
Abstract
Background:
Graves' ophthalmopathy (GO) develops or worsens in up to one-third of patients treated with radioactive iodine (RAI) for Graves' hyperthyroidism. We sought to identify the prevalence of development or worsening of GO in patients treated with RAI for Graves' hyperthyroidism and to identify the risk factors associated with that outcome.
Methods:
We identified a retrospective cohort of consecutive patients treated with RAI at Mayo Clinic (Rochester, MN) between 2005 and 2006. We assessed their medical records for evidence of hypothyroidism and development or worsening of GO in the year after therapy. Hypothyroidism was defined as thyrotropin >3.0 mIU/L or free thyroxine <0.8 ng/dL.
Results:
We identified 291 consecutive patients who received RAI therapy during the study period, with 195 out of 291 having complete follow-up data for a one-year period. GO was present in 46 out of 195 patients (23.6%) at baseline. After RAI treatment, GO developed or worsened in 25 out of 195 patients (12.8%) and it was associated with hypothyroidism at first follow-up (p=0.011) with an odds ratio (OR) of 3.3 [95% confidence interval (CI) 1.3–8.7]. More smokers than nonsmokers developed new or worse GO (17.7% vs. 11.8%), but that difference did not reach statistical significance (p=0.35). Preexisting GO (24% of patients) was associated with a higher risk for negative GO outcome compared with patients who had no GO at baseline (11%; p=0.021). Both development of hypothyroidism by the first visit after RAI therapy (OR 3.6) and preexistent GO (OR 2.8) remained significant in a multivariate analysis. Development of hypothyroidism was more likely in patients with longer duration to first follow-up (p<0.001). By 6–8 weeks after RAI treatment, the prevalence of hypothyroidism was ∼40%, while that of hyperthyroidism was only 20%.
Conclusions:
The presence of hypothyroidism at the first assessment of thyroid function after RAI administration is a strong predictor for adverse GO outcome. This risk is highest in patients with preexisting GO. We suggest that in order to prevent clinical hypothyroidism and the associated risk for GO, the optimal time for first measurement of fT4 is before 6 weeks after RAI therapy.
Introduction
Methods
Overview and study design
We assembled a retrospective cohort of GD patients treated with RAI for hyperthyroidism and reviewed their medical records or used a telephone questionnaire regarding development or worsening of GO in the year after this treatment.
Setting and participants
We used the Mayo Clinic electronic medical records to identify all patients with GD who received RAI at Mayo Clinic (Rochester, MN) between January 1, 2005, and December 31, 2006. The RAI dose was chosen based on thyroid size and percent uptake with the goal of administering 0.2 mCi of 131I/g of thyroid tissue. The goal of therapy with RAI was induction of hypothyroidism. RAI treatment was delivered at Mayo Clinic, while the follow-up was performed at Mayo Clinic or by patients' local medical providers. We included all patients for whom thyroid status data and, if needed, eye exam data during the first 12 months post-RAI could be retrieved.
Intervention
We followed the patients for a total of 12 months (±3 months) for the development or deterioration of GO and for documentation of their thyroid status (or until biochemical hypothyroidism developed). In addition, we collected demographic information, smoking status, thyroid size, dose of RAI, use of antithyroid drugs, use of corticosteroids, and time to first follow-up. When available, the data were collected from the Mayo Clinic electronic medical records, which included all patients with preexisting GO who had continued follow-up with the ophthalmologists and/or endocrinologists at Mayo Clinic. Other patients (40% of the cohort) who did not have regular follow-up at Mayo Clinic were initially contacted by mail with a second mailing sent to those not answering within 2 months of the first request. Patients who requested a telephone interview in their mailing response or who did not respond to the second mailing were contacted by telephone by one of the physician investigators. Mailed inquiries and telephone interviews were conducted by one of the physician investigators (J.P.B., S.B., M.N.S.) who followed a uniform series of questions (Supplementary Data, available online at
Definitions
Hypothyroidism was defined as thyrotropin (TSH) >3.0 mIU/L or free thyroxine (fT4) <0.8 ng/dL. The diagnosis of GO was made only if confirmed by the patient's endocrinologist or ophthalmologist in the medical record. Worsening of GO at any point during the year of follow-up was diagnosed from medical records if two or more of the following had occurred: worsening of proptosis, diplopia, soft tissue features or visual acuity, need for systemic or surgical GO therapy, or if patient's self-assessment of disease indicated deterioration. This was primarily reflected by one or more of the following: increase in intensity of symptoms, increase in number of symptoms, decreased ability to perform daily activities, or decreased quality of social interaction. Soft tissue changes included changes in periorbital edema or erythema, chemosis, conjunctival injection, and caruncular changes. The documentation in the records made by the evaluating physician at the time was used to make that determination. For the final analysis, patients with GO were divided into two groups: (i) new or worsened GO; and (ii) unchanged or improved GO. Corticosteroid prophylaxis was defined as >2 weeks of treatment with a pharmacological dose of glucocorticoids (GCs). Hyperthyroidism after RAI treatment was defined as a suppressed TSH level with an elevated fT4 value. Euthyroidism or subclinical hyperthyroidism during follow-up was defined as having normal fT4 (0.8–1.8 ng/dL) with TSH between 0.1 and 3.0 mIU/L or TSH <0.1 mIU/L, respectively.
Ethics approval
The Mayo Clinic Institutional Review Board approved the protocol without the need for informed consent. Records of patients who had not given prior authorization to have their medical records reviewed for research purposes were excluded in compliance with Minnesota Statute. The authors of this article have certified that they comply with the Principles of Ethical Publishing (6).
Statistical analysis
Group statistics for the continuous variables were expressed as mean and standard deviation or median with interquartile range (IQR), depending on the normalcy of distribution. Categorical variables were summarized as percentages. Comparison between groups was based on two-sample t-test for continuous variables and Persons' chi-squared test for categorical variables. Univariate and multivariate analyses to identify potential risk factors for GO development or worsening were performed with the logistic regression model using SAS© software version 9.2. Results of these analyses were summarized as odds ratios (ORs), 95% confidence intervals (CIs), and p-values. p-Values were reported with three digits if <0.1.
Results
We evaluated a cohort of 291 GD patients who received RAI treatment for hyperthyroidism during the period January 2005 through December 2006. From these we excluded 96 patients from further analysis based on their refusal to allow access to their records, death, not being traceable by mail or not having complete thyroid or eye data for the year after RAI therapy. We have, therefore, included in the final analysis 195 patients (Fig. 1). These patients had evidence of GD for a median duration of 2 months (IQR 1–5 months) before they received treatment with RAI. We found the prevalence of GO at baseline to be 23.6% (46/195), with 38 patients having mild and 8 having moderate-to-severe GO. Smoking prevalence was 17.4% (34/195). The group consisted of 156 women (80%). Baseline characteristics of this cohort are described in Table 1. In a sensitivity analysis, we compared this cohort with the de-identified 2005 source cohort (including all patients except those who did not allow their data to be utilized for research purposes) and found age (mean for analyzed cohort 50.2±14.7 years vs. 51.3±15.5 years for the source cohort, p=0.4), sex distribution (women 80% vs. 74.1%, p=0.1), smoking percentage (17.4% vs. 13.2%, p=0.3), and thyroid size (35.1±10.7 g vs. 35.3±14.6 g, p=0.6) to be equivalent between the groups.
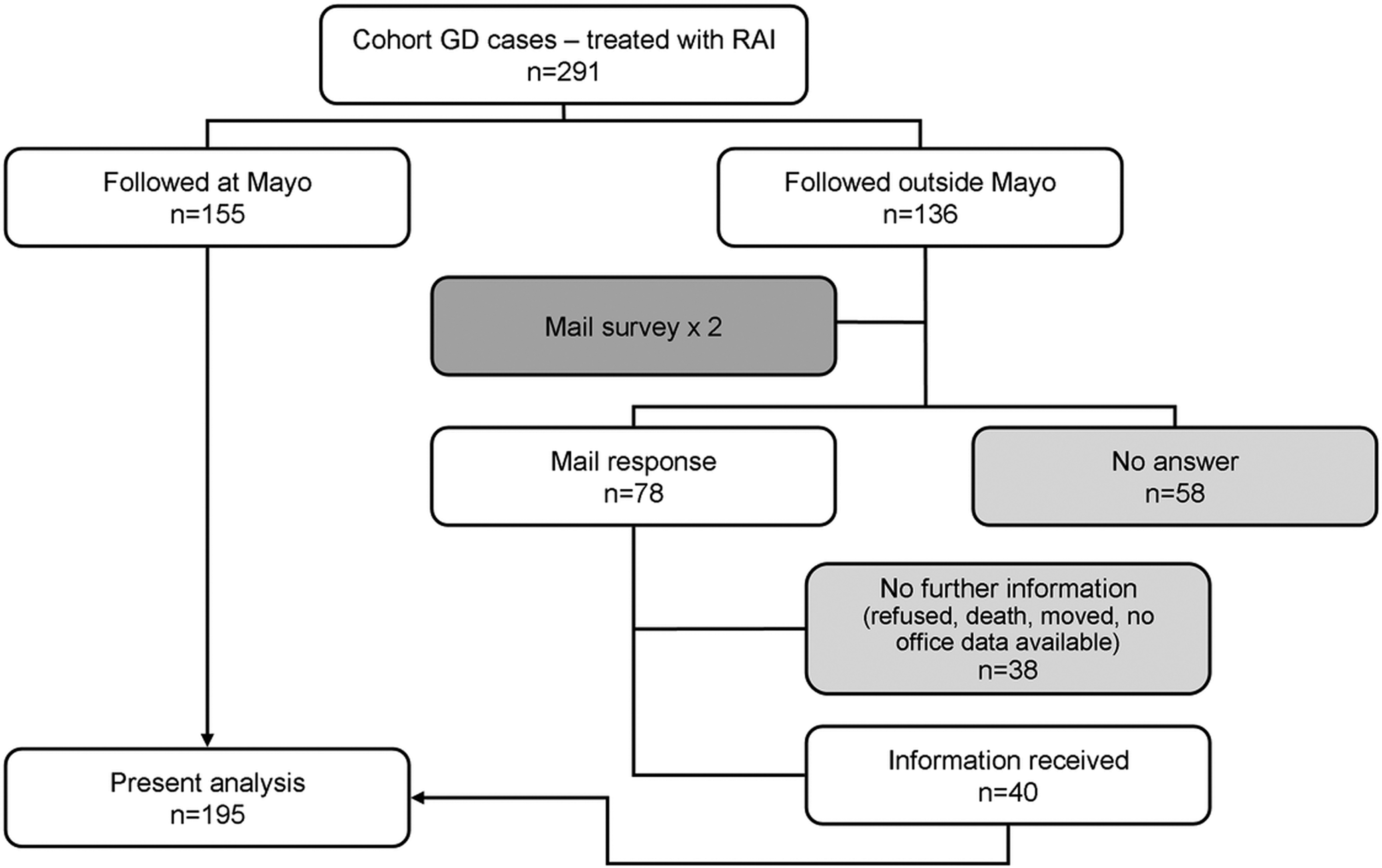
Flow of patients into the study.
GO, Graves' ophthalmopathy; SD, standard deviation; IQR, interquartile range; T3, triiodothyronine; TRAb, TSH receptor antibody; ATD, antithyroid drug; RAI, radioactive iodine.
After one year of follow-up, 39 patients carried a diagnosis of GO (20%), including 15 new GO cases and 24 preexisting cases. In the 46 out of 195 cases with GO at baseline, the eye disease subsequently deteriorated in 10 patients. In 9 out of 46 (19.63%) patients, the GO did not progress and in 27 out of 46 (58.7%) patients, it improved. Overall, after RAI treatment, GO developed or worsened in 25 out of 195 patients (12.8%). Of these, 4 required orbital surgery (decompression, 3; strabismus surgery, 1), and 2 patients required systemic GC therapy.
Hypothyroidism was present at the first follow-up visit in 102 out of 195 (52.3%) patients and was strongly associated with GO development or deterioration with an OR of 3.3, [CI: 1.3–8.7], p=0.011 (Fig. 2). Given the controversy surrounding the upper limit for a normal TSH value, we conducted a sensitivity analysis with the cut-off point set at 4.5 mIU/L. The results were essentially the same, as the classification changed in only two patients (OR 3.5 [CI 1.3–9.1]). More smokers than nonsmokers developed new or worse GO (17.7% vs. 11.8%) during the year after RAI, but that difference did not reach statistical significance (p=0.35). GCs were selectively used in patients with active preexistent GO, in smokers with GO or in patients already taking GC for other conditions. The average dose (prednisone) was 0.5 mg/kg (range 0.2–0.8), and it was used for 9 weeks on average (range 2–16). No GC side-effects were reported.
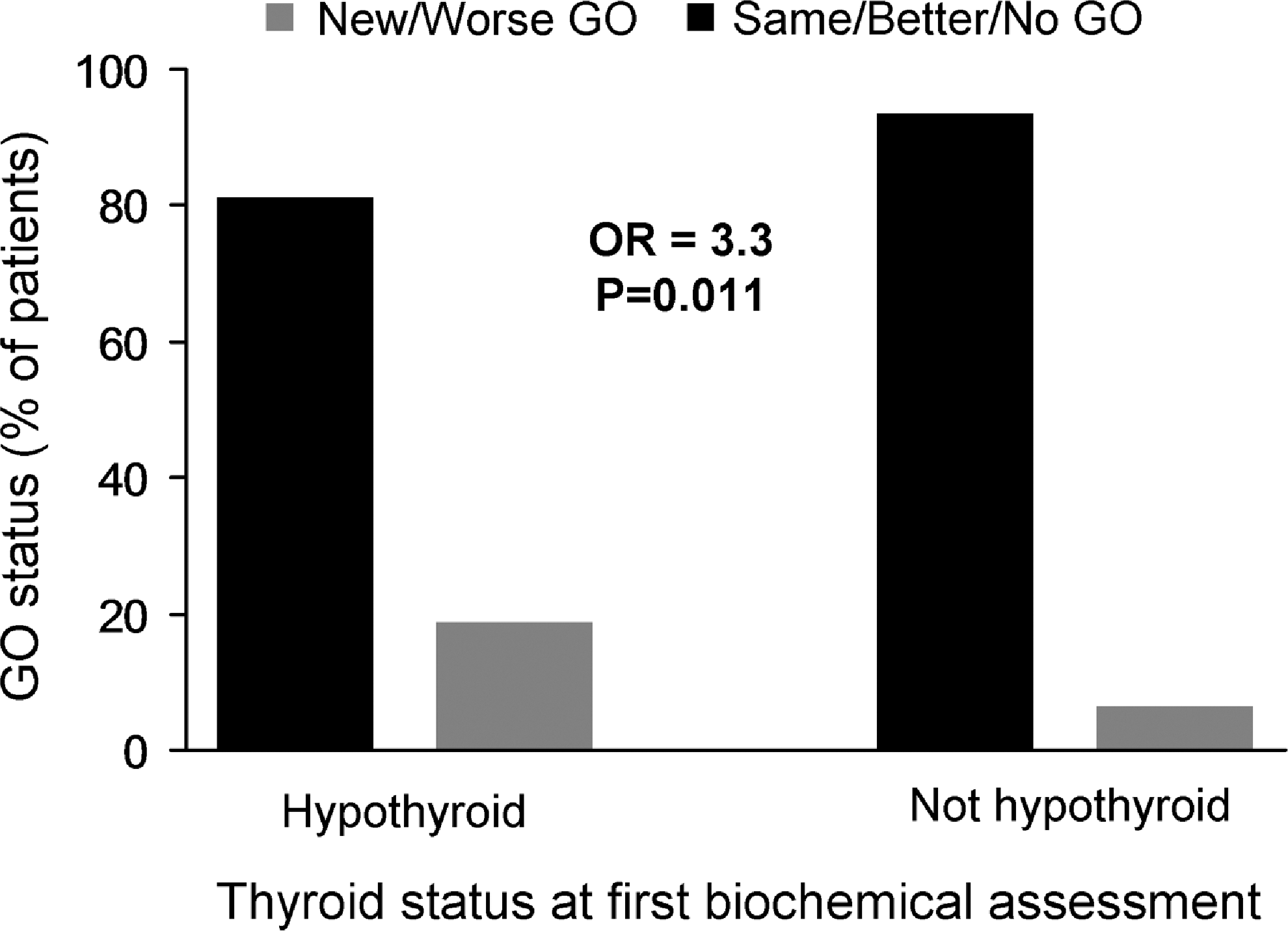
Graves' ophthalmopathy (GO) changes correlated with thyroid status at first biochemical assessment. The odds ratio (OR) is derived from the multivariate analysis detailed in Table 2. Hypothyroidism at the first follow-up was present in 102 patients (52%), while GO developed or deteriorated in 25 patients (13%).
In our cohort, only 3 out of 149 patients without GO at baseline received GC for prophylaxis, and none of those developed GO. The risk for GO deterioration was not decreased in patients treated with prophylactic GC who had preexisting GO at baseline (p=0.60). Preexisting GO was associated with a higher risk for a negative GO outcome compared with patients who had no GO at baseline, as 24% of patients with GO at baseline experienced deterioration, while 11% of patients with no GO at baseline developed GO (p=0.021). A multivariate analysis was performed and included hypothyroid status at the first follow-up, steroid prophylaxis, smoking status, fT4 at baseline, sex, age, 24-hours RAI uptake, thyroid size, and dose of RAI. The factors that remained independently significant were development of hypothyroidism by the first follow-up visit after RAI therapy (OR=3.6) and preexisting GO (OR=2.8) (Table 2).
Reference for statistical comparison: ahyper/euthyroid; bno; cnonsmoker.
CI, 95% confidence interval.
Time to first visit after RAI therapy in our cohort was a median of 69 days (IQR 53–88). As expected, patients who were hypothyroid at the first follow-up had a longer time period between RAI treatment and first follow-up (median 81 days, IQR 63–96) compared with those who were not hypothyroid at the first visit (median 57 days, IQR 39–74, p<0.001). In multivariate analysis, duration to first follow-up remained a predictor of hypothyroidism with an OR 1.05/day increase in follow-up time [CI 1.03–1.07]. The only other parameter that was found to be inversely associated with hypothyroidism development by the time of the first follow-up was the size of the thyroid (OR for hypothyroidism=0.97/g increase in thyroid weight [CI 0.93–0.99]).
We divided the cohort based on time to follow-up into six groups: those seen within 6 weeks of RAI, between 6 and 8 weeks, 8 and 10 weeks, 10 and 12 weeks, 12 and 16 weeks, and >16 weeks. We compared the prevalence of hypothyroidism between the groups as well as the persistence of overt hyperthyroidism (Fig. 3 and Table 3). We found that the prevalence of hyperthyroidism decreased as expected between the groups (p<0.001), and dropped below 25% in groups with first follow-up after 6 weeks. In order to better understand the positive and negative outcomes for each specific follow-up period, we calculated the ratio between euthyroidism and hypothyroidism at each time to follow-up. We found the ratio to drop below 1.0, favoring hypothyroidism, starting from follow-up period of 8–10 weeks and then to decrease linearly thereafter.
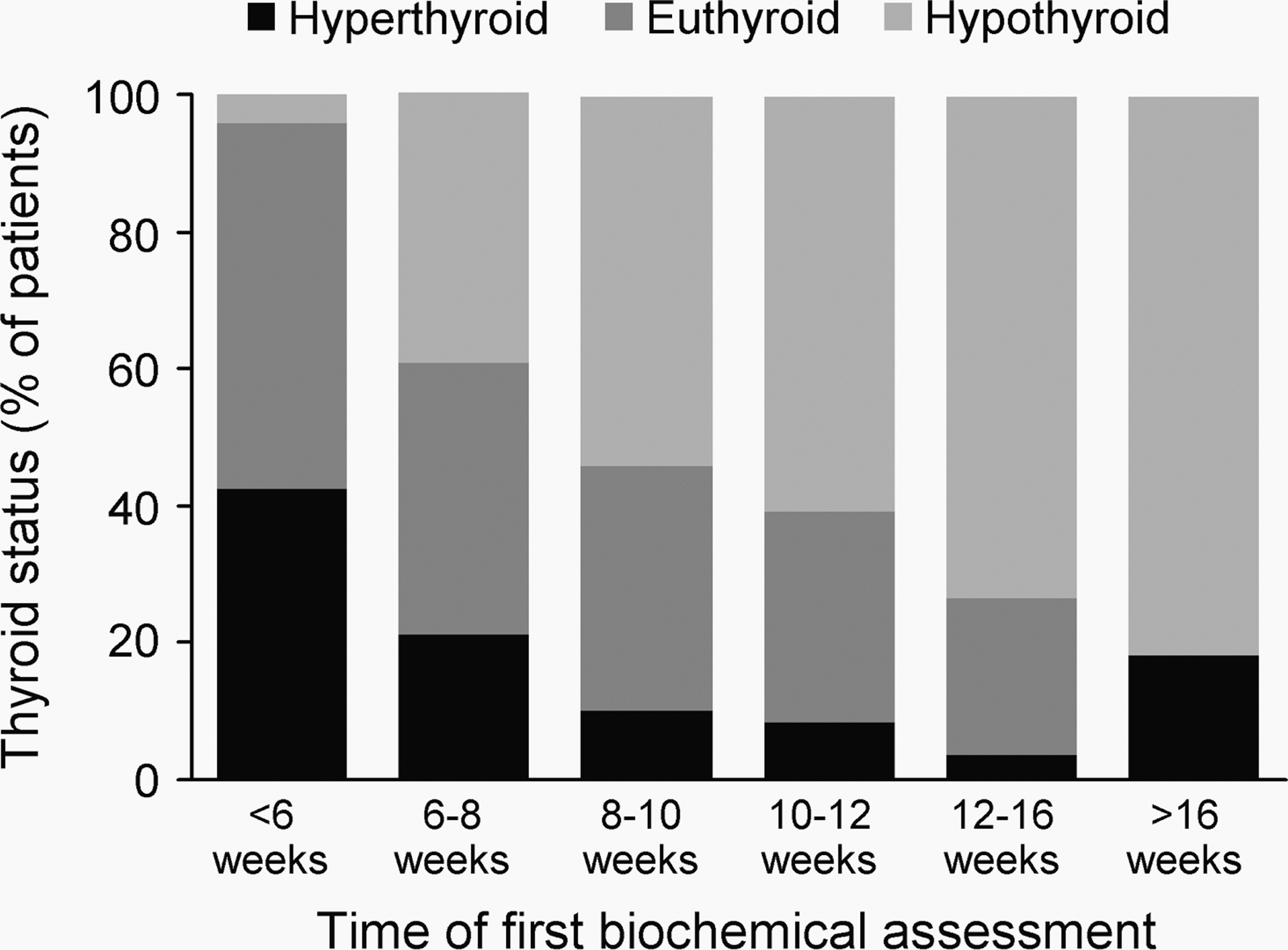
Distribution of thyroid status after radioactive iodine treatment, at the time of first biochemical assessment. Patients with normal free thyroxine and still suppressed thyrotropin were included in the euthyroid group. Patients evaluated after 16 weeks missed their initial recommended evaluation.
Discussion
While RAI therapy is associated with an increased risk for GO development or deterioration (1,2,7), the risk factors for this outcome are incompletely defined. In the current study, we confirmed that the presence of hypothyroidism at the first follow-up post-RAI therapy is a factor strongly associated with GO development or deterioration. We also demonstrate that the development of hypothyroidism by the first follow-up is closely related to the time interval to that follow-up. An association between hypothyroidism and GO was first suggested by Almqvist et al. (8). Subsequently, Tallstedt et al. (5) noted that early administration of L-T4 was associated with a reduction in development or deterioration of GO. However, their data do not support TSH elevation as the cause for GO changes. Other studies showing prevention of GO deterioration post-RAI with early L-T4 therapy (9) and decrease TSH receptor antibody (TRAb) levels with addition of L-T4 therapy to antithyroid therapy (10) suggest that the deficit of thyroid hormone itself might be a factor in GO development. In addition, the study by Perros et al. (9) concluded that prevention of hypothyroidism in patients with minimally active or inactive eye disease is protective against GO deterioration and that these patients can undergo RAI therapy without concurrent steroid prophylaxis if hypothyroidism is avoided. In accordance, the American Thyroid Association (ATA) guidelines for the management of hyperthyroidism recommend avoidance of biochemical hypothyroidism (11), a recommendation in agreement with the European Group on Graves' Orbitopathy consensus statement on the management of GO (12).
While smoking is a well-established risk factor for GO development or deterioration (13), we did not find it to be predictive of GO development or deterioration in our cohort. This is likely due to the low prevalence of smokers in our population [18% for Olmsted County (14) and 17.4% in our study, compared with ≥40% for other studies (1,2)]. Nevertheless, encouraging these patients to pursue a dedicated smoking cessation program represents an important component of GO management, based on previous data.
In our study, prophylactic corticosteroid treatment in parallel with RAI administration was not protective for GO development or worsening. This finding runs counter to several other studies showing a protective effect (1,15) and likely reflects selection bias, because it was our practice at Mayo Clinic during the years covered by this study to offer prophylactic steroids only to GO patients deemed at high risk for deterioration.
We found that the risk for disease progression in patients with GO at baseline is higher than the risk of disease development in patients with no baseline GO. This finding underlines the importance of avoiding RAI therapy in moderate-to-severe and active GO cases, as recommended by the ATA guidelines (11). On the other hand, consistent with previous data (1,7,16), the majority of patients with preexistent GO improved by the end of the follow-up period. In addition, the distribution of new GO (10 cases) versus worsened GO (15 cases) places our results somewhere between those of Bartalena et al. (1) (mainly preexistent GO) and Traisk et al. (2) (mainly new GO), and probably relates to the specifics of our population and practice.
The follow-up interval after RAI therapy is at present a matter of personal preference among endocrinologists. While some take a proactive stance and schedule patients for follow-up at 6 weeks, others wait for 3 months in order to ensure that the patients are hypothyroid before initiating L-T4 therapy while others prevent hypothyroidism altogether by initiating L-T4 therapy at 2 weeks post-RAI (5,9). We consider this last approach as the most appropriate method for preventing GO deterioration in those with preexistent GO. If early L-T4 therapy is not initiated, we suggest that the optimum interval for first follow-up is at a time when there is a relatively low rate of residual hyperthyroidism combined with a high ratio of euthyroidism. This approach minimizes both the risk of GO development/worsening and the symptoms associated with hypothyroidism. Assessing fT4 levels before 6 weeks demonstrated hyperthyroidism in 43% of patients, yet the majority of patients were euthyroid by that time and only one patient (3.6%) was hypothyroid. Therefore, our data support the assessment of T4 levels earlier than 6 weeks after RAI therapy, as 40% of patients were already hypothyroid when tested between 6 and 8 weeks. Patients still hyperthyroid at first follow-up could be reassessed every 1–2 weeks, and hormone therapy can be initiated once fT4 levels normalize. While not examined in this study, clinical experience would suggest that the optimum time to begin testing is between 3 and 5 weeks. Assuming that measurement of fT4 would have 100% efficacy at preventing overt hypothyroidism, we have determined that in our population 28 patients would need testing before 6 weeks in order to prevent 10 cases of hypothyroidism (number needed to treat [NNT]=2.8). Concern that early L-T4 therapy may cause symptomatic hyperthyroidism was addressed in previous reports (5,9), showing that early L-T4 therapy (started at 50 μg daily 2 weeks after RAI treatment) required discontinuation due to symptoms of thyrotoxicosis in only 7 out of 314 patients (2.2%).
Our study has a number of limitations. We acknowledge that the relatively small number of outcome events identified (25) limits the number of predictors that can reliably be evaluated, as 10 events per predictive variable are generally required (17). The retrospective nature of our cohort also limits the availability of some parameters, particularly TRAb titers. It also limits our ability to further qualify some parameters, including the functional scoring of diplopia, clinical activity score (CAS), or the severity of GO. In order to minimize the risk of selection bias, we contacted all 40% of the identified cohort patients who were followed for some part of the year outside of Mayo Clinic. We were able to obtain data for 1 out of 3 of this group, limiting, but not eliminating, the impact of this bias on our results. In a sensitivity analysis, we found that GO outcome was actually worse for patients followed outside Mayo (24% vs. 9%, p=0.001), with a trend toward more hypothyroidism in that outside group (58% vs. 49%, p=0.3), arguing against surveillance bias. The possibility of diagnostic bias was limited by our high threshold for diagnosing GO deterioration, using the same criteria as utilized in other studies (3). We required the presence of objective evidence for GO deterioration beyond patients' self-assessment. Future prospective studies will be able to mitigate these limitations as well as include CAS, GO severity, TRAb, and quality of life in the data collection for a more informative analysis.
In conclusion, we have identified the presence of hypothyroidism at the first biochemical assessment after RAI administration as a strong predictor for GO deterioration or development of new GO. This risk is highest in patients with preexisting GO. We suggest that in order to prevent clinical hypothyroidism and the associated risk for GO, the optimal time for first measurement of fT4 is before 6 weeks after RAI therapy.
Footnotes
Disclosure Statement
The authors have no competing financial interests to disclose.