
Abstract
Background:
Some studies have demonstrated a correlation between the presence of a BRAF mutation and aggressive characteristics, including lymph node metastasis in papillary thyroid carcinoma (PTC). Prophylactic central neck dissection (CND) has been proposed for treatment of PTC. Given the potential complications of CND, we undertook a prospective study to determine the correlation between the BRAF mutation and lymph node metastasis.
Methods:
A total of 51 patients with PTC underwent total thyroidectomy and routine prophylactic CND. All patients were tested for the BRAF mutation.
Results:
Positive lymph nodes were found in 54.9% of patients. The BRAF mutation was found in 15 patients (29%). BRAF was not correlated with lymph node metastases. Lymph node metastases were correlated with multifocality (p=0.005) and angiolymphatic invasion (p=0.003) in univariate analysis. Age was also significant in multivariate analysis.
Conclusions:
Testing for the BRAF mutation does not help in deciding whether or not to perform CND.
Introduction
P
To establish standardized procedures, guidelines have been published for the management of thyroid cancer. This initiative was spearheaded by the most important associations worldwide: the American Thyroid Association (ATA) (7), the European Thyroid Association (ETA) (8), and the Latin American Thyroid Society (LATS) (9). The guidelines are designed to stratify the risk of recurrence and mortality of the neoplasias, while standardizing surgical and radioactive iodine therapy. The treatment of central compartment lymph nodes was included as a specific theme in the guidelines published by the ATA in 2009 (7).
Residual metastatic lymph nodes represent the most common site of disease persistence and recurrence, and can be associated with poor outcome, especially in older patients (>45 years) and T3 tumors. The incidence of lymph node metastasis in PTC in the central compartment and in the lateral compartment has been studied in some populations (10). In the Japanese population, the incidence of clinically undetected lymph node metastasis detected after surgical removal and histopathological analysis was as high as 80% (11,12).
Since there are no reliable preoperative methods for detecting these metastases (13,14), and because the morbidity of central compartment dissection is significantly higher than thyroidectomy alone, recommending elective dissection remains controversial. In the last edition of the ATA guidelines (7) it was suggested that patients with neoplasias classified as T3 or T4 by the Union for International Cancer Control (UICC) could be submitted to elective dissection of the central compartment.
In an effort to stratify the risk of thyroid neoplasias, various classification systems and clinical, histopathological, and, more recently, molecular factors have been correlated with a poorer prognosis. Recently, the 17799T>A (p.V600E) mutation of the BRAF gene was correlated with various factors of poor prognosis, including a greater incidence of lymph node metastasis (15 –25). All of the studies presented in the literature are retrospective studies.
The knowledge that we have acquired with regard to the 17799T>A (p.V600E) mutation is still very recent and, while its application in the diagnosis of PTC is very clear, the question of whether it can be useful in predicting the prognosis of the patients remains obscure. With regard to the Brazilian population, we still have little information and no prospective studies involving research on the 17799T>A (p.V600E) mutation and elective dissection.
The objective of the present study was to evaluate if presence of the BRAF 17799T>A (p.V600E) mutation could be used as a criterion to perform selective neck dissection of the central compartment, focusing on the association between the mutation and the presence of lymph node metastasis.
Patients and Methods
This study was approved by the hospital's ethics committee. All patients gave their informed written consent to participate.
We prospectively selected patients with thyroid nodules detected using ultrasound-guided fine needle aspiration biopsy (US-FNAB) that had cytological diagnoses of suspicious for PTC or PTC, corresponding to the Bethesda V and VI nomenclature (26). No patients previously underwent any cervical surgery, external radiotherapy, or radioactive iodine treatment. Lymph node metastases were diagnosed before surgery by US-FNAB with cytological diagnosis and positive thyroglobulin washout.
Patients with clinical conditions that made postoperative hypoparathyroidism more likely or who had associated disorders in whom hypoparathyroidism would have been particularly aggravating were excluded. Three patients were excluded due to associated clinical problems that could cause severe postoperative complications: one patient diagnosed with schizophrenia and two patients with previous gastric bypass surgery.
From April 2009 to December 2010, a total of 370 thyroidectomies were performed. All patients were treated at the Head and Neck Surgical Service of the Institute of Cancer of the State of Sao Paulo (ICESP) and were operated on by the same team. Fifty-two consecutive patients with cytological diagnosis suspicious for PTC or PTC (Bethesda V and VI) were selected and evaluated. All patients were submitted to a total thyroidectomy and PTC was confirmed by frozen section. After confirmation of the diagnosis, all patients with no lymph node metastasis detected previously or even during intraoperative procedure were submitted to elective dissection of the bilateral central compartment. Patients with previously detected lymph node metastasis confirmed by FNAB or during surgery by frozen section were submitted to therapeutic dissection of the affected compartment and the central compartment. Dissections were carried out in accordance to anatomical parameters established by the ATA and the American Academy of Otolaryngology–Head and Neck Surgery without monitoring of the laryngeal nerves (27,28).
All specimens were evaluated by the ICESP Pathology Service, following the standardized protocol of the Pathology Department of the University of Sao Paulo Medical School. Thyroidectomy specimens were fixed and submitted to serial cross-sectional cuts with a spacing of 3–5 mm. The cuts were carried out in the craniocaudal direction. In this way, the entire thyroid is included in the paraffin study, enabling the detection of multiple foci of neoplasia, even if they are microscopic. The products of these cervical dissections were sent separately from those of the thyroid, since the thyroid was submitted to frozen section analysis before dissection (only one patient had a benign result after the frozen section and was excluded from the study). The cervical dissection products were manually dissected by the pathologist. Fifty-one patients were tested for the BRAF mutation. In the cases that presented multifocality, mutational analysis of 17799T>A (p.V600E) mutation was carried out for all foci.
All of the following parameters were analyzed: sex, age, tumor size, histological subtype, angiolymphatic and extrathyroidal invasion, multifocality, and presence of lymph node metastases and stage of disease. The seventh edition of the AJCC Cancer Staging Manual was used for the TNM classification (29).
p.V600E mutation analysis
Extraction of DNA from material conserved in paraffin
For each microtube of 1.5 mL, three sections equivalent to 10 μm were obtained. To these tubes, 1 mL of xylene preheated in an incubator at 95°C was added. Microtubes were agitated and placed in an incubator at 37°C for 30 minutes, and then centrifuged for 5 minutes at 15,000 g, after which the supernatant was discarded. For effective elimination of the paraffin, this step was repeated another two times. The samples were then submitted to two washings with 500 μL absolute ethanol to remove the organic solvent. After each addition of absolute ethanol, the microtubes were centrifuged at 13,000 g for 5 minutes at 4°C and the supernatant discarded. The samples were dried by inverting the microtubes on absorbent paper.
For DNA extraction, 20 μL of proteinase K (10 mg/mL) and 480 μL of a solution of 2.5 mL of Tris HCl 1 M (pH 8.0); 500 μL EDTA 0.5M (pH 8.0); 250 μL of Tween 20; and 46.75 mL of deionized water was added to each microtube. The samples were incubated for 18 hours at 37°C. Two extractions were carried out with 500 μL of phenol–chloroform. The tubes were carefully inverted and centrifuged at 13,000 g for 2 minutes at 4°C. The supernatants were transferred to new microtubes and a new extraction was carried out with phenol–chloroform. DNA extracted from NPA cells (a melanoma cell line containing a biallelic BRAF p.V600E mutation) was used as positive control (kindly provided by E.T. Kimura). As negative control, we used DNA extracted from normal thyroid tissue that showed the wild type sequence of exon 15 of the BRAF gene.
After extraction, all of the DNA samples were quantified in a Nano Drop 1000 Overview spectrophotometer (Thermo Fisher Scientific) at a wavelength of 260 nm (1.0 unit OD 260=50 μg/mL). The ideal established DNA quality was 1.75 for readings at 260 and 280 nm.
For confirmation of the presence or absence of the p.V600E mutation, sequencing of the products generated by polymerase chain reaction (PCR) was carried out (30).
The equipment used for the sequencing was an ABI Prism 3130xl (Applied Biosystems), employing the commercially prepared Big Dye Terminator v3.1 Cycle Sequencing Kit, and the same primers employed in the PCR amplification.
The sequences obtained were compared with the sequence of exon 15 of the BRAF gene; the Ensembl Genome Browser sequence was used as reference.
For sequence analysis, the program Sequence Scanner v1.0 (Applied Biosystems) was used.
Statistical analysis
Data were processed using SPSS 13.0 software. The continuous variables are presented as mean±standard deviation (SD), while categorical variables are presented as absolute and relative (percentages) frequencies. Univariate analyses were carried out using the Fisher's exact, Pearson chi-squared, Student's t, and Mann–Whitney tests when appropriate and p-values <0.05 were considered statistically significant. Multivariate analysis was carried out using logistic regression to determine the influence of histological characteristics and the p.V600E mutation in the lymph node metastases.
Results
Of the 52 patients, 51 patients were completely evaluated, consisting of 41 female patients (80%) with a mean age of 43.6±15.8 years, ranging from 13 to 75 years.
Six patients were diagnosed with lymph node metastases in the lateral compartment before surgery and therefore were submitted to dissection of the central compartment and dissection of the affected lateral compartment, in addition to the total thyroidectomy. The remaining 45 patients presented no evidence of preoperative metastasis and were submitted to total thyroidectomy and elective dissection of the central compartment. The number of lymph nodes dissected ranged from 5 to 74. The extension of dissection of the central compartment was the same for all patients, and all surgeries were performed by the same surgeon.
Macroscopic neoplastic invasion of a portion of the recurrent laryngeal nerve was detected in one patient. During follow-up, transient and permanent dysphonia were diagnosed in 3.9% and 1.9%, respectively. Transient hypoparathyroidism was found in 31%, and despite parathyroid reimplantation, 12% progressed to definitive hypoparathyroidism. We defined postoperative hypoparathyroidism as a requirement for vitamin D or calcium supplementation (or both) to maintain normal calcium concentrations after thyroidectomy. Postoperative vocal cord mobility was assessed by laryngoscopy. Exclusion criteria for recurrent laryngeal nerve palsy analysis included pre-existing nerve palsy before the intervention. Findings of recurrent palsy or a persistent requirement of vitamin D or calcium supplementation 6 months after surgery were used as definition for definitive dysphonia or definitive hypoparathyroidism in this study.
Tumor size ranged from 5 to 90 mm, with a mean of 18.4±16.4 mm. Classic PTC was seen in 31 cases (60%), follicular variant of PTC was found in 10 (20%), and Hürthle cell variant in 4 cases (8%). Six cases were classified as microcarcinomas. There were no tall cell variants in our specimens.
Multifocality was observed in 27 cases (53%). Extrathyroidal extension was noted in 14 cases (27.5%), and angiolymphatic invasion in 9 cases (17%). Lymph node metastases were detected in 28 patients (54.9%).
When we analyzed all 51 patients, only the p.V600E mutation was found in exon 15. Fifteen cases of 51 (29.4%) were positive for the mutation. Thirteen cases were female. Nevertheless, the female sex was not related to the p.V600E mutation (p=0.703).
Twelve cases with the p.V600E mutation had a classical variant. Of the four cases of the Hürthle cell variant, only one was positive for the p.V600E mutation.
Among the 15 BRAF-positive cases, only 8 cases had a central lymph node metastasis. Among 36 BRAF-negative cases, 20 cases had central node metastasis (p=1). In addition, no difference in the p.V600E mutation presence was found according to age, tumor size, extrathyroidal extension, multifocality, and angiolymphatic invasion (Table 1).
SD, standard deviation.
Among 22 cases with central node metastasis and absent peroperative clinical or ultrasound findings, only 6 cases (27%) had the p.V600E mutation. One year after treatment, all six of these cases had an undetectable thyroglobulin.
The presence of lymph node metastases had a weak correlation with younger age (p=0.070). Poorer prognostic histological factors like multifocality (p=0.005) and angiolymphatic invasion (p=0.003), were significantly associated with lymph node metastases.
Multivariate regression analysis showed that younger age (p=0.070; odds ratio [OR] 0.94) and multifocality (p=0.005; OR 10.97) are independent variables associated with the presence of lymph node metastases (Fig. 1).
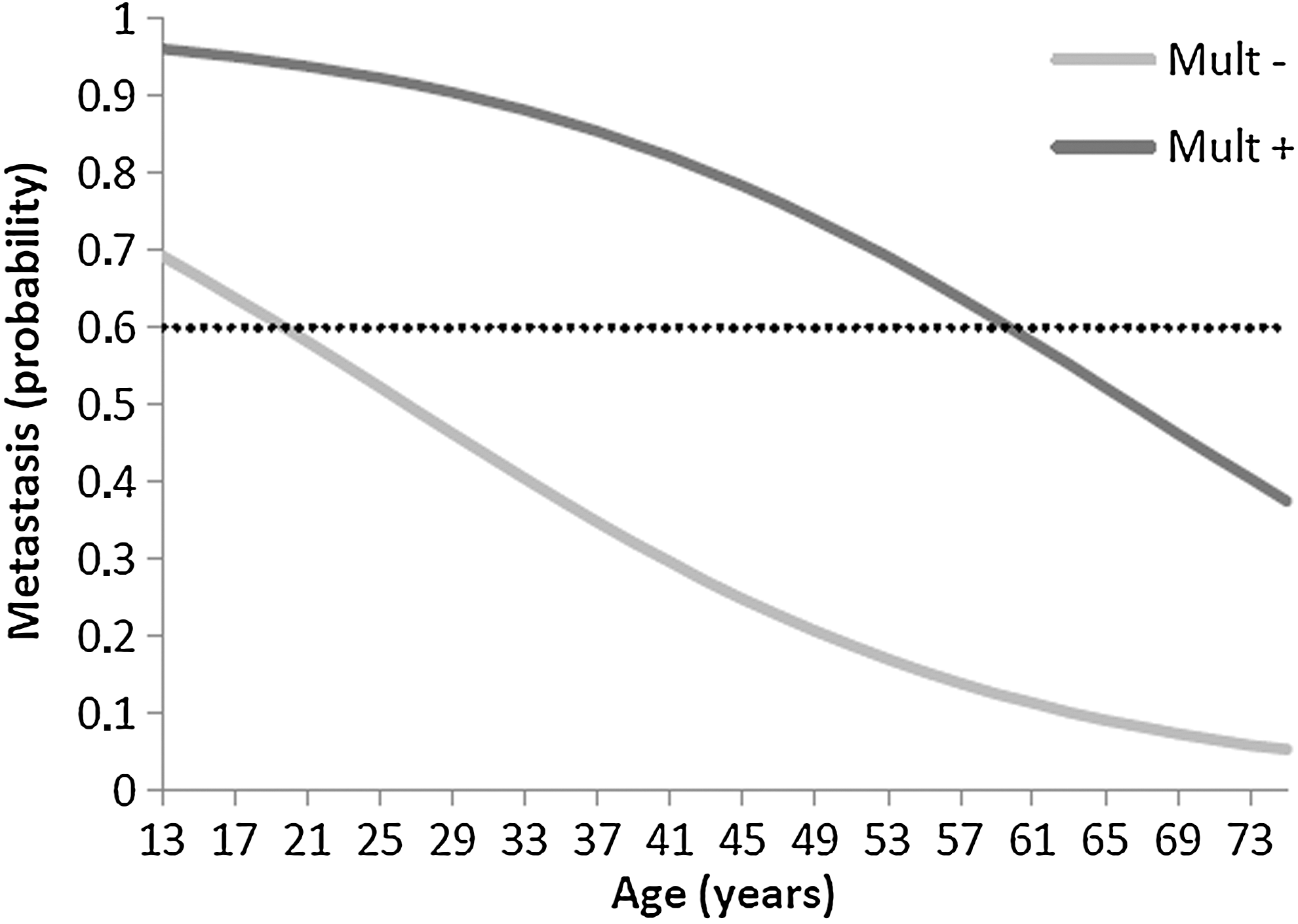
Logistic regression demonstrating the probability of having lymph node metastases according to age and multifocality.
In Figure 1, the dotted line indicates the point of greatest sensitivity and specificity of our model. This occurs at ∼60% chance of having lymph node metastasis. Therefore, we could infer that patients without multifocality achieve this incidence at ∼20 years of age, while patients with multifocality achieve this incidence at ∼60 years of age.
After one year of follow-up, we found that six patients had elevated thyroglobulin levels. Three patients with lung metastases, one patient with pulmonary and bone metastases, one patient with lymph node metastases in the lateral compartment, and one patient with an unlocalized residual or recurrent tumor. Of these patients, only one was positive for the p.V600E mutation.
Discussion
Prophylactic neck dissection is not routinely performed in our department. It is well-accepted that the presence of metastasis is correlated with persistence and recurrence in PTC (31). Despite a higher risk of local recurrence, the presence of lymph node metastases usually does not alter the mortality of patients <45 years of age.
The study published by Lundgren (32) in 2006 with a sample of 5554 patients challenged this notion. A study based on the Surveillance, Epidemiology, and End Results (SEER) data collected from 9904 patients concluded that lymph node metastasis is an independent risk factor for mortality in patients over the age of 45. There are no prospective studies that evaluate the impact of dissection of the central compartment with regard to recurrence and death related to the disease (33,34).
The central compartment can be dissected safely when the procedure is performed by experienced surgeons. Henry et al. (35) reported 50 patients submitted to elective central neck dissection, with only 6% transient recurrent laryngeal nerve paralysis and 8% transient hypoparathyroidism, similar to our findings. They report no cases of definitive recurrent laryngeal nerve paralysis or hypoparathyroidism. We diagnosed a higher frequency of transient hypoparathyroidism (31%) because we routinely measured serum ionic calcium at first 48 hours postsurgery, and 11% had signs of hypoparathyroidism during the follow-up.
There is further evidence that dissection of the central compartment may improve staging in around 30% of the patients with tumors of <2 cm and who initially do not present lymph node metastasis, and which for other reasons were not recommended for RAI treatment, and who were later recommended to receive RAI due to identification of metastasis after lymph node dissection (36). We detected 28 patients with lymph node metastases, with 43% only after central neck dissection, thereby modifying their tumoral stage.
The presence of the BRAF p.V600E mutation emerged as a promising marker of aggressiveness of PTC and may be associated with poorer prognosis. Most reported studies found an association between the p.V600E mutation and the presence of lymph node metastasis (15 –25). Therefore, we hypothesized that the presence of a BRAF mutation could be useful to decide whether or not to perform a prophylactic central neck dissection.
We found the p.V600E mutation in 29% of our PTC patients, similar to the findings in the literature. The presence of the p.V600E mutation was not related to sex, age, and tumor size, nor to pathological characteristics that are well-known to be associated with poorer prognosis (extrathyroidal extension, multifocality, angiolymphatic invasion, and lymph node metastasis). Therefore, poorer prognosis was not related to the p.V600E mutation in our study. It was not the aim of this study to analyze the molecular profile of the metastases. It may be that the presence of the p.V600E mutation alone was not sufficient to result in a more aggressive metastasis, and another mutation is needed to transform a micrometastasis into a clinical apparent metastasis. A BRAF mutation could be only the first step of a series of events needed to transform a tumor into an aggressive tumor.
Lymph node metastases were strongly related to multifocality (OR 10.97) (37,38). In our previously reported article, 15% of multicenter micro-PTC was found (39). In this study, 53% of multifocality was found (27 tumors), independently of tumor size or extravascular invasion. This high frequency can be attributed to the careful pathologic search for PTC of any size in our institution. Lymph node metastasis was also related to younger age. Age was shown to be another important predictive factor of metastasis (40). Since we had only initial data, we found that younger patients have a larger number of lymph node metastases. We could also construct a model to predict the presence of lymph node metastasis considering age and multifocality. According to the model, we could expect young patients (<20 years old) without multifocal tumors and older patients (<60 years old) with multifocal tumors to present with lymph node metastasis.
In conclusion, the presence of a BRAF mutation in the primary tumor was not a helpful tool in the decision to perform a prophylactic central neck dissection. Known clinical and pathological aspects (younger age, multifocality, and angiolymphatic invasion) were related to neck metastasis. Younger age and multifocality are important aspects to consider in our patients, because they can be identified before surgery. Therefore, careful and highly sensitive ultrasound and FNAB in preoperative evaluation provide important information to detect multifocality and eventually improve surgery planning.
Footnotes
Acknowledgments
We thank FAPESP (2009/07544-0) for funding and resources, the Department of Endocrinology and Metabolism of the Faculty of Medicine at University of Sao Paulo, and the ICESP Board of Directors. We also thank Dr. Fabio Luiz de Menezes Montenegro (Faculty of Medicine, University of Sao Paulo) for his contribution to the article.
Disclosure Statement
The authors declare that no competing financial interests exist.