
Abstract
Background:
The diffuse sclerosing variant of papillary thyroid carcinoma (DSV-PTC) is a unique variant of PTC that is characterized by extensive lymphovascular invasion of tumor cells in a background of lymphocytic thyroiditis. The lymphatic emboli contain tumor cells as well as macrophages, but the recruitment of these macrophages is not well understood. The aim of this study was to determine the relationship between the expression of Decoy receptor 3 (DcR3), the recruitment of tumor-associated macrophages (TAMs), and lymphatic invasion in DSV-PTC.
Methods:
We retrospectively examined 14 cases of DSV-PTC using immunohistochemistry studies. The density of TAMs, lymphatic vessel density, lymphatic invasion, tumor emboli area, and DcR3 expression were assessed. Statistical analyses were performed using Fisher's exact test, unpaired t-test, and linear regression.
Results:
The lymphatic tumor emboli contained a relatively higher density of TAMs than stroma and classical PTC (CPTC) areas. In addition, the number of lymphatic invasions and the size of the tumor emboli area were positively correlated with the number of M2 TAMs. A higher density of M2 TAMs was associated with older patients and larger tumor size. Moreover, DcR3 was expressed only in lymphatic tumor cells and squamous metaplastic tumor cells, but not in macrophages and CPTC. In addition, the preferential expression of DcR3 in tumors was associated with higher levels of M2 TAMs and lymphatic invasion.
Conclusion:
Despite the fact that the exact relationship between DcR3, M2 macrophages, and lymphatic invasion in DSV-PTC remains to be elucidated, our findings suggest that DcR3 expression in DSV-PTC tumor cells may promote the polarized macrophage differentiation toward the M2 phenotype. This phenomenon may further promote lymphatic invasion of DSV-PTC tumor cells.
Introduction
In a preliminary study, we found that the lymphatic tumor emboli in DSV-PTC are mixed together with many macrophages. This peculiar phenomenon evoked our interest to investigate the role of these tumor-associated macrophages (TAMs). TAMs have been previously described in various malignant tumors, including carcinomas of the lung (3,4), pancreas (5,6), larynx (7), endometrium (8), kidney (9), and colorectum (10), as well as in lymphomas (11,12). However, the functional role of TAMs in thyroid cancer was not clear until the publication of two recent reports (13,14), in which TAM infiltration was significantly increased in poorly or undifferentiated carcinomas, and was associated with poor prognosis in these patients.
It has been known that M1-polarized macrophages show tumor-suppressive functions and are capable of killing microorganisms or tumor cells, whereas M2-polarized macrophages, in contrast, display tumor-supportive functions and have important roles in angiogenesis, lymphangiogenesis, matrix remodeling, and tumor metastasis. Furthermore, higher densities of M2-polarized macrophages are associated with more aggressive behavior and poor outcome in many malignant tumors (4 –6,9,11 –13). Recent studies have shown that Decoy receptor 3 (DcR3) is capable of modulating macrophage differentiation toward the M2 phenotype (5,15), specifically by down-regulation of MHC class II expression in TAMs.
In this study, we describe a unique phenomenon of preferential expression of DcR3 and dominant infiltration of M2 macrophages in DSV-PTC, which significantly correlates with the peculiar pattern of massive intralymphatic growth in this tumor.
Materials and Methods
Clinicopathological analysis
We retrieved a total of 14 surgical cases of DSV-PTC from 1020 cases of PTC in our pathology archive of Taipei Veterans General Hospital. The pathology slides were reviewed by two authors (W.-C.C. and A.-H.Y.), and the pathological diagnosis of DSV-PTC was based on the criteria described in the 2004 World Health Organization (WHO) scheme (16). All cases in this study group were staged according to the AJCC/UICC TNM system (17). All patient material was processed following the ethics regulations of the Institutional Review Board of the hospital. The clinical and follow-up data were collected by reviewing the patient's medical records. For patient management, we generally follow the guidelines of the American Thyroid Association (18). In addition to total thyroidectomy, prophylactic central LN dissection (LND) was performed unless there was a high risk of permanent hypoparathyroidism or to prevent injury to the recurrent laryngeal nerve. Therapeutic central and lateral LND were performed if the LN was palpable or if biopsy of nodes was positive for metastasis. Adjuvant radioactive iodine (RAI) ablation is usually applied for high-risk types of PTC. The dosimetry of RAI therapy was adjusted if metastasis existed. External beam radiotherapy was usually chosen for tumors not responsive to RAI treatment. Chemotherapy was considered if other treatment modalities failed. Patients who were alive and without clinical or pathological evidence of disease recurrence or metastasis on the latest follow-up were designated as AND (alive no disease), while those with clinical (confirmed by RAI whole-body scan) or pathological (confirmed by cytologic or histopathological examination) evidence of recurrent or metastatic disease on the latest follow-up were designated as AWD (alive with disease).
Immunohistochemical and morphometric analyses
We performed immunohistochemical staining on 4 μm formalin-fixed paraffin-embedded tissue sections following routine procedures. The working conditions of primary antibodies are listed in Table 1. All sections were labeled using a polymer-HRP staining kit (BOND™; Leica Microsystems, Wetzlar, Germany), and double staining for CD68/CD163 and DcR3/TTF-1 was labeled using an additional polymer-AP staining kit (BOND; Leica Microsystems). Adequate immunoreactive tissue samples from the tonsils and lungs were used as positive controls. Sections stained without the primary antibody were used as negative controls. The stained sections were digitized using a Nikon DS-Fi1 digital microscope camera, and analyzed using ImageJ software (v. 1.44, National Institutes of Health).
HIER, heat-induced epitope retrieval; DcR3, Decoy receptor 3.
Macrophages within the tumor emboli, stroma, or classical PTC (CPTC) were separately assessed by CD68 staining. M2 macrophages were identified by CD163 staining. Sections were initially scanned at low magnification (100×) to identify the areas with the highest density of TAMs (TAM hot-spots). Average TAM count was assessed by counting a minimum of five TAM hot-spots at 200× (0.28 mm2) magnification on the digitized photomicrograph. The total area of lymphatic tumor emboli was measured to calculate the actual macrophage density.
Lymphatic vessel density (LVD) was defined as the mean D2-40 positive lymphatic channels in five random 100× (1.12 mm2) fields. The lymphatic invasion index (LI) was defined as the average number of tumor cell–containing D2-40–positive lymphatic channels in five random 100× fields. The tumor emboli area was defined as the average area of lymphatic tumor emboli in five random 100× fields.
The expression of DcR3 was defined as the percentage of cells with unequivocal cytoplasmic staining. The tumors expressing low levels of DcR3 were defined as <10% of total tumor cells with positive cytoplasmic staining, whereas the other tumors were classified as high-expressing tumors. Co-localization of DcR3 and TTF-1 was assessed by double staining.
Statistical analysis
Statistical analyses were performed using the Statistical Product and Service Solutions (v. 19.0; SPSS, Chicago, IL) and GraphPad Prism (v. 5.0; La Jolla, California, USA). The median value of macrophage count was used as a cut-off point to dichotomize the continuous variables. Fisher's exact test was used to compare between categorical variables, and unpaired two-sided t-test was used to compare between continuous variables. Linear regression was used to analyze the correlation between two continuous variables. A value of p<0.05 was considered statistically significant.
Results
Clinicopathological findings
The clinicopathological features of the 14 DSV-PTCs are summarized in Table 2. In brief, the average age of patients at initial presentation was 35.4 years (range 13–61 years), and there was a female predominance (F:M=3.7:1). All patients received total thyroidectomy with or without LND. Eight patients received additional RAI treatment, and three received additional radiotherapy and/or chemotherapy. The mean follow-up time was 47 months (range 1–165 months). In addition to the typical histopathological features of DSV-PTC (Fig. 1A, B), five cases also harbored a main tumor mass consisting of CPTC (Fig. 1C). Extrathyroid extension was observed in 9 (64%) cases. Vascular invasion in the perithyroid tissue was found in 3 (21%) cases. Twelve (86%) cases had local cervical LN metastasis at initial presentation. Recurrence of tumor or LN metastasis on subsequent follow-up was observed in 5 (37%) cases. Distant metastases were noted in 3 (21%) cases, with the lung as the most common metastatic site. Nine tumors were classified as stage I (64.3%), 1 as stage II (7.1%), 2 as stage IVa (14.3%), and 2 as stage IVc (14.3%).

Histopathological features of diffuse sclerosing variant of papillary thyroid carcinoma (DSV-PTC).
Patients received radioactive iodine therapy.
Patients received radiation therapy and/or chemotherapy.
(m), multifocal tumor; AND, alive no disease; AWD, alive with disease, DOD, died of disease; ETE, extrathyroid extension; F, female; FU, follow-up; LN, lymph node; M, male; MTS, metastasis; NA, not available; VI, vascular invasion.
Distribution and quantity TAMs in DSV-PTC
CD68/CD163 double staining showed that TAMs are more concentrated in the lymphatic tumor emboli, with the majority (76%) of macrophages being of the M2 phenotype (Fig. 2A–C). Although macrophage density in stroma and CPTC were noticeably lower than in lymphatic tumor emboli (Fig. 2D), the proportions of M2 macrophages (M2/M ratios) were similar to those in lymphatic tumor emboli (Fig. 2E).
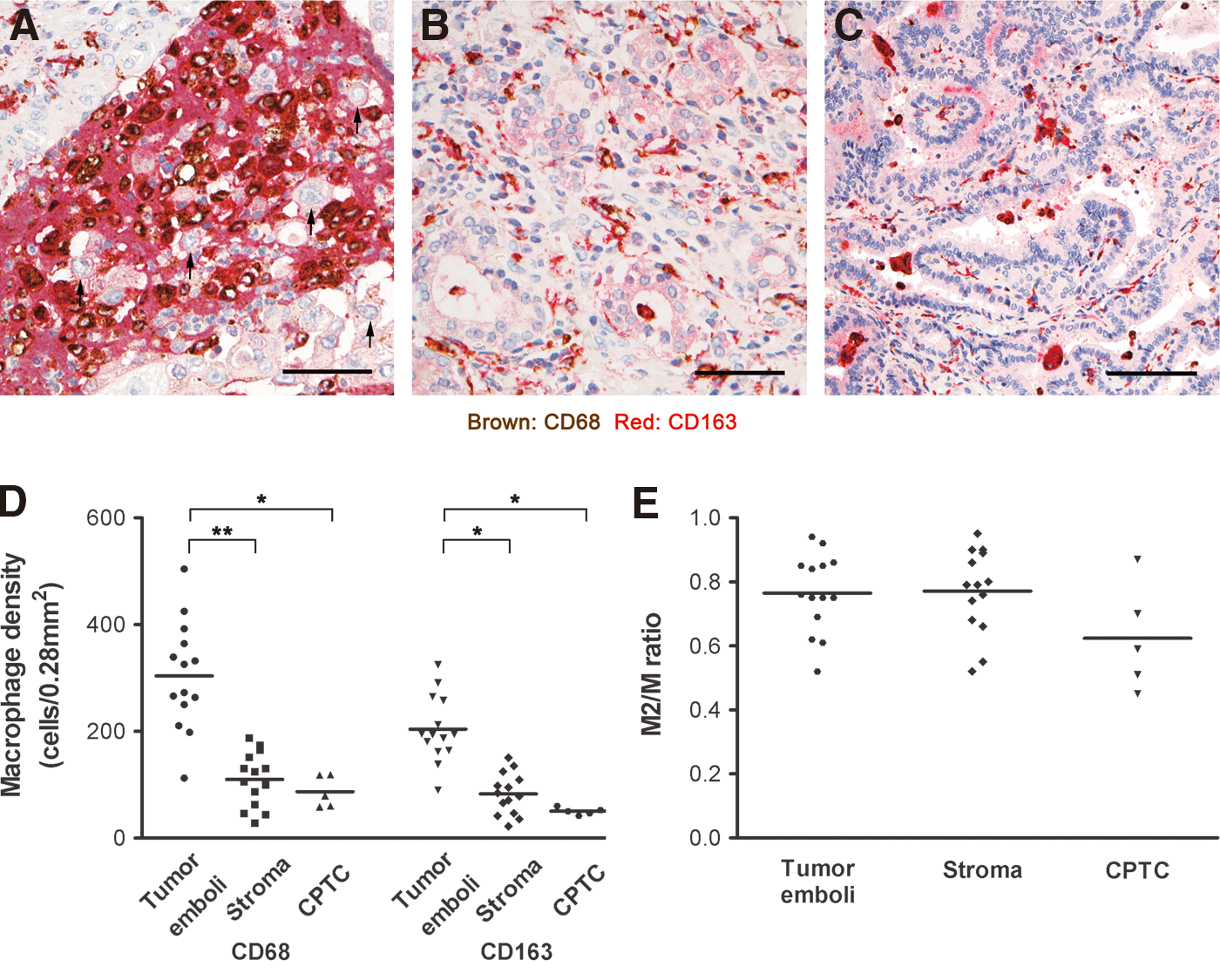
Distribution of CD68- and CD163-positive macrophages in DSV-PTC. Representative photomicrographs show double immunohistochemical staining of CD68- and CD163-positive macrophages in
Correlation between macrophage density and clinicopathological features
The median number of lymphatic TAMs was used to divide the cases into two groups, and the correlation to clinicopathological features are listed in Table 3. The M2 (CD163-positive) TAM density was significantly associated with older age (p=0.024) and larger tumor size (p=0.022), whereas total (CD68-positive) TAM density was not significantly associated with any clinicopathological factors.
p<0.05.
TAMs and lymphatic invasion in DSV-PTC
The increase in M2 TAMs was associated with an increase in lymphatic invasion (Fig. 3A) and size of tumor emboli (Fig. 3B), and to a lesser extent, LN metastases (Fig. 3C). LVD had an inverse relationship with the number of M2 TAMs (Fig. 3D).

Correlations between
DcR3 expression in DSV-PTC
Double staining for DcR3/TTF-1 indicated that DcR3 was exclusively expressed in DSV-PTC tumor cells and not in macrophages (Fig. 4A). In addition, the expression of DcR3 was confined to lymphatic tumor emboli (Fig. 4B) and tumor cells with squamous metaplasia (Fig. 4C), while CPTC (Fig. 4D) and nontumorous tissue was completely without expression. DcR3 expression was positively associated with M2 differentiation (Fig. 4D), lymphatic invasion (Fig. 4E), and size of emboli (Fig. 4F). A trend toward increased LN metastases (Fig. 4G) was also noted. However, LVD was lower in high DcR3-expressing tumors (Fig. 4H).
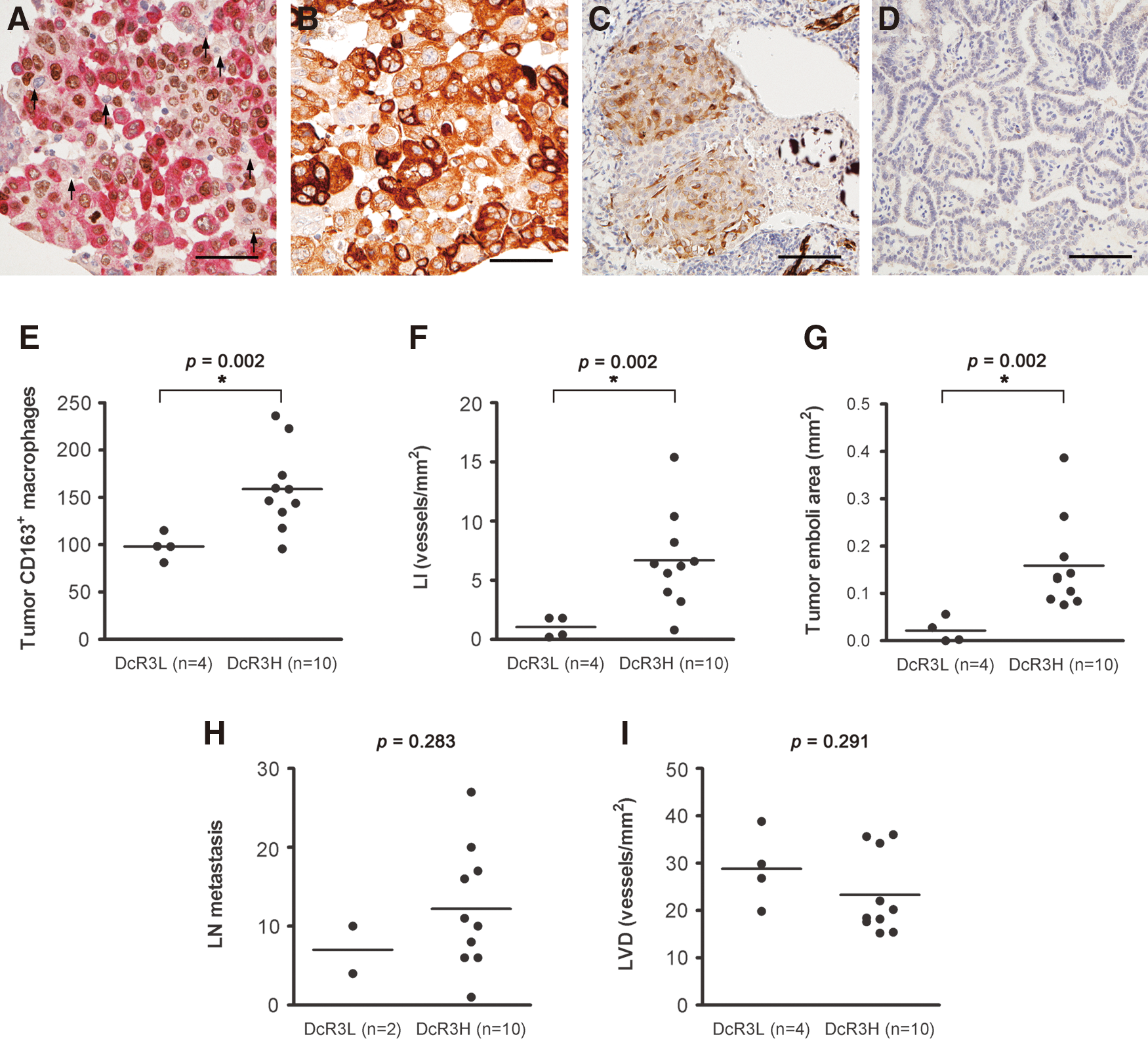
Decoy receptor 3 (DcR3) expression in DSV-PTC.
Discussion
Extensive lymphatic invasion with dilated lymphatic spaces filled with PTC cells is a prominent feature in DSV-PTC, and it is often the predominant histopathological growth pattern. Our study shows that the lymphatic emboli in DSV-PTC are, in fact, a heterogeneous population, consisting of tumor cells and macrophages. Moreover, the majority of these TAMs expressed CD163, a well-established marker for M2-polarized macrophages (19,20). There was also a strong correlation between increased M2 TAMs and lymphatic invasion, suggesting that M2 TAMs have an important role in the process of lymphatic invasion. In addition, higher levels of M2 TAMs were strongly associated with older age and larger tumor size, with a trend toward a higher pathological stage. Finally, the preferential expression of DcR3 in tumor tissue was associated with higher levels of M2 TAMs and lymphatic invasion, suggesting that DcR3 may induce polarized macrophage differentiation toward the M2 phenotype, which, in turn, promotes lymphatic invasion.
M2 macrophages have poor antigen-presenting capability, produce factors that suppress T-cell proliferation and activity, and are better adapted at scavenging debris, promoting angiogenesis, and tissue remodeling. Recently, Wyckoff et al. (21) reported that an EGF-CSF1 macrophage-tumor cell paracrine interaction may facilitate blood vessel invasion in breast cancer. Although it is conceivable that similar mechanisms may be responsible for the dominant lymphatic invasion in DSV-PTC, further studies are needed to prove this.
Although DcR3 expression is found in many cancers (5,22 –24), its role is not well understood. Recent studies have demonstrated that inflammation is a key factor in the induction of DcR3 expression, which was observed in epithelial cells in acute appendicitis (25) or Crohn's disease (26). In our study, DcR3 was expressed only in lymphatic tumor cells and squamous metaplastic tumor cells but not in macrophages and CPTC. We speculate that the inherent inflammatory microenvironment of DSV-PTC may be responsible for the induction of DcR3 expression in tumor cells. On the other hand, the lack of intimate contact between tumor cells and inflammatory cells in CPTC may explain the lack of DcR3 expression in CPTC tumor cells. Therefore, we further speculate that activation of the DcR3 gene may be a critical step in bridging the transformation from CPTC to DSV-PTC.
The major limitation of the current study is its shortage of DSV-PTC cases. As a result, certain clinicopathological parameters were not significantly correlated with tumor TAM density and DcR3 expression. Another limitation is the lack of long-term follow-up in some cases, which may have been the reason for lack of correlation between tumor TAM density and DcR3 expression with disease-free survival and overall survival of the patients. We anticipate that inclusion of additional cases and a longer follow-up time may produce more definitive results should these studies be performed.
In conclusion, our study revealed a close relationship between inflammation, DcR3 expression, M2 TAMs, and lymphatic invasion in DSV-PTC. Our results suggest that DcR3 may be a potential therapeutic target against lymphatic metastasis in this specific type of thyroid tumor.
Footnotes
Acknowledgments
This work was supported by Taipei Veterans General Hospital (V98C1-047) and the National Science Council (NSC96-2628-B-075-003 and NSC99-2320-B-075-002). The authors also thank Hsui-Hsun Ma, Li-Rung Liao, and Chih-Yang Chiu from the Department of Pathology and Laboratory Medicine, Taipei Veterans General Hospital for their technical assistance in immunohistochemistry studies.
Disclosure Statement
The authors declare that no competing financial interests exist.