
Abstract
Background:
Monitoring changes in the thyroid bed (TB) is one of the clinical mainstays for surveillance of recurrent thyroid carcinoma. Fine-needle aspiration (FNA) is a diagnostic tool that is commonly used to aid in the identification of residual or recurrent disease. The aim of our study was to evaluate the efficacy of ultrasound-guided FNA of the TB in detecting recurrent thyroid cancer and to correlate the findings with clinicopathologic parameters to identify predictors of TB recurrence.
Methods:
We retrieved cases of soft tissue masses within the TB that were evaluated for recurrence between January 1, 2006, and February 1, 2011. All ultrasound-guided FNA biopsies clinically suspected to indicate a lymph node metastasis and specimens with lymphocytes were excluded from the data.
Results:
Of the 291 patients identified for evaluation of recurrence, 250 had papillary thyroid carcinoma (PTC), 10 had follicular carcinoma, 22 had medullary carcinoma, 7 had Hürthle cell carcinoma, and 2 had a previous thyroidectomy for an unknown type of thyroid carcinoma. For all FNAs that were clinically suspicious or intermediate for recurrence, the rate of positivity was 71.8% (209 patients). All cases diagnosed as “positive for PTC” or “suspicious for PTC” on TB FNA were found to have soft tissue metastasis on follow-up surgical resection. This resulted in a negative predictive value of 88.4% and a positive predictive value of 100%. The average time between thyroidectomy and TB FNA was 73.5 months. Of the patients with a previous diagnosis of PTC, those with suspicious/positive cytology were more likely to be women, to be older at thyroidectomy, to have documented metastasis to other sites as well as extrathyroidal extension and multifocal primary disease as compared with nondiagnostic/negative cytology cases. Patient age ≥45 years, primary tumor size at thyroidectomy, and surgical resection margin status had no statistical significance for predicting risk of TB recurrence.
Conclusion:
TB recurrence of PTC is most likely to occur in patients who have the following clinicopathologic parameters: documented metastasis to any site, extrathyroidal extension, and increased number of primary cancer foci.
Introduction
Methods
Patient population
Specimens were retrieved from the Anatomic Pathology database of Mayo Clinic in Rochester using the SNOMED CT® (College of American Pathologists, Northfield, IL) as either “Thyroid bed, FNA” or “Soft tissue, FNA” between January 1, 2006, and February 1, 2011. The patient inclusion criteria included age of 18 years or older at the time of FNA, primary neoplasm having been located in the thyroid and resected prior to the FNA, and the FNA biopsy location having been within the anterior neck (region VI). Any specimen that had clinical (including US evaluation) or pathologic evidence that the FNA was of lymph node origin was excluded from the study. Of the total 300 initial patients identified, one pediatric patient and eight adult patients that did not consent to participate in research were excluded, leaving 291 patients in the study. The study was approved by the Mayo Clinic Institutional Review Board.
Only one FNA per patient was included in the study. If a patient had multiple FNAs from the same lesion during the time of the study, only the most conclusive or positive sample was included. If a nondiagnostic sample was followed by a sample with a definitive diagnosis in any other category, the subsequent FNA was included and the nondiagnostic sample was excluded from the study. If multiple FNAs from a single patient had the same diagnosis, the first FNA was preferentially selected. In addition, if the nodule proved to be benign residual thyroid tissue, the specimens were included in the “negative” category.
Clinicopathologic parameters were documented by reviewing electronic medical charts. The following were recorded: age, sex, date of thyroidectomy, tumor size of the largest primary tumor, extrathyroidal extension, surgical margin status of thyroidectomy specimen, metastasis at time of thyroidectomy, interval time between thyroidectomy and TB FNA, serum Tg and calcitonin levels at FNA, Tg levels on the washout specimen, and follow-up therapy after FNA diagnosis. If any data for a particular patient were not documented within the electronic medical record, that data for that particular category were not included in the analysis. For example, if the size of the FNA-targeted nodule was not documented, that patient was not included in the analysis for the size of the FNA target.
Slide review
We utilized the Bethesda system for reporting thyroid cytopathology (8). The category of atypia of undetermined significance (AUS) is used sparingly in our institution, and almost all of our thyroid FNA cases are classified as negative, nondiagnostic, suspicious, or positive for papillary thyroid cancer (PTC). The rate of AUS within our institution is less than 1% (9,10). Only three cases of PTC were labeled as AUS. The slides from those three cases were then re-reviewed to further subclassify them into the current diagnostic categories. Two of the cases were reclassified as nondiagnostic and one case was reclassified as suspicious for PTC.
Statistical methods
All analyses were conducted using SAS version 9 (SAS Institute Inc., Cary, NC). Categorical data were summarized with frequencies and percentages, and continuous data were summarized with means and standard deviations. Clinical-pathologic characteristics at the time of FNA (age, sex, tumor size, etc.) were compared between those with nondiagnostic/negative versus suspicious/positive FNA TB result, with chi-square (χ2) tests for categorical data and Kruskal–Wallis tests for continuous data. The risk of a suspicious or positive FNA result was compared with respect to characteristics of the primary tumor at time of prior thyroidectomy using Cox proportional hazards regression. Hazard ratios, along with 95% confidence intervals, were reported, and p values less than 0.05 were considered statistically significant. Even though all differentiated thyroid cancer subtypes were evaluated, only the data for PTC were included in this article.
Results
A total of 291 patients with FNA of the TB were identified. Based on the original diagnosis at thyroidectomy, there were 250 patients with PTC, 22 with medullary carcinoma, 10 with follicular carcinoma, 7 with Hürthle cell carcinoma (HCC), and 2 with an unknown thyroid tumor type (Table 1). In all subtypes except for HCC, there was a female predominance. The mean age for the entire cohort was 50 years, but the HCC patients were distinctly older (all ≥45, mean age, 75 years). The mean size of the FNA target for all categories was 1.3 cm (range, 0.3–8.3 cm). The FNA reading was metastatic/recurrent thyroid pathology in 209 cases (71.8%); benign, noncancerous thyroid tissue in 66 cases (22.7%), and FNA was nondiagnostic in 16 cases (5.5%). All patients were consistently diagnosed with the same neoplasm from beginning to end of care, starting at thyroidectomy to TB FNA, and on selected patients that had follow-up surgical resection after FNA.
FNA, fine-needle aspiration.
Features at FNA
Given the very high prevalence of PTC in this cohort, consistent with the clinical distribution of the thyroid malignancy subtype, we focused our analysis on this subgroup. Most (70.0%) of the patients were women, with a mean age of 49 years (Table 2). The distribution of age was similar between the nondiagnostic/negative and the suspicious/positive groups, while the sex distribution differed significantly (p=0.0174). Serum Tg levels at the time of TB FNA were significantly higher (p<0.0001) in the suspicious/positive group with a mean level of 133.0 ng/mL (SD, 860.2 ng/mL) versus a mean level of 5.7 ng/mL (SD, 33.6 ng/mL) in the non-diagnostic/negative group. Three patients in the nondiagnostic/negative group and 12 patients in the suspicious/positive group had Tg washout levels, with higher levels occurring in the suspicious/positive group. The mean size of the TB FNA target was 1.3 cm for the suspicious/positive group and 1.1 cm for the nondiagnostic/negative group (Fig. 1) (p=0.04).
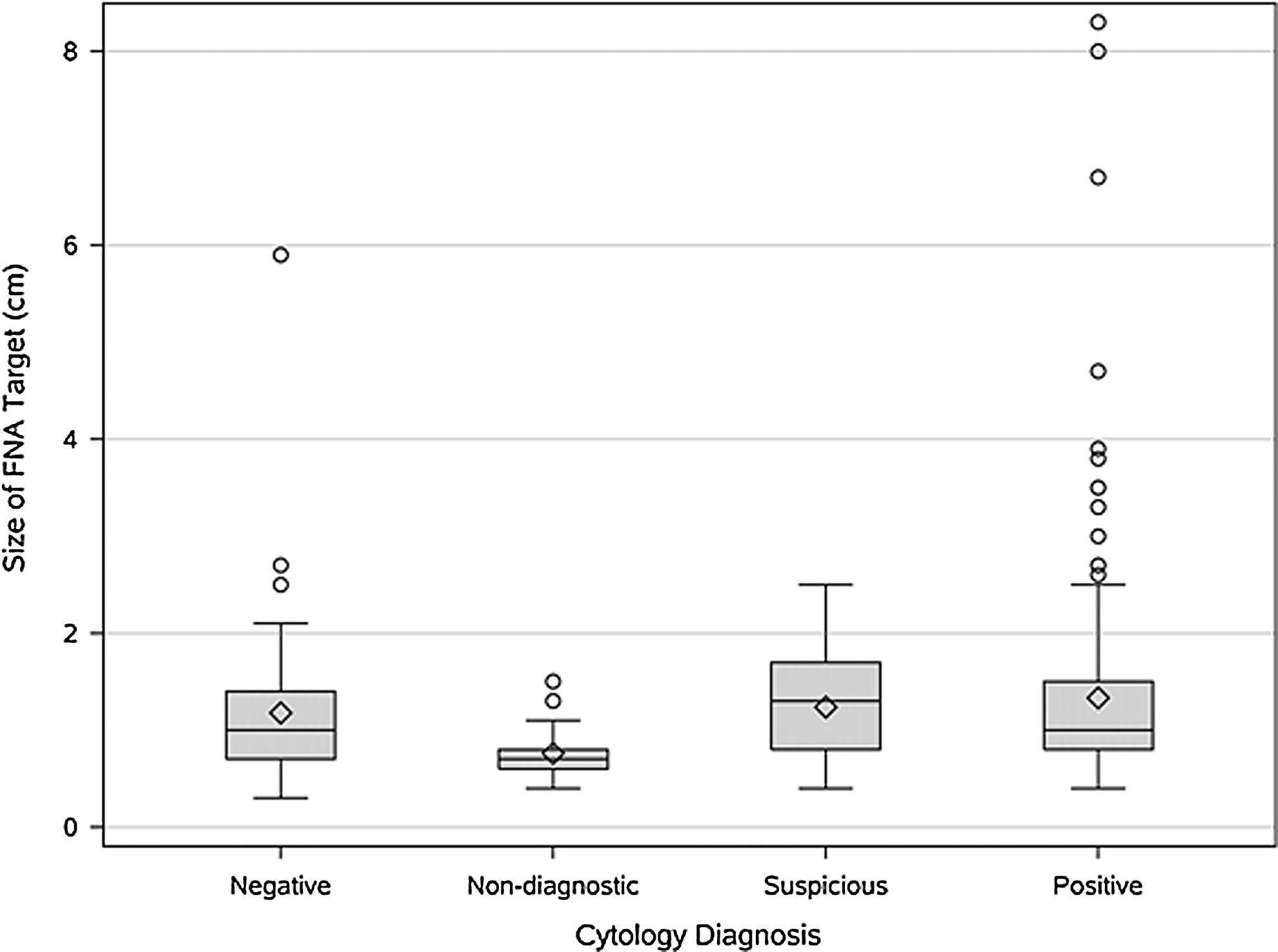
Size of FNA target for papillary thyroid carcinoma (PTC) classified by FNA result.
χ2 test.
Kruskal–Wallis test.
Primary malignancy features
At thyroidectomy, most (50%) neoplasms were larger than 2 cm, 39.3% were 1 to 2 cm, and 10.7% were smaller than 1 cm. Tumor size was not found to be significantly associated with the likelihood of a suspicious/positive FNA. The average age at thyroidectomy was 43.2 years, and increasing age was associated with higher risk of recurrence (HR for 1 year increase=1.02, p=0.004). Patients with multiple foci (HR=1.48, p=0.01), regional metastases (HR=1.77, p=0.04), or extrathyroidal extension (HR=1.57, p=0.003) were more likely to have recurrence. A higher number of positive lymph nodes at initial pathology was also significantly associated with increased risk of recurrence (p=0.03). Neither T-stage nor clinical stage was found to be associated with recurrence risk (Table 3).
Hazard ratio given for one unit per level increase for continuous/ordinal variables; p value from model including predictor continuously.
CI, confidence interval.
Treatment decisions
Thirteen patients (18.8%; total, 69 patients) with either a nondiagnostic or negative FNA proceeded to treatment. Nine patients were treated because of a positive lymph node FNA that was done concurrently at the time of TB FNA, and four patients proceeded onto surgery for multiple suspicious nodules on US (Fig. 2). Of these 13 patients, nine had surgery, two received radioactive iodine, and two underwent percutaneous ethanol ablation (PEI). Of the nine patients that had surgery, eight showed recurrent TB disease.
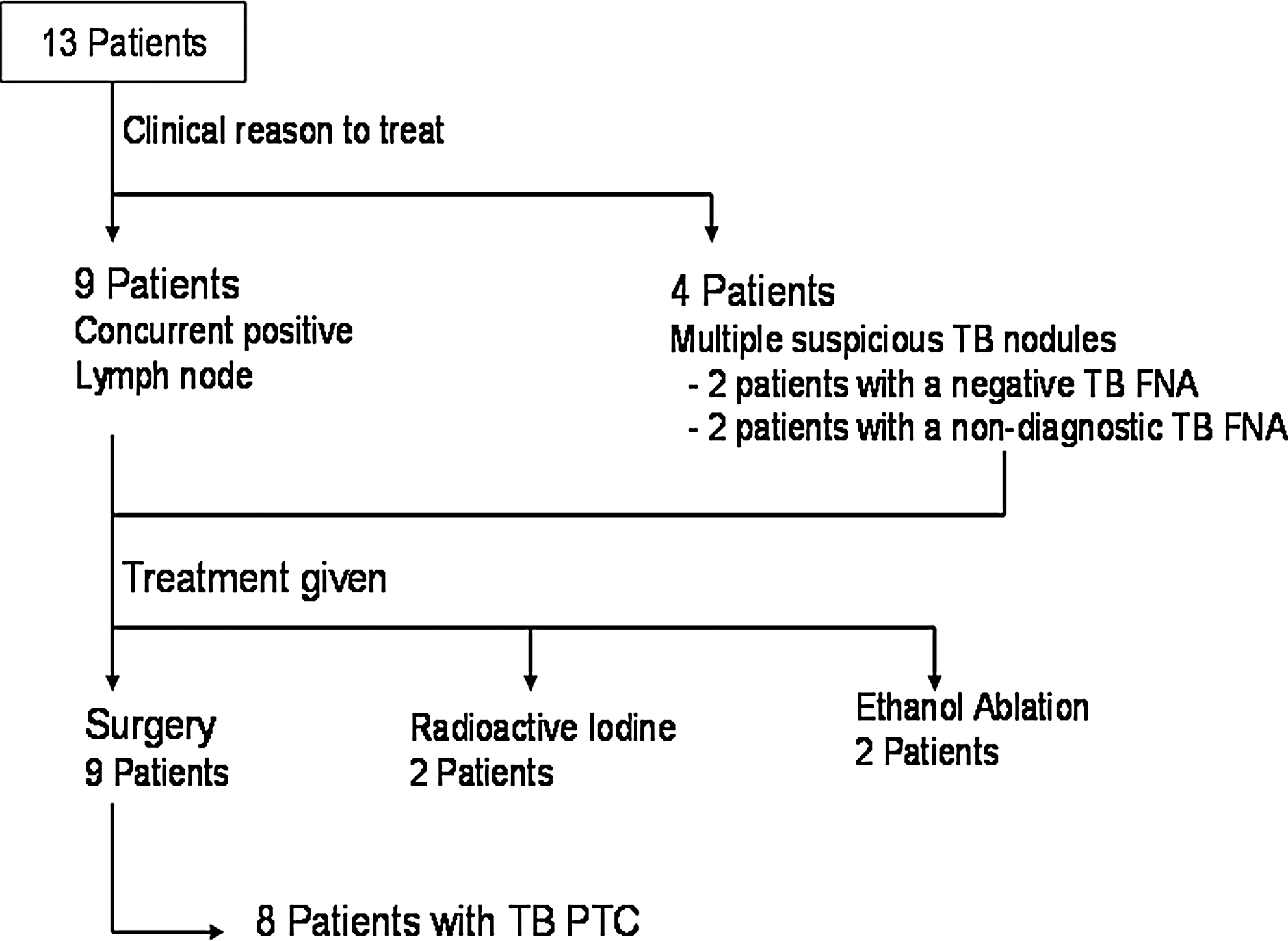
Diagram showing the diagnostic reasons to proceed with treatment in 13 patients who had negative or nondiagnostic FNA and their histologic surgical outcomes.
Of the patients that had a nondiagnostic/negative TB FNA (69 total patients), 81.2% received no treatment and continued with observation (Table 4). Of the patients with a suspicious/positive TB FNA, 16 (9%) were clinically observed due to various reasons such as patient age, comorbidities that limited life expectancy, and patient preference. Forty-four patients (24.7%) underwent PEI and 106 (59.6%) were treated surgically. The remaining patients underwent external beam radiation, chemotherapy, or radioactive iodine based on their clinical picture.
χ2 test.
Survival analysis
Kaplan–Meier curves (Fig. 3), comparing the time it took from the date of thyroidectomy to a suspicious/positive TB FNA, showed a plateau after 20 years overall. Patients with regional or distant metastasis or any number of lymph node metastases, and extrathyroidal extension had a suspicious/positive FNA earlier than the comparative patients without metastasis and/or with lesions confined to the thyroid gland.
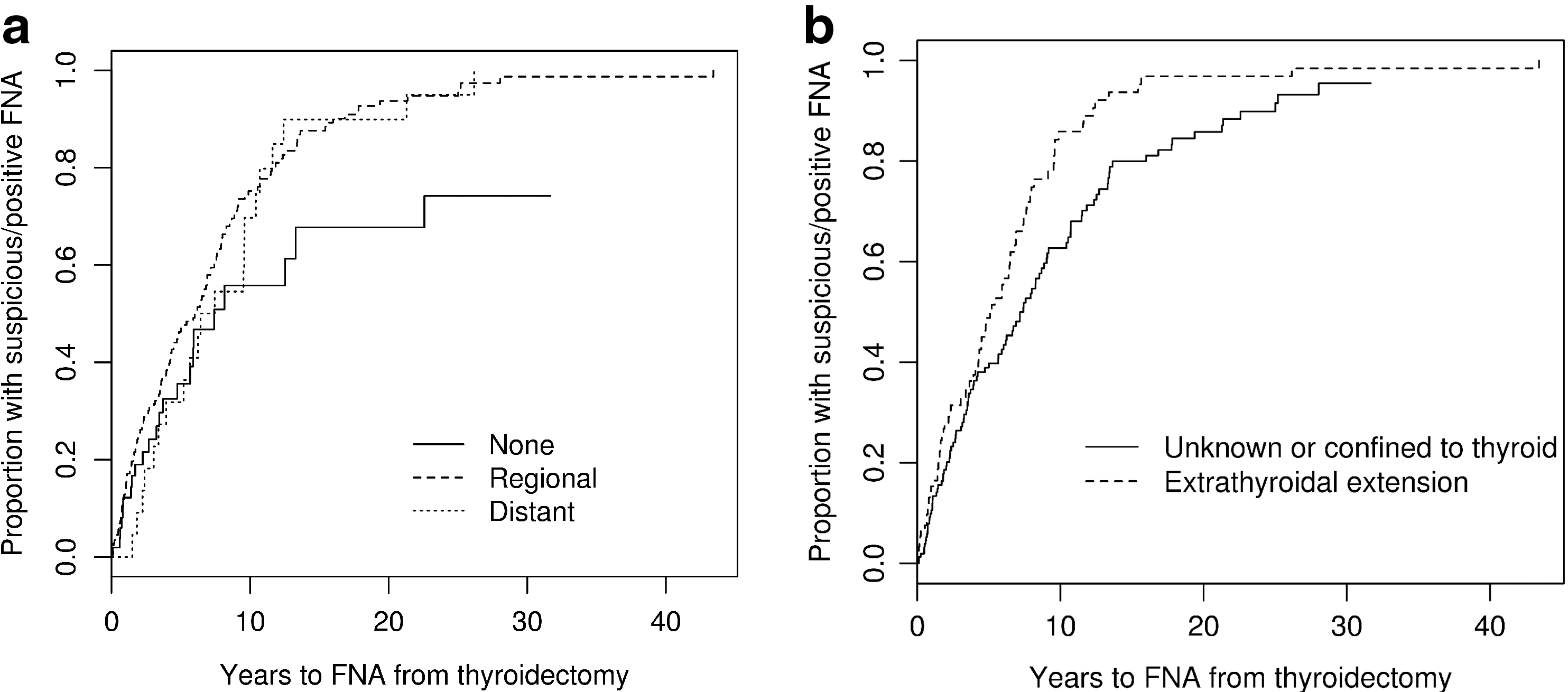
Kaplan–Meier curves comparing years from date of thyroidectomy to proportion of the suspicious/positive FNA result broken down by site of metastasis
Discussion
The purpose of this study was to identify risk factors or predictors that lead to the presence of TB recurrence and document the treatment rendered based on FNA diagnosis. An extensive analysis was performed for all differentiated thyroid cancer subtypes. However, due to the small population size of patients with medullary thyroid carcinoma, follicular carcinoma, and HCC, we felt that the reproducibility of the data might be in question and therefore elected to only publish the most basic information regarding age, sex, margin status, and size of the FNA target. For PTC, our results show that most patients in this cohort were women and the likelihood of a positive FNA from TB was directly correlated with serum Tg, multifocal disease, extrathyroidal extension, and number of positive lymph nodes or metastasis to any site. Patient age ≥45 years, sex, and margin status at the time of initial thyroidectomy had no impact on that tumor recurrence.
The rather low number of patients with Tg measurements from the FNA washout reflects the difficulty in interpreting such values given the inability, in this particular location, to distinguish between residual thyroid tissue and thyroid carcinoma. Therefore, this was a case-by-case decision; however, it could be used in future studies. In contrast, given its higher clinical use, we had a standardized approach to Tg washout measurement from lymph node FNA and are currently pursuing reflex testing based on cytology results.
In 14 patients, despite repeating FNA, the results remained nondiagnostic, most likely representing previous surgical scarring or granulation tissue (11,12). Two of these patients continued to receive treatment. The average size of these lesions was 0.8 cm (range, 0.4–1.5 cm, Fig. 1), emphasizing that the risk of a nondiagnostic FNA increases inversely proportionally with the size of the nodule.
Thirteen patients that had a negative or nondiagnostic TB FNA diagnosis continued on to receive treatment regardless of a negative or inconclusive result (Fig. 2). The eight patients that had positive TB metastasis at surgery were used to calculate the false-negative rate and a negative predictive value of 88.4%. It is important to note that two patients also received localized PEI in the TB and therefore could also be included as false-negative TB FNAs. However, it is uncertain as to whether there were true soft tissue metastases since no tissue was available for verification. Therefore, at best, the negative predictive value is 88.4% and in actuality it might be much lower. This is a reality that most physicians face with cytology specimens because most patients do not have tissue follow-up following a negative FNA diagnosis.
Treatment of patients with recurrent thyroid carcinoma continues to be diverse, with some institutions recommending neck dissection as a possible treatment option (5), whereas others recommend close clinical observation based on the clinical picture of tumor size and burden (4). At our institution, the average time between thyroidectomy and TB FNA of 73.5 months reiterates the indolent course of these neoplasms overall and perhaps reinforces the need for an individualized treatment, in which the risks and benefits of various options are considered and potential treatment-related comorbidities are minimized. We would advocate that in a neoplasm with such a good long-term clinical prognosis, the treatment modalities used should have minimal comorbidity and less invasive procedures should be investigated. In our series, less than half of the cohort with diagnosed PTC by FNA in the TB proceeded to neck dissection (46.6%), while a much newer procedure, PEI, is gaining attraction, with 18.6% patients treated this way, owing to its favorable risk–benefit ratio.
The limitations of our study include the fact that this was a retrospective study, which therefore makes it difficult to quantify the decision that led to FNA and impossible to provide a denominator for the cohort with PTC followed over that period. In addition, 148 patients had their thyroidectomy with follow-up care at our institution, which leaves a large minority of patients with thyroidectomy performed elsewhere in which the outside pathology report was directly incorporated into our data set. However, all of the patients had histologic correlation with disease type upon recurrence seen on FNA.
The strengths of our study include the presence of strong multidisciplinary expertise in pathology, endocrinology, and radiology, with a relatively uniform clinical approach to PTC therapy and, to our knowledge, the largest study analyzing the approach to TB FNAs from a pathologic specimen standpoint.
The results of our study confirm that US FNA is an excellent diagnostic tool in assessing TB recurrences in PTC, with only 5.6% of patients (14/250) experiencing nondiagnostic results. This rate is similar to the nondiagnostic rate reported with FNAs from native thyroid nodules (13). The diagnostic reach of the procedure in experienced hands is impressive, with lesions as small as 0.3 cm being successfully aspirated, and 50% of the evaluated lesions being 1 cm or smaller.
Conclusion
When the need for further evaluation arises in PTC patients with TB lesions, FNA is a reliable tool with only a few (5.6%) patients having nondiagnostic results. Furthermore, the pretest probability of disease can be better quantified by using our data, knowing that the TB lesion is likely to be positive if there is documented metastasis to any site, extrathyroidal extension, and multifocal primary thyroidal disease at thyroidectomy.
Footnotes
Disclosure Statement
All authors have no conflict of interest to disclose.