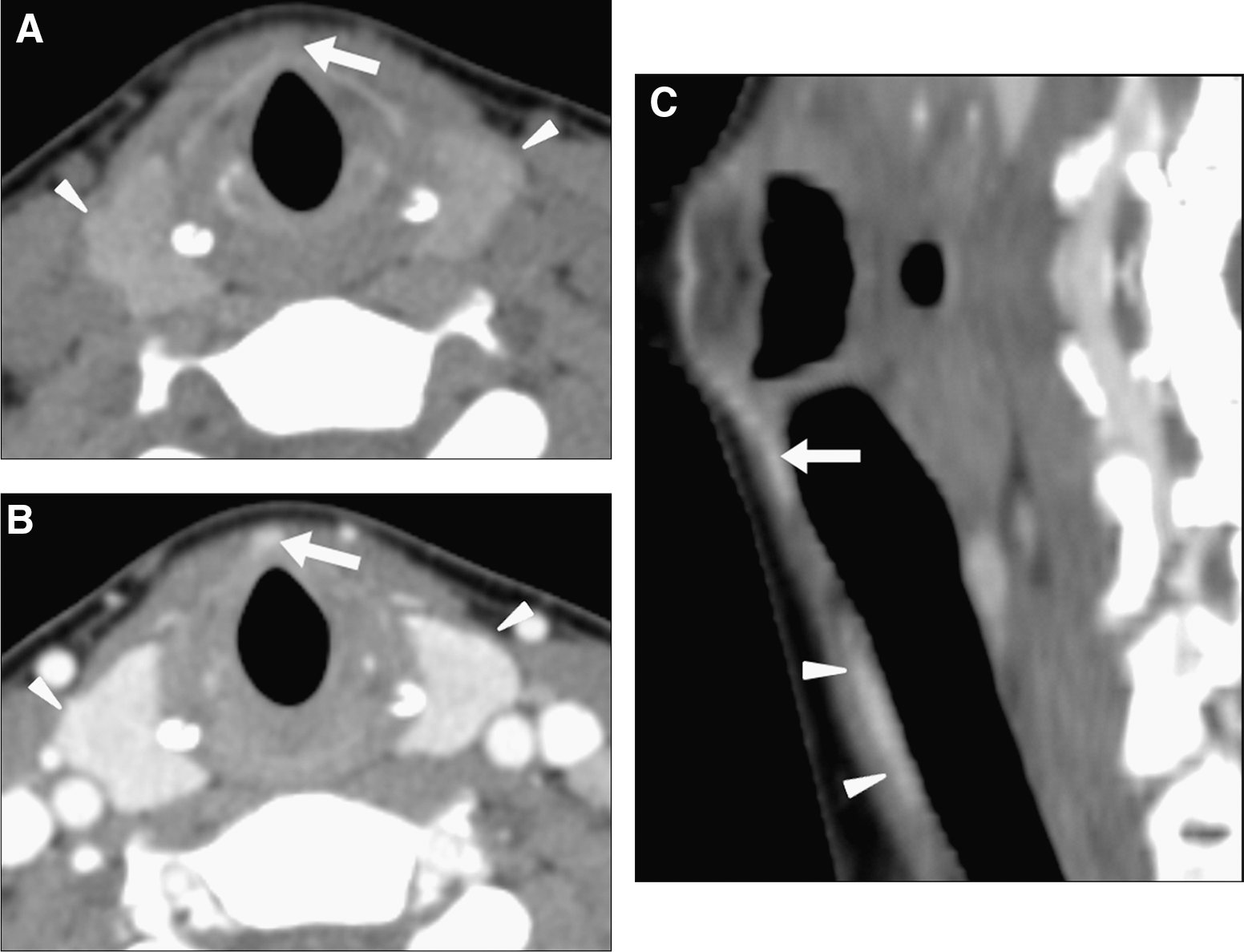
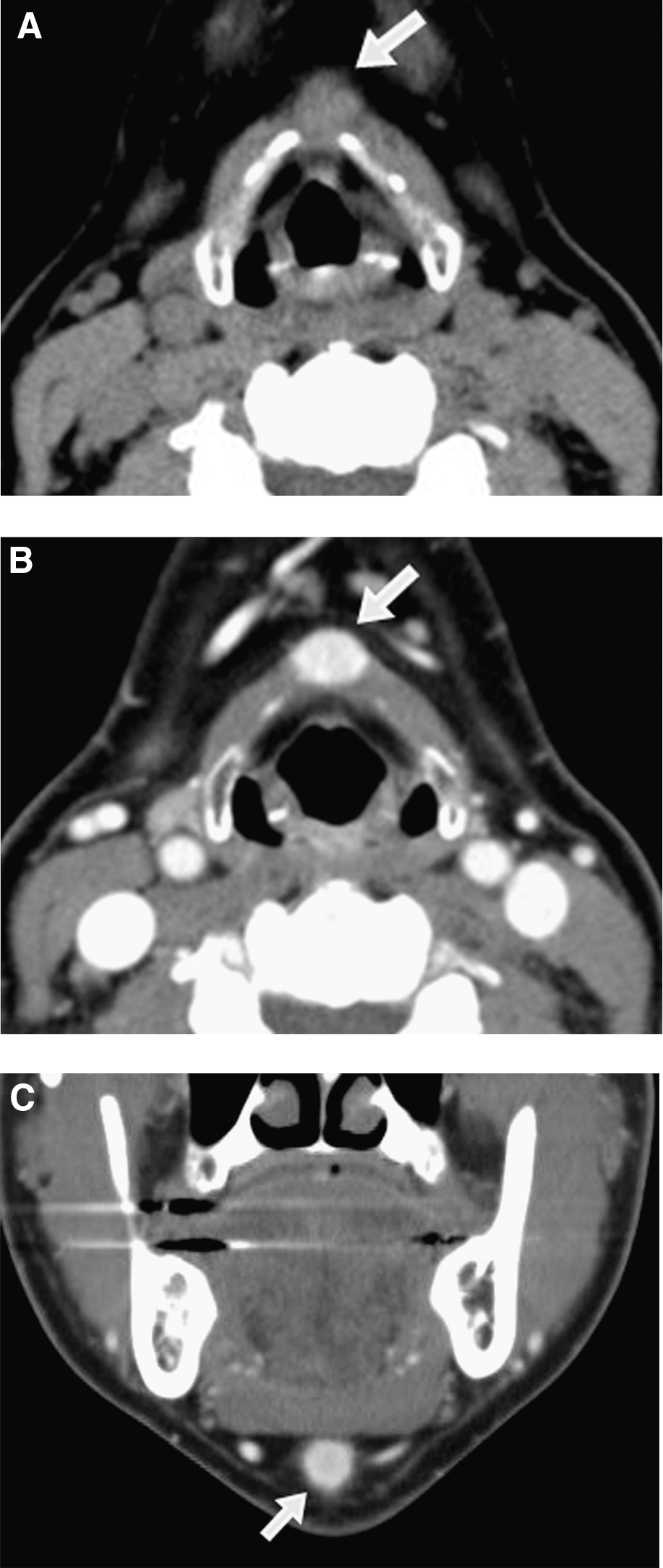
Midline pyramidal lobe focally separated from the main thyroid gland in a 35-year-old woman. Nonenhanced axial
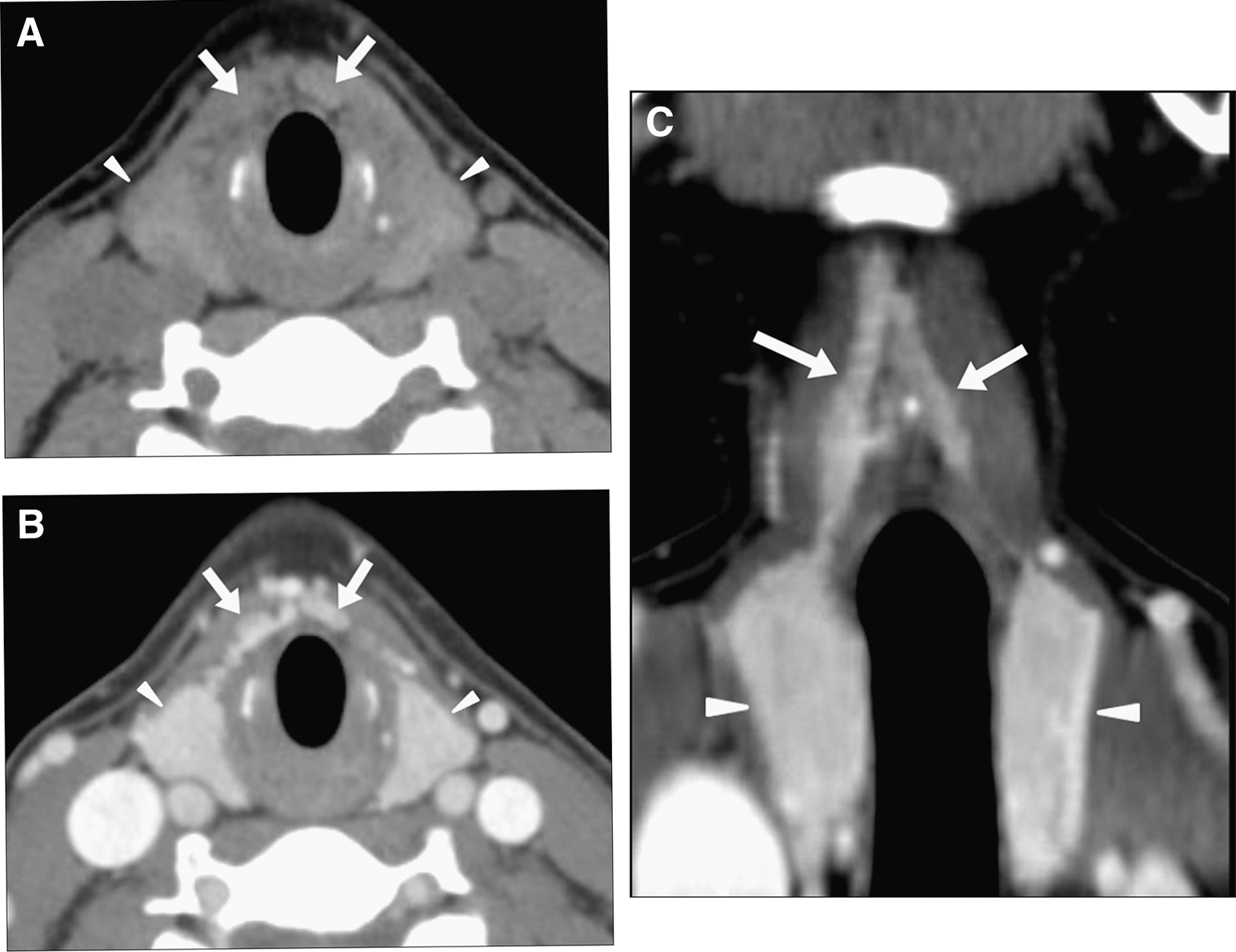
Bilateral pyramidal lobe in a 43-year-old woman. Nonenhanced axial
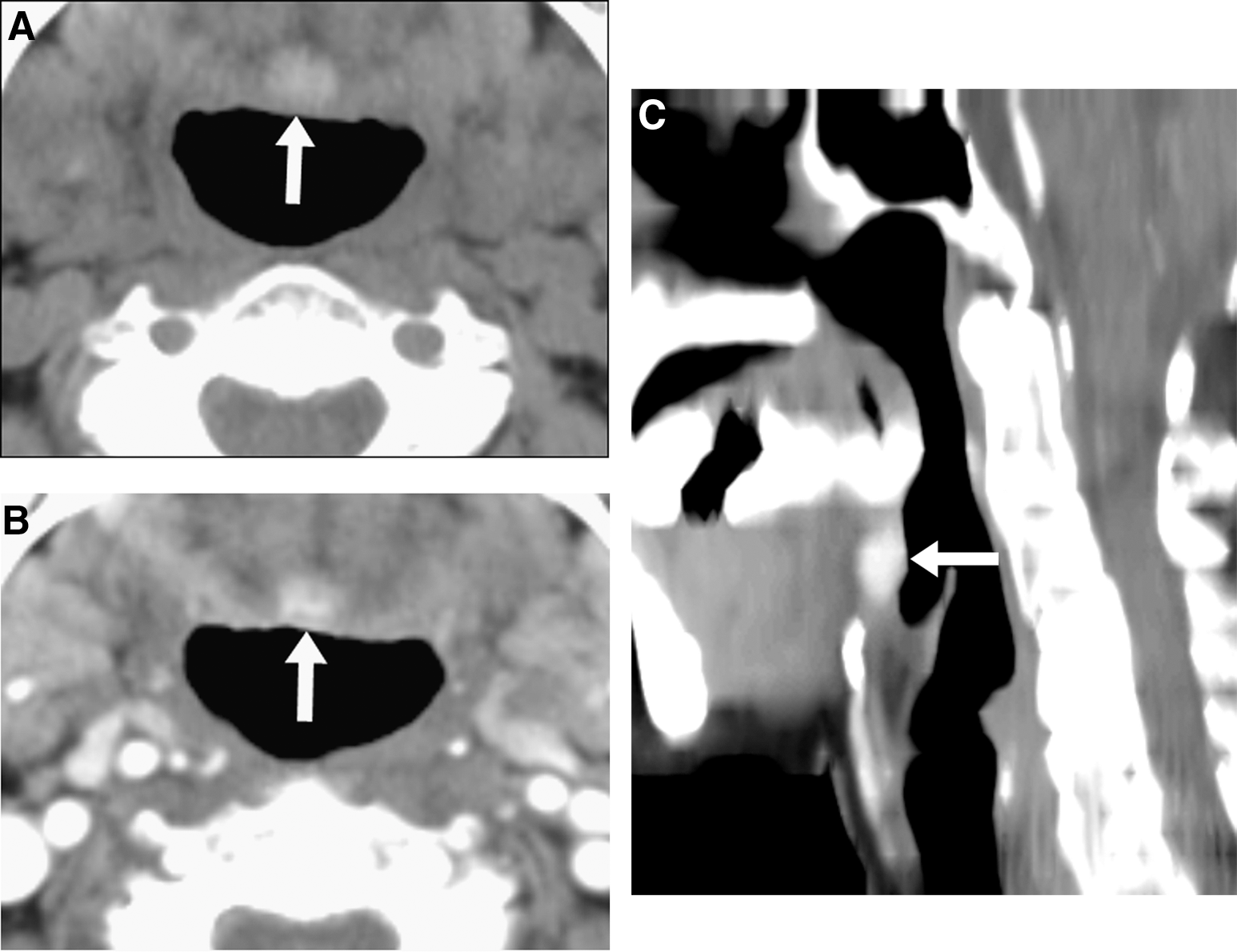
An accessory thyroid at the tongue base (1 cm in the largest diameter) in a 61-year-old woman. Nonenhanced axial
An accessory thyroid in the midline portion of the anterior upper neck (1.2 cm in the largest diameter) in a 58-year-old woman. Nonenhanced axial
The location of the pyramidal lobe was classified in accordance with its origin, for example, right, left, midline, or bilateral. The pyramidal lobe was classified into one of four categories according to the location of the upper end: tongue base, hyoid bone, thyrohyoid membrane, or thyroid cartilage. Separation of the pyramidal lobe was defined by a lack of visualization of the pyramidal lobe on one or more axial images between the pyramidal lobe and the main thyroid gland. The presence, location, length, volume, and upper end of the pyramidal lobe and its separation or continuity with the main thyroid gland were investigated. The anteroposterior (AP) diameter of the main thyroid (i.e., the mean of the largest AP diameter measured at both thyroid lobes on axial CT images) and the isthmus (the largest AP diameter on axial CT images) were measured. The AP diameter of the main thyroid was measured on contrast-enhanced axial CT, but any increase in the AP diameter due to thyroid nodules was excluded. The location of the accessory thyroid was classified as the upper level (suprahyoid or hyoid neck), mid-level (infrahyoid neck), and lower level (thoracic inlet or upper mediastinum).
Statistical analysis
All data were compared using Fisher's exact test, chi-square test, Cochran-Mantel-Haenszel test, or Student's t-test, and p<0.05 was considered statistically significant. All statistical analyses were performed using SAS 9.2 for Windows (SAS Institute, Inc., Cary, NC). Fisher's exact and chi-square tests were used for comparison of categorical variables, and Student's t-test was used for comparison of quantitative variables.
Results
The patients underwent neck CT for the following reasons: trauma (n=19), known thyroid malignancy (n=892), cervical lymphadenopathy (n=175), palpable neck mass (n=364), oropharyngolaryngeal malignancy (n=107), vocal cord palsy (n=23), postchemotherapy CT follow-up (n=224), inflammatory or infectious neck lesion (n=362), parathyroid abnormality (n=9), and patient request (n=25). There was a significant difference in the prevalence of the pyramidal lobe between the groups with different clinical reasons for neck CT scanning (p<0.0001, chi-square test).
Data for patient sex and age, prevalence and size of the pyramidal lobe, size of the AP diameter of the main thyroid and the isthmus, and the frequency of other anomalies and variants are summarized in Table 1. The pyramidal lobe was observed in 981 patients (693 women and 288 men; age 19–70 years; average age, 46.0 years) with a frequency of 44.6% (288/811 men, 693/1389 women). The mean AP diameter, transverse diameter, and length of the pyramidal lobe were 2.3, 5.9, and 20.8 mm, respectively. Among other anomalies and variants, accessory thyroids were detected in 44 patients (2%) at the upper level (n=26), mid-level (n=15), and lower level (n=3). Among 2200 patients, 17 cases of complete separation between the right and left thyroid lobes were found; there were no cases of thyroid aplasia or ectopic thyroid.
Data are presented as mean±SD or as n (%).
AP, anteroposterior.
The prevalence of the pyramidal lobe in patients at each institution is summarized in Table 2. The range of pyramidal lobe prevalence reported from participating institutions was between 28% and 55% (mean, 44.6%). A similar prevalence of pyramidal lobes was found in 3 and 8 participating institutions, respectively, and there was a statistical difference in the pyramidal lobe prevalence between institutions (95% confidence interval [CI] estimation for proportion). However, there was no significant difference in pyramidal lobe prevalence between age subgroups (p>0.05, chi-square test and Cochran-Mantel-Haenszel test).
CI, 95% confidence interval.
The comparison of pyramidal lobe prevalence between men and women is shown in Table 3. There was a statistical difference in the frequency, patient age, separation, AP diameter, and the level at which the upper end of the pyramidal lobe was detected between the sexes (p<0.05, chi-square test, Fisher's exact test, Cochran-Mantel-Haenszel test, and Student's t-test). The locations of the pyramidal lobes were right (n=275, 28.0%), midline (n=252, 25.7%), left (n=426, 43.4%), and bilateral (n=28, 2.9%). Pyramidal lobes originating from the left side of the thyroid were most common, and the difference between men and women was statistically significant (p=0.0467, chi-square test). The number of pyramidal lobes showing separation from the main thyroid gland was 90 (19 men, 71 women), and the remaining cases (n=891) showed continuity with the main thyroid gland (269 men, 622 women); there was no significant difference in the continuity or separation of the thyroid gland between men and women (p=0.0714, chi-square test). In terms of pyramidal lobe size, there was only a significant difference in the AP diameter of the pyramidal lobe between men and women (p=0.0328, Student's t-test). Among patients with pyramidal lobes, there was no significant difference in the AP diameter of the main thyroid between men and women (p=0.6405, Student's t-test), but there was a significant difference in the AP diameter of the isthmus (p=0.0005, Student's t-test).
Data are presented as mean±SD or as n (%). p-Values of significant difference between men and women, by chi-square test, Fisher's exact test, Cochran-Mantel-Haenszel test, and Student's t-test (two-tailed) with statistical significance set at α=0.05.
Data for the upper end of the pyramidal lobe are summarized in Table 4. Among both men and women, the most common level of the upper end of the pyramidal lobes was the thyroid cartilage, but there was a significant difference in the level of the upper end of the pyramidal lobe between men and women (p<0.0001, Fisher's exact test). However, there was no statistical difference in the location of the upper end of the pyramidal lobe between the age subgroups (p=0.1275, Fisher's exact test).
Data are presented as n (%). p-Values of significant difference between the level of upper end, by chi-square test and Fisher's exact test, with statistical significance set at α=0.05.
Each institution used a different slice thickness for neck CT scans, including 2 mm (367/2200, 16.7%), 2.5 mm (747/2200, 33.9%), and 3 mm (1086/2200, 49.4%) (Table 5). The detection rate of the pyramidal lobe was higher using a 2-mm slice thickness (53.7%) than using a thickness of 2.5 mm (44.4%) and 3 mm (41.6%). There was a statistical difference in the slice thickness between patients with and without a pyramidal lobe (p=0.0003, chi-square test), but there was no statistical difference in the location, level of upper end, or separation of the pyramidal lobe according to different slice thicknesses (p>0.05, chi-square test).
Data are presented as n (%). p-Values of significant difference between slice thickness of neck CT, by chi-square test and Fisher's exact test with statistical significance set at α=0.05.
CT, computed tomography.
Discussion
The thyroid gland is an endocrine organ, located in the anterior neck and plays a critical role in the regulation of several metabolic functions (1). The pyramidal lobe reflects the inferior part of the thyroglossal duct, which is formed during the descent of the thyroid diverticulum from the floor of the pharynx (9,10). The anatomical anomalies or variants of the thyroid gland include the pyramidal lobe, accessory thyroid, ectopic thyroid, absence or separation of isthmus, and retrotracheal extension. (1 –10). The accessory and ectopic thyroids were distinguished in this study according to the presence or absence of the main thyroid in a normal thyroid fossa.
The thyroid gland has an attenuation of ∼120 Hounsfield units on CT scans due to its high iodine concentration. This feature makes it easily identifiable, although its CT appearance can be affected by several conditions such as Graves' disease, Hashimoto thyroiditis, adenoma, or malignancy (11). Rather than neck CT, thyroid US has been used worldwide for the evaluation of thyroid abnormality (12). However, Braun et al. (3) have emphasized that detection of the pyramidal lobe in the preoperative evaluation is important to prevent the presence of residual thyroid tissue during total thyroidectomy. Furthermore, preoperative neck CT is valuable in identifying the presence of calcification, cysts, necrosis, or hemorrhage of the thyroid nodules; in determining the margin of the lesion and invasion to adjacent organs; and in assessing lymph node metastasis to the neck or mediastinum (13). To the best of our knowledge, no data on the sonographic detection of thyroid pyramidal lobes or accessory thyroid tissue have been reported as of yet, although US does not have a radiation hazard unlike CT. However, thyroid US may be able to replace neck CT in the preoperative evaluation of the thyroid pyramidal lobe or other thyroid variations in patients with thyroid cancer.
Reported frequencies of pyramidal lobe occurrence range from 15% to 75% (2 –7). In a previous single-center study using 3-mm slice-thickness neck CT, the pyramidal lobe was observed in 41.3% (135/327) of cases, was more common in the left thyroid gland (54.1%, 73/135), was bilateral in 1.5% (2/135) cases, and was separated from the main thyroid gland in 12.6% (17/135) cases (8). In the present study, the pyramidal lobe was observed in 44.6% (981/2200) of cases, was more common in the left thyroid gland (43.4%, 426/981), was bilateral in 2.9% (28/981) cases, and was separated from the main thyroid gland in 9.2% (90/981) cases. Thus, there was no significant difference in the frequency, left-side predominance, bilaterality, or rate of pyramidal lobe separation between the previous single-center study and the present multicenter study. Based on data from neck CT scans, the rate of bilaterality of the pyramidal lobe, in both this study and the previous single-center study, was lower than that in previous reports based on anatomical studies of cadavers, which reported rates ranging from 3.3% to 10% (5 –7). The low bilaterality rate in this study could be related to the study criteria that excluded patients with small pyramidal lobes <6 or 9 mm in length.
We observed that pyramidal lobe characteristics between men and women differed significantly with respect to frequency, age, location, AP diameter of the pyramidal lobe, level of the upper end, and AP diameter of the isthmus. The frequency, AP diameter of the pyramidal lobe, and AP diameter of the isthmus were higher in women than in men. However, in the previous single-center study, there was no significant difference in frequency, age, location, AP diameter of the pyramidal lobe, or level of the upper end between sexes (8). The reason for the difference in the results between the single-center and this multicenter study is not clear, but it may be related to the selection bias of a single-center study or the inclusion of multiple readers and 2- or 2.5-mm slice thickness used in CT scans in the multicenter study. In particular, there is a significant difference in the level of the upper end of the pyramidal lobe between men and women in this study; it is possible that the thicker AP diameter of the isthmus in women enabled a better delineation of the pyramidal lobe on CT when using a 2- or 2.5-mm slice thickness.
Although 3 different slice thicknesses (2, 2.5, and 3 mm) were used in the CT scans in this study, more accurate analysis might have been possible with thinner slices. The rate of detection of the pyramidal lobe was higher when the slice thickness was 2 mm rather than 2.5 or 3 mm. However, there was no significant difference in the location, the level of the upper end, or the separation of the pyramidal lobe between the three slice thicknesses. This observation could be related to the fact that pyramidal lobes <9 mm in length were excluded from the 3-mm slice-thickness group, while only pyramidal lobes <6 mm in length were excluded from the 2-mm slice-thickness group. Therefore, accurate evaluation for smaller-sized anomalies or variations of the thyroid may require neck CT scans with thinner slices.
Our study has several limitations. First, the patients underwent neck CT scanning for various reasons, including head and neck abnormalities; thus, they may not represent the general population. Furthermore, patients aged <19 years and >70 years were not included in this study. Neck CT was the only tool used in this study, and the results of the neck CT scans were not compared to those of other modalities such as ultrasonography or radioisotope scan. Finally, different neck CT modalities and protocols, including slice thickness, were employed in this study.
In conclusion, our study indicates that neck CT is useful for detecting the presence, size, configuration, and location of the pyramidal lobe and other thyroid variations.
Footnotes
Acknowledgment
The statistical consultation was supported by the Catholic Research Coordinating Center of the Korea Health 21 R&D Project (A070001), Ministry of Health & Welfare, Republic of Korea.
Disclosure Statement
The authors declare that no competing financial interests exist.