
Abstract
Background:
Treatment of the symptomatic lingual thyroid is typically accomplished through surgical resection using a transcervical approach, which carries a high risk of treatment-related morbidity and leaves a visible scar on the neck. In order to reduce morbidity and eliminate visible scarring, this study utilized transoral robotic surgery (TORS) in performing lingual thyroidectomy.
Methods:
Between October 2009 and October 2010, three patients with symptomatic lingual thyroid were enrolled in this prospective study. Primary symptoms included dysphagia (two patients) and hemorrhage (one patient). A da Vinci robotic system (Intuitive Surgical, Inc., Sunnyvale, CA) was used to perform TORS in all patients. A face-up 30° endoscope was inserted through the oral cavity, and two instruments were positioned on either side of the endoscope. We evaluated the robotic set-up time, operating time, volume of blood loss, surgery-related complications, postoperative symptomatic improvement, and cosmetic results.
Results:
The transoral robotic lingual thyroidectomy was successfully performed in all patients. The mean operating time was 43 minutes (range 35–50 minutes), and an average of 11 minutes (range 10–15 minutes) was required to set up the robotic system. All patients were satisfied with their cosmetic results and the improvement of their symptoms after the operation. There were no perioperative complications or significant bleeding. The average volume of blood loss during the operation was 25 mL.
Conclusions:
The use of TORS for lingual thyroidectomy was both technically feasible and safe, suggesting that it may be considered a viable alternative to other invasive surgical approaches in patients with symptomatic lingual thyroid.
Introduction
Most patients with a lingual thyroid are asymptomatic, and detection occurs during a routine examination. When symptoms are present, however, they can include dysphagia, dysphonia, dyspnea, and hemorrhage (1,2). The treatment for symptomatic lingual thyroid is not yet standardized, which is largely due to the relative rarity of the condition. Danner et al. (3) described the efficacy and safety of radioactive iodine ablation (RIA) as a nonsurgical treatment of the lingual thyroid. This method, however, could induce acute thyroiditis and sialoadenitis.
Translingual, mandibulotomy, and transcervical approaches have been used to resect lingual thyroid tissue at the base of the tongue (4 –6). However, these procedures are invasive, have high morbidity, and leave a visible scar on the face and neck. Alternatively, a transoral approach has several advantages. Access to the lingual thyroid is gained through the oral cavity without an external incision; therefore, it is associated with decreased morbidity and does not leave a visible scar. It is difficult, however, to obtain an adequate view of the tongue base with either the naked eye or a microscope, and to efficiently resect the lesion at the base of the tongue whether using standard surgical instruments or a laser. In this study, we performed a transoral robotic lingual thyroidectomy using a da Vinci Surgical System in patients with symptomatic lingual thyroid. Our results suggest that the use of transoral robotic surgery (TORS) for the surgical treatment of lingual thyroid is both safe and feasible in the clinical setting.
Materials and Methods
Patients
Between October 2009 and October 2010, three patients were enrolled in this prospective study, which sought to validate the use of TORS for lingual thyroid resection (Table 1). We applied robotic technology for an off-label use to resect a symptomatic lingual thyroid. The Institutional Review Board of Yonsei University approved the protocol, and informed consent was obtained from each patient. One man and two women were enrolled in the study, aged 29, 41, and 35 years, respectively. Both the 29-year-old male patient and the 41-year-old female patient presented to the outpatient clinic with a chief complaint of dysphagia for several months. In both patients, a protruding mass was observed in the midline area of the tongue base on physical examination of the head and neck (patients 1 and 2). The 35-year-old female patient initially presented with a chief complaint of recurrent blood-tinged sputum. On physical examination, she too was found to have a protruding mass at the base of the tongue (Fig. 1A) (patient 3).

FOSS, functional outcome swallowing scale; TORS, transoral robotic surgery.
Preoperative procedure
All patients were treated as outpatients and underwent a complete physical examination, including a 70° rigid endoscopy. Computed tomography was performed to evaluate the extent of the lesion at the base of the tongue and to look for thyroid tissue in the pretracheal area (Fig. 2). Thyroid function tests were performed to check the levels of thyroid hormone in each patient preoperatively.
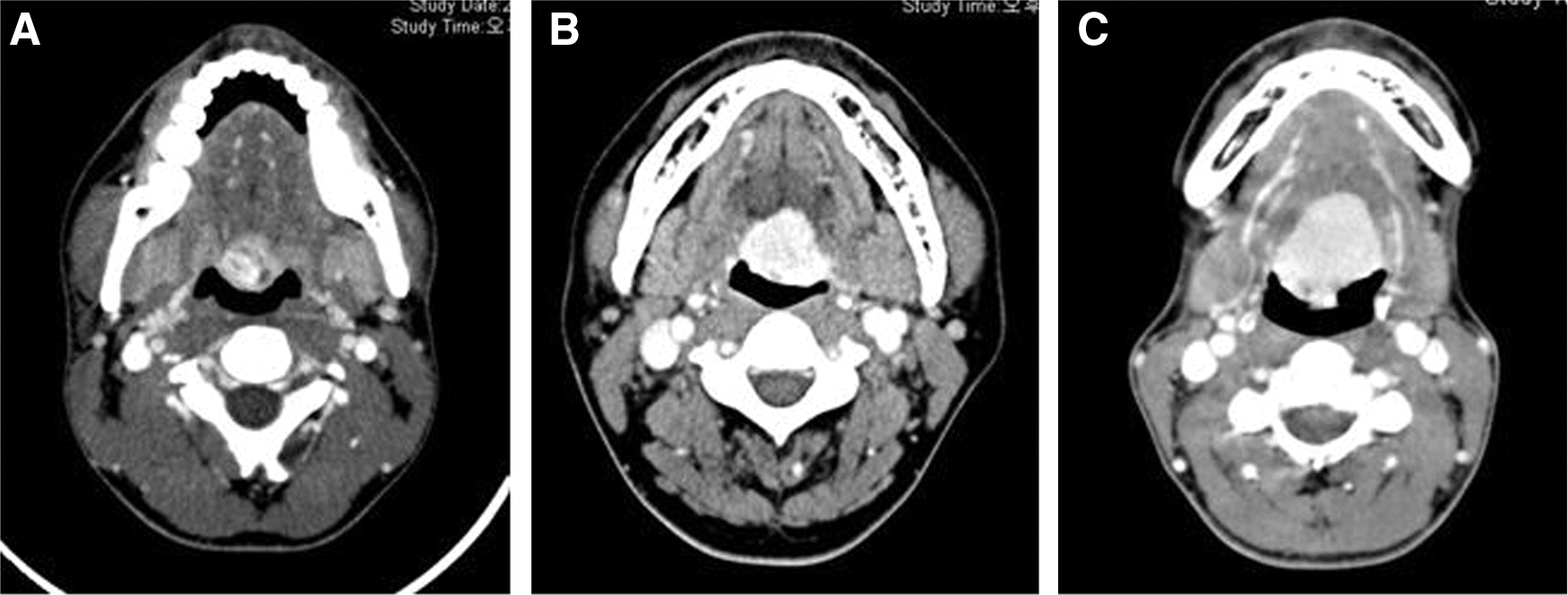
Computed tomography was performed to evaluate the extent of the lesion at the base of the tongue and to look for thyroid tissue in the pretracheal area:
da Vinci robot configuration
The da Vinci robot (Intuitive Surgical, Inc., Sunnyvale, CA) was used to perform the operation. This surgical robotic system consisted of a surgeon's console, a surgical bed, and a manipulator cart where three robotic arms were instrumented. While standing at the console, the surgeon was able to view three-dimensional magnified images generated from the endoscopic arm on the manipulator cart. The operation itself was performed using the remaining two articulated instrument arms, which were controlled from the surgeon's console.
Robotic system settings
The operating room and robotic system were set up as described in previous studies (7,8). The patient was positioned supine on the surgical bed, and general anesthesia was administered. Nasotracheal intubation was performed to maintain the airway during the operation. The surgical bed was turned around so that the foot side of the surgical cart was angled at 180° relative to the anesthesia team. The patient's head was then placed at the foot side of the surgical bed. The manipulator unit was positioned on the patient's right side so that it could form an angle of 30° with the surgical cart. When approaching the base of the tongue, an FK (Gyrus Medical, Inc., Maple Grove, MN) or Crowe–Davis retractor was used to open the oral cavity. The endoscopic arm was placed at the center of the oral cavity, and the two instrument arms were positioned to form an angle of 30° with the endoscopic arm bilaterally (Fig. 3). An adequate surgical view was obtained using a 30° face-up endoscope (Fig. 4A, D). The instrument arms were equipped with a 5-mm spatula cautery on the right side and 5-mm Maryland forceps on the left.

The FK or Crowe–Davis retractor was used to open the oral cavity. The endoscopic arm was placed at the center of the oral cavity, and the two instrument arms were positioned to form an angle of 30° with the endoscopic arm bilaterally.

Transoral robotic lingual thyroidectomy in patient 1.
Transoral robotic lingual thyroidectomy
The resection margin was marked using a 5-mm spatula cautery at the base of the tongue. Subtotal lingual thyroid resection was circumferentially performed along the marked margin, maintaining the direction of the spatula cautery tip toward the hyoid bone (Fig. 4B, E). Significant bleeding could occur from injury to the lingual artery during dissection of the tongue base, which would be difficult to control and likely impede the view of the operative field. Therefore, the surgeon was careful not to injure the lingual artery, and a laryngeal hemoclip was used to control any bleeding. Fibrin glue was applied to the surgical site for protection from saliva contamination, and the wound was allowed to heal by secondary intention (Fig. 4C, F).
Results
Adequacy of exposure
In each case, an FK retractor or Crowe–Davis was utilized to obtain an adequate view of the tongue base where the lingual thyroid was located.
Ability to perform transoral robotic lingual thyroidectomy
The surgeon successfully performed the transoral robotic lingual thyroidectomy in all cases. During the TORS surgical procedure, a 30° endoscope provided an adequate view of the tongue base and aided the surgeon in determining the extent of the lesion. The surgeon utilized a bimanual approach by controlling two instrument arms equipped with a spatula cautery and Maryland forceps. In addition, the lesion could be resected in multiple planes within the narrow oral cavity using the articulated robotic instrument arms.
Operative time
The mean overall operative time was 43 minutes (range 35–50 minutes) to perform the robotic procedure, including 11 minutes (range 10–15 minutes) for obtaining adequate exposure and robotic positioning (Table 2).
Complications
There were no significant complications related to the surgical procedure. The average blood loss during the TORS procedure was 25 mL, and no transfusions were required.
Functional outcomes
Full swallowing function returned in all patients within 3 days of surgery, and none of the patients required a feeding tube. The functional outcome swallowing scale (FOSS) was utilized to measure subjective swallowing function. Salassa devised the FOSS scoring system to evaluate swallowing function in six stages (9). Stages 0–2 indicate normal function or compensated abnormal function in swallowing, while stages 3–4 indicate decompensated abnormal function. Stage 5 requires a non-oral feeding route for nutrition. None of the patients in this study received tracheotomies, and they were extubated immediately after the operation. None of the patients required re-intubation to manage airway patency due to bleeding or tissue swelling. The average hospital stay was 4 days. At the last outpatient visit, patient satisfaction with cosmetic results was measured on a graded scale of I (extremely satisfied) to V (extremely dissatisfied) (10). All patients were extremely satisfied with the lack of a visible postoperative scar (grade I in all patients).
Follow-up
The average follow-up period was 25 months (range 24–27 months). All patients remained without recurrent symptoms or an increase in the size of the residual lingual thyroid. In addition, all three patients were satisfied with the treatment outcome and the cosmetic results at the last outpatient clinic visit.
Discussion
Microscopic amounts of thyroid tissue can be found in up to 10% of the population, and 0.01% of these patients are symptomatic (11,12). Symptoms are most often seen in female patients, and tend to manifest during times of dramatic hormonal change such as puberty and menopause. Additional functional thyroid tissue does not exist in 70%–80% of patients with lingual thyroid (12,13), and 33% of these patients are in a hypothyroid state (14). van der Gaag et al. (15) speculated that maternal anti-thyroid immunoglobulin may impede the normal descent of thyroid tissue in the fetus as well as induce the associated hypothyroidism; there is, however, no further evidence that would support this concept. Castanet and Polak (16) reported that genetic alterations of FOXE1 could lead to an abnormal thyroid development. In addition, De Felice et al. (17) reported that Foxe1/Titf2-null mutant mice exhibited a cleft palate and either a sublingual or completely absent thyroid gland. In addition, human patients with thyroid agenesis and cleft palate have been described, and the patients were homozygous for a mutation in FOXE1/TTF2 (18,19). The prevalence of lingual thyroid was higher in patients with a family history of thyroid disease. It is important to inquire about any family history of thyroid disease to evaluate the risk of thyroid carcinoma originating from the lingual gland. In addition, a more aggressive treatment was required in patients with a family history of Cowden disease (14). The frozen section of the specimen could help the surgeon in distinguishing malignant from benign lingual thyroid tissue. In cases of lingual thyroid carcinoma, a total lingual thyroidectomy is more appropriate to eradicate the disease. However, most of the lingual thyroid carcinoma is follicular carcinoma, according to previous reports. Therefore, there are limits in the role of frozen section to detect these pathologies, because follicular carcinomas can only be confirmed if capsular invasion is detected on histology.
Although various medical and surgical treatment methods have been used to manage the symptomatic lingual thyroid, a gold-standard treatment method has not yet been established. One method includes suppressing thyrotropin using medications such as levothyroxine, and subsequently treating with radioactive iodine if patients do not respond to medication alone (3). Radioactive iodine, however, could induce acute thyroiditis and sialoadenitis. Translingual, mandibulotomy, and transcervical approaches have been utilized for the surgical treatment of the lingual thyroid (4 –6). However, these invasive procedures carry high rates of morbidity and leave visible scars on the face and neck. Some studies have used a transoral approach with or without laser to resect lingual thyroid tissue (20). It remains difficult, however, to adequately visualize the tongue base and to resect the lesion with a laser and standard surgical instruments. The transoral surgery performed using a microscope and laser to remove lesions at the tongue base is typically limited by poor visualization or difficulties using standard surgical instruments. The base of the tongue is not easily viewed either by the naked eye or with a microscope, and resection is difficult due to the fulcrum effect of long surgical instruments and the straight line generated by the laser.
Compared with conventional transoral surgery, the robotic surgical system is able to generate a three-dimensional magnified view of the oral cavity, and the endoscopic arm allows for an adequate view of the tongue base. This system enables the surgeon to employ a bimanual technique by controlling two instrument arms. Multiplanar resection can be performed within a limited working space due to the flexibility of the tip of the instrument arm. Using these technological advantages, the operations performed in this study were both efficient and safe, as evidenced by the short operation times and minimal blood loss. In addition, all patients enrolled in the study recovered rapidly and were very satisfied with their treatment outcomes and cosmetic results.
The use of TORS for a lingual thyroidectomy was both technically feasible and safe, suggesting that it may be a viable alternative to other invasive surgical approaches in patients with symptomatic lingual thyroid.
Footnotes
Disclosure Statement
No competing financial interests exist.